angiogenic markers: molecular targets for personalized medicine in pituitary adenoma
TRANSCRIPT

Angiogenic markers: molecular targets for personalized medicine in pituitary adenoma
Cancer research is probably the most active and rapidly developing area of fundamental research, and cancer pathology probably makes the best case for personalized medicine [1]. The current trend seems to be a search for biomarkers in vari-ous types of cancer (e.g., breast [2], renal [3] and colorectal [4]) to provide the best diagnostic and personalized treatments for patients. Personalized medicine aims to identify needs of the individ-ual patient and biomarkers to predict needs and risks [5], and offers the safest and most effective therapeutic strategy based on the genetic/proteic profile of each subject [6].
Pituitary adenomas are typically slow-growing and histologically benign tumors, but can become clinically destructive, invade adjacent structures and recur after treatment. Unlike many other tumors that become aggressive and appear to depend upon angiogenesis in the process, the angiogenic pattern of pituitary adenomas is a controversial subject in many studies [7–11].
Over the past few decades, much work has been carried out to better elucidate the role of angiogenesis in the growth and development of tumors. The majority of cancers depend on the angiogenic process to survive, with malignant tumors being highly vascularized compared with their normal tissue counterparts. Metastatic potential, tumor aggressiveness, overall prognosis
and response to treatment all correlate with tumor angiogenesis in a variety of solid tumors. The process of angiogenesis is the result of a balance between stimulating and inhibiting factors in tumors, and also in pituitary adenomas. The most important angiogenic players, with various roles in angiogenesis, are VEGF, VEGF recep-tor (VEGFR)-2 and basic FGF (bFGF). Notch cell-surface receptors interacting with various cell membrane ligands (Jagged and DII molecules) are also involved in the angiogenic process [12]. Much attention has been focused on the VEGF family and their receptors that mediate proan-giogenic effects. VEGF signals mainly through VEGFR-2, which is expressed at elevated levels by endothelial cells engaged in angiogenesis.
A variety of angiogenic inhibitors serve as impor-tant system regulators. These include angiostatin, endostatin and thrombospondin-1 [12].
Thus, exploring angiogenic relationships in the pituitary adenoma by looking at serum and tissue protein profiles may help to distinguish between noninvasive and invasive tumors, and determine a personalized course of action for each case.
Since angiogenesis plays an important role in the pathogenesis of tumors, the control of these processes represents a rational approach to treatment [13] and, in view of the previously
Aim: Pituitary adenomas are typically slow-growing and histologically benign tumors that can occasionally behave in a malignant-like manner, invading adjacent structures or recurring after treatment. Using protein ana lysis methods and multiplex xMAP assays, we aimed to find out if these particular types of tumors express angiogenic markers VEGF and basic FGF (bFGF), which are associated with tumor growth and invasiveness, and quantify them in order to establish their usefulness as biomarkers. Materials & methods: We have analysed the expression of angiogenic markers VEGF and bFGF in serum and tissue specimens from 66 pituitary adenomas (43 invasive and 23 noninvasive). For serum analysis, we used xMAP and ELISA, and for tissue analysis, we performed histopathology and immunohistochemistry. Results & conclusion: We measured the serum angiogenic factors in pituitary adenomas. The quantification methods revealed significant differences between pituitary adenoma patients and controls, for both VEGF (212.4 vs 112.5 pg/ml in controls) and bFGF (mean value of 12.6 vs 10.8 pg/ml in controls), and also differentiated between invasive and noninvasive adenomas (p < 0.05). The tissue expression of VEGF and bFGF strongly correlated with their serum level increase. Our findings can be further developed into methods for selection of patients suitable for personalized, antiangiogenic therapy.
KEYWORDS: adenoma n angiogenesis n bFGF n multiplex assay n personalized medicine n pituitary n VEGF
Cristiana Tanase*1, Elena Codrici1, Ionela Daniela Popescu1, Maria Linda Cruceru2, Ana-Maria Enciu1,2, Radu Albulescu1,3, Vasile Ciubotaru4
& Dorel Arsene1
1Victor Babes National Institute of Pathology, 99-101 Spl. Independentei, 050096, Bucharest, Romania 2Carol Davila University of Medicine, Bucharest, Romania 3National Institute for Chemical-Pharmaceutical R&D, Bucharest, Romania 4Bagdasar Arseni Hospital, Neurosurgery Department, Bucharest, Romania *Author for correspondence: [email protected]
539ISSN 1741-054110.2217/PME.13.61 © 2013 Future Medicine Ltd
ReseaRch aRticle ReseaRch aRticle
Personalized Medicine (2013) 10(6), 539–548
part of
For reprint orders, please contact: [email protected]

ReseaRch aRticle Tanase, Codrici, Popescu et al.
mentioned trend towards personalized medicine, a customized therapy schedule.
These angiogenic and growth factors, although intensively studied on tumoral tissue, have been less investigated in the serum of pitu-itary adenomas patients, with only scarce data being published more than 5 years ago [14–16]. The last 3 years have contributed only slightly to general knowledge and VEGF remained the main focus [10,11], while other factors, such as proliferation or apoptosis markers [17], or extra cellular matrix components [18], were concomitantly investigated.
The aim of our study was to evaluate the molecular angiogenic pattern in serum, charac-terized by VEGF and bFGF levels, based on new proteomic methods, such as xMAP multiplex ana lysis, which allow simultaneous biomarker ana lysis. We foresee them as possible therapeutic targets and invasiveness markers, and possibly the core for a wider panel of biomarkers.
Materials & methods �n Samples
Serum and tumoral tissue were collected from 66 patients with pituitary adenomas (27 men and 39 women; mean age: 45 years; range: 21–68 years) from the Neurosurgical Unit, Bagdasar-Arseni Hospital (Bucharest, Roma-nia). Serum samples were also collected from a subset of 15 patients 1 and 4 months after sur-gery; these samples were collected from the cases of prolactin (PRL)-secreting and cases of mixed growth hormone (GH)- and PRL-secreting adenoma. Serum samples from 20 healthy con-trols (12 men and 8 women; mean age: 57 years; range: 25–70 years) were also obtained. Writ-ten informed consent had been obtained upon sample prelevation according to The Helsinki II Declaration, and the study was approved by the Local Ethics Committee. The collection of total peripheral blood from patients and controls has been achieved in vacutainers (Systems, Becton Dickinson, Allschwil, Switzerland) without anti-coagulant. Serum was aliquoted and stored at -80°C until ana lysis. Pituitary adenoma tissue samples were formalin fixed and embedded in paraffin for immunohistochemical ana lysis.
�n Clinical baseline characteristics Pituitary adenomas are classified as: function-ing (considered according to hormonal hyper-secretion associated with a specific syndrome), which produce one or more hormones, and nonfunctioning (lack of a hormone-related syn-drome), depending on their secretory products. Our study included 66 pituitary adenomas, out of which 41 were functioning pituitary adeno-mas – 23 GH-secreting, nine prolactinomas, seven mixed GH- and PRL-secreting, and two adreno corticotrophic hormone (ACTH)-secreting. The majority of mixed GH- and PRL-secreted adenomas and prolactinomas were invasive in the cavernous sinus. Out of 66 pitu-itary adenomas, 43 were invasive – 24 with sinus invasion and 23 noninvasive (Table 1).
�n ELISA & xMAP ana lysis for serum VEGF & bFGFImmunoenzymatic ELISA ana lysis was per-formed with Quantikine® – Human VEGF Immunoassay and Human bFGF Immunoas-say (R&D Systems, MS, USA). Serum level of angiogenic markers was determined according to the manufacturers’ protocol. All samples were assayed in duplicate and the mean values of VEGF or bFGF were taken into account. Optical density was measured at 450 nm on an Anthos Zenyth microplate reader (Biochrom Ltd, Cambridge, UK). Minimum detectable concentration was less than 9.0 pg/ml for VEGF and less than 3.0 pg/ml for bFGF.
The xMAP assay was performed according to the manufacturers’ protocols and the plates were analyzed using Luminex 200 system (Luminex Corp., TX, USA). Angiogenic growth factor lev-els were determined using the Human Cytokine 12-plex Kit (R&D Systems), with 12 analyte-specific bead sets, among them VEGF and bFGF. Multiplex data acquisition and ana lysis were performed using STarStation 2.3 (Applied Cytometry Systems, Sheffield, UK).
�n Histopathology & immunohistochemistryParaffin-embedded tumor tissue was sliced into 7-µm thin sections. The slides were stained with
Table 1. Distribution of cases of pituitary adenomas according to clinical features.
Clinical feature Invasive Noninvasive Total
Functioning 29 12 41
Nonfunctioning 14 11 25
Total 43 23 66
Personalized Medicine (2013) 10 (6)540 future science group

Angiogenic markers as targets for personalized medicine in pituitary adenoma ReseaRch aRticle
Hematoxylin and Eosin and examined on an Olympus BX51 microscope (Olympus Corpo-ration, Tokyo, Japan). The adenoma type and the extent of invasion in the neighboring tis-sue were examined. The microvessel richness within the tumor and adjacent tissues was also assessed in a qualitative manner (rich, poor or absent). Immunohistochemistry was performed on the paraffin-embedded material using the EnVision + Dual Link System Peroxidase kit (Dako, CA, USA), according to the manufac-turer’s instructions. Primary antibodies against the following antigens were used: VEGF (1:50 dilution) and bFGF (1:50 dilution; Santa Cruz Biotechnology, CA, USA) and Ki-67 (1:50 dilu-tion; Dako, Glostrup, Denmark). We assessed which cells expressed the angiogenic markers and with what intensity in the various tumor types. Ki-67 positivity was examined in the most active areas and reported as a percentage.
�n Statistical ana lysisData were expressed as the mean ± standard error of three independent repeats. Differences between the groups were analyzed by unpaired Student’s t-test; p values less than 0.05 were considered statistically significant. The c2-test (×2, p) and Pearson correlation (r, p) were used to explore the association between angiogenic marker expressions. Statistical ana lysis was per-formed using SPSS 19.0 software (SPSS Inc., IL, USA).
Results�n Serum angiogenic markers
The ana lysis of serum angiogenic factors from pituitary adenomas cases was performed by ELISA and by xMAP assays. This revealed sig-nificant differences between patients and control groups, both for VEGF and bFGF levels.
The mean level of serum VEGF, as measured by ELISA assay, was 212.4 pg/ml (range between 144.5 pg/ml and 261.8 pg/ml), which was sig-nificantly higher than controls (112.5 pg/ml; p < 0.01) (Figure 1a). Using xMAP technol-ogy, the median level of soluble VEGF was 220.1 pg/ml for patients compared with con-trols – 115.3 pg/ml (p < 0.01). Statistically sig-nificant differences between patients with inva-sive and noninvasive pituitary adenomas have been recorded (225.8 pg/ml vs 187.3 pg/ml; p < 0.05) (Figure 1b). When comparing patients with invasive pituitary adenomas in cavern-ous sinus with noninvasive pituitary adenomas patients in sinus, statistically significant differ-ences were also observed (233.9 vs 200.1 pg/ml;
p < 0.05). Concerning the functional activity, our results for VEGF did not reveal significant differences between functioning (213.8 pg/ml) and nonfunctioning (209.9 pg/ml) pituitary ade-nomas. In the group of functioning adenomas, the distribution of serum VEGF levels between secretory subclasses were: 230 pg/ml in mixed GH- and PRL-secreting adenomas; 218.3 pg/ml in PRL-secreting adenomas; 207.8 pg/ml in GH-secreting adenomas; and 207.2 pg/ml in ACTH-secreting adenomas.
The serum level of bFGF in patients with pituitary adenomas has varied between 6.3 and 16.3 pg/ml, as measured by ELISA assay, with a mean value of 12.6 pg/ml versus 10.8 pg/ml (controls; p < 0.05; Figure 2a). Using xMAP assay, the median level of soluble bFGF was 12.1 pg/ml for patients compared with controls – 10.2 pg/ml (p < 0.05).
Pituitary adenomas Control
Invasive Noninvasive
300
200
100
0
275
250
225
200
175
150
VE
GF
ser
um
leve
ls (
pg
/ml)
VE
GF
ser
um
leve
ls (
pg
/ml)
Figure 1. Assessement of VEGF serum levels in pituitary adenomas. (A) Serum VEGF assessment in pituitary adenoma patients versus healthy controls and (B) invasive adenoma versus noninvasive adenoma.
www.futuremedicine.com 541future science group

ReseaRch aRticle Tanase, Codrici, Popescu et al.
Statistically significant differences were found between patients with invasive and noninvasive pituitary adenomas (14.7 vs 8.6 pg/ml; p < 0.01) (Figure 2b). When comparing invasive pituitary adenomas in cavernous sinus with noninvasive pituitary adenomas, statistically significant dif-ferences were observed (14.3 vs 11.6 pg/ml; p < 0.05). Our results for bFGF did not reveal statistically significant differences between functioning (13.1 pg/ml) and nonfunctioning (11.8 pg/ml) pituitary adenomas. The distribu-tion of mean bFGF serum levels in functioning adenomas was 13.2 pg/ml in mixed GH- and PRL-secreting adenomas, 15.2 pg/ml in PRL-secreting adenomas, 12.3 pg/ml in GH-secreting adenomas and 12.5 pg/ml in ACTH-secreting adenomas.
Analysis of correlation of serum levels of angiogenic markers (VEGF and bFGF) with clinicopathological features and with Ki-67 pro-liferation index led to the results summarized in Table 2.
Our study revealed a good correlation between VEGF and bFGF (p < 0.05 and r = 0.530). We also found good correlation between invasiveness and each of the two fac-tors: VEGF (p = 0.001) and bFGF (p < 0.001). There was poor correlation between these mark-ers and adenoma functionality; we concluded that both functioning and nonfunctioning ade-nomas may show invasive capacity; an impor-tant aspect to consider when clinical evaluation is performed. There were no differences in the serum levels of VEGF and bFGF that could be correlated to age and sex.
Serum samples from 15 cases of PRL-secreting and mixed GH- and PRL-secreting pituitary adenomas have also been analyzed after surgery. We observed a decreased serum level for VEGF (~15%) and bFGF (~12%) 1 month after surgery, which was maintained 4 months later.
We further evaluated the correlation between Ki-67 proliferation index and angiogenesis through their respective serum markers; we observed good correlations of the two soluble biomarkers with Ki-67 proliferation index (p < 0.05), as well as between VEGF and bFGF (p < 0.05), as detailed in Table 3 and Figure 3. This suggests serum VEGF and bFGF as potential biomarkers for monitoring drug therapy.
�n Tissue angiogenic markersOn immunohistochemical ana lysis, at a quali-tative evaluation, the angiogenesis was signifi-cantly higher in invasive pituitary tumors when compared with noninvasive tumors. VEGF and bFGF were expressed in 85 and 75% of cases in the whole series, respectively. Their tissue expression was found to be strongly cor-related with the serum levels. Both endothelial and tumor cells expressed VEGF and bFGF. In noninvasive adenomas, tumor cells were mostly negative for VEGF, with only scattered microvascular endothelia being faintly stained. On the other hand, in invasive tumors, posi-tive staining was noticed mainly in the tumor cell population, exceeding 50% of tumoral cells (Figure 4).
Immunohistochemical ana lysis also identi-fied heterogeneous distribution of angiogenic markers in the same tumor, with increased staining at the invasion front.
25
20
15
10
0Pituitary adenomas Control
Invasive Noninvasive
5
25
20
15
10
0
5
Bas
ic F
GF
ser
um
leve
ls (
pg
/ml)
Bas
ic F
GF
ser
um
leve
ls (
pg
/ml)
Figure 2. Assessement of basic FGF serum levels in pituitary adenomas. (A) Serum basic FGF assessment in pituitary adenoma patients versus healthy controls and (B) invasive adenoma versus noninvasive adenoma.
Personalized Medicine (2013) 10 (6)542 future science group

Angiogenic markers as targets for personalized medicine in pituitary adenoma ReseaRch aRticle
DiscussionDifferences in the angiogenic pattern of pitu-itary adenomas have yielded highly controver-sial results concerning hormonal phenotypes, size and invasion [10,19–21]. In 2012, Sánchez-Ortiga et al. demonstrated a correlation between angiogenic factors, their receptors and pituitary adenoma invasiveness (e.g., in patients with cav-ernous sinus tumor invasion, these factors had higher levels than in patients with non invasive tumors) [11]. Our results demonstrated that angiogenic factors (VEGF and bFGF) are more elevated in invasive adenomas compared with noninvasive ones.
Although pituitary tumors appear to be quan-titatively less vascular than expected, it remains conceivable that new vessels develop within the tumor. Interestingly, as VEGF and bFGF receptors have been reported to be expressed in both normal pituitary cells [22,23] and adenoma cells [24,25], the two cytokines may exert their mitogenic effects on tumor cells as well. Luque et al. demonstrated on animal models, that two different types of anti-VEGF therapy decreased both vascularity and proliferation [26].
Unlike many other solid tumors, in which angiogenesis seems to drive the malignancy [1–4], in pituitary adenomas there are different opinions regarding the correlation between aggressive-ness, vascularity or angiogenic markers [8,27–29]. In 2012, Perez-Millán [19] confirmed the results of Itoh et al. [20], suggesting that angiogenesis
in tumoral pituitary may occur with changes in the diameter and shape of blood vessels. Discovery of the nonangiogenic mechanisms that drive aggression in many of these tumors could shed light on cancer biology as a whole. In recent years, patients with aggressive pituitary adenomas and carcinomas have also been treated with temozolomide, a new antineoplastic agent addressing an epigenetic mechanism [30]. There-fore, these tumors may be unique and of great interest while studying angiogenesis-dependent and -independent tumors [9].
Invasive adenomas are more vascularized and have a higher expression of angiogenic fac-tors according to Sánchez-Ortiga [11] and de la Torre [31]. Macroprolactinomas have been shown to be significantly more vascular than micro-prolactinomas [7]. This finding fits with the clinical observation that macroprolactinomas may grow to a considerable size because they are invasive adenomas. Invasive macroprolactinomas
Table 2. Correlation between VEGF and basic FGF serum level with clinicopathological features and Ki‑67 index.
Soluble VEGF Soluble bFGF
<190 pg/ml ≥190 pg/ml c² p-value <10 pg/ml ≥10 pg/ml c² p-value
Gender
M 11 16 0.69 0.403 10 17 1.3 0.25
F 12 27 20 19
Age (years)
<60 22 35 2.58 0.107 26 31 0.004 0.94
≥60 1 8 4 5
Ki-67 index
<3% 12 12 3.81 0.05 18 6 13.27 <0.01
≥3% 11 31 12 30
NF 10 15 0.47 0.49 14 11 1.8 0.17
Fn 13 28 16 25
NI 14 9 10.5 0.001 18 5 15.32 <0.001
I 9 34 12 31
bFGF: Basic FGF; F: Female; Fn: Functioning; I: Invasive; M: Male; NF: Nonfunctioning; NI: Noninvasive.
Table 3. Correlation between proliferation and angiogenic markers.
Marker Ki‑67 VEGF Basic FGF
Ki‑67 Pearson correlation 1 0.648 0.657
p‑value – <0.05 <0.05
VEGF Pearson correlation 0.648 1 0.530
p‑value <0.05 – <0.05
Basic FGF Pearson correlation 0.657 0.530 1
p‑value <0.05 <0.05 –
www.futuremedicine.com 543future science group

ReseaRch aRticle Tanase, Codrici, Popescu et al.
have been found to be more vascular than their noninvasive counterparts. This is likely related to the invasiveness of these tumors [31].
Expression of angiogenic markers varies depending on the secretory feature of the ade-noma. For example, as we mentioned above, macroprolactinomas exhibit a higher level of angiogenic markers among functioning adeno-mas. Nonfunctioning and ACTH- and GH-secreting adenomas may display higher levels of angiogenic markers (VEGF, VEGFR-2 and bFGF) than normal tissue [27,32].
In 2010, Cristina et al. reported that prolac-tinomas had higher VEGF protein expression compared with nonfunctioning or ACTH- and GH-secreting adenomas [10]. Perez-Millán in 2012 [19] and Cristina in 2010 [10] revealed the involvement of angiogenesis in pituitary adeno-mas, founding/showing an increased VEGF expression in a cohort of human prolactinomas, and a strong correlation of angiogenic factors in different pituitary adenoma types [10,19]. The results regarding high VEGF expression in pro-lactinomas were also demonstrated in an animal model [33].
Regarding subtype expression of angiogenic factors, Sánchez-Ortiga et al. in 2012 found a trend toward lowered VEGFR expression in functioning versus nonfunctioning pituitary adenomas [11]. The receptor expression did not differ between subtypes or functional status.
Serum levels of VEGF and bFGF showed dif-ferent levels between patient subgroups, accord-ing to secretory pattern of the adenoma: higher levels for PRL-secreting and GH-/PRL-secreting adenomas, compared with nonsecreting adeno-mas. However, the level of statistical signifi-cance is moderate. We found similar patterns of differential expression in tissue.
Recent advances in multiplex protein assays opened the possibility of simultaneous quantifi-cation of markers at high sensitivity and speci-ficity. There are insufficient data regarding the actual levels of VEGF in the serum of adenoma patients [16,34], which has been used thus far as an evolution marker after treatment. There are previous studies that assessed, qualitatively or semi-quantitatively, tumor behavior and the expression of bFGF, a well-characterized angio-genic growth factor and its receptors (e.g., FGF receptors [FGFRs]) [23,35,36].
Elevated levels of angiogenic factors, such as VEGF, have been reported in patients diagnosed with all types of pituitary tumors. The expression of both VEGF and bFGF was seen to correlate with pituitary tumor size and aggression [37].
Our findings regarding serum levels of VEGF and bFGF revealed significant differ-ences between patients and control groups. Moreover, these results also differentiated inva-sive from noninvasive pituitary adenomas. Our results suggest VEGF and bFGF as prognostic markers, with possible further use to personal-ize medicine and tailor treatment. The findings are supported by immunohistochemical results, which were consistent with other reports, show-ing hetero geneity of staining [10]. According to some studies, VEGF correlations with tumor
280
260
240
220
200
180
160
140
280
260
240
220
200
180
160
140
0 2 4 6 8 10
Ki-67 (%)
0 2 4 6 8 10
Ki-67 (%)
VE
GF
(p
g/m
l)
20
15
10
5
bF
GF
(p
g/m
l)
bFGF (pg/ml)
VE
GF
(p
g/m
l)
6 10 14 18
Figure 3. Correlation between proliferation and angiogenic markers. (A) Correlation between VEGF and Ki‑67. (B) Correlation between bFGF and Ki‑67. (C) Correlation between VEGF and bFGF. bFGF: Basic FGF.
Personalized Medicine (2013) 10 (6)544 future science group
Angiogenic markers as targets for personalized medicine in pituitary adenoma ReseaRch aRticle
invasiveness and proliferation are inconsistent; this suggests that VEGF may not directly con-tribute to tumoral invasion, but may regulate pathways that lead to increased tumor volume or mediate invasiveness [28,38]. This is supported by the observation that VEGF expression is not strictly associated with endothelium and vessels, but is also expressed by adenoma cells as well [38]; and our results also illustrate this.
The lack of consistency in VEGF inhibition response could be a consequence of an ‘intracrine’ mechanism of action, mediated by intracellular-confined receptors [39,40], or significant increase of endostatin, a potent angiogenesis inhibitor found to be coelevated with VEGF in most patients with pituitary adenomas [14]. This increase may be accountable for the findings of diminished effect of antiangiogenic drugs in these tumors. Many studies have also shown a good correlation between bFGF expression and clinicopathologi-cal parameters, including pituitary tumor diam-eter, invasiveness and patient outcome [15,41–43]. The role of FGFRs in cancer signaling is reviewed in Holzmann et al. [44]; but little is known about their involvement in pituitary adenoma. How-ever, they have different roles in pituitary tumori-genesis; FGFR4 shows protumorigenic activity [45], whereas FGFR2 is involved in apoptotic signaling [46].
Although pituitary neoplasms often behave as benign, nonmalignant entities, the potential of serum VEGF and bFGF as markers of aggres-sive tumor behavior becomes increasingly more useful, similar to its already-stated utility in other solid tumors.
Moreover, we found that serum levels of both VEGF and bFGF were correlated with the Ki-67 proliferation index, suggesting that thera-peutically addressing angiogenic processes (via VEGF/bFGF signaling pathways) may result in a further decrease of tumor cell proliferation.
VEGF and bFGF may constitute the core of a larger cytokine panel for tumor behavior. Comparative ana lysis of the data obtained by the two assays for serum proteins (ELISA and multiplex-xMAP) showed a very good level of concordance.
�n Antiangiogenic therapy in pituitary tumorsThe correlation found between serum levels of VEGF, bFGF and Ki-67 index suggest that a subgroup of pituitary adenoma patients may ben-efit from antiangiogenic-targeted therapy. The increased use of antiangiogenic drugs for cancer treatment has emerged from decades of extensive
basic and clinical research. The clinical benefits of such drugs, however, are relatively modest. Improvements are likely to come from a more thorough understanding of the molecular and cel-lular mechanisms governing tumor angiogenesis, and the response to antiangiogenic therapies [37]. A number of recent advances promise to bring about such improvements. These include new findings in the VEGF and the VEGFR family, discovery of the Notch–Dll4 signaling pathway in tumor angiogenesis, identification of the mecha-nisms of resistance to antiangiogenic drugs and observations that suggest a role of angiogenesis in the survival and growth of cancer stem cells.
Many of these discoveries suggest strategies for improving the clinical benefits of antiangiogenic therapy. These strategies include the development of better preclinical models in order to study the biology of tumor angiogenesis and antiangiogenic therapies. Treatments such as sorafenib or suni-tinib, which inhibit cellular signaling by target-ing the receptor tyrosine kinases of VEGF, may have a role in the treatment of aggressive pituitary adenomas [11].
Such improvements will also be critical in the use of long-term antiangiogenic therapy in the adjuvant setting in patients with early-stage
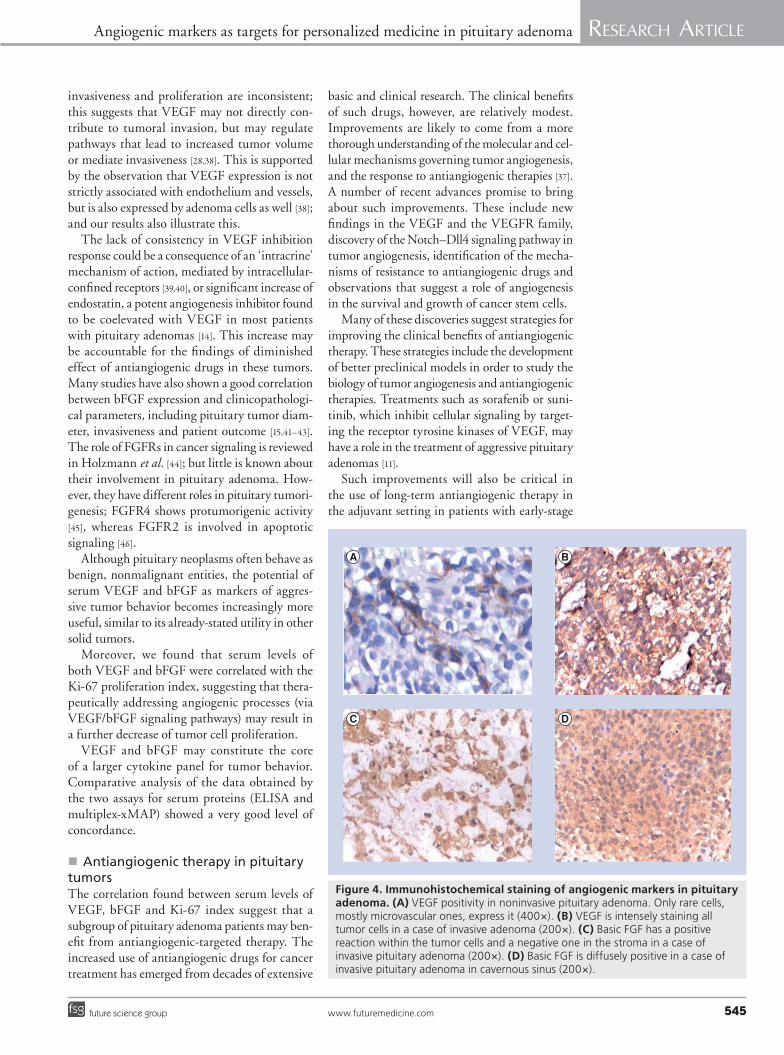
Figure 4. Immunohistochemical staining of angiogenic markers in pituitary adenoma. (A) VEGF positivity in noninvasive pituitary adenoma. Only rare cells, mostly microvascular ones, express it (400×). (B) VEGF is intensely staining all tumor cells in a case of invasive adenoma (200×). (C) Basic FGF has a positive reaction within the tumor cells and a negative one in the stroma in a case of invasive pituitary adenoma (200×). (D) Basic FGF is diffusely positive in a case of invasive pituitary adenoma in cavernous sinus (200×).
www.futuremedicine.com 545future science group

ReseaRch aRticle Tanase, Codrici, Popescu et al.
ReferencesPapers of special note have been highlighted as:n of interestnn of considerable interest
1 Shiekh FA. Personalized nanomedicine: future medicine for cancer treatment. Int. J. Nanomedicine 8, 201–202 (2013).
2 Patani N, Martin LA, Dowsett M. Biomarkers for the clinical management of breast cancer: international perspective. Int. J. Cancer 133, 1–13 (2012).
3 Craven RA, Vasudev NS, Banks RE. Proteomics and the search for biomarkers for renal cancer. Clin. Biochem. 46, 456–465 (2012).
4 de Cuba EM, Kwakman R, van Egmond M et al. Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer: future possibilities for personalised treatment by use of biomarkers. Virchows Arch. 461, 231–243 (2012).
5 Koomen JM, Haura EB, Bepler G et al. Proteomic contributions to personalized cancer care. Mol. Cell. Proteomics 7, 1780–1794 (2008).
nn� Presents the contribution of proteomics to the prevention and cure of personalized cancer.
6 González-Beltran A, Tagger B, Finkelstein A. Federated ontology-based queries over cancer data. BMC Bioinformatics 13 (Suppl. 1), S9 (2012).
7 Turner HE, Nagy Z, Gatter KC, Esiri MM, Harris AL, Wass JA. Angiogenesis in pituitary adenomas – relationship to endocrine function, treatment and outcome. J. Endocrinol. 165, 475–481 (2000).
Executive summary
� Personalized medicine is the current trend in cancer research and its aim is to identify those patients that would best benefit from newly developed therapies.
� Proteomic ana lysis is a useful tool for biomarker medicine and allows quantification of putative serum molecules that may act as disease predictors or personalized treatment indicators.
� Angiogenic markers have been associated with high invasiveness/poor prognosis in almost every type of malignancy.
� Some pituitary adenomas have malignant‑like behavior and we have demonstrated that this particular subgroup associates with statistically higher levels of serum VEGF and bFGF, compared with the noninvasive group.
� Both functioning and nonfunctioning adenomas may show invasive capacity, an aspect that should be taken into consideration when clinical evaluation is performed.
� Although considered benign tumors, pituitary adenoma patients display increased serum levels of angiogenic markers, which correlate with invasiveness.
disease. The magnitude and diversity of targets for antiangiogenic approaches suggest numerous possibilities for antiangiogenic drug combina-tions that should be much more effective than monotherapy of malignant and benign tumors.
ConclusionAnalysis of angiogenic markers may provide useful insights into angiogenesis and its role in determining phenotype and behavior of pituitary tumors.
Our results demonstrate a tendency of invasive pituitary tumors to be more vascularized than noninvasive ones, and as a result of newly devel-oped antiangiogenic therapies, a particular sub-group of patients may benefit from personalized anti-VEGF therapy.
Furthermore, serum angiogenic mark-ers – VEGF and bFGF – may prove useful tools for prognosis and prediction of response to therapy.
These markers may develop into targets for antiangiogenic therapy in patients with invasive pituitary adenomas, which are noncompliant to total surgical resection or in patients with recur-rences. The added knowledge would hopefully lead to newly emerged synergistic drug combina-tions. Personalized medicine will further select those patients that would surely benefit from molecular antiangiogenic therapy.
Considering the potential of simultaneous detection and quantitation of multiple analytes, xMAP provides a robust tool to investigate and monitor biomarkers.
AcknowledgementsThe authors would like to thank AI Neagu and L Necula for technical assistance, AI Nita and A Petrescu for assis-tance with statistical ana lysis, and I Radu for technical and linguistic assistance.
Financial & competing interests disclosureThis work was partially supported by Grant POS CCE 685-152/2010 and POS CCE SMIS number 549/12024. The authors have no other relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research The authors state that they have obtained appropriate insti tutional review board approval or have followed the princi ples outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addi-tion, for investi gations involving human subjects, informed consent has been obtained from the participants involved.
Personalized Medicine (2013) 10 (6)546 future science group

Angiogenic markers as targets for personalized medicine in pituitary adenoma ReseaRch aRticleReseaRch aRticle
8 Takada K, Yamada S, Teramoto A. Correlation between tumor vascularity and clinical findings in patients with pituitary adenomas. Endocr. Pathol. 15(2), 131–139 (2004).
9 Cohen AB, Lessell S. Angiogenesis and pituitary tumors. Semin. Ophthalmol. 24(3), 185–189 (2009).
10 Cristina C, Perez-Millán MI, Luque G et al. VEGF and CD31 association in pituitary adenomas. Endocr. Pathol. 21(3), 154–160 (2010).
11 Sánchez-Ortiga R, Sánchez-Tejada L, Moreno-Perez O, Riesgo P, Niveiro M, Picó Alfonso AM. Over-expression of vascular endothelial growth factor in pituitary adenomas is associated with extrasellar growth and recurrence. Pituitary doi:10.1007/s11102-012-0434-4 (2012) (Epub ahead of print).
12 Kerbel RS. Tumor angiogenesis. N. Engl. J. Med. 358(19), 2039–2049 (2008).
n� Presents molecular events and research advances in tumor angiogenesis.
13 Ciccarelli A, Daly AF, Beckers A. The epidemiology of prolactinomas. Pituitary 8(1), 3–6 (2005).
14 Gruszka A, Kunert-Radek J, Pawlikowski M, Stepien H. Serum endostatin levels are elevated and correlate with serum vascular endothelial growth factor levels in patients with pituitary adenomas. Pituitary 8(2), 163–168 (2005).
15 Komorowski J, Jankewicz J, Stepien H. Vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF) and soluble interleukin-2 receptor (sIL-2R) concentrations in peripheral blood as markers of pituitary tumours. Cytobios 101(398), 151–159 (2000).
n� Reports angiogenic markers as diagnostic markers for pituitary tumors.
16 Nagai Y, Ando H, Nohara E, Yamashita H, Takamura T, Kobayashi K. Plasma levels of vascular endothelial growth factor in patients with acromegaly. Horm. Metab. Res. 32(8), 326–329 (2000).
17 Yarman S, Kurtulmus N, Canbolat A, Bayindir C, Bilgic B, Ince N. Expression of, p53 and vascular endothelial growth factor (VEGF) concomitantly in growth hormone-secreting pituitary adenomas; which one has a role in tumor behavior? Neuro. Endocrinol. Lett. 31(6), 823–828 (2010).
18 Cornelius A, Cortet-Rudelli C, Assaker R et al. Endothelial expression of endocan is strongly associated with tumor progression in pituitary adenoma. Brain Pathol. 22(6), 757–764 (2012).
19 Perez-Millán MI, Berner SI, Luque GM et al. Enhanced nestin expression and small blood vessels in human pituitary adenomas.
Pituitary doi:10.1007/s11102-012-0421-9 (2012) (Epub ahead of print).
20 Itoh J, Serizawa A, Kawai K, Ishii Y, Teramoto A, Osamura RY. Vascular networks and endothelial cells in the rat experimental pituitary glands and in the human pituitary adenomas. Microsc. Res. Tech. 60(2), 231–235 (2003).
21 Turner HE, Harris AL, Melmed S, Wass JA. Angiogenesis in endocrine tumors. Endocr. Rev. 24(5), 600–632 (2003).
22 Vidal S, Lloyd RV, Moya L, Scheithauer BW, Kovacs K. Expression and distribution of vascular endothelial growth factor receptor Flk-1 in the rat pituitary. J. Histochem. Cytochem. 50(4), 533–540 (2002).
23 Fukui S, Otani N, Nawashiro H et al. Subcellular localization of basic fibroblast growth factor and fibroblast growth factor receptor 1 in pituitary adenomas. Brain Tumor Pathol. 19(1), 23–29 (2002).
24 Miyajima K, Takekoshi S, Itoh J, Kakimoto K, Miyakoshi T, Osamura RY. Inhibitory effects of anti-VEGF antibody on the growth and angiogenesis of estrogen-induced pituitary prolactinoma in Fischer 344 rats: animal model of VEGF-targeted therapy for human endocrine tumors. Acta Histochem. Cytochem. 43(2), 33–44 (2010).
25 Horiguchi H, Jin L, Ruebel KH, Scheithauer BW, Lloyd RV. Regulation of VEGF-A, VEGFR-I, thrombospondin-1, -2, and -3 expression in a human pituitary cell line (HP75) by TGFbeta1, bFGF, and EGF. Endocrine 24(2), 141–146 (2004).
26 Luque GM, Perez-Millán MI, Ornstein AM, Cristina C, Becu-Villalobos D. Inhibitory effects of antivascular endothelial growth factor strategies in experimental dopamine-resistant prolactinomas. J. Pharmacol. Exp. Ther. 337(3), 766–774 (2011).
27 Niveiro M, Aranda FI, Peiro G, Alenda C, Pico A. Immunohistochemical ana lysis of tumor angiogenic factors in human pituitary adenomas. Hum. Pathol. 36(10), 1090–1095 (2005).
28 Fukui S, Nawashiro H, Otani N et al. Vascular endothelial growth factor expression in pituitary adenomas. Acta Neurochir. Suppl. 86, 519–521 (2003).
n� An interesting assessement of VEGF expression in pituitary adenomas.
29 Fukui S, Otani N, Nawashiro H et al. The association of the expression of vascular endothelial growth factor with the cystic component and haemorrhage in pituitary adenoma. J. Clin. Neurosci. 10(3), 320–324 (2003).
30 Moshkin O, Syro LV, Scheithauer BW et al. Aggressive silent corticotroph adenoma
progressing to pituitary carcinoma: the role of temozolomide therapy. Hormones (Athens) 10(2), 162–167 (2011).
31 de la Torre NG, Wass JA, Turner HE. Morphologic changes and molecular regulation of angiogenesis in pituitary adenomas. Front. Horm. Res. 32, 133–145 (2004).
32 McCabe CJ, Boelaert K, Tannahill LA et al. Vascular endothelial growth factor, its receptor KDR/Flk-1, and pituitary tumor transforming gene in pituitary tumors. J. Clin. Endocrinol. Metab. 87(9), 4238–4244 (2002).
33 Cristina C, Diaz-Torga G, Baldi A et al. Increased pituitary vascular endothelial growth factor-a in dopaminergic D2 receptor knockout female mice. Endocrinol. 146(7), 2952–2962 (2005).
34 Paisley AN, O’Callaghan CJ, Lewandowski KC et al. Reductions of circulating matrix metalloproteinase 2 and vascular endothelial growth factor levels after treatment with pegvisomant in subjects with acromegaly. J. Clin. Endocrinol. Metab. 91(11), 4635–4640 (2006).
35 Qian ZR, Sano T, Asa SL et al. Cytoplasmic expression of fibroblast growth factor receptor-4 in human pituitary adenomas: relation to tumor type, size, proliferation, and invasiveness. J. Clin. Endocrinol. Metab. 89(4), 1904–1911 (2004).
36 McCabe CJ, Khaira JS, Boelaert K et al. Expression of pituitary tumour transforming gene (PTTG) and fibroblast growth factor-2 (FGF-2) in human pituitary adenomas: relationships to clinical tumour behaviour. Clin. Endocrinol. 58(2), 141–150 (2003).
37 Tanase CP, Neagu M, Albulescu R. Key signaling molecules in pituitary tumors. Expert Rev. Mol. Diagn. 9(8), 859–877 (2009).
38 Salehi F, Agur A, Scheithauer BW, Kovacs K, Lloyd RV, Cusimano M. Biomarkers of pituitary neoplasms: a review (Part II). Neurosurgery 67(6), 1790–1798 (2010).
39 Hanahan D. Signaling vascular morphogenesis and maintenance. Science 277(5322), 48–50 (1997).
40 Oliner J, Min H, Leal J et al. Suppression of angiogenesis and tumor growth by selective inhibition of angiopoietin-2. Cancer Cell 6(5), 507–516 (2004).
41 Ezzat S, Smyth HS, Ramyar L, Asa SL. Heterogenous in vivo and in vitro expression of basic fibroblast growth factor by human pituitary adenomas. J. Clin. Endocrinol. Metab. 80(3), 878–884 (1995).
n� First report of bFGF in human pituitary adenomas.
www.futuremedicine.com 547future science group

ReseaRch aRticle Tanase, Codrici, Popescu et al.ReseaRch aRticle
42 Asa SL, Ramyar L, Murphy PR, Li AW, Ezzat S. The endogenous fibroblast growth factor-2 antisense gene product regulates pituitary cell growth and hormone production. Mol. Endocrinol. 15(4), 589–599 (2001).
43 Fukui S, Otani N, Nawashiro H et al. Nuclear accumulation of basic fibroblast growth factor as a predictor for the recurrence
of pituitary adenomas. J. Neurooncol. 57(3), 221–229 (2002).
44 Holzmann K, Grunt T, Heinzle C et al. Alternative splicing of fibroblast growth factor receptor IgIII loops in cancer. J. Nucleic Acids 2012, 950508 (2012).
45 Ezzat S, Zheng L, Zhu XF, Wu GE, Asa SL. Targeted expression of a human pituitary
tumor-derived isoform of FGF receptor-4 recapitulates pituitary tumorigenesis. J. Clin. Invest. 109(1), 69–78 (2002).
46 Zhu X, Lee K, Asa SL, Ezzat S. Epigenetic silencing through DNA and histone methylation of fibroblast growth factor receptor 2 in neoplastic pituitary cells. Am. J. Pathol. 170(5), 1618–1628 (2007).
Personalized Medicine (2013) 10 (6)548 future science group