anemia - osu center for continuing medical education - anemia of chronic... · whose quality of...
TRANSCRIPT

www.npjournal.org The Journal for Nurse Practitioners - JNP 261
ANEMIAOF CHRONICDISEASE IN THEELDERLY
ABSTRACTMany experienced cliniciansfeel comfortable with thediagnosis and treatment ofanemia. However, the anemiaof chronic diseases so preva-lent in the elderly may repre-sent a diagnostic challenge.New treatment strategies arenow available for patientswhose quality of life isadversely affected by thisproblem that is commonlyignored.
Keywords: anemia of chronicdisease, low iron production,normocytic normochromicanemia
Maren Mayhew
toid arthritis (RA), and Crohn disease, among others.Other diseases implicated in ACD are liver disease (alco-holic cirrhosis), heart failure, chronic obstructive pul-monary disease, and diabetes. Multiple trauma can alsocause ACD.The list of diseases or conditions associatedwith ACD continues to grow as new research uncoversthe relations.
PREVALENCE AND SIGNIFICANCEAnemia as a general condition is common in the eld-
erly.2 The prevalence can reach 44% in men older than85.3 Prevalence has been difficult to quantify in the past,partly because of limitations of the various research
The anemia of chronic disease (ACD) is a commonproblem in elderly patients and may represent a diagnos-tic challenge even for the experienced nurse practition-er.Although subtle, anemia may have a serious effect onthe quality of life of the elderly patient.This article dis-cusses common anemias in the elderly, with an emphasison ACD and its treatment (Box 1).
The most common cause of anemia in the elderly isACD, which was recognized as a diagnostic entity in1962.1 Three causes are generally agreed on: cancer andcancer treatment, inflammation or infection, and patientswith HIV who are taking zidovudine.The inflammationor infectious disease category includes malaria, rheuma-
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 261

April 2006262 The Journal for Nurse Practitioners - JNP
studies.The following findings have been confirmed byseveral studies2:
• The prevalence of anemia varies among differentgroups.
• Hospitalized patients have the highest rate of ane-mia; high rates are also found in nursing homes.
• Anemia is more prevalent in elderly men thanwomen.
• The prevalence increases with age.• An increased prevalence occurs in patients with
Alzheimer disease.• Increased mortality is found in anemic patients.Anemia has significant adverse effects on the patient’s
clinical, functional, and economic status. However, studieshave not been done to quantify the effect of anemia onthe elderly patient.2 The main symptom of anemia isfatigue, and fatigue clearly can have a serious effect onquality of life.4
TYPES OF ANEMIASAnemia is classified either by pathophysiology or cell size(mean cell volume [MCV], equates to size) (Box 2).5 Tounderstand anemia in the elderly, it is necessary to addressboth pathophysiology to understand cause and cell size asa method of diagnosis.These classifications have beencombined in this article to facilitate discussion.
CAUSEErythropoiesis as a process normally declines duringaging.This makes it difficult to sort normal aging fromthe effect of chronic disease.Also, it is often difficult todetermine the cause of an anemia in the elderly. Studiesestimating the cause of anemia in the elderly find that,for many patients, no cause can be confirmed.2 In manycases the cause is multifactorial. Most of the diseases list-ed under ACD have other mechanisms for causing ane-mia in addition to the ACD.
The etiology of ACD is not fully understood. Itappears to be caused by inflammatory cytokines such asinterleukin, tumor necrosis factor, and interferon alfaand beta.6 These cytokines play three roles.The firstrole is that red blood cell survival is slightly decreased.This leads to anemia.The second role is a depressedresponse to the anemia.The body produces erythro-poiein, but the amount is low compared to what a nor-mal body would make with the same severity of ane-mia.The bone marrow fails to increase the production
of red blood cells sufficient to compensate for the ane-mia.The third role is that inflammation causes iron tobe retained in the reticuloendothelial system ratherthan being released to the RBCs developing in themarrow. Inflammation causes a direct inhibition of thisprocess.The patient has iron but is unable to use it, sothere is no iron deficiency per se.
Chronic Renal FailureThe main cause of anemia in patients with CRF isinsufficient production of erythropoietin by the diseasedkidneys.7 This is an absolute decrease in productionbecause of the kidney damage, not a relative decrease asin ACD.This process leads to decreased RBC produc-tion, and the resulting anemia is more severe than thatseen in ACD.
Oral iron (generic)Intravenous iron sucrose (Venofer)Epoetin (Procrit, Epogen)Darbepoetin (Aranesp)Zidovudine (Retrovir)
Box 1. Medications Discussed in This
Article
Microcytic HypochromicIron deficiency
MacrocyticFolate deficiencyVitamin B12 deficiency
Normocytic NormochromicIncreased loss or destruction of blood
Acute blood lossHemolytic disorders
Decreased red blood cell (RBC) production Aplastic anemia, bone marrow infiltrationEarly iron deficiencyChronic renal failure (CRF)Endocrine deficiency states (hypothyroidism)ACD
Adapted from Brill JR, Baumgardner DJ. Normocytic anemia. AmFam Physician. 2000;62(10):2255-2264.
Box 2. Classification of Anemia in the
Elderly, Organized by Cell Size and
Pathology
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 262
www.npjournal.org The Journal for Nurse Practitioners - JNP 263
Gastrointestinal Blood Loss and Nutritional DeficitIron deficiency in the elderly is often caused by acute orchronic gastrointestinal (GI) blood loss. Folate and vitaminB12 deficiencies are also seen in the elderly because ofinadequate intake or absorption. It may be symptoms ofthese other deficiency problems that bring the ACD to theattention of the clinician.
DIAGNOSIS OF ANEMIA
Signs and SymptomsMost anemias are discovered on routine laboratory tests.The patient often does not complain of or evidence anysymptoms. Other disease states may be aggravated orfound concurrent with anemia.
The most common symptom of anemia is fatigue.Although some might assume that the most importantsymptom to manage in palliative medicine is pain,fatigue is one of the top two symptoms (along withanorexia) for distress in patients who are terminallyill.8 In fact, fatigue is a problem in 75% to 90% ofpatients with terminal illness. It is described as tired-ness, a general lack of energy not relieved by rest,diminished mental capacity, and weakness. It may beso severe it causes profound difficulty in performingactivities of daily living. Fatigue contributes todecreased exercise tolerance, frailty, immobility, anddepression. Fatigue is a common complaint in the eld-erly and it is hard to know when it is significant.Researchers suggest it is underdiagnosed and under-treated.9 Many diseases in the elderly can cause fatiguedirectly and may also produce anemia, which can in
turn increase the fatigue.This makes it extremely dif-ficult to diagnose the true cause of the fatigue. A goodexample of this is the deconditioning the patientexperiences as a result of cancer, which is common inaddition to anemia.
It is essential for the clinician to determine what partanemia might play in contributing to fatigue.Assess theseverity of the fatigue by talking to the patient to deter-mine the effect on the patient’s quality of life.Thedegree of patient distress and disability will help deter-mine how aggressive the clinician should be in the treat-ment of the anemia.
Research suggests that anemia found in associationwith heart failure is correlated with increased mortality.Approximately 17% of patients with heart failure haveanemia, 60% of which may be found to be ACD.Anemiacontributes to the disease progression of heart failure,and the anemia can exacerbate ischemic heart disease orcause high-output failure.10
Differential DiagnosisThe diagnosis of ACD is one made by exclusion, and
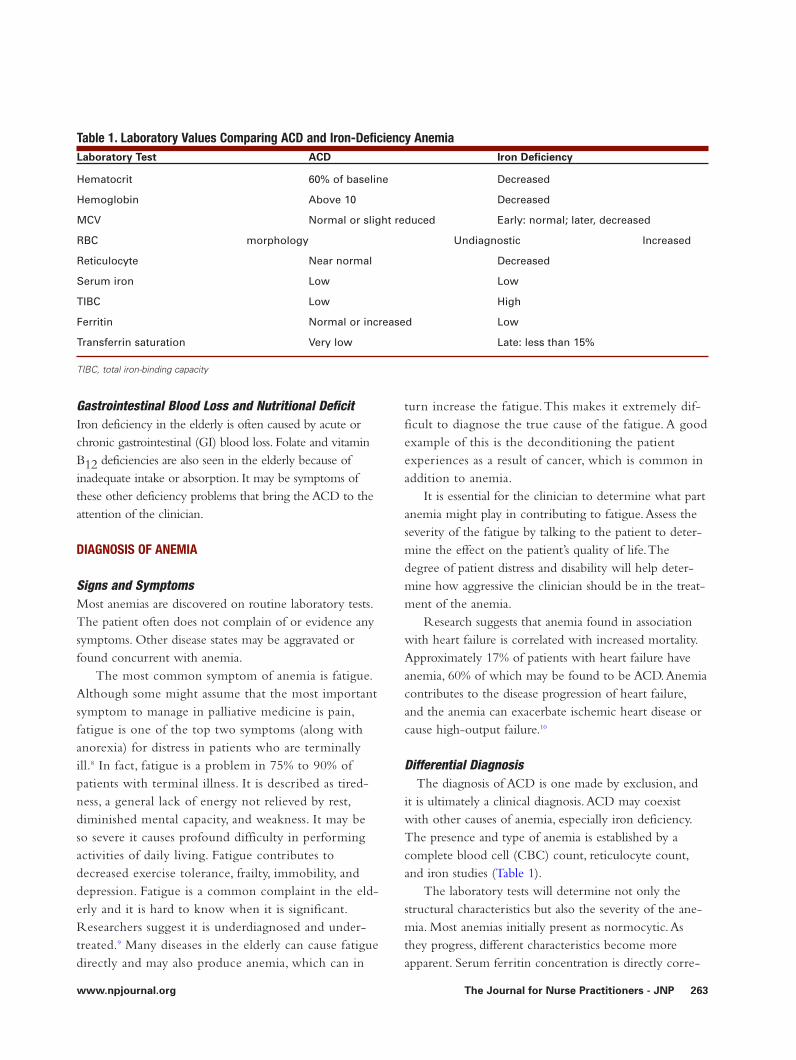
it is ultimately a clinical diagnosis.ACD may coexistwith other causes of anemia, especially iron deficiency.The presence and type of anemia is established by acomplete blood cell (CBC) count, reticulocyte count,and iron studies (Table 1).
The laboratory tests will determine not only thestructural characteristics but also the severity of the ane-mia. Most anemias initially present as normocytic.Asthey progress, different characteristics become moreapparent. Serum ferritin concentration is directly corre-
Table 1. Laboratory Values Comparing ACD and Iron-Deficiency AnemiaLaboratory Test ACD Iron Deficiency
Hematocrit 60% of baseline Decreased
Hemoglobin Above 10 Decreased
MCV Normal or slight reduced Early: normal; later, decreased
RBC morphology Undiagnostic Increased variability
Reticulocyte Near normal Decreased
Serum iron Low Low
TIBC Low High
Ferritin Normal or increased Low
Transferrin saturation Very low Late: less than 15%
TIBC, total iron-binding capacity
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 263

April 2006264 The Journal for Nurse Practitioners - JNP
lated to the reticuloendothelial iron stores. Reducedserum ferritin means low iron stores; this is the onlycause of low serum ferritin.Tests will document thatthe iron stores in ACD are normal. Another test thatshould be obtained is the transferrin saturation.Thetransferrin saturation is the ratio of serum iron toTIBC and will be low in both ACE and iron-defi-ciency anemia.
Other causes of anemia should be excluded beforeACD can be diagnosed.Thus, the clinician mustsearch for CRF, iron deficiency and blood loss, vita-min B12 and folate deficiencies, and other problems asdictated by the laboratory results.The diagnosis ofiron-deficiency anemia is confirmed by bone marrowexamination.This test is expensive and painful andrequires patient cooperation; thus, it is often not feasi-ble in the elderly.1
To summarize, ACD is a mild normocytic nor-mochromic anemia characterized by low reticulocyteindex, low serum iron, and low TIBC, with normal orincreased ferritin, in a patient with a systemic (aninflammatory component) disease.
TREATMENT
General PrinciplesIt is tempting to base treatment of ACD solely on lab-oratory values. However, other factors must be consid-ered.Treatment must be based on the cause of the ane-
mia, and, if the anemia is severe or causing symptoms,it must be treated and not ignored. Otherwise, it isusually not necessary to treat ACD.Treatment in thatcase would consist of optimal control of the underly-ing cause (Box 3).
Commonly, patients with ACD have a hemoglobinlevel of around 30 and a hematocrit of about 10 andmanage well.The anemia has developed slowly, and thepatient has adjusted to it. Patients with heart failure havea decreased ability to tolerate anemia.They may becomesymptomatic even with hemoglobin or hematocrit at ahigher level. Some patients with ACD complain offatigue. Others decrease their activity level to alleviatethe fatigue and do not complain.
However, these changes, even if small, may lead to adecreased quality of life.The patients are less able to carefor themselves and do what they want to do.They needa higher level of care, sometimes necessitating placementin a nursing home or care center.The clinician may con-sider physical therapy to improve their endurance if theyare able to tolerate it. Other patients need energy con-servation techniques, such as doing the most difficultactivities at a time when they are feeling their best andtaking frequent rest periods. Consider other therapy ifthese methods are not sufficient.
Transfusions can be useful for immediate treatmentin severe, symptomatic anemia.The drawbacks to the useof transfusions include allergic reactions, limited bloodsupply, and risk of disease transmission.The patient alsomust go to a facility to receive the transfusion, thusincreasing the cost, work, and expense.
Iron-deficiency anemias can be treated with oraliron.The usual recommended dose is between 150and 200 mg elemental iron daily. Higher doses areneeded when iron is poorly absorbed.The recom-mended dietary intake of iron for older persons is 10mg/day. Adverse effects of iron therapy are abdominaldiscomfort, nausea, vomiting, and constipation.Theseadverse reactions can lead to decreased food intake,bowel impaction, and other problems, includingunnecessary GI examinations, and can lead todecreased compliance with iron therapy. One studyshowed significantly lower incidence of adverse effectsand effective treatment of iron deficiency with the useof doses as low as 15 mg instead of 150 mg.11 Thisstudy is particularly impressive in that the subjectswere older than 80. An additional factor to consider is
A. Monitor for fatigue in the patient B. Monitor for anemia through routine CBC countsC. If a patient complains of fatigue, do a thorough
assessment to determine the cause of the fatigue D. If the patient has anemia (confirmed through labo-
ratory work) 1. Evaluate the laboratory findings 2. Perform additional tests as needed to determine
the cause of the anemia E.To treat
1.Treat any medical condition that is amenable totreatment
2.Treat any other cause for the anemia F. If the anemia does not improve
1. Evaluate the effect the anemia is having on thepatient’s quality of life
2. If it is significant, consider whether treatmentwith epoetin might help
Box 3. Clinical Practice Implication
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 264

www.npjournal.org The Journal for Nurse Practitioners - JNP 265
that with oral iron therapy bowel movements turnblack, masking any GI bleeding that might be present.
Intravenous iron sucrose (Venofer) is indicated fortreatment of iron-deficiency anemia in patients undergo-ing chronic hemodialysis who are receiving supplementalerythropoietin therapy.12 It is also used for iron-deficien-cy anemia in patients who cannot tolerate oral iron. It isgiven intravenously by infusion or by slow injection overa period of at least 15 minutes. Slow infusion ratesdecrease the risk of hypotension.The dose is 5 mL ironsucrose (100 mg elemental iron). Common adverse reac-tions include allergy, hypotension, cramps or leg cramps,nausea, headache, vomiting, and diarrhea.
Epoetin Alfa TreatmentEpoetin is an additional therapeutic option that was
shown to be effective in treating many anemias ofdecreased RBC production.The use of this drug hasbeen studied most extensively in the treatment of anemiaof CRF, whereby it is generally effective if the patient isadequately dialyzed.13
The effectiveness of epoetin therapy is less well docu-mented in ACD. One study found that there was usually agood patient response to epoetin used in treating ACD
caused by RA,AIDS, malignancies, and inflammatorybowel disease.14 In cancer, the response rate has been 40%to 80%, depending on the study.6 In RA, most patients haveshown a positive response to epoetin.15
Epoetin is being tried for patients with heart failureand anemia. Darbepoetin was shown to increase thehemoglobin level and to improve symptoms. However, adecrease in mortality in these patients with heart failurewas not documented.16
An interesting new use of epoetin is for the pre-vention of blood transfusions during surgery.Thescarcity of blood for transfusions has lead to a searchfor alternatives for patients undergoing elective sur-gery. Although donation of autologous blood is thepreferred alterative, elderly patients are often unable tomake new RBCs quickly enough. Epoetin has beenshown to facilitate the production of autologous bloodthat can be donated before elective surgery.17 Patientswho will benefit most are patients with a hematocritof 33 to 39 whose blood loss during surgery is expect-ed to be 1000 and 3000 mL.
Epoetin is relatively expensive as a treatment.18 Itcosts about $300 per dose of 20,000 units, whichwould total about $1,200 per month, given weekly.
Table 2. Dosage and Administration of EpoetinDisease When to Use Starting Dose Increase Dose When Maximum Dose Decrease or Stop
CRF — 50-100 8 wk, CBC 300 U/kg HCT 36% or
U/kg not increased increase of more
TIW by 5-6 points than 4 points in
2-wk period
Cancer or Serum 150 — — —
cancer erythropoietin U/kg
therapy level <200 TIW
mU/mL
HIV On zidovudine, 100 In 8 wk, if 300 U/kg NA
serum U/kg response not
erythropoietin TIW satisfactory
level <500 m
mU/kg
Surgery — 100 — 600 U/kg —U/kg
weekly
Information from drug package insert. TIW, three times week.
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 265

April 2006266 The Journal for Nurse Practitioners - JNP
Epoetin therapy may be reimbursed under Medicare PartB, providing strict requirements are followed.The compa-nies who deliver the medication and fill out the reim-bursement forms for the medication are a good source forinformation about reimbursement requirements in yourarea. See Table 2 for specific dosage and administrationinformation in anemias caused by other diseases and Box4 for additional information about the use of epoetin.
Darbepoetin alfa (Aranesp)20 is another medicationthat is closely related to erythropoietin. It is indicated foranemia, secondary to renal failure, and anemia secondaryto cancer chemotherapy. Off-label indication for this
product is anemia secondary to malignancy.Absorptionof this product is slow with the peak concentrationoccurring at 24 to 72 hours in patients with CRF and71 to 123 in patients with cancer.
SummaryAnemia is a common finding in the elderly. One of thefrequent problems responsible for this condition is ACD,which is caused by decreased RBC production. It is gen-erally not treated. However, if the anemia is causing signif-icant fatigue, which is interfering with the patient’s qualityof life, treatment with epoetin may be effective. Epoetin
IndicationsAnemia as a result of renal failure; anemia as a result of can-cer chemotherapy; surgery, reduce need for blood transfu-sions during surgery; anemia as a result of zidovudine thera-py; anemia, symptomatic
Off-label IndicationsAnemia (due to hepatitis C management); anemia (due tomalignancy); anemia (due to myelodysplastic syndromes);anemia (due to donation prophylaxis); anemia (due to post-partum blood loss); anemia (due to rheumatic disease); ane-mia of prematurity; anemia, sickle cell; Castleman disease;Gaucher disease; hemoglobinuria, paroxysmal nocturnal
ContraindicationsUncontrolled hypertension; known hypersensitivity tomammalian cell–derived products; known hypersensitivityto albumin (human)
WarningsThrombotic events and increased mortality: In patientsreceiving hemodialysis with cardiac disease, epoetin increasesthe risk of mortality because of thrombotic events. Inwomen with metastatic carcinoma of the breast, onchemotherapy, epoetin showed increased thrombotic events.
Pure red cell aplasia (PRCA) was reported, predomi-nantly in patients with CRF.
Albumin: Epoetin contains albumin; it carries an extremelyremote risk of transmission of viral disease and Creutzfeldt-Jakob disease. No cases have been identified.
Patients with CRF: Hypertension, blood pressure may riseduring epoetin therapy. Hypertensive encephalopathy andseizures have been observed.Thrombotic events, patients mayrequire increased anticoagulation to prevent clotting of theartificial kidney.
Patients with HIV treated with zidovudine:Treatment hasnot been linked to exacerbation of hypertension, seizures,and thrombotic events.
Adverse ReactionsThe adverse reactions depend on the reason the medication isbeing used. It is generally well tolerated. Fever, diarrhea, nau-sea, edema, and local reaction are the most likely reactions.
Laboratory MonitoringMonitor the hemoglobin weekly. CBC counts should be per-formed “regularly” according to the package insert. Beforetreatment, the patient’s transferrin saturation should be at least20%, and the serum ferritin should be elevated. Benefits aregenerally apparent after 4 to 8 weeks but may be seen as earlyas 2 weeks.
Dosage and AdministrationEpoetin is given subcutaneously. Epoetin dosing wasstudied most extensively in CRF and cancer. Epoetin wasinjected three times a week in the earlier studies. It isused weekly in patients before surgery.Weekly use isbecoming more common.19 One dosage used for ACDcaused by cancer is 20,000 units weekly. Epoetin reachespeak plasma levels in 5 to 24 hours after subcutaneousinjection.The long-lasting form of erythropoietin, darbe-poetin, has been used monthly.
Increases in dose should be made no more frequentlythan once a month. If the hemoglobin level is increasingand approaching 12 g/dL, the dose should be reduced byapproximately 25%. Hold the epoetin if the hemoglobinlevel continues to increase, until the hemoglobin levelbegins to decrease. Restart at a dose 25% below the pre-vious dose. If the hemoglobin level increases by morethan 1 g/dL in 2 weeks, decrease dose by 25%. Once thetarget hemoglobin level is achieved, the dose should betitrated to the lowest dose necessary to maintain thehemoglobin value.
Box 4. Epoetin Alfa Treatment
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 266

www.npjournal.org The Journal for Nurse Practitioners - JNP 267
does not have a specific indication by the Food and DrugAdministration listed for use in ACD, but many cliniciansare beginning to use it successfully to improve the qualityof life in elderly patients with ACD.
References
1. Fitzsimons EJ, Brock JH. The anaemia of chronic disease. BMJ.2001;322(7290):811-812.
2. Beghe C, Wilson A, Ershler WB. Prevalence and outcomes of anemia ingeriatrics: a systematic review of the literature. Am J Med. 2004;116(7A):3S-10S.
3. Ania BJ, Suman VJ, Fairbanks VF, Melton LJ III. Prevalence of anemia inmedical practice: community versus referral patients. Mayo Clin Proc.1994;69(8):808-809.
4. Gabrilove J. Anemia and the elderly: clinical considerations. Best Pract ResClin Haematol. 2005;18(3):417-422.
5. Brill JR, Baumgardner DJ. Normocytic anemia. Am Fam Physician.2000;62(10):2255-2264.
6. Gardner LB, Benz EJ. Anemia of chronic diseases. In: Hoffman. Hematology:basic principles and practice. 4th ed. Philadelphia, Pa: Churchill Livingstone;2005.
7. National Kidney Foundation. NKF-K/DOQI clinical practice guidelines foranemia of chronic kidney disease: update 2000. Am J Kidney Dis.2001;37(suppl 1):S182-S238.
8. Ross RD, Alexander CS. Management of common symptoms in terminally illpatients: part I. Fatigue, anorexia, cachexia, nausea, and vomiting. Am FamPhysician 2001;64(5):807-814.
9. Cella D, Passik S, Peterman C, Jacobsen PS, Breitbart W. Progress towardguidelines for the management of fatigue. Oncology. 1998:12(11A):369-377.
10. Givertz MM, Colucci, Braunwald E. Clinical aspects of heart failure;pulmonary edema, high-output failure. In: Zipes DP, Libby P, Bonow RO,Braunwald E, eds. Braunwald’s heart disease: a textbook of cardiovascularmedicine. 7th ed. Philadelphia, Pa: Saunders; 2005.
11. Rimon E, Kagansky N, Kagansky M, et al. Are we giving too much iron? Low-dose therapy is effective in octogenarians. Am J Med. 2005;118:1142-1147.
12. PI Iron Sucrose (Venofer). Mosby’s Drug Consult 2006. 16th ed. St Louis, Mo:Mosby; 2006.
13. Pendse S, Singh AK. Complications of chronic kidney disease: anemia,mineral metabolism, and cardiovascular disease. Med Clin N Am.2005;89(3):549-561.
14. Krantz SB. Erythropoietin and the anaemia of chronic disease. Nephrol DialTransplant. 1995;10(suppl l2):10-17.
15. Pincus T, Olsen NJ, Wolfe F, et al. Multicenter study of recombinant humanerythropoietin in corrections of anemia in rheumatoid arthritis. Am J Med.1990;89(2):161-168.
16. Cleland JG, Sullivan JT, Ball S, et al. Once-monthly administration ofdarbepoetin alfa for the treatment of patients with chronic heart failure andanemia: a pharmacokinetic and pharmacodynamic investigation. JCardiovasc Pharmacol. 2005;46(2):155-161.
17. Goodnough LT, Terri TG, Andriole GL. Erythropoietin therapy. N Engl J Med.1997;336(13):933-938.
18. Epoetin [package insert]. Thousand Oaks, Calif: Amgen.19. Erythropoietin (Procrit, Epogen) revisited. Med Lett. 2001;43(W1104B):40-41.20. Darbepoetin [package insert]. Thousand Oaks, Calif: Amgen.
Maren Mayhew, MS,ANP, GNP, CRNP, has worked inoffice, nursing home, and home care settings in the Washington,DC, area for more than 25 years. She has also served as afaculty member in several NP programs. She has coedited fivebooks for nurse practitioners, including A PharmacologyTextbook for Primary Care Providers. In accordance withnational ethical guidelines, she has disclosed that she has nofinancial relationships with business or industry. She may bereached at [email protected].
1555-4155/06/$ see front matter© 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.nurpra.2006.03.002
Sign up to receive a FREE subscription, plusFREE access to the onlineversion of the journal.*
Visit
www.npjournal.org
today!
* npjournal.org is open to all visitors
through December 31, 2005. Request
your free subscription today to ensure
continued access.
261-267_YJNP176_Mayhew_CP.qxd 4/5/06 2:46 PM Page 267