anatomic and hemodynamic correlations in carotid...
TRANSCRIPT

Anatomic and HemodynamicCorrelations in Carotid Artery StenosisBY JAMES A. DEWEESE, M.D., ALLYN G. MAY, M.D., ELLIOT 0. LIPCHIK, M.D.,AND CHARLES G. ROB, M.D.
Abstract:A natomicandHemodynamicCorrelationsin CarotidArteryStenosis
• Pressures were measured in the carotid arteries of 61 patients proximal anddistal to atherosclerotic plaques which were carefully studied by angiographyand anatomical dissection.
(1) An atherosclerotic plaque causing a constriction of less than 47%luminal diameter leaving a lumen greater than 3.0 mm in diameter never causedpressure drops of greater than 10 mm Hg. Stenoses of greater than 63% luminaldiameter leaving lumens less than 1.0 mm in diameter always caused pressuredrops.
(2) Atherosclerotic plaques producing defects which narrowed the lumenfell into a distinct pattern:
(a) Type 1 lesions—This basic lesion filled the bulb of the internalcarotid artery near its origin, causing a 1 to 2 cm smooth ellipticalencroachment on the lumen.
(b) Type 2 lesions—Short localized areas of thickening in addition tothe basic lesion caused bar-like defects of the lumen at the origin of the internalcarotid artery or near the distal end of the lesion.
(c) Type 3 lesions—Multiple bar-like defects were sometimes seen.(d) Type 4 lesions—The areas of increased thickening of the lesion
were sometimes quite narrow, producing diaphragm-like defects on the lumen.Although theoretically these various types of stenoses should produce
different hemodynamic changes, insufficient numbers of observations weremade to corroborate these presumptions.
(3) Angiograms in general mimicked the gross appearance of the plaquesand predicted the actual degree of stenosis produced but did not identify manydiaphragm defects, ulcerations, or small thrombi.
ADDITIONAL KEY WORDSangiography embolismendarterectomy
atherosclerotic plaquespressure changes
thrombosisblood flow
• It is well known that an arterial stenosis candecrease distal blood flow and arterial pres-sure. It is less well known that a very markedconstriction may be required before anyhemodynamic changes occur. When a "criticalstenosis" is present, small increases in constric-tion cause significant reductions in flow and
From the Departments of Surgery and Radiology,University of Rochester School of Medicine andDentistry, 260 Crittenden Boulevard, Rochester, NewYork, 14620.
Supported in part by the United States PublicHealth Service Grant H.E. 07922-05.
Strok: Vol. I, MayJun» 1970
pressure.1"8 The atherosclerotic lesion at thebifurcation of the common carotid arterycommonly associated with symptoms of cere-brovascular insufficiency is a good example ofa localized arterial stenosis. The immediatelyadjacent vessels are usually of normal caliber.Previous studies on small groups of patientsindicated that atherosclerotic stenoses causingocclusions of less than 47% luminal diameter(72% luminal area) did not decrease distalcarotid artery pressure. Stenoses producingconstrictions of greater than 60% luminaldiameter (84% luminal area) almost alwayscaused decreases in pressures and flows.3-1"1 Any
149
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from
DEWEESE, MAY, LIPCHIK, ROB
decrease in arterial pressure distal to a stenosisreflects a comparable percentage decrease inblood flow through the narrowed vessel.'-'- ° Themeasurement of pressure drop across a
a 0% stenosis, and occlusion of the vessel was a100% stenosis.
The absolute value (in millimeters) ofnarrowest diameter of the stenosis was also
% stenosis =(internal diameter of vessel — diameter of lumen in plaque) X 100
internal diameter of vessel
constriction is more practical than measuringblood flow and provides direct evidence ofhemodynamic changes.
It was felt desirable to extend theseobservations to a larger group of patients inhopes of determining more accurately whatdegree of carotid artery stenosis was hemody-namically significant. Careful dissections ofthromboendarterectomy specimens wereplanned to determine how accurately thearteriogram mimicked the anatomical speci-mens. The patterhs of narrowing produced bythe atherosclerotic plaque and their possiblehemodynamic significance were additional ob-jects of the study.
MethodThe 61 patients in this series underwent carotidendarterectomy for symptomatic atheroscleroticocclusive disease at the University of RochesterMedical Center. Angiograms, carotid arterialpressures, and the anatomy of the resectedatherosclerotic plaque from the carotid arterybifurcation were studied.
ANGIOGRAMS
Angiograms of carotid artery bifurcations in twoplanes were obtained by direct carotid arteriogra-phy in five instances and arch aortography in theremaining 56 patients.
Four-vessel angiography was obtained byinjecting 40 to 50 cc of sodium iothalamate(Angio-CONRAY) into the ascending aortathrough a catheter inserted percutaneously via thefemoral or axillary artery. Simultaneous biplaneviews of the arteries were obtained in each studyfor visualization of the two diameters of thevessels.
The degree of stenosis in percent wasdetermined by measuring the diameter of theradiopaque column at its narrowest point in theinternal carotid artery and relating it to thenormal luminal diameter of the vessel at thispoint. The wall of the artery was not visible andtherefore its limits were estimated by drawinglines between the radiopaque border of the distalcommon carotid artery and the radiopaqueborders of the first normal-appearing portion ofthe internal carotid artery distal to the plaque. Ifthere was no narrowing of the vessel, it was called
recorded. All measurements were made directlyon the radiographs. These measurements werecorrected for magnification to give the absolutediameter in millimeters. In our laboratory, thevessels are enlarged between 20 and 25% on theradiographs.
Careful observations of the site of narrowingand shapes of the radiopaque column in theregion of the carotid artery bifurcation wererecorded. It was possible to make accuratemeasurements in 53 of 61 angiograms. Inadequatevisualization in eight angiograms was due to poortechnique or overlapping structures.
ARTERIAL PRESSURES
Arterial pressures were obtained at the time of theoperation after mobilization of the carotid artery.Pressures were measured with a mercury ma-nometer connected by a short length of plastictubing to a No. 22 needle inserted into the artery.Mean pressures were determined by adding to thediastolic pressure one-third of the differencebetween the diastolic and systolic pressures.Proximal pressures were measured in the commoncarotid artery. The needle was then inserted intothe internal carotid artery beyond the plaque andthe distal pressure measured. Then the carotidartery was occluded and a second distal pressurerecorded as the backflow pressure.
ANATOMY OF THE ATHEROSCLEROTIC PLAQUE
Most of the endarterectomies were performed bymaking a longitudinal incision through theadventitia of the artery and establishing thecorrect plane of dissection between the plaque andouter media before occluding the carotid artery. Itwas then usually possible to remove the entirespecimen intact. The diameter of the centrallumen was measured with steel rods at varyingdiameters in increments of 0.5 mm. The diameterof the vessel was determined by measuring thediameter of the plaque at the point of maximalnarrowing. The degree of stenosis was determinedas before by the formula given previously.
The plaques were carefully examined and indifferent specimens tangential, longitudinal ortransverse cuts were made and the anatomydrawn. It was not possible to remove all of thespecimens intact. Careful measurements of thelumen were possible in 41 of 61 patients.
150 Stroke, Vol. I, May-June 1970
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

CAROTID ARTERY STENOSIS
FIGURE 1
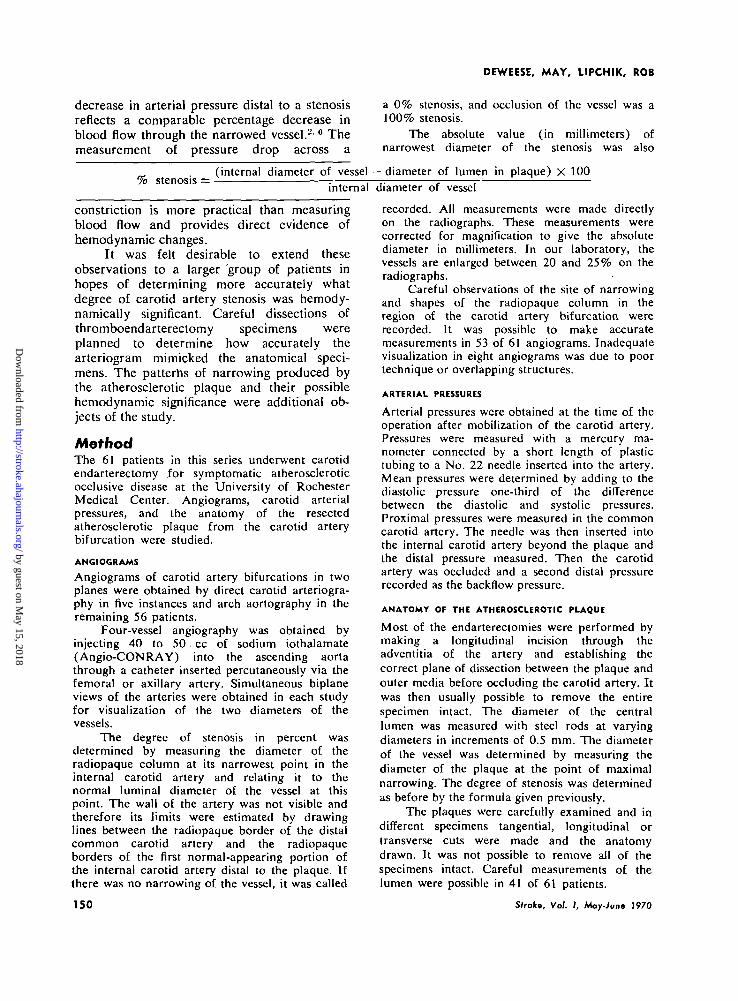
A. Atherosclerotic plaque from carotid bifurcation which has been cut tangentially. The plaqueis thickest at the origin of the external and internal carotid arteries and thins out at theproximal and distal extent of the lesion (type 1). A metal rod with a diameter of 2.5 mmis through the lumen at a point where the plaque is 6 mm in diameter. Therefore, there is a58% constriction of the luminal diameter. There was no difference in proximal and distalpressures. B. Oblique view of angiogram of the same patient demonstrating the smoothelliptical encroachment on the lumen of the internal carotid artery produced by the plaque(type 1). Measurements indicated there was a 2 mm lumen on the angiogram and that therewas a 60% stenosis. There was no pressure drop.
ResultsANATOMY OF THE ATHEROSCLEROTIC PLAQUE
The extent.of the atherosclerotic plaquing wasremarkably similar in all specimens (figs. 1-3).The medial and intimal thickening and degen-eration began about 1 cm proximal to thecarotid bifurcation, extended only a fewmillimeters into the external carotid artery, andextended about 1.5 cm into the internal carotidartery to a point just beyond the bulbousportion of the proximal internal carotid artery.The plaque became very thin near its proximaland distal ends where it appeared to melt intomore normal vessel walls (figs. 1A and 2A). Itwas quite easy to separate the atherosclerotic
Stroke, Vol. I, May-June 1970
core from the media over the central portionsof the lesion, but it became more difficult toseparate the media from the adventitia andintima near the thinner ends of the lesion.
The atherosclerotic plaque was charac-teristically thickest at the origins of the internaland external carotid arteries and in the bulbousportions of the proximal internal carotidartery. This produced a smooth ellipticalencroachment on the lumen of the internalcarotid artery as was best demonstrated bycutting the carotid bifurcation gross specimentangentially or on the oblique view of theangiogram (type 1) (fig. IB).
Frequently, the plaque was quite thick at
151
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from
DEWEESE, MAY, LIPCHIK, ROB
FIGURE 2
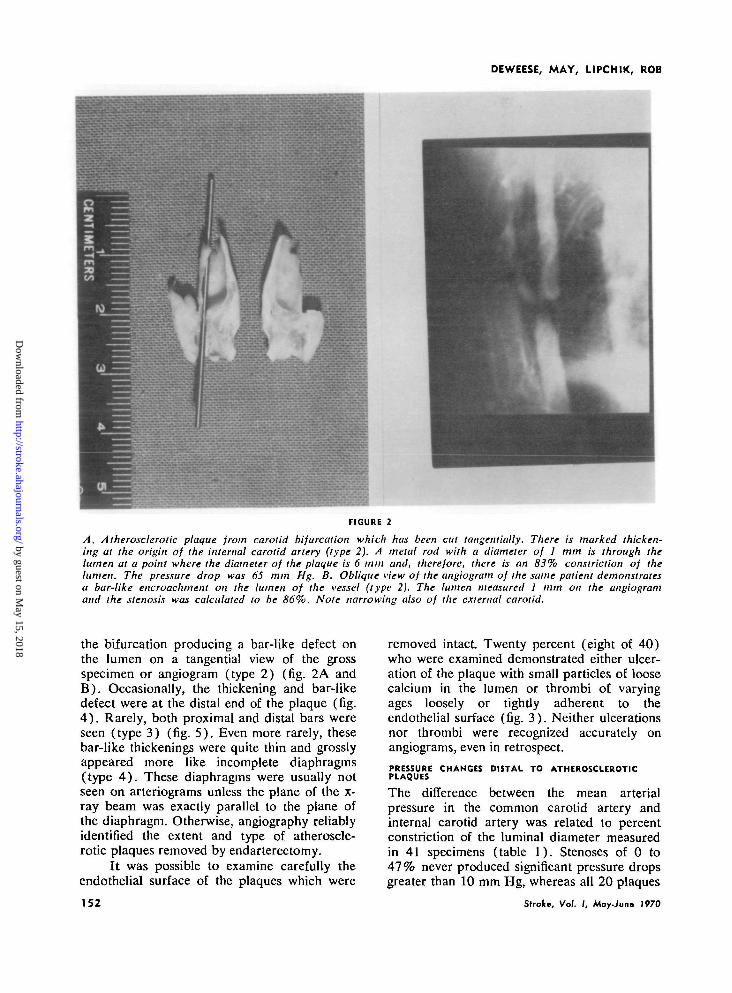
A. Atherosclerotic plaque from carotid bifurcation which has been cut tangentially. There is marked thicken-ing at the origin of the internal carotid artery (type 2). A metal rod with a diameter of 1 mm is through thelumen at a point where the diameter of the plaque is 6 mm and, therefore, there is an 83% constriction of thelumen. The pressure drop was 65 mm Hg. B. Oblique view of the angiograin of the same patient demonstratesa bar-like encroachment on the lumen of the vessel (type 2). The lumen measured 1 mm on the angiogramand the stenosis was calculated to be 86%. Note narrowing also of the external carotid.
the bifurcation producing a bar-like defect onthe lumen on a tangential view of the grossspecimen or angiogram (type 2) (fig. 2A andB) . Occasionally, the thickening and bar-likedefect were at the distal end of the plaque (fig.4 ) . Rarely, both proximal and distal bars wereseen (type 3) (fig. 5) . Even more rarely, thesebar-like thickenings were quite thin and grosslyappeared more like incomplete diaphragms(type 4 ) . These diaphragms were usually notseen on arteriograms unless the plane of the x-ray beam was exactly parallel to the plane ofthe diaphragm. Otherwise, angiography reliablyidentified the extent and type of atheroscle-rotic plaques removed by endarterectomy.
It was possible to examine carefully theendothelial surface of the plaques which were
152
removed intact Twenty percent (eight of 40)who were examined demonstrated either ulcer-ation of the plaque with small particles of loosecalcium in the lumen or thrombi of varyingages loosely or tightly adherent to theendothelial surface (fig. 3) . Neither ulcerationsnor thrombi were recognized accurately onangiograms, even in retrospect.
PRESSURE CHANGES DISTAL TO ATHEROSCLEROTICPLAQUES
The difference between the mean arterialpressure in the common carotid artery andinternal carotid artery was related to percentconstriction of the luminal diameter measuredin 41 specimens (table 1). Stenoses of 0 to47% never produced significant pressure dropsgreater than 10 mm Hg, whereas all 20 plaques
Strode, Vol. I, May-June 1970
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

CAROTID ARTERY STENOSIS
Atherosclerotic plaque from internal carotid arterydemonstrating bar-like narrowing at the distal end ojthe plaque (type 2). Metal pin is through the lumen.The endothelial surface of the plaque is lined withfresh and old thrombus, some of which is easily dis-lodged by the metal pin. The lesion produced an 83%stenosis and a pressure drop of 50 mm Hg.
producing stenoses greater than 63% causedpressure drops of greater than 10 mm Hg (figs.2A and 3). Stenoses producing 48 to 62%constriction of the luminal diameter might ormight not produce significant pressure drops. Aplaque producing a 58% stenosis which did notresult in any pressure drop is illustrated infigure 1A.
The differences in pressures were relatedto percent constriction as measured on 53angiograms (table 2). It was again observedthat stenosis of 0 to 47% never producedpressure drops greater than 10 mm Hg. In allinstances where there was greater than a 63%stenosis there was some pressure drop (figs.2B, 4 and 5). Stenoses of 48 to 62%might ormight not cause pressure drops (fig. IB).
Strok; Vol. I, May-June 1970
FIGURE 4
Angiogram of carotid artery bifurcation demonstrat-ing a bar-like encroachment on the lumen of the in-ternal carotid artery at the distal end of the athero-sclerotic plaque (type 2). The lumen was JJ mm indiameter and the stenosis was calculated to be 80%.There was a pressure drop of 56 mm Hg.
In general, there was close agreementbetween the measured percent stenosis in grossspecimens and on angiograms. There was lessthan a 10% difference in these measurementsin 28 of 34 patients where the comparisoncould be made. The angiographical measure-ments were 11 to 25% greater than the
TABLE 1
Pressure Drop Across Stenosis as Related toPercent Constriction Measured in Gross Specimen
Groijspecimen
itenosb, %
0-4748-6263-90
0 mm Hg
440
Pressure1-10 mm
190
dropHg >10mm Hg
03
20
153
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

DEWEESE, MAY, LIPCHIK, ROB
Angiogram of carotid artery bifurcation. The athero-sclerotic plaque is of varying thicknesses with bar-like defects on the lumen near both the proximal anddistal ends of the plaque (type 3). There was an 86%stenosis causing a pressure drop of 100 mm Hg. Thelumen was 1 mm in diameter at its narrowest.
specimen measurements in four patients and13 to 20% less than the specimen in twopatients (figs. 1 and 2).
In most instances it was quite easy toobtain an accurate measurement of the remain-ing lumen in the carotid artery on angiograms.It was more difficult to estimate the internaldiameter of the vessel without a plaque.Therefore, the pressure drop across thestenosis was related to the absolute luminaldiameter as measured on angiograms in 43patients (table 3). If the lumen was 0 to 1.5mm in diameter there was always a greaterthan 10 mm Hg pressure drop (figs. 2, 4 and5). If the lumen was greater than 1.5 to 3.0mm there might or might not be a pressuredrop (fig. 1). If the lumen was greater than 3.0mm, there was never a pressure drop greaterthan 10 mmHg.
154
TABLE 2
Pressure Drop AcrossPercent Constriction on
Arteriogramitertoib, % 0
0-4748-6263-95
Discussion
mm Hg
460
Stenosis asAngiogram
Pressure dropl-10mm Hg
4102
Related to
>10 mm Hg
03
24
The results of the pressure drops occurringacross varying degrees of stenosis were re-markably similar to previous studies of smallergroups of patients.8"" A stenosis causingconstriction of less than 47% luminal diameter(72% luminal area) never caused a significantdecrease in distal pressure of greater than 10mm Hg. All stenoses causing a greaterocclusion than 63% of luminal diameter (87%luminal area) produced some pressure drop. Inthe range of stenoses between 47% and 63%,the results of the pressure drops were notconsistent. It was not possible, therefore, toassign a specific degree of stenosis as being thedividing line between an insignificant andsignificant stenosis as was possible in experi-mental models.1'2 From a practical viewpoint,however, one can state that if an angiogramdemonstrates less than a 47% narrowing of theluminal diameter of the carotid artery or thepatent lumen is greater than 3.0 mm indiameter, the stenosis is not hemodynamicallysignificant. A 63% constriction of luminaldiameter or a patent lumen less than 1.0 mm indiameter is always hemodynamically signifi-cant.
The arteriogram, in general, accuratelydescribed the gross appearance of the athero-sclerotic lesions at the carotid bifurcation. Infour instances, however, the arteriogram indi-cated the stenosis to be 11 to 25 % more severe
TABLE 3
Pressure Drop Across Stenosis asLuminal Diameter by Arteriogram
Luminaldiameter, mm 0
0-1.51.5-3.0>3.0
mm Hg
035
Pressure dropl-10mm Hg
0103
Related
>10 mm
1930
fo
Hg
Sirok; Vol. I, May-June 1970
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

CAROTID ARTERY STENOSIS
than it actually was. In only two cases did thearteriogram indicate that the stenosis was 13 to20% less than when the specimen itself wasmeasured. Unfortunately, it was not possible toidentify small thrombi or ulcerations onangiograms in the 20% of specimens demon-
its component parts and the hemodynamiceffects of these parts were individuallyanalyzed.2 The hemodynamically dominantcomponent of an arterial stenosis is its outflowtract, i.e., the expansion to normal distallumen. Of considerably less significance is the
Equation 1. AP = AP, + APB, where AP = pressure drop across stenosisAP, = contribution of stenosis length to pressure dropAPE = contribution of distal luminal expansion of pres-
but sure drop
/Aand APE = p x V r X ( ^ i
Thus, it may be written:
where fi — viscosity of bloodR = radius of arteryL = length of stenosisVi = velocity of blood in unstenosed arteryA2 = cross-sectional area of stenosed arterial lumenAx = cross-sectional area of normal arterial lumenp — density of blood
Equation 2. AP = p ?
strating such potential sources of emboli.Blood flow through and pressure drop
beyond an arterial stenosis result from theinteraction of numerous local and systemicvariables. The systemic variables includecardiac output, peripheral vascular resistance,velocity of blood flow, collateral circulation,luminal size of the artery, viscosity of blood,and heart rate. The local variables havinghemodynamic influence include the cross-sectional luminal area remaining patent withinthe stenosis and, possibly, the shape of thestenosis. Many of these variables are interde-pendent, a change in one resulting in simulta-neous changes in others.
Several investigators have shown that acertain degree of arterial constriction, termed"critical stenosis," must be exceeded beforeany appreciable hemodynamic alteration oc-
length of the constriction, and of negligibleimportance is the proximal luminal contrac-tion. The hemodynamic effect of an arterialstenosis may be expressed mathematicallyas:
The above equations were derived forconditions of laminar and steady flow. Never-theless, when they have been applied toexperimental observation on flow throughstenoses in blood vessels the fit has been veryclose. In addition the formula has been used topredict the degree of stenosis that might benecessary to decrease flow in arteries ofdifferent caliber and with different velocity offlow; these predictions have been accurate.
Assuming that the hemodynamic contri-bution of stenosis shape occurs predominantlyat the distal luminal expansion, then Equation2 may be modified to read:
curs. At first there was a lack of consistencyamong investigators concerning the magnitudeof this "critical stenosis." But this apparentlack of agreement disappeared when theanatomy of the arterial stenosis was reduced to
Strok; Vol. I, May-June 1970
where f (i/>) = the function representing thehemodynamic effect of stenosis shape.
The magnitude of the contribution of f(tp) to AP has already been the object ofexperimental investigation. In the considera-
155
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

DEWEESE, MAY, LIPCHIK, ROB
TABLE 4
Relationship of Shape of Stenosis to ArterialPressure Drop and Percent Stenosis
Presiure drop
33502215285
10100454
1058
100003
Shape of rtonoili*
1
1411141
2121
4412
Percent tttnoiii
6060605855555050505050505050505050505048
*Type 1: gradual, elliptical encroachment onlumen; type 2: bar defect; type 3: multiple bardefects; type 4: diaphragm.
tion of stenosis shape on hemodynamic effects,the length of stenosis, the presence of multiplestenoses in series, and the configuration of theoutflow tract may be profitably examined.There is agreement that length has a measur-able, although small, hemodynamic effect.7'8
The influence of length becomes much largerwhen the degree of luminal constriction 4ssevere.- VonRuden et al.8 found that theaddition of identical but distinct arterialstenoses in series causes hemodynamic changesessentially the same as those of increasedlength. A series of stenoses causing differentdegrees of luminal narrowing was found tohave the same effect as the most constrictingstenosis alone. The effect of differences inconfiguration of the distal luminal expansion ofthe stenosis was studied by Holen andSchwartz." They found that gradual distalexpansion diminished the hemodynamic in-fluence of a stenosis in an in vitro systemwhereas it had no perceptible influence in an invivo canine aorta preparation. Thus, givenstenoses of the same degree of luminalconstriction the shapes that might be expectedto differ in hemodynamic influence may be
156
categorized as long and short. In terms of thecarotid atheromas encountered in this series ofpatients, the lesions may be grouped as followsin order of hemodynamic importance:
Multiple bars > single bar > > dia-phragms or smooth stenosis, or
Type 3 > Type 2 > > Type 4 or Type 1In attempting to correlate the hemody-
namic contribution of shape of the atheromas,it is necessary to realize that lesions producingmodest degrees of luminal constriction will bepredominantly of type 1. Indeed, of theatheromas producing less than 48% luminalconstriction, 50% were type 1 shape, whereasof those producing more than 62% constric-tion, only 14% were of type 1 shape.Therefore, if hemodynamic differences due toshape are to become apparent, one mustanalyze the atheromas which constrict thelumen from 48% to 6 3 % , i.e.,'which are notso disparate in degree of luminal constrictionand which are at the threshold of criticalstenosis. Table 4 ranks 20 carotid atheromas inorder of degree of luminal constriction andcorrelates the shape of the atheromas and thepressure drop. There is no statistically signifi-cant distribution of the shape of atheromaswith regard to pressure drop. There is,however, a positive correlation between themagnitude of pressure drop and the degree ofluminal constriction. The shape of carotidatheromas did not seem to influence thehemodynamic effects of the resulting arterialstenosis in this study, but the possibility shouldbe considered in evaluation of larger series oflesions.
References1. Mann FC, Herrick JF, Essex HE, et a l : The
effect on blood flow of decreasing the lumenof a blood vessel. Surgery 4 : 249-252 (Aug)1938
2. May AG, DeWeese JA, Rob CG: Hemodynamic
effects of arterial stenosis. Surgery 53: 513-
524 (Apr) 1963
3. May AG, Van de Berg L, DeWeese JA, et a l :
Critical arterial stenosis. Surgery 54: 250-259
(July) 1963
4. Crawford ES, DeBakey ME, Blaisdell FW, et
a l : Hemodynamic alterations In patients with
cerebral arterial insufficiency before and after
operation. Surgery 48: 76-94 (July) 1960
5. Crawford ES, Wukasch DW, DeBakey ME:
Stroke, Vol. /, May-June 1970
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

CAROTID ARTERY STENOSIS
Hemodynamic changes associated with carotid Surg Gynec & Obst 128: 729-734 4Apr)artery occlusion: An experimental and clinical 1969study. Baylor Cardiovascular Research Center 8. VonRuden WJ, Blaisdell FW, Hall AD, et a l :Bull 1 :3 -10 (Fall) 1962 Multiple arterial stenoses: Effect on blood
6. Tindall GT, Odom GL, Cupp HB Jr, et a l : flow. Arch Surg (Chicago) 89: 307-315Studies on carotid artery flow and pressure. J (Aug) 1964Neurosurg 19: 917-923 (Nov) 1962 9. Holen J, Schwartz SI: Effects of gradual
7. Kindt GW, Youmans JR: The effect of expansion on arterial stenosis. Bull Mathstricture length on critical arterial stenosis. Biophysics 29: 533-540 (Sept) 1967
Strok; Vol. I, MoyJvn, 1970 157
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from

ROBJAMES A. DEWEESE, ALLYN G. MAY, ELLIOT O. LIPCHIK and CHARLES G.
Anatomic and Hemodynamic Correlations in Carotid Artery Stenosis
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1970 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.1.3.149
1970;1:149-157Stroke.
http://stroke.ahajournals.org/content/1/3/149on the World Wide Web at:
The online version of this article, along with updated information and services, is located
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Answer
Permissions and Rights QuestionServices. Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page underthe Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notStrokepublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 15, 2018
http://stroke.ahajournals.org/D
ownloaded from