anatomy of the lens gross anatomy the lens is an intraocular avascular biconvex disc of gelatinous...
TRANSCRIPT

ANATOMY OF THE LENSANATOMY OF THE LENSGrossGross AnatomyAnatomyThe lens is an intraocular avascular biconvex disc of The lens is an intraocular avascular biconvex disc of gelatinous transparent substance: contained within an gelatinous transparent substance: contained within an elastic transparent capsule. It alters its shape according elastic transparent capsule. It alters its shape according to theI requirements of the accommodative process. It to theI requirements of the accommodative process. It is suspended between the iris anteriorly and the is suspended between the iris anteriorly and the vitreous body posteriorly. The space between the iris vitreous body posteriorly. The space between the iris and the lens is called the and the lens is called the posterioer chamber. posterioer chamber. Posteriorly, the lens is separated from the vitreous face Posteriorly, the lens is separated from the vitreous face by a narrow by a narrow retro-lental fluidretro-lental fluid space.space.The lens is maintained in position within the eye by a The lens is maintained in position within the eye by a special suspensory ligament called the special suspensory ligament called the zonule, zonule, which is which is attached to the ciliary body and to the lens capsule. attached to the ciliary body and to the lens capsule. The The suspensory ligament suspensory ligament forms a delicate membrane forms a delicate membrane covering the inner surface of the ciliary body and its covering the inner surface of the ciliary body and its processes. It then passes on to the lens dividing into processes. It then passes on to the lens dividing into three layers which are attached to the anterior capsule, three layers which are attached to the anterior capsule, the equator and the posterior capsule of the lens.the equator and the posterior capsule of the lens.

ANATOMYANATOMY

The lens The lens measures measures about 9 mm. diameter and 3 - 4 about 9 mm. diameter and 3 - 4 mm. in thickness. At birth, the lens weighs about 60 mg mm. in thickness. At birth, the lens weighs about 60 mg which increases slowly in a linear progression to a which increases slowly in a linear progression to a weight of approximate 250 mg at the age of 70 years. weight of approximate 250 mg at the age of 70 years. Its anterior surface is less convex than the posterior. Its anterior surface is less convex than the posterior. The The radius of curvature radius of curvature of the anterior surface is10 of the anterior surface is10 mm. while that of the posterior surface is 6 mm. The mm. while that of the posterior surface is 6 mm. The refractive index refractive index of the lens cortex is 1.38 and that the of the lens cortex is 1.38 and that the nucleus is 1.40. The nucleus is 1.40. The refractive refractive (coverging) (coverging) power power of of the lens is approximaelythe lens is approximaely16 - 22 dioptres when inside the eye but is 16 - 22 dioptres when inside the eye but is approximately 60 - 70 dioptres when in air.approximately 60 - 70 dioptres when in air. Microscopic AnatomyMicroscopic AnatomyHistologically, the lens consists essentially of a mass of Histologically, the lens consists essentially of a mass of transparent cells, called the transparent cells, called the lens fibres, lens fibres, enclosed in an enclosed in an elastic membrane, called the elastic membrane, called the lens capsule. lens capsule. The lens is The lens is composed of three distint portions :composed of three distint portions :

The Lens CapsuleThe Lens Capsule..—This is a very elastic —This is a very elastic transparent non-cellular membrane which completely transparent non-cellular membrane which completely surrounds the lens. Its thickness is not uniform, being surrounds the lens. Its thickness is not uniform, being thickest near the equator and thinnest at the anterior thickest near the equator and thinnest at the anterior and posterior poles of the lens.and posterior poles of the lens.The Lens EpitheliumThe Lens Epithelium..—The anterior epithelium —The anterior epithelium consists of a single layer of cubical cells covering the consists of a single layer of cubical cells covering the anterior surface of the lens substance and lying anterior surface of the lens substance and lying between the latter and the capsule. There is no between the latter and the capsule. There is no corresponding posterior epithelium.corresponding posterior epithelium.

The Lens Fibres and Cement The Lens Fibres and Cement SubstanceSubstance..—The bulk of the lens is —The bulk of the lens is composed of successive laminae of fibres, but composed of successive laminae of fibres, but between these there is some kind of cement between these there is some kind of cement substance having the same refractive index as substance having the same refractive index as the fibres and gluing them together. The lens the fibres and gluing them together. The lens substance comprises a cortex and a nucleus.substance comprises a cortex and a nucleus.The The lens cortexlens cortex consists of concentric consists of concentric lamellae of long hexagonal transparent fibres lamellae of long hexagonal transparent fibres which are arranged in structure of an onion. which are arranged in structure of an onion. The The nucleusnucleus consists of the compressed consists of the compressed central portions of lens cortex which gradually central portions of lens cortex which gradually undergoes a process of sclerosis and becomes undergoes a process of sclerosis and becomes optically denser and harder than the cortical optically denser and harder than the cortical fibres.fibres.

The Suspensory Ligament of the The Suspensory Ligament of the LensLens (the Zonule). (the Zonule). —The zonule is a —The zonule is a band-shaped gel-structure stretching band-shaped gel-structure stretching from the ciliary body to the periphery from the ciliary body to the periphery of the lens. The zonule is of the lens. The zonule is inserted inserted into the zonular lamellae in a belt into the zonular lamellae in a belt running concentrically round the running concentrically round the equator of the lens. Its equator of the lens. Its anterior anterior surface surface runs straight from the lens runs straight from the lens to meet the ciliary processes just to meet the ciliary processes just behind their apices. Its behind their apices. Its posterior posterior surface surface is bow-shaped curving along is bow-shaped curving along the inner surface of the bodythe inner surface of the body

Functions of the LensFunctions of the LensStatic Dioptric FunctionStatic Dioptric Function. . —Together with the —Together with the cornea, the lens forms the eye's dioptric cornea, the lens forms the eye's dioptric system, which to converge parallel light rays system, which to converge parallel light rays from a distant object to a focus on the from a distant object to a focus on the photoreceptor layer of the retina.photoreceptor layer of the retina.Dynamic Dioptric FunctionDynamic Dioptric Function.—.—The refractive The refractive power of the lens varies with the distance of the power of the lens varies with the distance of the object of regard so that a perfect image is object of regard so that a perfect image is formed on the retina at all distances. This formed on the retina at all distances. This dynamic alteration in the refractivedynamic alteration in the refractivepower of the lens to see clearly at all distances, power of the lens to see clearly at all distances, known as known as accommodation, accommodation, is achieved by a is achieved by a change in the curvature of the lens, mainly its change in the curvature of the lens, mainly its anterior surface.anterior surface.

Protective FunctionProtective Function.—.—The lens also The lens also protects the retina by absorbing the ultra protects the retina by absorbing the ultra violet rays.violet rays.
CHEMISTRY OF THE LENSCHEMISTRY OF THE LENSThe adult lens contains approximately 65% The adult lens contains approximately 65% water and 34% proteins. The remaining 1 % is water and 34% proteins. The remaining 1 % is made up of inorganic compounds. Lens made up of inorganic compounds. Lens dehydration is maintained by an active sodium dehydration is maintained by an active sodium pump in the epithelium.pump in the epithelium.
ACCOMMODATIONACCOMMODATIONAccommodation is the act of altering the dioptric power Accommodation is the act of altering the dioptric power of the lens in order to keep the image in sharp focus on of the lens in order to keep the image in sharp focus on the retina when the gaze is directed from far to near the retina when the gaze is directed from far to near objects.objects.This is accomplished by means of increasing the This is accomplished by means of increasing the curvature of the lens surfaces particularly the anterior curvature of the lens surfaces particularly the anterior surface, and thus changing its refractive power. The surface, and thus changing its refractive power. The degree of accommodation varies with the distance of degree of accommodation varies with the distance of the object of regard. Accommodation is most active in the object of regard. Accommodation is most active in children and decreases gradually throughout life. This is children and decreases gradually throughout life. This is probably due to the fact that as age advances the probably due to the fact that as age advances the ciliary muscle atrophies aod lens becomes less elastic, ciliary muscle atrophies aod lens becomes less elastic, and thus changes its shape with difficulty.and thus changes its shape with difficulty.Mechanism of AccommodationMechanism of AccommodationAccommodation comprises two mechanisms, namely, Accommodation comprises two mechanisms, namely, an an active contraction of the ciliary muscle, active contraction of the ciliary muscle, followed by followed by passive change of the shape of the lens.passive change of the shape of the lens.


CATARACTCATARACTGeneral ConsiderationsGeneral ConsiderationsA cataract means cloudiness or opacity of the lens A cataract means cloudiness or opacity of the lens substance or its capsule. This definition includes substance or its capsule. This definition includes vacuoles, water clefts, dense areas reflecting or vacuoles, water clefts, dense areas reflecting or refracting light, and punctuate microscopic spots in the refracting light, and punctuate microscopic spots in the lens substance. Cataracts most commonly develop as lens substance. Cataracts most commonly develop as part of the normal part of the normal aging process aging process and are called and are called senile senile cataracts, cataracts, but sometimes they are but sometimes they are developmental. developmental. Cataracts may also be Cataracts may also be acquired acquired as a result of ocular as a result of ocular pathology, metabolic defects, systemic disease, toxins pathology, metabolic defects, systemic disease, toxins or trauma. Depending on the location and the extent of or trauma. Depending on the location and the extent of lenticular opacity, light rays passing through the lens lenticular opacity, light rays passing through the lens may be blocked or scattered, resulting in a blurred may be blocked or scattered, resulting in a blurred retinal image or a bothersome glare.retinal image or a bothersome glare.

Diagnostic Methods for CataracDiagnostic Methods for CataracttExamination of the Visual Acuity.Examination of the Visual Acuity.—Distant —Distant and near and near vision with the appropriate glasses would be tested. vision with the appropriate glasses would be tested. Nuclear cataracts affect vision more than peripheral Nuclear cataracts affect vision more than peripheral cortical cataracts.cortical cataracts.Examination of the Pupillary ResponsesExamination of the Pupillary Responses. . —The —The direct and consensual pupillary responses are usually direct and consensual pupillary responses are usually affected to a slight extent by the lens opacities.affected to a slight extent by the lens opacities.Examination of the Lens by Direct Focal Examination of the Lens by Direct Focal Illumination. Illumination. —Lens opacities appear in the pupillary —Lens opacities appear in the pupillary area as grey or white areas against a black background.area as grey or white areas against a black background.Slit-lamp BiomicroscopySlit-lamp Biomicroscopy.—The .—The extent, density, type extent, density, type and location of the cataract can accurately determined and location of the cataract can accurately determined by slit-lamp biomicroscopy.by slit-lamp biomicroscopy.
Examination of the Red Reflex.Examination of the Red Reflex. Examination of the Iris Shadow by Oblique Focal Examination of the Iris Shadow by Oblique Focal Illumination.Illumination.——
Refraction and Retinoscopy.Refraction and Retinoscopy. ——Retinoscopy often confirms that lens Retinoscopy often confirms that lens opacities are opacities are the the cause of a patient's poor cause of a patient's poor vision. vision. A-Scan and B-Scan Ultrasonography.A-Scan and B-Scan Ultrasonography.

CLASSIFICATION OF CATARACTCLASSIFICATION OF CATARACT
DEVELOPMENTALDEVELOPMENTAL
SENILESENILE
ACQUIREDACQUIRED::TraumaticTraumatic
Complicating Ocular PathologyComplicating Ocular Pathology
Associating Systemic DiseaseAssociating Systemic Disease

Classification of CataractsClassification of Cataracts
By Etiology By Etiology Senile or age-relatedSenile or age-related
Congenital and juvenileCongenital and juvenileTraumatic.Traumatic.

Classification of Cataracts.Classification of Cataracts.(Cataract defined as any lens opacity)(Cataract defined as any lens opacity)
By Anatomic LocationBy Anatomic Location
CorticalCortical
NuclearNuclear
Posterior sub capsularPosterior sub capsular
MixedMixed

classification of cataract according to morphology
1. Sub capsular• Anterior• Posterior
2. Nuclear 3. Cortical4. Christmas tree

Classification of CataractsClassification of Cataracts
By Etiology By Etiology Senile or age-relatedSenile or age-related
Congenital and juvenileCongenital and juvenileTraumatic.Traumatic.

Classification of CataractsClassification of Cataracts Associated with intraocular diseasesAssociated with intraocular diseases::
uveitis /inflammationuveitis /inflammation glaucomaglaucoma retinal detachment retinal degeneration (retinitis retinal detachment retinal degeneration (retinitis
pigmentosa, gyrate atrophy)pigmentosa, gyrate atrophy) persistent hyperplasic primary vitreous, aniridia, persistent hyperplasic primary vitreous, aniridia,
Peters' anomaly, sclerocornea.Peters' anomaly, sclerocornea. micro-ophthalmus, Norris's disease, micro-ophthalmus, Norris's disease, retinoblastoma,retinoblastoma, retrolental fibroplasias, high myopia,retrolental fibroplasias, high myopia, retinal anoxia (Burger's disease, Takayasu's retinal anoxia (Burger's disease, Takayasu's
arthritis),arthritis), anterior segment necrosisanterior segment necrosis

Classification of CataractsClassification of Cataracts Associated with systemic diseases: Associated with systemic diseases:
Metabolic disorders: diabetes; galactosemiaMetabolic disorders: diabetes; galactosemia; ; hypoparathyroidism/hypocalcemia; Lowe's, Albright's, hypoparathyroidism/hypocalcemia; Lowe's, Albright's, Wilson's, Fabry's, and Refsum's diseases; homocystinuriaWilson's, Fabry's, and Refsum's diseases; homocystinuria
Renal disease: Lowe's and Alport's diseasesRenal disease: Lowe's and Alport's diseases
Skin diseaseSkin disease: congenital ectodermal dysplasia;Werner's : congenital ectodermal dysplasia;Werner's and Rothmund-Thomson syndromes; a topic dermatitisand Rothmund-Thomson syndromes; a topic dermatitis
Connective tissue/skeletal disordersConnective tissue/skeletal disorders: myotonic : myotonic dystrophy; Conradi's and Marfan's syndromes; bone dystrophy; Conradi's and Marfan's syndromes; bone dysplasias; dislocated lensesdysplasias; dislocated lenses
Central nervous systemCentral nervous system: Marinesco-Sjögren's : Marinesco-Sjögren's syndrome, bilateral acoustic neuroma syndrome, bilateral acoustic neuroma (neurofibromatosis type 2)(neurofibromatosis type 2)

Classification of CataractsClassification of Cataracts
Caused by noxious agentsCaused by noxious agents: : Ionizing radiation: x-ray, ultraviolet Ionizing radiation: x-ray, ultraviolet
rays, infrared rays, microwavesrays, infrared rays, microwaves
Pharmaceuticals: steroids, Pharmaceuticals: steroids, naphthalene, triparanol, lovastatin, naphthalene, triparanol, lovastatin, ouabain, ergot, chlorpromazine, ouabain, ergot, chlorpromazine, thallium (acetate and sulfate), thallium (acetate and sulfate), dinitrophenol, dimethyl sulfoxide, dinitrophenol, dimethyl sulfoxide, psoralens, miotics, psoralens, miotics, paradichlorobenzene, sodium seleniteparadichlorobenzene, sodium selenite

Classification according to maturity
Immature Mature
Hypermature Morgagnian


Mature cataract
DEVELOPMENTAL CATARACTDEVELOPMENTAL CATARACTCongenital Congenital cataracts are present at birth or within 3 cataracts are present at birth or within 3 months after birth. months after birth. Developmental Developmental cataracts are not cataracts are not evident at birth but may form during infancy or evident at birth but may form during infancy or adolescence. They normally remain stationary adolescence. They normally remain stationary throughout life.throughout life.Etiology.Etiology.—The cause may be either one of the following :—The cause may be either one of the following :1. A 1. A hereditary defect, hereditary defect, usually of the dominant type, which is usually of the dominant type, which is transmitted by the fathertransmitted by the fatheror mother. It is due to an anomaly in the chromosomal pattern.or mother. It is due to an anomaly in the chromosomal pattern.2. A 2. A maternal nutritional deficiency maternal nutritional deficiency during the process of during the process of development leading to adevelopment leading to alowered blood calcium. It may be accompanied by signs of rickets.lowered blood calcium. It may be accompanied by signs of rickets.3. A 3. A maternal infection maternal infection during the early months of pregnancy, during the early months of pregnancy, e.g. e.g. rubella.rubella.4. A 4. A deficient oxygenation, e.g. deficient oxygenation, e.g. due to repeated placental due to repeated placental haemorrhages.haemorrhages.5. A 5. A familial incidence, familial incidence, which is dependent upon a genetic which is dependent upon a genetic influence or some maternal abnormality. influence or some maternal abnormality. SymptomsSymptoms.—The child is usually brought for examination because the .—The child is usually brought for examination because the parents may notice that the pupil is white or that the child holds things parents may notice that the pupil is white or that the child holds things too close to his eyes.too close to his eyes.

S S ENILE CATARACTENILE CATARACTSenile cataract denotes an age-related bilateral Senile cataract denotes an age-related bilateral progressive opacification of the lens affecting progressive opacification of the lens affecting elderly people not suffering from local or elderly people not suffering from local or systemic disease. It commonly affects persons systemic disease. It commonly affects persons over 50 years of age and is due to a process of over 50 years of age and is due to a process of aging and degeneration. Sometimes, there aging and degeneration. Sometimes, there appears to be a familial tendency to cataract appears to be a familial tendency to cataract formation in which case the lens opacity may formation in which case the lens opacity may occur at an earlier age in successive occur at an earlier age in successive generations. It is controversial whether the generations. It is controversial whether the cataract is genetically determined or cataract is genetically determined or environmentally influenced.Ccataract is usually environmentally influenced.Ccataract is usually bilateral, but often one side is more advanced bilateral, but often one side is more advanced than the other. than the other.
Clinical PictureClinical PictureSymptoms.Symptoms.——The patients may complain of one or The patients may complain of one or more of the following symptcmore of the following symptcGradual Diminution of Vision without Pain or Discharge.Gradual Diminution of Vision without Pain or Discharge. Uniocular Diplopia or Polyopia. Uniocular Diplopia or Polyopia. Myopia. Myopia. Positive Scotomata. Positive Scotomata. Glare. Glare. Altered Colour PerceptionAltered Colour Perception
Signs.Signs.—Senile cataract is essentially a process in —Senile cataract is essentially a process in which the transparency of is impaired by changes which the transparency of is impaired by changes either in the cortex or in the nucleus. The principal sign either in the cortex or in the nucleus. The principal sign is a whitish opacity within the pupillary area, the eye is a whitish opacity within the pupillary area, the eye appearing otherwise quiti A white pupil appearing otherwise quiti A white pupil (leucocoria) (leucocoria) is is usually seen as a late manifestation of cataract.usually seen as a late manifestation of cataract.

Intumescent CataractIntumescent Cataract.— .— Sometimes, Sometimes, during the immature stage of cataract during the immature stage of cataract formation, the lens absorbs an increasing formation, the lens absorbs an increasing amount of fluid from the aqueous and becomes amount of fluid from the aqueous and becomes swollen, swollen, it it intumescent. The swollen lens intumescent. The swollen lens pushes the iris forwards, reduces the depth of pushes the iris forwards, reduces the depth of the anterior chamber and may block the angle, the anterior chamber and may block the angle, hence there is a tendency to secondary hence there is a tendency to secondary glaucoma.glaucoma. The Mature Stage.The Mature Stage.—A cataract is called —A cataract is called mature, mature, when complete opacification of the when complete opacification of the fibres extends to the capsule.fibres extends to the capsule.

Complications of Complications of hypermature cataract:hypermature cataract:
11) ) Secondary glaucomaSecondary glaucoma : : phakomorphic glaucoma : The swollen cataract may cause a phakomorphic glaucoma : The swollen cataract may cause a
pupillary block and give rise to glaucomapupillary block and give rise to glaucoma Phakolytic glaucoma: The lens matter might leak out into the Phakolytic glaucoma: The lens matter might leak out into the
AC. Here it gets engulfed by macrophages which then go and AC. Here it gets engulfed by macrophages which then go and block the trabecular meshwork.block the trabecular meshwork.
2) 2) UveitisUveitis;; Phakoanaphylactic uveitis: The lens matter leaks out and Phakoanaphylactic uveitis: The lens matter leaks out and
sensitises the uveal tissue. phakoanaphylactic uveitis occurs.sensitises the uveal tissue. phakoanaphylactic uveitis occurs.3) 3) SubluxationSubluxation and dislocation of lens : Along with and dislocation of lens : Along with
the hyper maturity , there is associated degeneration of the the hyper maturity , there is associated degeneration of the zonules. This may give rise to subluxation and dislocation of zonules. This may give rise to subluxation and dislocation of lens.lens.
4) 4) RaptureRapture of lensof lens:: A swollen Morgagnian cataract may A swollen Morgagnian cataract may burst releasing milky fluid into the AC. This will produce burst releasing milky fluid into the AC. This will produce glaucoma and uveitis.glaucoma and uveitis.
Therefore lens extraction should be done in the immature or Therefore lens extraction should be done in the immature or mature stage not only to improve vision but to prevent mature stage not only to improve vision but to prevent complications of hypermature cataract. complications of hypermature cataract.
TREATMENT OF SENILE CATARACTTREATMENT OF SENILE CATARACTThThe only treatment of senile cataract is by e only treatment of senile cataract is by surgical removal of the opaque lens. The surgical removal of the opaque lens. The action should be undertaken on the worse eye action should be undertaken on the worse eye as soon as the vision in the better eye less as soon as the vision in the better eye less than 6/18, or when the patient's ability to work than 6/18, or when the patient's ability to work is threatened. It is no longer necessary to wait is threatened. It is no longer necessary to wait until the cataract is mature. With modern until the cataract is mature. With modern surgical techniques, an immature presents no surgical techniques, an immature presents no difficulty in its removal. However, if the cataract difficulty in its removal. However, if the cataract shows signs of maturity, it should be extracted shows signs of maturity, it should be extracted even if the vision in the better eye is still even if the vision in the better eye is still perfect.perfect.

COMPLICATED CATARACTS ASSOCIATED WITH COMPLICATED CATARACTS ASSOCIATED WITH SYSTEMIC DISEASE:SYSTEMIC DISEASE:
Cataracts Associated with Metabolic Cataracts Associated with Metabolic Disturbances Disturbances (Metabolic Cataracts): (Metabolic Cataracts): (a) (a) Diabetic Diabetic cataract.cataract. (b) (b) Galactosemic cataract.Galactosemic cataract.(c) (c) Hypocalccemic cataract.Hypocalccemic cataract. (d) (d) Hypothyroidic cataract.Hypothyroidic cataract.(e) (e) Myotonic cataract.Myotonic cataract. (f) (f) Deficiency cataract.Deficiency cataract.
Cataracts Associated with Skin Diseases:Cataracts Associated with Skin Diseases:Atopic dermatitis Atopic dermatitis (Eczema).(Eczema).Poikiloderma atrophicans Poikiloderma atrophicans (Rothmund Syndrome).(Rothmund Syndrome).Sclero-Poikiloderma Sclero-Poikiloderma (Werner Syndrome).(Werner Syndrome).Anhidrotic ectodermal dysplasia.Anhidrotic ectodermal dysplasia.

Extracapsular cataract extraction
1. Anterior capsulotomy
2. Completion of incision
3. Expression of nucleus
4. Cortical cleanup
6. Polishing of posterior capsule, if appropriate
5. Care not to aspirate posterior capsule accidentally
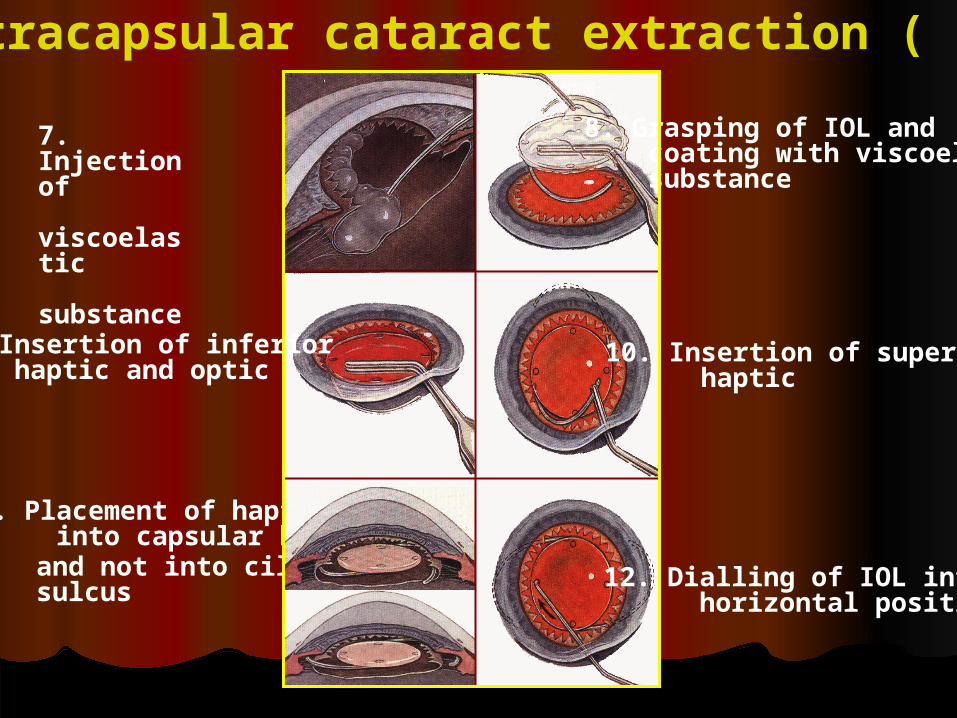
8. Grasping of IOL and coating with viscoelastic substance
Extracapsular cataract extraction ( cont. )
7. Injection of viscoelastic substance
9. Insertion of inferior haptic and optic
11. Placement of haptics into capsular bag
10. Insertion of superior haptic
12. Dialling of IOL into horizontal position
and not into ciliary sulcus

PhacoemulsificationPhacoemulsification During During
phacoemulsification, phacoemulsification, phaco for short, the phaco for short, the surgeon makes a small surgeon makes a small incision, where the cornea incision, where the cornea meets the conjunctivameets the conjunctiva
The surgeon then uses The surgeon then uses the probe, which vibrates the probe, which vibrates with ultrasound waves, to with ultrasound waves, to break up (emulsify) the break up (emulsify) the cataract and suction out cataract and suction out the fragmentsthe fragments

Two things happen Two things happen during cataract surgery: during cataract surgery: the clouded lens is the clouded lens is
removedremoved a clear artificial lens is a clear artificial lens is
implanted to replace the implanted to replace the original clouded lens original clouded lens
This lens implant is made This lens implant is made of PMMA,plastic, acrylic of PMMA,plastic, acrylic or silicone and becomes or silicone and becomes a permanent part of the a permanent part of the eyeeye
Reference:Reference:
1. Clinical ophthalmology1. Clinical ophthalmology
ByBy
Jack KanskiJack Kanski
2. Lecture notes in ophthalmology2. Lecture notes in ophthalmology
3. Parson’s diseases of the eye3. Parson’s diseases of the eye