annals-diabetes tipo ii
TRANSCRIPT

inthe
clinicin the clinic
Type 2 DiabetesScreening and Prevention page ITC3-2
Diagnosis and Evaluation page ITC3-4
Treatment page ITC3-5
Practice Improvement page ITC3-13
CME Questions page ITC3-16
Section EditorBarbara Turner, MD, MSEDSankey Williams, MDDarren Taichman, MD, PhD
Physician WriterSandeep Vijan, MD, MS
The content of In the Clinic is drawn from the clinical information and education resources of the American College of Physicians (ACP), includingPIER (Physicians’ Information and Education Resource) and MKSAP (MedicalKnowledge and Self-Assessment Program). Annals of Internal Medicineeditors develop In the Clinic from these primary sources in collaboration withthe ACP’s Medical Education and Publishing Division and with the assistance of science writers and physician writers. Editorial consultants from PIERand MKSAP provide expert review of the content. Readers who are interested in these primary resources for more detail can consult http://pier.acponline.org, http://www.acponline.org/products_services/mksap/15/?pr31, and other resources referenced in each issue of In the Clinic.
CME Objective: To provide information about the screening and prevention, diag-nosis, and treatment of type 2 diabetes.
The information contained herein should never be used as a substitute for clinicaljudgment.
© 2010 American College of Physicians
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

Should we screen for type 2diabetes?Current data suggest that about 1 in4 persons with diabetes are unawareof their disease (1). Diabetes has afairly long asymptomatic phase, dur-ing which many patients will devel-op early disease complications. Somegroups have therefore suggestedscreening for diabetes every 3 yearsin persons older than 45 years and inpersons younger than 45 years whohave diabetes risk factors (Box) (3).
There is no consensus on whoshould be screened for diabetes orhow often. There is no direct evi-dence that screening improveshealth outcomes. Limited indirectevidence suggests that screening isunlikely to substantially improveoutcomes or to be cost-effectivewhen applied broadly (4, 5), andevidence-based guidelines focuson persons with particular risk fordiabetes complications, in whomthe diagnosis may alter manage-ment strategies (6).
Which patients are likely tobenefit from diabetes screening?Diabetes screening is most likely toimprove outcomes in patients withrisk factors for cardiovascular disease,particularly hypertension, becauseblood pressure treatment goals differaccording to the presence of diabetes(7). The same may be true of personswith dyslipidemia, although studieson the benefits of screening in thesepatients are lacking.
Diabetes is more likely to be de-tected in those with risk factors forthe disease (Box). However, beyondthe increased prevalence of disease,little evidence supports improvedclinical outcomes with screening inpersons without hypertension, andthus recommendations are basedlargely on expert opinion.
Can type 2 diabetes be prevented?Several high-quality randomizedtrials have shown that lifestylechanges in diet and exercise leadto substantial reductions in the in-cidence of type 2 diabetes in pa-tients with “prediabetes.” Predia-betes is defined as an impairedfasting glucose or impaired glu-cose tolerance that does not meetthe diagnostic criteria for diabetes(Table 1). These dietary and exer-cise programs achieved modestweight loss (generally 5% to 7% ofbody weight) yet are markedly effective.
© 2010 American College of Physicians ITC3-2 In the Clinic Annals of Internal Medicine 2 March 2010
1. American DiabetesAssociation. DiabetesStatistics. 2007. Ac-cessed at www.dia-betes.org/diabetes-basics/diabetes-statistics/ on 20 January2010.
2. Wild S, Roglic G,Green A, et al. Globalprevalence of dia-betes: estimates forthe year 2000 andprojections for 2030.Diabetes Care.2004;27:1047-53.[PMID: 15111519]
3. American DiabetesAssociation. Stan-dards of medical carein diabetes---2010.Diabetes Care.2010;33 Suppl 1:S11-61. [PMID: 20042772]
4. CDC Diabetes Cost-Effectiveness StudyGroup, Centers forDisease Control andPrevention. The cost-effectiveness ofscreening for type 2diabetes. JAMA.1998;280:1757-63.[PMID: 9842951]
5. Hofer TP, Vijan S, Hay-ward RA. Estimatingthe microvascularbenefits of screeningfor type 2 diabetes.Int J Technol AssessHealth Care. 2000; 16:822-33.[PMID: 11028137]
6. U.S. Preventive Servic-es Task Force. Screen-ing for type 2 dia-betes mellitus inadults: U.S. PreventiveServices Task Forcerecommendationstatement. Ann In-tern Med.2008;148:846-54.[PMID: 18519930]
7. Hoerger TJ, Harris R,Hicks KA, et al.Screening for type 2diabetes mellitus: acost-effectivenessanalysis. Ann InternMed. 2004;140:689-99. [PMID: 15126252]
Diabetes is one of the most common illnesses encountered by in-ternists. An estimated 23.6 million persons have diabetes in theUnited States, and only 17.9 million of these cases have been diag-
nosed (1). The incidence of diabetes is increasing because of the aging andchanging ethnic mix of the population and because of worsening obesity. Onthe basis of current trends, the prevalence of diabetes is expected to nearlydouble by 2030 (2). Although diabetes care is improving by many measures,complications are still common, and diabetes remains the leading cause of visualloss, amputation, and end-stage renal disease in the United States (1). In addi-tion, diabetes is a substantial risk factor for atherosclerotic disease, which is theleading cause of morbidity, mortality, and expenditures in persons with diabetes.
Screening andPrevention
Risk Factors for Type 2 Diabetes• Age >45 y• First-degree relative with type 2
diabetes• African-American, Hispanic, Asian,
Pacific Islander, or Native-American ethnicity
• History of gestational diabetes ordelivery of infant weighing ≥9 lbs
• The polycystic ovary syndrome• Overweight, especially abdominal
obesity• Cardiovascular disease, hypertension,
dyslipidemia, or other features of themetabolic syndrome
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

© 2010 American College of PhysiciansITC3-3In the ClinicAnnals of Internal Medicine2 March 2010
In a randomized, unblind, controlled trialof 522 overweight Finnish patients withimpaired glucose tolerance (mean age, 55years), an intervention aimed at a 5% re-duction in weight decreased the incidenceof newly diagnosed type 2 diabetes over 3years from 23% to 11%. The interventioninvolved personal counseling sessions toencourage a reduction in total and satu-rated fat intake to less than 30% and 10%of energy consumed, respectively; an in-crease in fiber intake; and moderate exer-cise for at least 30 min/d (8).
The Diabetes Prevention Project, a ran-domized, controlled trial of 3234 U.S. pa-tients with prediabetes (mean age, 51years; mean body mass index, 34 kg/m2),showed that a lifestyle modification pro-gram aimed at a 7% weight loss reducedthe cumulative incidence of diabetes over3 years from 29% to 14% compared withplacebo (9). The 10-year follow-up showedpersistence of the initial beneficial effect ofthe lifestyle changes. However, the inci-dence rates of diabetes in the lifestyle andplacebo group were similar after the study,implying that the intervention must bemaintained to see additional benefit (10).
In a randomized, controlled trial of 577 Chi-nese adults with impaired glucose tolerancerandomly assigned to diet, exercise, both, orneither, the incidence of diabetes over 6years was 68% among persons in the neithergroup, 44% in the diet group, 41% in the ex-ercise group, and 46% in the both group. All3 interventions showed statistically signifi-cant reductions in diabetes progression (11).
Some medications can prevent diabetes onset in patients with prediabetes.
In the medication group of the Diabetes Pre-vention Project, metformin (850 mg twicedaily) reduced the cumulative incidence of
diabetes from 29% to 22% over 3 years. Thisreduction was significant but smaller thanthat observed with lifestyle intervention (9).The 10-year follow-up again showed persist-ence of the initial beneficial effect, althoughthe incidence rates in the metformin and placebo group were similar after thestudy period (10).
In the randomized, double-blind, interna-tional Study to Prevent Non–Insulin-Dependent Diabetes Mellitus, which in-volved 1429 patients with impaired glu-cose tolerance, acarbose (100 mg 3 timesdaily) reduced the incidence of diabetesfrom 42% to 32% compared with place-bo. The relative risk reduction over 3 yearswas 25% (12).
The DREAM (Diabetes Reduction Assess-ment With Ramiripril and RosiglitazoneMedication) trial randomly assigned 5269adults without previous cardiovascular dis-ease but with impaired fasting glucose, im-paired glucose tolerance, or both to rosiglita-zone, 8 mg/d, or placebo and to rosi glita- zone, up to 15 mg/d, or placebo. After a me-dian 3 years, 11.6% of patients who receivedrosiglitazone developed diabetes or diedcompared with 26.0% of patients who re-ceived placebo (hazard ratio, 0.40 [95% CI,0.35 to 0.46]). Cardiovascular event rateswere statistically similar in both groups (13).
The implications of disease preven-tion interventions on the effective-ness of diabetes screening programshave not been fully elucidated, butscreening is generally needed toidentify the high-risk prediabetespopulation. The best option isprobably to consider screening per-sons who are at reasonably high-risk for the disease (Box) and toimplement preventative measures inthose who have prediabetes.
8. Tuomilehto J, Lind-ström J, Eriksson JG,et al; Finnish DiabetesPrevention StudyGroup. Prevention oftype 2 diabetes melli-tus by changes inlifestyle among sub-jects with impairedglucose tolerance. NEngl J Med.2001;344:1343-50.[PMID: 11333990]
9. Knowler WC, Barrett-Connor E, Fowler SE,et al; Diabetes Pre-vention Program Re-search Group. Reduc-tion in the incidenceof type 2 diabeteswith lifestyle inter-vention or met-formin. N Engl J Med.2002;346:393-403.[PMID: 11832527]
10. Knowler WC, FowlerSE, Hamman RF, etal; Diabetes Preven-tion Program Re-search Group. 10-year follow-up ofdiabetes incidenceand weight loss inthe Diabetes Preven-tion Program Out-comes Study.Lancet.2009;374:1677-86.[PMID: 19878986]
11. Pan XR, Li GW, HuYH, et al. Effects ofdiet and exercise inpreventing NIDDMin people with im-paired glucose toler-ance. The Da QingIGT and DiabetesStudy. Diabetes Care.1997;20:537-44.[PMID: 9096977]
12. Chiasson JL, JosseRG, Gomis R, et al;STOP-NIDDM TrailResearch Group.Acarbose for preven-tion of type 2 dia-betes mellitus: theSTOP-NIDDM ran-domised trial.Lancet.2002;359:2072-7.[PMID: 12086760]
13. Gerstein HC, Yusuf S,Bosch J, et al;DREAM (DiabetesREduction Assess-ment with ramipriland rosiglitazoneMedication) Trial In-vestigators. Effect ofrosiglitazone on thefrequency of dia-betes in patientswith impaired glu-cose tolerance orimpaired fasting glu-cose: a randomisedcontrolled trial.Lancet.2006;368:1096-105.[PMID: 16997664]
Table 1. Diagnostic Criteria for Type 2 Diabetes*Diagnosis Hemoglobin A
1cLevel, % Fasting Plasma Glucose†
mmol/L mg/dL
Prediabetes 6.0 to 6.4 5.55 to 6.94 100 to 125Diabetes ≥6.5 ≥7.0 ≥126
* A random glucose of 11.1 mmol/L or greater (≥200 mg/dL), with classic diabetes symptoms, may beindicative of diabetes. However, the test should be confirmed by checking fasting glucose or hemoglo-bin A1c. If an oral glucose tolerance test is used, a 2-hour postglucose load level of 11.1 mmol/L orgreater (≥200 mg/dL) is considered diagnostic of diabetes, whereas levels of 7.8 to 11.0 mmol/L (140to 199 mg/dL) are diagnostic of impaired glucose tolerance.
† Fasting is defined as no caloric intake for at least 8 h.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

14. American Associa-tion of Clinical En-docrinologists/American College of En-docrinology. State-ment on the Use ofA
1cfor the Diagnosis
of Diabetes. Accessed atwww.aace.com/pub/pdf/guidelines/AA-CEpositionA1cfeb2010.pdf on 4 February2010.
© 2010 American College of Physicians ITC3-4 In the Clinic Annals of Internal Medicine 2 March 2010
What are the diagnostic criteriafor type 2 diabetes innonpregnant adults?Clinicians should confirm the diag-nosis of diabetes in persons with clas-sic symptoms (polyuria, polydipsia,polyphagia, and weight loss) or evi-dence of diabetes complications (ret -in opathy, nephropathy, neuropathy,impotence, acanthosis nigricans, orfrequent infections). Diabetes may bediagnosed by a fasting plasma glucoselevel of 7.0 mmol/L or greater (≥126mg/dL), or when there are classicsymptoms by a nonfasting glucoselevel greater than 11.1 mmol/L (>200mg/dL); each should be confirmed ona different day. Impaired fasting glu-cose, or prediabetes, can be diagnosedin persons with fasting glucose levelsof 5.6 to 6.9 mmol/L (100 to 125 mg/dL) (Table 1).
A hemoglobin A1c
level of 6.5% orgreater is now recommended forthe diagnosis of type 2 diabetes(3, 14), because of its ease of use(because no fasting is required) andreliability relative to fasting glucose
measurement. The elevated hemoglobin A
1cvalue should be
confirmed by repeat testing.
A hemoglobin A1c level of 6.0% orgreater may identify patients mostlikely to benefit from interventionsaimed at preventing type 2 diabetes(for example, patients similar tothose identified as having predia-betes by fasting glucose or glucosetolerance tests).
What should the initial evaluationof patients with newly diagnosedtype 2 diabetes include?Providers should conduct a detailedhistory and physical examination,including assessment of blood pres-sure and an inspection for possiblediabetes complications, such as neu-rologic and foot examinations. Lab-oratory tests should assess levels ofglucose control (hemoglobin A1c),lipid profile, and nephropathy(urine microalbumin/creatinine ra-tio). At diagnosis, ophthalmologicassessment should be conducted toevaluate for retinopathy.
Diagnosis andEvaluation
Diagnosis and Evaluation... Type 2 diabetes is common and should be considered whenpatients present with suggestive symptoms (for example, polyuria or polydipsia), signs(for example, acanthosis nigricans), or complications of disease (for example, retinopa-thy). The diagnosis of diabetes can be confirmed by a hemoglobin A1c value of 6.5% orhigher, or by fasting plasma glucose levels greater then 7.0 mmol/L (126 mg/dL) on 2occasions at least 1 day apart. However, random plasma glucose levels and oral glucosetolerance testing can also be used to diagnose type 2 diabetes. Newly diagnosed pa-tients should be examined for hypertension, as well as neurologic, ophthalmologic, andpodiatric complications. The initial laboratory evaluation should include an assessmentof glucose control, a lipid profile, and a urine microalbumin/creatinine ratio.
CLINICAL BOTTOM LINE
Screening and Prevention... Little direct evidence shows clinical benefit frombroad-based screening programs for type 2 diabetes. The most evidence-basedapproach is to screen persons with other cardiovascular risk factors (hypertensionand perhaps dyslipidemia), because diabetes status alters the management goalsin these patients. Diabetes can be prevented in patients with prediabetes with ex-ercise and dietary programs aimed at modest weight loss. Medication may be in-dicated in those who cannot achieve lifestyle goals.
CLINICAL BOTTOM LINE
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

15. Intensive blood-glu-cose control withsulphonylureas or in-sulin compared withconventional treat-ment and risk ofcomplications in pa-tients with type 2 di-abetes (UKPDS 33).UK Prospective Dia-betes Study (UKPDS)Group. Lancet.1998;352:837-53.[PMID: 9742976]
16. Thomas DE, ElliottEJ, Naughton GA. Ex-ercise for type 2 dia-betes mellitus.Cochrane DatabaseSyst Rev.2006;3:CD002968.[PMID: 16855995]
© 2010 American College of PhysiciansITC3-5In the ClinicAnnals of Internal Medicine2 March 2010
What are the components ofnondrug therapy for patients withtype 2 diabetes?Lifestyle changes, primarily dietand exercise, are the cornerstonesfor the management of type 2 dia-betes and should be consideredfirst-line therapy unless severe hy-perglycemia requires immediatemedication treatment. No one dietor exercise regimen applies to allpatients with diabetes, and an indi-vidualized assessment should beused to develop a feasible strategy.
In a study of patients with newly diag-nosed type 2 diabetes, diet initially im-proved hemoglobin A
1clevels by 2.25
percentage points. However, control dete-riorated over time, and most patients even-tually required drug therapy (15).
A meta-analysis of 14 randomized trialscomparing exercise with no exercise in a to-tal of 377 patients with type 2 diabetesshowed that exercise significantly im-proved glycemic control, reduced visceraladipose tissue, and reduced plasma triglyc-eride levels even without weight loss (16).
What is the role of home glucosemonitoring for patients with type2 diabetes?Home glucose monitoring lets pa-tients and providers assess glucosecontrol longitudinally. Home moni-toring is part of the standard of carefor patients using insulin therapy toallow sensible dose adjustments andto help determine whether symptomsare due to hyperglycemia or hypo-glycemia. The optimum frequency ofhome monitoring has not been for-mally evaluated. The role of homeglucose monitoring to guide oraltherapy is less clear; a formal evidencereview found no consistent benefitsbut was limited by poor-quality datawith mixed intervention approachesand comparators (17).
Patients are generally advised tomonitor fasting and premeal glucose levels. However, postpran-dial measurement may be helpful inpatients with elevated hemoglobin
A1c levels despite normal fastinglevels. Some observational datasuggest that postmeal glucose ex-cursions may be tied to cardiovas-cular risk, leading some experts torecommend routine postprandialmonitoring. However, no trialshave shown that treating these ex-cursions reduces cardiovascular risk.
What target for glycemic controlshould physicians aim for inpatients with type 2 diabetes?The optimum target for glycemiccontrol is an area of mounting con-troversy. Most organizations andquality measurement groups advocatea target hemoglobin A1c level of 7%or less for most patients, based on theresults of the UKPDS (United Kingdom Prospective Diabetes
Treatment
General Advice about Diet and Exercise forPatients with Type 2 Diabetes
Diet• Stress the importance of moderation.• Base calorie recommendations on the goal of
achieving near-ideal body weight. Areasonable starting formula for weightmaintenance is as follows: 10 calories perpound of current body weight, plus 20% forsedentary patients; 33% for those whoengage in light physical activity; 50% forthose who are moderately active; and 75%for heavily active patients.
• Weight loss will require caloric restriction belowthese levels. Reducing caloric intake by15%–20% from maintenance levels is areasonable goal to produce gradual weight loss.
• Advise patient to avoid saturated fats.• Encourage regular meal schedule, particularly if
patient is receiving insulin.• Inform patient that frequent, small meals
might aid in weight loss and control of bloodglucose levels.
• Advise patient to choose complex carbohydrates(e.g., whole grains, cereals) over simple sugars(e.g., sweets).
Exercise• Individualize exercise regimen, consider
current level of activity, living situation, andcomorbid conditions.
• Consider beginning with 15 min of low-impactaerobic exercise 3 times per week for patientswho can exercise and gradually increasing thefrequency and duration to 30–45 min ofmoderate aerobic activity 3–5 d per wk.
• Caution patients receiving drug therapy abouthypoglycemia during and after exercise.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

17. Weischen LM, Bloe-mendal E, Nijpels G,et al. Self-monitoringof blood glucose inpatients with type 2diabetes who arenot using insulin.Cochrane DatabaseSyst Rev. 2005; 18:CD0050060. [PMID15846742]
18. Holman RR, Paul SK,Bethel MA, et al.Long-term follow-upof intensive glucosecontrol in type 2 dia-betes. N Engl J Med.2008;359:1577-89.[PMID: 18784090].
19. Gerstein HC, MillerME, Byington RP, etal. Action to ControlCardiovascular Riskin Diabetes StudyGroup. Effects of in-tensive glucose low-ering in type 2 dia-betes. N Engl J Med.2008;358:2545-59.[PMID: 18539917]
© 2010 American College of Physicians ITC3-6 In the Clinic Annals of Internal Medicine 2 March 2010
Study) (15). This randomized studyof 3867 patients with newly diag-nosed type 2 diabetes found that ascompared with dietary measuresalone, a more-intensive therapeuticapproach aimed at achieving a lowerhemoglobin A1c level resulted in fewermicrovascular complications over 10years (particularly the need for retinalphotocoagulation) but no clear bene-fit in cardiovascular outcomes. How-ever, because the study enrolled pa-tients with newly diagnosed milddisease, the results might not be gen-eralizable to other patients with dia-betes. In addition, by the end of thestudy, the mean hemoglobin A1c levelwas 8% in the intensive-treatmentgroup, making it difficult to firmly es-tablish the hemoglobin A1c targetneeded for a reduction in diabetescomplications.
In a 20-year follow-up of a subset of pa-tients after completion of the UKPDS study,the patients initially randomly assigned tointensive control had lower rates of my-ocardial infarction (16.8 vs. 19.6 per 1000patient-years) and death (26.8 vs. 30.3 per1000 patient-years), although differencesin glycemic control were not maintainedbetween groups (18).
This implies that early control mayhave a “memory” effect and mayprovide distant benefits, but alsothat significant benefits take manyyears to occur.
Some experts advocate more ag-gressive targets for glycemic controlor treating to near-normal glucoselevels when possible. Three trialsrecently evaluated this approach.
A study of 10 251 patients with type 2 dia-betes (mean age, 62.2 years) randomly as-signed participants to an intensive-treatmentgroup with a target hemoglobin A
1clevel less
than 6.0% or to a more conventional target-ed hemoglobin A
1clevel of 7.0% to 7.9%. The
achieved levels of control were 6.4% and7.5%, respectively. After a mean follow-up of3.5 years, the rate of cardiovascular endpoints (nonfatal myocardial infarction, non-fatal stroke, or cardiovascular death) did notdiffer, but the trial was stopped due to a 22%increase in total mortality in the intensive-control group (5.0% vs. 4.0%; P = 0.04).
Hypoglycemia and weight gain were morefrequent in the intensive-control group (19).
A randomized study of 1791 veterans withpreviously treated diabetes (mean age, 60.4years), compared an intensive-treatment ap-proach aiming to lower hemoglobin A
1clevel
by 1.5% with standard therapy over a medianof 5.6 years. Despite a median hemoglobin A
1c
level of 6.9% in the intensive-treatment groupcompared with 8.4% in the control group, therates of cardiovascular or total mortality,stroke, heart failure, need for vascular surgery,amputation, or microvascular events did notdiffer (20).
In a randomized study of 11 140 patients, anintensive-treatment group targeted a hemo-globin A
1clevel of 6.5% or more and achieved
a mean hemoglobin A1c
level of 6.5% over 5years compared with 7.3% in a standard-treatment control group. The rate ofnephropathy was reduced (4.1% vs. 5.2%; P = 0.006), but rates of cardiovascular eventsor mortality did not differ (21).
Interpretation and reconciliation ofthe results of the 4 major glucose-lowering trials is difficult. Moderateglucose control early in the diseasecourse (for example, a mean hemo-globin A1c level of 7% over the first 10years, but with a worsening trend overthat period) seems to eventually helpto decrease cardiovascular events andmortality. Whether more aggressivecontrol, at least in the short term,provides benefit or increases mortalityis debated. It is unclear whether anyspecific subgroups of patients areharmed or receive benefit from moreaggressive control. Current recom-mendations are to aim to control hemoglobin A
1cto less than 7% for
patients with diabetes, particularlyearly in the course of disease.Glycemic targets, however, must beindividualized by considering a patient’s risk for hypoglycemia, co-morbid conditions that limit life ex-pectancy, and factors that may limitthe safety of attempting aggressiveglucose control.
When should the treatment oftype 2 diabetes include drugs?Once a hemoglobin A1c goal is es-tablished, pharmacologic manage-ment should be instituted if diet
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

20. Duckworth W,Abraira C, Moritz T,et al; VADT Investiga-tors. Glucose controland vascular compli-cations in veteranswith type 2 diabetes.N Engl J Med.2009;360:129-39.[PMID: 19092145]
21. Patel A, MacMahonS, Chalmers J, et al;ADVANCE Collabora-tive Group. Intensiveblood glucose con-trol and vascularoutcomes in pa-tients with type 2 di-abetes. N Engl JMed. 2008;358:2560-72. [PMID: 18539916]
© 2010 American College of PhysiciansITC3-7In the ClinicAnnals of Internal Medicine2 March 2010
and exercise do not achieve thegoal. In general, initiation of phar-macologic therapy should not bedelayed while awaiting the resultsof diet and exercise except in moti-vated and adherent patients. If dietand exercise have not accomplishedthe targeted reduction in glycemicvalues within approximately 6weeks, pharmacologic therapyshould be initiated (3, 14, 22). Inaddition, those with severe hyper-glycemia or symptoms may requirepharmacologic intervention imme-diately, although severe hyper-glycemia is not clearly defined. Inaddition to lifestyle changes in dietand exercise, most patients shouldbe treated with metformin.
How should physicians selecttherapies for a patient fromamong the many oral drugsavailable for type 2 diabetes?Table 2 provides an overview of theclasses of oral agents available totreat type 2 diabetes. Data are in-sufficient regarding the relative
efficacy of many of the availableoral therapies for type 2 diabetes atimproving clinical end points.
In the UKPDS, in patients whowere more than 120% of ideal bodyweight, metformin was superior tosulfonylureas and insulin in reducing mortality, despite identical levels ofglycemic control (23). Metforminalso had lower rates of hypoglycemiaand weight gain than insulin or sul-fonylureas. Metformin should not beused in patients with severe renal in-sufficiency (glomerular filtration rate< 30 mL/min per 1.73 m2), sympto-matic heart failure, or severe liverdisease, and must be stopped beforeradiologic procedures requiring intravenous contrast dye because ofthe risk for lactic acidosis.
In patients with contraindications orintolerance to metformin, the choiceof oral agents should be based on pa-tient preferences regarding potentialside effects, efficacy, and cost. Al-though most drugs achieve similar
Table 2. Oral Medications for Type 2 DiabetesDrug Initial Dose Maximum Dose Usual Dose
Biguanide
Metformin 500 mg bid or 850 mg/d 2550 mg/d 500–1000 mg bid
Metformin XR 500 mg/d 2000 mg/d 1500–2000 mg/d
Sulfonylurea
Glimepiride 1–2 mg/d 8 mg/d 4 mg/d
Glipizide 2.5–5 mg/d 40 mg/d 10–20 mg/d (or bid)
Glipizide SR 5 mg/d 20 mg/d 5–20 mg/d (or bid)
Glyburide 2.5–5 mg/d 20 mg/d 5–20 mg/d (or bid)
Glyburide micronized 0.75–3 mg/d 12 mg/d 3–12 mg/d (or bid)
Thiozolidinedione
Pioglitazone 15–30 mg/d 45 mg/d 15–45 mg/d
Rosiglitazone 4 mg/d (or bid) 8 mg/d 4–8 mg/d (or bid)
α-Glucosidase inhibitors
Acarbose 25 mg tid 100 mg tid 25–100 mg tid
Miglitol 25 mg tid 100 mg tid 25–100 mg tid
Meglitinides
Repaglinide 0.5 mg before meals 4 mg before meals (16 mg/d). 0.5–4 mg before Wait ≥7 d between dose mealsincreases)
Netaglinide 120 mg tid before meals 120 mg tid before 60–120 mg tid before (60 mg tid if near meals mealsglycemic goals)
Dipeptidyl peptidase IV inhibitor
Sitagliptin 100 mg/d 100 mg/d 100 mg/d
Saxagliptin 2.5 mg/d 5 mg/d 5 mg/d
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

22. AACE Diabetes Mel-litus Clinical PracticeGuidelines TaskForce. American As-sociation of ClinicalEndocrinologistsmedical guidelinesfor clinical practicefor the managementof diabetes mellitus.Endocr Pract.2007;13 Suppl 1:1-68. [PMID: 17613449]
23. UK Prospective Dia-betes Study (UKPDS)Group. Effect of in-tensive blood-glu-cose control withmetformin on com-plications in over-weight patients withtype 2 diabetes(UKPDS 34). Lancet.1998;352:854-65.[PMID: 9742977]
24. Yki-Järvinen H,Kauppila M, Kujan-suu E, et al. Compari-son of insulin regi-mens in patientswith non-insulin-de-pendent diabetesmellitus. N Engl JMed. 1992;327:1426-33. [PMID: 1406860]
© 2010 American College of Physicians ITC3-8 In the Clinic Annals of Internal Medicine 2 March 2010
glycemic control, differences inmechanism, tolerability, and the tim-ing of administration may help to individualize care. For example, non-sulfonylurea insulin secretagogues(nateglinine, replaglinide) and the α-glucosidase inhibitors (acarbose,miglitol) can be administered beforemeals and may therefore be useful topatients with irregular mealtimes (forexample, truck drivers).
Most patients with diabetes haveworsening glycemic control over timeand will require more than one agentto maintain adequate glycemic con-trol. Increasing the dose of existingoral agents is generally the first step,although the response from dose es-calation, particularly with metforminand sulfonylureas, is limited. Patientstherefore often require the addition ofa second oral agent. Although datashowing the effect of various drugcombinations on glycemic control areavailable, few studies have assessedclinical end points. Several combina-tion formulations are available andmay provide advantages in conven-ience or cost for some patients. Sul-fonylureas and thiozolidinedionesmay each cause hypoglycemia; thio-zolidinediones may also cause weightgain. Patients should be warned aboutthese possibilities and educated torecognize and treat hypoglycemia.
When should physicians considerinsulin therapy for patients withtype 2 diabetes?Patients who do not achieve adequateglycemic control with oral medica-tions, whether alone or in combina-tion, are candidates for insulin therapy.The Box lists other indications.
Many insulin formulations are avail-able, differing primarily in their onsetof action and duration (Table 3). Nosingle regimen has been established assuperior (24). Most patients achieve a1- to 2-percentage point decrease inhemoglobin A1c level after starting in-sulin (25, 26). When intensiveglycemic control is planned, fastingglucose values of less than
6.7 mmol/L (<120 mg/dL) are rea-sonable. The primary risks of insulinare hypoglycemia and weight gain,and patients must be warned aboutthese possibilities and educated to rec-ognize and treat hypoglycemia (15).
When insulin therapy begins, mostpatients can be treated with a oncedaily injection. Patients without hypo-glycemia can often be treated with asingle bedtime dose of neutral prota-mine Hagedorn (NPH) in combina-tion with an oral agent. In patientswho have normal fasting glucose orhigh-risk for hypoglycemia, glargineor detemir may be a preferred firstchoice. Starting doses of insulin aretypically 0.1 to 0.2 U/kg. If the hemo-globin A
1cremains above goal despite
normal fasting glucose levels, prandialinsulin may be considered.
A combination of an insulin and anoral agent (typically either NPH orglargine with metformin) can beeffective and can limit insulin doseto once daily at bedtime, which isoften more acceptable to patients(27). Some patients need twice-dai-ly insulin to achieve glycemic tar-gets, but more-frequent injectionshave not been shown to substan-tially improve control in most pa-tients with type 2 diabetes.
What other options are availableif control is inadequate ontraditional oral drugs or insulin?Two newer injectable agents and 1newer oral agent are available forcontrol of blood glucose in type 2diabetes.
Other Indications for Insulin Therapyin Patients With Type 2 Diabetes• New diagnosis with severe,
symptomatic hyperglycemia• Hospitalization, where frequent
changes in diet and such proceduresas contrast imaging studies make oralagents relatively unsafe
• Pregnancy, where insulin is consideredthe standard of care (although recentstudies suggest that some oral agentsalso are safe to use)
• Intolerance of oral medications
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

25. Buse JB, Wolffenbut-tel BH, Herman WH,et al. DURAbility ofbasal versus lispromix 75/25 insulin ef-ficacy (DURABLE) tri-al 24-week results:safety and efficacy ofinsulin lispro mix75/25 versus insulinglargine added tooral antihyper-glycemic drugs inpatients with type 2diabetes. DiabetesCare. 2009;32:1007-13. [PMID: 19336625]
26. Hayward RA, Man-ning WG, Kaplan SH,et al. Starting insulintherapy in patientswith type 2 diabetes:effectiveness, com-plications, and re-source utilization.JAMA.1997;278:1663-9.[PMID: 9388085]
© 2010 American College of PhysiciansITC3-9In the ClinicAnnals of Internal Medicine2 March 2010
Pramlintide is a synthetic form ofthe pancreatic hormone amylin.Pramlintide requires preprandialdosing, making it somewhat lessconvenient than other agents formany patients with diabetes. Pram-lintide is typically started at a doseof 60 mg subcutaneously beforemeals, and increased to 120 mg if itis tolerated. The dose of short-acting insulins should be decreasedby 50% before starting pramlintideto minimize the risk for hypo-glycemia. Blood sugar should bechecked before and after meals andat bedtime; when pramlintide doseis stabilized, insulin dosing shouldbe optimized. The most commonside effects are nausea and hypo-glycemia, which may require a dosereduction or discontinuation.
Exenatide is an incretin mimetic,which acts through glucagon-likepeptide 1, a naturally occurring hor-mone involved in glucose
homeostasis. Exanatide has manyeffects, including enhanced glucose-dependent insulin secretion; delayedgastric emptying; and, in many pa-tients, decreased appetite andweight loss. Exenatide should beconsidered in persons receiving oralagents who have not achievedglycemic goals. It is not approved bythe U.S. Food and Drug Adminis-tration for combination with in-sulin, although some studies suggestit is effective in this setting (28, 29).The primary risks of exenatide aregastrointestinal effects, notably nau-sea and vomiting, and possibly in-creased risk for pancreatitis.
Exenatide should be started at 5 μgsubcutaneously twice daily. Patientstaking sulfonylureas should have theirdose reduced to avoid hypoglycemia;a change in metformin dose is notnecessary. The dose of exenatide canbe increased to 10 μg twice daily inpersons who tolerate the drug.
Table 3. Onset and Mechanisms of Action of Various Types of Insulin*Pharmacodynamic Characteristic
Currently AvailableInsulin Preparations† Onset Peak Duration
Insulin classRapid-acting (insulin analogues ≤30 min 0.5–3 h 3–5 h
lispro, aspart, glulisine) Short-acting (human regular) 0.5–1 h 2–5 h Up to 12 hIntermediate-acting 1.5–4 h 4–12 h Up to 24 h
(human NPH)Long-acting (insulin analogues 0.8–4 h Relatively Up to 24 h
glargine, detemir) peakless Human insulin mixtures
70% NPH/30% regular 0.5–2 h 2–12 h Up to 24 h50% NPH/50% regular 0.5–2 h 2–5 h Up to 24 h
Analogue mixtures75% lispro <15 min 1–2 h Up to 24 h
protamine/25% lispro 50% lispro <15 min 1–2 h Up to 24 h
protamine/50% lispro 70% aspart 10–20 min 1–4 h Up to 24 h
protamine/30% aspart
NPH = Neutral protamine Hagedorn.
* The time course of action of each insulin may vary among persons or at different times in the sameperson. Because of this variation, the time periods indicated here should be considered general guide-lines only. Inhaled insulin powder (Exubera, Pfizer) has been omitted because it has been withdrawnfrom the market.
† Preperations vary within class. Please see package inserts for specific pharmacodynamic data.
‡ Blood glucose–lowering effect.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

27. Yki-Järvinen H, RyysyL, Nikkilä K, et al.Comparison of bed-time insulin regi-mens in patientswith type 2 diabetesmellitus. A random-ized, controlled trial.Ann Intern Med.1999;130:389-96.[PMID: 10068412]
28. Sheffield CA, KaneMP, Busch RS, et al.Safety and efficacyof exenatide in com-bination with insulinin patients with type2 diabetes mellitus.Endocr Pract.2008;14:285-92.[PMID: 18463034]
29. Yoon NM, CavaghanMK, Brunelle RL, etal. Exenatide addedto insulin therapy: aretrospective reviewof clinical practiceover two years in anacademic en-docrinology outpa-tient setting. ClinTher. 2009;31:1511-23. [PMID: 19695400]
30. Vijan S, Hayward RA.Treatment of hyper-tension in type 2 di-abetes mellitus:blood pressuregoals, choice ofagents, and settingpriorities in diabetescare. Ann InternMed. 2003;138:593-602.[PMID: 12667032]
© 2010 American College of Physicians ITC3-10 In the Clinic Annals of Internal Medicine 2 March 2010
Sitagliptin is an oral dipeptidylpeptidase-IV (DPP-IV) inhibitorthat also works through the in-cretin and glucagon-like peptide 1pathway. Sitagliptin is dosed at 100mg/d. It can be used alone or incombination with other oral drugs,particularly metformin. The mainside effects of sitagliptin are nausea,diarrhea, headache, and upper res-piratory symptoms. It may also in-crease the risk for pancreatitis.
Saxagliptin is a newly approved oralDPP-IV inhibitor. It is dosed at2.5 to 5 mg/d, with the lower dosepreferred in persons with renal in-sufficiency or those on other drugsthat strongly inhibit cytochromeP450 3A4/5. The most commonside effects are headache, upper res-piratory symptoms, and urinarytract infections.
What novel therapeutic optionsare on the horizon for patientswith type 2 diabetes?Several additional DPP-IV in-hibitors are being developed, in-cluding one (vildagliptin) that hasbeen approved for use in the Euro-pean Union. Liraglutide, a long-acting injectable glucagon-like pep-tide 1 analogue, was recently approvedby the U.S. Food and Drug Adminis-tration. It is similar to exenatide but isapproved for once-daily injection. Ex-enatide is currently being reviewed foronce-weekly injection.
Besides glycemic control, whatother clinical interventions reducecomplications of type 2 diabetes?Hypertension is a major risk factorfor diabetes complications, andblood pressure control may be themost important treatment to reducecomplications in patients with dia-betes. Patients with diabetes andhypertension should receive aggres-sive therapy aimed at maintaining ablood pressure of less than 135/80mm Hg (30–32). The best choiceof agents for blood pressure controlhas not been defined. A combina-tion of a thiazide diuretics and
either an angiotensin-converting enzyme (ACE) inhibitor or an an-giotensin-receptor blocker (ARB)may be preferred treatment inmany patients with diabetes andhypertension. Both ACE inhibitorsand ARBs prevent the progressionof microalbuminuria in patientswith type 2 diabetes. Other agentsshould be added as needed toachieve blood pressure goals (30).
Treatment of dyslipidemia is also apriority in patients with diabetes.For primary prevention, evidencesuggests that nearly all patientswith diabetes who are older than40 years benefit from statin thera-py, regardless of initial level of low-density lipoprotein (LDL) choles-terol. Optimum LDL cholesteroltargets, however, have not been es-tablished, and moderate dosing ofstatins is recommended (33, 34).For secondary prevention, statin useshould be encouraged in all patientswithout contraindication. Opti-mum LDL targets have not beenestablished; some evidence suggeststhat higher-dose statin therapy (forexample, simvastatin, 80 mg, oratorvastatin, 80 mg) may be moreeffective than lower-dose statintherapy in patients with existingcoronary artery disease (35, 36).
Aspirin therapy is generally recom-mended for patients with type 2 di-abetes (3), although its benefit inpreventing progression of cardiovas-cular disease in patients with diabetes is unclear. A recent ran-domized, controlled study of aspirinuse in patients with type 1 or 2 dia-betes found no evidence to supportthe use of aspirin for the primaryprevention of cardiovascular events(37). Patients with a history of heartdisease and no contraindicationshould take aspirin, 75 to 325 mg/d.
Retinal examinations reduce the in-cidence of vision loss in patientswith type 2 diabetes. Examinationfrequency for patients withouthigh-risk retinal lesions may range
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

31. Snow V, Weiss KB,Mottur-Wilson C;Clinical Efficacy Sub-committee of theAmerican College ofPhysicians. The evi-dence base for tightblood pressure con-trol in the manage-ment of type 2 dia-betes mellitus. AnnIntern Med 2003;138: 587-92.[PMID: 12667031]
32. Holman RR, Paul SK,Bethel MA, et al.Long-term follow-upafter tight control ofblood pressure intype 2 diabetes. NEngl J Med.2008;359:1565-76.[PMID: 18784091]
33. Vijan S, Hayward RA;American College ofPhysicians. Pharma-cologic lipid-lower-ing therapy in type 2diabetes mellitus:background paperfor the AmericanCollege of Physi-cians. Ann InternMed. 2004;140:650-8. [PMID: 15096337]
34. Snow V, AronsonMD, Hornbake ER, etal; Clinical EfficacySubcommittee ofthe American Col-lege of Physicians.Lipid control in themanagement oftype 2 diabetes mel-litus: a clinical prac-tice guideline fromthe American Col-lege of Physicians.Ann Intern Med2004; 140: 644-9.[PMID: 15096336]
35. LaRosa JC, GrundySM, Waters DD, et al;Treating to New Tar-gets (TNT) Investiga-tors. Intensive lipidlowering with ator-vastatin in patientswith stable coronarydisease. N Engl JMed. 2005;352:1425-35. [PMID: 15755765]
36. Cannon CP, Braun-wald E, McCabe CH,et al. Intensive ver-sus moderate lipidlowering with statinsafter acute coronarysyndromes. N Engl JMed. 2004; 350:1495-504.[PMID: 15007110]
© 2010 American College of PhysiciansITC3-11In the ClinicAnnals of Internal Medicine2 March 2010
Table 4. Antihypertensive Agents in Type 2 Diabetes*Antihypertensive Agent Notes Advantages Disadvantages
ACE inhibitors ADA and ACP Cardioprotective Caution with advanced advocate as Renoprotective renal failurefirst-line agent
ARBs ADA and ACP Cardioprotective Expensiveadvocate as Renoprotective Caution with advanced second-line agent renal failure
β-Blockers Use in patients Cardioprotective Can mask with known CAD Most are inexpensive hypoglycemia
May be associated with weight gain and metabolic abnomalities
Thiazide diuretics Often used in May reduce CHF May elevate blood combination with Inexpensive glucose levelsother agents to Cardioprotectiveachieve blood pressure targets.ACP advocates asfirst-line age.
α-Blockers Use only if target Can help alleviate Do not protect against blood pressure symptoms of benign CHF. Generally must cannot be reached prostatic hypertrophy be used with other with other agents agent
Calcium-channel Use if target blood Some evidence Appear to offer less blockers pressure cannot be suggests this class is cardioprotection than
reached with ACE cardioprotective other antihypertensive inhibitors, ARBs, agentsand thiazides
*ACE = angiotensin-converting enzyme; ACP = American College of Physicians; ADA = American Dia-betes Association; ARB = angiotensin-receptor blocker; CAD = coronary artery disease; CHF = conges-tive heart failure.
from 1 to 3 years, depending onunderlying risk (34). Measurementof urine microalbumin/creatinineratio helps to guide the use of ACEinhibitors or ARBs in persons withnephropathy and to reduce the riskfor progression to end-stage renaldisease. Neuropathy screening andfoot care are essential in reducingthe risk for amputation. Painfulneuropathy is uncommon in type 2diabetes but can be treated withmany agents.
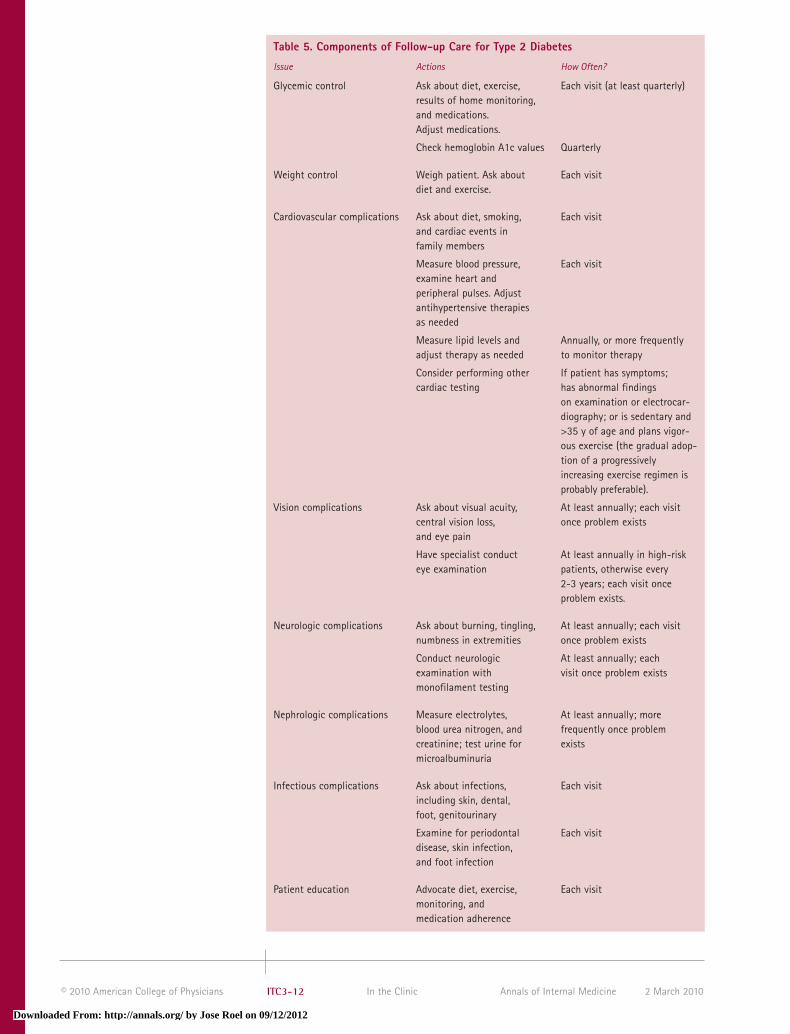
How frequently should physiciansee patients with type 2 diabetes,and what should physiciansinclude in follow-up visits?No direct evidence examines theideal frequency of visits for patientswith type 2 diabetes. Expert opin-ion and the recommended frequen-cy of monitoring hemoglobin A1clevels suggest that quarterly visitsare reasonable; for patients withstable disease, this can be reduced
to every 6 months (3). Table 5 listscomponents of follow-up.
When should generalist physiciansconsult specialists to care forpatients with type 2 diabetes?Meta-analyses have found that dia-betes education by a certified educa-tor is effective in improving manykey domains in diabetes care, includ-ing glycemic control, although thedurability of these effects is not clear.
Endocrinology consultation is help-ful when there are questions aboutdiagnosis or when glycemic manage-ment has become difficult (for exam-ple, in patients with highly labileblood glucose levels). Patients whoare pregnant or contemplating preg-nancy should be referred to assistwith glucose control, because poorglucose control is associated with ad-verse fetal outcomes.
Ophthalmologic examination,whether by ophthalmology,
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
© 2010 American College of Physicians ITC3-12 In the Clinic Annals of Internal Medicine 2 March 2010
Table 5. Components of Follow-up Care for Type 2 Diabetes
Issue Actions How Often?
Glycemic control Ask about diet, exercise, Each visit (at least quarterly)results of home monitoring, and medications. Adjust medications.
Check hemoglobin A1c values Quarterly
Weight control Weigh patient. Ask about Each visitdiet and exercise.
Cardiovascular complications Ask about diet, smoking, Each visitand cardiac events in family members
Measure blood pressure, Each visitexamine heart and peripheral pulses. Adjustantihypertensive therapiesas needed
Measure lipid levels and Annually, or more frequently adjust therapy as needed to monitor therapy
Consider performing other If patient has symptoms; cardiac testing has abnormal findings
on examination or electrocar-diography; or is sedentary and>35 y of age and plans vigor-ous exercise (the gradual adop-tion of a progressivelyincreasing exercise regimen isprobably preferable).
Vision complications Ask about visual acuity, At least annually; each visit central vision loss, once problem existsand eye pain
Have specialist conduct At least annually in high-risk eye examination patients, otherwise every
2-3 years; each visit onceproblem exists.
Neurologic complications Ask about burning, tingling, At least annually; each visit numbness in extremities once problem exists
Conduct neurologic At least annually; each examination with visit once problem existsmonofilament testing
Nephrologic complications Measure electrolytes, At least annually; more blood urea nitrogen, and frequently once problem creatinine; test urine for existsmicroalbuminuria
Infectious complications Ask about infections, Each visitincluding skin, dental, foot, genitourinary
Examine for periodontal Each visitdisease, skin infection, and foot infection
Patient education Advocate diet, exercise, Each visitmonitoring, and medication adherence
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

37. Belch J, MacCuish A,Campbell I, et al; Pre-vention of Progres-sion of Arterial Dis-ease and DiabetesStudy Group. Theprevention of pro-gression of arterialdisease and diabetes(POPADAD) trial: fac-torial randomisedplacebo controlledtrial of aspirin andantioxidants in pa-tients with diabetesand asymptomaticperipheral arterialdisease. BMJ.2008;337:a1840.[PMID: 18927173]
© 2010 American College of PhysiciansITC3-13In the ClinicAnnals of Internal Medicine2 March 2010
What measures do U.S.stakeholders use to evaluate thequality of care for patients withtype 2 diabetes?The Ambulatory Care Quality Al-liance recommends several meas-ures of diabetes care. Note thatthese do not perfectly align withclinical targets. The Box describesthe current standards of care, whichare widely endorsed.
Note that the clinical targets forblood glucose and blood pressureare specifically designed to identifypoor control rather than optimumcontrol. These are not necessarilyclinical targets but instead
acknowledge several issues, such asvariation in populations treated byphysicians, issues of measurementreliability, and the achievability ofclinical goals.
What do professional organizationsrecommend regarding the care ofpatients with type 2 diabetes?Several profession associationspublish guidelines for diabetescare. Note that these do not al-ways agree on all aspects and thatthe nature of the organization in-evitably influences recommenda-tions. Many guidelines for dia-betes can be found at the NationalGuideline Clearinghouse
Podiatry evaluation is helpful formanagement of lesions, such as cal-luses or deformities, which requireintervention to reduce the risk forfoot ulcers and amputation.
When should patients with type 2diabetes be hospitalized?Some patients with severe, sympto-matic hyperglycemia may requirehospitalization, particularly at thetime of diagnosis. Diabetic ketoaci-dosis or hyperosmolar coma requires hospitalization for man-agement. Diabetes complications,including cellulites in need of intra-venous antibiotic therapy, may re-quire hospitalization.
optometry, or through retinalphotography, should be conductedevery 1 to 3 years depending onprevious examination results andthe degree of glycemic control(38). Other conditions (for exam-ple, known retinopathy, glaucoma,cataracts) may require more fre-quent examination.
Nephrology evaluation is prudent inpatients whose glomerular filtrationrate has decreased to less than 45mL/min per 1.73 m2, or in whom theorigin of renal insufficiency is unclear.Patients with hyperkalemia, acidemia,or difficult-to-control blood pressuremay also benefit.
Current Standards of Diabetes Care
Eye Examination• Percentage of patients who received
a retinal or dilated eye examinationby an eye care professional(optometrist or ophthalmologist)during the reporting year or duringthe previous year if a patient is atlow risk for retinopathy.
• A patient is considered low-risk if all 3of the following criteria are met: thepatient is not taking insulin, the patienthas a hemoglobin A
1clevel <8.0%; and
the patient had no evidence ofretinopathy in the past year.
Hemoglobin A1c
Management• Percentage of patients with diabetes
with one or more hemoglobin A1c
test(s) conducted during themeasurement year.
Hemoglobin A1c
Management Control• Percentage of patients with diabetes
whose most recent hemoglobin A1c
level was >9.0% (poor control).
Lipid Measurement• Percentage of patients with diabetes
with ≥1 low-density lipoprotein (LDL)cholesterol level test (or allcomponent tests).
LDL Cholesterol Level• Percentage of patients with diabetes
with most recent LDL cholesterol levelless than 2.59 mmol/L (<100 mg/dL)or less than 3.37 mmol/L (<130 mg/dL).
Blood Pressure Management• Percentage of patients with diabetes
who had their blood pressuredocumented in the past year as lessthan 140/90 mm Hg.
Treatment... Diet and exercise are the cornerstones for achieving glycemic control inpatients with type 2 diabetes, and clinicians should stress the importance of lifestylemodification regardless of whether patients also require pharmacologic therapy.Metformin is superior to sulfonylureas and insulin in reducing mortality and shouldbe considered in patients without contraindications or intolerance to metformin.However, data comparing the many other oral and insulin-based therapies are limit-ed, and clinicians should consider effectiveness, potential side effects, comorbid con-ditions, costs, and patient preferences when selecting treatment regimens forglycemic control. The optimum target for glycemic control in patients with type 2diabetes is debated; a hemoglobin A
1clevel less than 7% is recommended but must
be individualized according to risks, particularly hypoglycemia, and factors whichmay limit benefits, such as short life expectancy or other factors that may limit theachievability of tight control. In addition to glycemic control, patients with type 2diabetes should be treated for dyslipidemia and should receive therapy aimed atmaintaining a blood pressure of less than 135/80 mm Hg.
CLINICAL BOTTOM LINE
Practice Improvement
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
38. Vijan S, Hofer TP,Hayward RA. Cost-utility analysis ofscreening intervalsfor diabeticretinopathy in pa-tients with type 2 di-abetes mellitus.JAMA. 2000;283:889-96. [PMID: 10685713]
39. Qaseem A, Vijan S,Snow V, et al; ClinicalEfficacy AssessmentSubcommittee ofthe American Col-lege of Physicians.Glycemic controland type 2 diabetesmellitus: the optimalhemoglobin A1c tar-gets. A guidancestatement from theAmerican College ofPhysicians. Ann In-tern Med.2007;147:417-22.[PMID: 17876024
inthe
c linicTool Kit
in the clinic
Type 2 Diabetes
PIER Moduleswww.pier.acponline.orgAccess the PIER module on type 2 diabetes. PIER modules provide evi-dence-based, updated information on current diagnosis and treatment inan electronic format designed for rapid access at the point of care.
Patient Informationwww.annals.org/intheclinic/toolkit-diabetes.htmlAccess the Patient Information material that appears on the followingpages for duplication and distribution to patients.http://diabetes.niddk.nih.gov/dm/pubs/type2_ES/index.htm (English)http://diabetes.niddk.nih.gov/dm/pubs/type2_ES/index.htm#Spanish (Spanish)Access information for patients by the National Institute of Diabetes andDigestive and Kidney Diseases: Type 2 Diabetes: What You Need toKnowwww.nlm.nih.gov/medlineplus/diabetes.htmlAccess MEDLINE Plus information about diabetes for patients, includ-ing an interactive tutorial available in both English and Spanish.
Clinical Guidelineswww.aace.com/pub/pdf/guidelines/DMGuidelines2007.pdfGuidelines from the American Association of Clinical Endocrinologistsguidelines, released in 2007, on the management of diabetes mellitus.www.bmj.com/cgi/content/extract/336/7656/1306Guidelines from The National Institute for Health and Clinical Excel-lence for the United Kingdom’s National Health Service, updated in2008, on management of diabetes type 2.http://diabetes.acponline.org/Access the ACP Diabetes Portal for clinical information, managementtools, and patient information regarding diabetes care.
Diagnostic Tests and Criteriahttp://pier.acponline.org/physicians/public/d296/tables/d296-t1.htmlList of screening and diagnostic tests for diabetes mellitus from theAmerican College of Physicians.
Quality Measureswww.qualitymeasures.ahrq.gov/search/searchresults.aspx?Type=3&txtSearch=diabetes&num=20Access information on National Quality Measures Clearinghouse relatingto diabetes.http://pier.acponline.org/qualitym/t002.htmlAccess quality measures related to diabetes from the Centers for Medicare& Medicaid Services Physician Quality Reporting Initiative (PQRI).
2 March 2010Annals of Internal MedicineIn the ClinicITC3-14© 2010 American College of Physicians
(www.guidelines.gov). The follow-ing organizations are 3 of the mostcommonly cited sources.
American College of Physicians (ACP)The ACP conducted systematic re-views of the evidence to constructguidelines on the management ofhypertension and lipids in type 2diabetes (30–34). In addition, theACP reviewed and rated existingguidelines for glycemic control anddeveloped an assessment of the bestexisting guidelines on the topic(39). Guidelines are available atwww.acponline.org/clinical_information/guidelines/.
American Diabetes Association (ADA)The ADA releases diabetes stan-dards of care yearly. The standardsare broad and encompass most rele-vant areas of diabetes screening,prevention, and management.Complete guidelines are availableat http://care.diabetesjournals.org/content/33/Supplement_1/S11.full.
American Association of ClinicalEndocrinologists (AACE)The AACE last updated theirguidelines in 2007. They are avail-able at www.aace.com/pub/pdf/guidelines/DMGuidelines2007.pdf.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
In the ClinicAnnals of Internal Medicine
Pati
ent
Info
rmat
ion
THINGS YOU SHOULDKNOW ABOUT TYPE 2DIABETES
What is type 2 diabetes?• In type 2 diabetes, a hormone called insulin cannot
adequately control the use of sugar from food. So,sugar builds up in the blood.
• If type 2 diabetes is not controlled, complicationsmay include vision loss, kidney damage, and poorcirculation and nerve damage that can lead toinfections, foot ulcers, and potentially amputation.Nerve damage may also lead to digestive problems.
• Type 2 diabetes is sometimes called non–insulin-dependent diabetes mellitus or adult-onset diabetes.
Who is most likely to get type 2 diabetes?• Overweight or inactive people
• People older than 45 years
• People with a family history of type 2 diabetes
• Women who had diabetes when they were pregnant.
• African Americans, Latinos, Native Americans, AsianAmericans, Native Hawaiians, and other PacificIslanders
How is type 2 diabetes diagnosed?• Your doctor may suspect diabetes if you have
symptoms such as increased thirst, urination, andfatigue. A diagnosis of diabetes is made with bloodtests that measure whether the glucose in yourblood is too high. Sometimes the blood testing isdone after fasting or after you eat food with sugar.
How is type 2 diabetes treated?• Type 2 diabetes is a long-term condition. Treatment is
focused on lowering high levels of blood glucose.Long-term goals are to prevent diabetes-relatedcomplications.
• The primary treatment is regular exercise and ahealthful diet. If diet and exercise are not effectiveenough, medications may be used to lower bloodsugar levels.
• Patients may practice regular self-testing to checkblood sugar levels at home. This allows them tomonitor how well diet, exercise, and any diabetesmedications are working.
How is type 2 diabetes different fromtype 1 diabetes?• In type 1 diabetes, the pancreas (where insulin is
made) is attacked by the body itself. These patientsneed to take insulin. Not all patients with type 2diabetes need insulin.
What are some symptoms of type 2diabetes?• Dry mouth, increased thirst, hunger, or urination
• Blurred vision, or numbness of the hands or feet
• Unexplained weight loss or fatigue
• Impotence
• Dark, velvety looking skin in the armpit or back of theneck
For More Information
American College of Physicians Foundation: HEALTH TiPS: Diabeteswww.acpfoundation.org/files/ht/diab_en.pdf
American Diabetes Association: Diabetes Basicswww.diabetes.org/diabetes-basics/type-2/
National Institute of Diabetes and Digestive and Kidney Diseases:Type 2 Diabetes: What You Need to Knowhttp://diabetes.niddk.nih.gov/dm/pubs/type2_ES/index.htm (English)http://diabetes.niddk.nih.gov/dm/pubs/type2_ES/index.htm#Spanish
(Spanish)
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
5.
4.
3.
CME Questions
2 March 2010Annals of Internal MedicineIn the ClinicITC3-16© 2010 American College of Physicians
A 72-year-old man comes to the officefor a follow-up evaluation. He has hadtype 2 diabetes mellitus for 13 years.Over the past 5 years, his hemoglobinA1c value has slowly increased to 9.8%,and his fasting blood glucose levels athome have frequently exceeded 10.0mmol/L (180 mg/dL). He has adhered torecommended lifestyle changes. Thepatient is currently on metformin, 1000 mg twice daily, and extended-release glipizide, 20 mg/d. He hashypertension treated with candesartanand hydrochlorothiazide andhyperlipidemia treated withatorvastatin.
Results of physical examination arenormal.
Which is the best next step in therapy?
A. Add insulin glargineB. Add pioglitazoneC. Add sitagliptinD. Double his dose of glipizide
A 68-year-old woman is reevaluatedafter laboratory studies show a fastingplasma glucose level of 6.3 mmol/L (113 mg/dL). She has a maternal familyhistory of type 2 diabetes mellitus.
On physical examination, blood pressureis 142/88 mm Hg and body mass index is29 kg/m2. Other vital signs andexamination findings are normal.
She undergoes an oral glucose tolerancetest, during which her 2-hour plasmaglucose level increases to 7.5 mmol/L(135 mg/dL).
Her hemoglobin A1c level is 5.8%, herlow-density lipoprotein cholesterol level is2.85 mmol/L (110 mg/dL), her high-densitylipoprotein cholesterol level is 1.24 mmol/L(48 mg/dL), and her triglyceride level is1.94 mmol/L (172 mg/dL).
Which is the most appropriate treatmentrecommendation to control her glucoselevel?
A. Acarbose administrationB. Diet and exerciseC. Metformin administrationD. Ramipril administrationE. Rosiglitazone administration
An 83-year-old woman who has hadtype 2 diabetes mellitus for 25 yearscomes to the office for routine care. Shealso has a history of hypertension,dyslipidemia, and coronary arterydisease. Her current antihyperglycemicregimen includes glipizide, pioglitazone,and insulin glargine, 24 U at bedtime.Fasting blood glucose levels at homerange between 6.11 and 8.33 mmol/L(110 and 150 mg/dL), and her mostrecent hemoglobin A1c value was 7.2%.Other medications include metoprolol,lisinopril, and simvastatin.
Physical examination shows a bloodpressure of 108/72 mm Hg, a pulse rateof 76/min, and a respiration rate of 16beats/min. Background retinopathy, a leftfemoral bruit, and mild loss of light-touch sensation in the feet are noted.
Results of laboratory studies show alow-density lipoprotein cholesterol levelof 1.7 mmol/L (65 mg/dL).
Which is the most appropriate treatmentfor this patient?
A. Add exenatide to her regimenB. Add metformin to her regimenC. Continue her current regimenD. Stop pioglitazone treatment
A 48-year-old man comes to the officeafter lunch for a routine physicalexamination. The patient isasymptomatic but overweight, with abody mass index of 29.2 kg/m2.Although he has no pertinent personalmedical history, he has a strong familyhistory of diabetes mellitus. He currentlytakes no medications.
Results of physical examination arenormal.
Results of routine laboratory studiesshow a random plasma glucose level of8.77 mmol/L (158 mg/dL).
Which term best describes his currentglycemic status?
A. Impaired fasting glucoseB. Impaired glucose toleranceC. The metabolic syndromeD. Type 2 diabetes mellitusE. Noncategorizable
An obese 44-year-old woman isevaluated for persistent hyperglycemia.For the past 3 months, she has followeda strict regimen of diet and exercise inan attempt to control her hyperglycemia.Home blood glucose monitoring hasshown preprandial levels between 6.66and 8.88 mmol/L (120 and 160 mg/dL)and occasional postprandial levelsexceeding 11.1 mmol/L (>200 mg/dL).She has a history of hypertension andhyperlipidemia. Current medicationsinclude lisinopril, hydrochlorothiazide,and pravastatin.
Vital signs and physical examinationfindings are normal, except for a bodymass index of 30 kg/m2.
The serum creatinine level is 70.7 µmol/L(0.8 mg/dL), and the urine is negative formicroalbuminuria.
Which is the most appropriate next stepin treatment to improve her glycemiccontrol?
A. Continue the diet and exercise foran additional 3 months
B. Begin exenatideC. Begin glimepirideD. Begin metforminE. Begin pioglitazone
1.
2.
Questions are largely from the ACP’s Medical Knowledge Self-Assessment Program (MKSAP, accessed athttp://www.acponline.org/products_services/mksap/15/?pr31). Go to www.annals.org/intheclinic/
to obtain up to 1.5 CME credits, to view explanations for correct answers, or to purchase the complete MKSAP program.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012