analysis of failure in the treatment of impacted maxillary ... · adjacent tooth, poor anchorage,...
TRANSCRIPT

ORIGINAL ARTICLE
Analysis of failure in the treatment of impactedmaxillary canines
Adrian Becker,a Gavriel Chaushu,b and Stella Chaushuc
Jerusalem and Tel-Aviv, Israel
Introduction: In this study, we aimed to evaluate the reasons for failure of orthodontic treatment for impactedmaxillary canines and to recommend measures to overcome them. Methods: Twenty-eight patients (ages,17.4 6 4.3 years) with 37 maxillary impacted canines were referred after a failed attempt to resolve the impac-tion. Reasons for failure were analyzed, and corrective measures undertaken. The success rate of the revisedtreatments and the durations of both treatments were recorded. Results: The mean duration of the failed treat-ments was 26.2 6 17.2 months. The failed treatments were mostly based on plane radiographs, intra-archdental anchorage, and elastic traction directly to the labial archwire. The major reasons for failure wereinadequate anchorage (48.6%), mistaken location and directional traction (40.5%), and ankylosis (32.4%).In several patients, there was more than 1 possible reason for failure. The success rate of the revisedtreatments was 71.4%, and the mean duration was 14.4 6 7.2 months. Repeat surgery was needed for62.9% of the canines in which corrective treatment was started, mostly to redirect the ligature wires. Thecorrective measures included the use of 3-dimensional imaging and a change in the direction of traction.Anchorage was reinforced by dental and skeletal means. Conclusions: Inaccurate 3-dimensional diagnosisof location and orientation of impacted teeth and failure to appreciate anchorage demands were the major rea-sons for failure in the treatment of impacted canines. (Am J Orthod Dentofacial Orthop 2010;137:743-54)
Today, most patients seeking correction of mala-lignment and malocclusion of the erupteddentition are assured of a predictable, superb
treatment outcome. This is reflected in the exacting de-mands established by the various examining bodies thathave been set up worldwide to regulate the admission ofprofessionals aspiring to the rank of specialist orthodon-tist or an equivalent title, and in the case presentationspublished in the clinical orthodontic literature.
However, when the patient’s malocclusion includesan impacted tooth, particularly a maxillary canine, someapprehension, doubt, or uncertainty creeps into theequation. The proposed treatment plan is usually ac-companied by a warning to the patient that treatmentof this particular element in the overall treatment planmight fail.
aClinical associate professor emeritus, Department of Orthodontics, Hebrew
University, Hadassah School of Dental Medicine, Jerusalem, Israel.bAssociate professor, Department of Oral and Maxillofacial Surgery, Maurice
and Gabriela Goldschleger School of Dental Medicine, Tel-Aviv University,
Tel-Aviv, Israel.cAssociate professor and Chair, Department of Orthodontics, Hebrew Univer-
sity, Hadassah School of Dental Medicine, Jerusalem, Israel.
The authors report no commercial, proprietary, or financial interest in the prod-
ucts or companies described in this article.
Reprint requests to: Stella Chaushu, Department of Orthodontics, Hebrew
University, Hadassah School of Dental Medicine, PO Box 12272, Jerusalem
91120, Israel; e-mail, [email protected].
Submitted, May 2008; revised and accepted, July 2008.
0889-5406/$36.00
Copyright � 2010 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2008.07.022
The chief reason for this striking contrast includesthe many complicating factors related to the impactedtooth that are not normally present in a fully erupteddentition. Thus, it is difficult to determine accuratelythe 3-dimensional (3D) position of the tooth in relationto both its crown and root, and the proximity to the rootsof other teeth.1-3 It is nearly impossible to clinicallyexamine for crown anomaly, color, shape, mobility,and pathology of an impacted tooth. Surgery isneeded, and it is difficult to determine directionallysuitable orthodontic forces that will resolve theimpaction, and whether they should include extrusion,rotation, crown tipping, or root uprightingcomponents.4,5 Treatment is likely to be extended andpainful,6 and the periodontal prognosis of the outcomeis difficult to predict.7-9
Analysis of the reasons for failure must considermany factors, which can be roughly divided into 3groups as follows.
1. Patient-dependent factors: abnormal morphologyof the impacted tooth, age, pathology of the im-pacted tooth, grossly ectopic tooth, resorption ofthe root of an adjacent tooth, and lack of compli-ance (eg, missed appointments, inadequate oralhygiene).
2. Orthodontist-dependent factors: mistaken posi-tional diagnosis and inappropriate directional force,missed diagnosis of resorption of the root of an
743

744 Becker, Chaushu, and Chaushu American Journal of Orthodontics and Dentofacial Orthopedics
June 2010
adjacent tooth, poor anchorage, inefficient appli-ance, and inadequate torque.
3. Surgeon-dependent factors: mistaken positional di-agnosis, exposure on the wrong side, or rummagingexposure; injury to the impacted tooth; injury to anadjacent tooth; soft-tissue damage; and surgerywithout orthodontic planning.
The purpose of this article was to examine the re-cords of patients with an impacted tooth whose originalorthodontic treatment did not resolve the impaction.The patients were referred to one of the authors. Weanalyzed the reasons for failure of the initial treatmentapproach, devised an alternative treatment approach,and evaluated its success.
MATERIAL AND METHODS
A sample of 28 patients (18 female, 10 male; ages,17.4 6 4.3 years) with 37 impacted canines was assem-bled from the private practices of the 3 authors. The pa-tients’ initial records showed that 26 impactions werepalatal, 9 were buccal, and 2 were in the midalveolus.All patients had been treated elsewhere for a malocclu-sion that included at least 1 impacted maxillary caninethat did not respond to treatment. They were referredby general practitioners or orthodontists and were takenconsecutively in the referral system for inclusion in ourinvestigative sample. In this study, an orthodontist wasdefined as a dentist who has received specialty trainingin a state-recognized university graduate orthodonticcourse.
Of the sample, 9 patients had bilateral impaction ofthe canines, and each failed canine was consideredseparately in the study. From the patient records, thefollowing treatment information was gathered.
1. Details related to the initial treatment: had the treat-ing practitioner received specialist orthodontictraining (as detailed above) with more or less than10 years of postgraduation experience, or was heor she a general practitioner with more or lessthan 10 years since graduating from dental school;was the patient transferred in relation to the surgicalexposure (before, after); was the patient transferredin relation to the stage of orthodontic treatment(before orthodontic treatment or after the failedtreatment); was radiographic documentation usedfor the original diagnosis; how many times wassurgical exposure performed on the tooth; was thesurgery successful; how was traction applied (pa-tients were differentiated into those whose tractionwas performed directly to the labial archwire andthose whose traction had 2 stages, first vertically
downward to clear the root of the incisor and thenlaterally into its place in the arch); was the anchor-age base intra-arch dental, interarch dental, extrao-ral, or implant; how much time elapsed between thestart of treatment and the realization of failure; andwhat were the assumed reasons for failure.
2. Details related to the second orthodontic treatment:were additional radiographic records needed; whatwas the outcome of revised treatment (success orfailure); how long was the revised treatment; whatwere the revised reasons for initial treatmentfailure; and what corrective measures were adopted(new surgery, altered direction of traction, rein-forced anchorage).
RESULTS
The patients were referred by 26 clinicians. Twentywere specialists, including 15 who had over 10 years ofexperience, and 6 were general practitioners, including3 with more than 10 years of experience. Most patients(26 of 28; 92.9%) were referred after surgery had beenperformed. In 2 (patients 11 and 22), space had beenprepared for the impacted teeth without surgery. It hadbeen optimistically expected that the teeth would eruptspontaneously, but that had not occurred. Twenty-fivepatients (89.3%) had been referred during active ortho-dontic treatment and 3 after the treatment was stoppedbecause of failure.
Table I describes the initial treatment plans. Pano-ramic and cephalometric films were available for all pa-tients, together with variable numbers of periapicalviews. Two patients had undergone 3D imaging, one(patient 8) with conventional spiral computed tomogra-phy (CT), and the other (patient 12) with cone-beam CT(CBCT). Among the 35 canines that had previouslybeen exposed, 10 (28.6%) had had 3 such episodes. In1 bilateral case (patient 3), who had been treated byopen exposure, the bonded attachments had failed onboth canines, and the tissues had subsequently rehealedover the teeth. In 2 (patients 6 and 24), the surgeon hadfailed to find the impacted tooth because of misdiagno-sis of labiolingual location.
Elastic traction, directly to the arch, was used for 26canines. For the 7 canines treated in 2 stages, an auxil-iary spring was used, with the express aim of eruptingthe canine into the palate as the initial maneuver. The or-thodontic anchorage used in all patients in this sampleconsisted exclusively of intraoral dental anchoragefrom other dental units with fixed bonded appliances;this was therefore omitted from Table I. The mean dura-tion of treatment, from start to realization of failure, was26.2 6 17.2 months. The reasons for failure, as assumed

Table I. Descriptions of initial treatments
Patient RecordsSurgeries
(n) TractionDuration
(mo)Assumed reason
for failure
1 P, C, Pa 1 D 72 Unknown
2 P, C, Pa 1 D 40 Unknown
3 P, C, Pa, O 2 D 10 Attachment failure
P, C, Pa, O 2 D 10 Attachment failure
4 P, C, Pa 1 D 12 Unknown
5 P, C, Pa 1 D 54 Unknown
6 P, C, O 1 X 10 Surgical
7 P, C, Pa 3 D 8 Attachment failure
8 CT 1 D 20 Ankylosis, incisor
root resorption
9 P, C, Pa 1 D 36 Not enough time
10 P, C, Pa 1 D 32 Erupted intractable
P, C, Pa 1 D 32 Erupted intractable
11 P, C, Pa - X 54 Inadequate
follow-up
12 CT 1 D 35 Ankylosis
CT 1 D 35 Ankylosis
13 P, C, Pa 1 TS 48 Ankylosis, incisor
root resorption
14 P, C, Pa 1 D 36 Incisor root
resorption
15 P, C, Pa 1 D 23 Incisor root
resorption
16 P, C, Pa 3 D 39 Ankylosis
17 P, C, O 3 D 48 Ankylosis
P, C, O 3 D 48 Ankylosis
18 P, C D 12 Unknown
19 P, C, Pa 3 D 28 Ankylosis
20 P, C, Pa 1 D 48 Unknown
21 P, C, Pa 1 D 30 Ankylosis
22 P, C, PA - X 30 Intractable position
23 P, C 1 D 18 Incisor root
resorption
P, C 1 D 18 Incisor root
resorption
24 P, C, Pa 3 X 9 Surgical
25 P, C, O 1 D 9 Ankylosis
P, C, O 1 D 9 Ankylosis
26 P, C, O 3 TS 7 Ankylosis
P, C, O 3 TS 7 Ankylosis
27 P, C, Pa 1 TS 7 Ankylosis
P, C, Pa 1 TS 7 Ankylosis
28 P, C, Pa 3 TS 14 Ankylosis
P, C, Pa 3 TS 14 Ankylosis
P, Panoramic; C, cephalogram; Pa, periapical; O, occlusal; CT,
computerized tomography; D, direct traction to archwire; TS, 2-stage
traction; X, surgery failed to find the tooth (patients 6 and 24) or
spontaneous eruption failed to occur (patients 11 and 22).
Two rows for a patient indicate bilateral impactions.
American Journal of Orthodontics and Dentofacial Orthopedics Becker, Chaushu, and Chaushu 745Volume 137, Number 6
by the practitioners, were ankylosis (17 teeth, 45.9%),incisor root resorption (6 teeth, 16.2%), intractableposition (3 teeth, 8.1%), attachment failure (3 teeth,8.1%), surgical failure (2 teeth, 5.4%), and inadequatefollow-up period (2 teeth, 5.4%). In 6 teeth (16.2%),
the orthodontist could find no explanation for thefailure, and, for 2 patients, 2 reasons were given.
Table II shows the supplementary records that wereconsidered necessary for each patient. As the result ofthe new information and consequent practical stepstaken, the success rate of the revised treatment planswas 67.6% for the whole group. However, 2 patients(2 canines) refused more treatment, yielding an actualsuccess rate of 71.4%. The mean duration of the newtreatment in the successful patients was 14.4 6 7.2months. After this, it became possible to diagnose thereasons for failure in each patient more accurately.The major causes were poor anchorage (18 teeth,48.6%), mistaken positional diagnosis and directionaltraction (15 teeth, 40.5%), and ankylosis (12 teeth,32.4%). Seven ankylosed teeth were treated by surgicalluxation and subsequent traction, but only 3 were suc-cessfully brought in their place in the arch. In 5 patients(6 teeth, 16.2%), resorption of the incisor roots hadescaped the practitioner’s notice until treatment wasadvanced. Three teeth (8.1%) failed to erupt becauseof interference of soft tissues. In 3 patients (8.1%), inad-equate space was considered to be a cause for nonerup-tion. In one (patient 6), surgery was initially performedat the wrong site, and, in another patient (24), the toothwas in an extremely difficult position; therefore, theseteeth remained unexposed after surgical intervention.In 2 patients (11 and 22), traction was never applied,and the first practitioner waited in vain for 54 and 30months, respectively, for the teeth to erupt unaided.Repeated bond failure of the attachments after surgeryin 2 patients (3 and 7) accounted for treatment failure.In 1 patient (24), both the first practitioner and the sur-geon did not realize that the canine crown was situatedon the palatal side between the central and lateral inci-sors, but its root was labial to the root of the lateral in-cisor. This created an intractable situation, from whichthere was no possibility of saving the tooth. In 1 patient(5), the treatment failed because of poor compliance(missed appointments) and inefficient appliances. Inseveral patients, there were 2 or more possible reasonsfor failure.
Table III summarizes the corrective measures takenfor this group of potentially failed patients. Surgery wasneeded for 22 of the 35 canines (62.9%). Of these, 7 (in5 patients) were to redirect the ligature wires to permita change in direction of traction, 3 (in 3 patients) to clearsoft tissues, 7 (in 4 patients) to luxate ankylosedcanines; 3 teeth needed bond attachments, and 2 werereoperated to expose them in their newly diagnosed po-sitions. In 2 patients, exposure was performed for thefirst time. Orthodontic corrective measures includedthe application of traction in 4 canines to which forces

Table II. Descriptions of the revised treatments
Patient Additional records Outcome Treatment duration (mo) Revised reasons for failure
1 No S 10 Direction, space, anchorage
2 No S 6 Direction, anchorage
3 No S 8 Attachment failure after surgery
No S 8 Attachment failure after surgery
4 No S 6 Inadequate space
5 No S 12 Missed appointments, inefficient appliance
6 CT S 14 Exposure in wrong site
7 No S 12 Attachment failure, direction
8 No S 10 Soft tissue, anchorage, incisor root resorption
9 No S 11 Direction, space, anchorage
10 No S 17 Direction, anchorage
No S 17 Direction, anchorage
11 CT S 6 No traction applied
12 No F - Ankylosis
No F - Ankylosis
13 CT S 15 Direction, soft tissue, anchorage, incisor root resorption
14 Pa S 16 Direction, incisor root resorption
15 CT S 18 Incisor root resorption, direction, anchorage
16 No S 9 Ankylosis*, anchorage
17 No F - Ankylosis, anchorage
No F - Ankylosis, anchorage
18 No S 8 Direction
19 CT No treatment - Unknown
20 CT No treatment - Direction
21 CT F - Ankylosis, anchorage
22 CT S 30 No traction applied
23 CT S 27 Incisor root resorption, direction
CT S 27 Incisor root resorption, direction
24 CT F - Intractable (pseudotransposition)
25 No F - Ankylosis, direction
No F - Ankylosis, direction
26 No F - Ankylosis, anchorage
No F - Ankylosis, anchorage
27 No S 12 Soft tissue, anchorage
No S 12 Soft tissue, anchorage
28 Pa S 25 Ankylosis*, anchorage
Pa S 25 Ankylosis*, anchorage
S, Success; F, failure; CT, computerized tomography; Pa, periapical.
Two rows for a patient indicate bilateral impactions.
*Canines whose ankylosis was resolved with surgical luxation, and the teeth were successfully brought into their place in the arch.
746 Becker, Chaushu, and Chaushu American Journal of Orthodontics and Dentofacial Orthopedics
June 2010
had never been applied. A change in the direction oftraction was mandatory for 15 canines. Anchoragewas reinforced by various methods in 18 canines and in-cluded heavier base archwires, intermaxillary elastics,and temporary implant devices in the more recent cases.Additional space was needed in 2 patients (2 canines).
Case presentations
Patient 6 had a mistaken positional diagnosis of thelabially impacted canine. The original clinician hadreferred the patient for full photographic facial anddental records, and cephalometric, panoramic, andanterior occlusal views (Fig 1). Based on these, sheassumed that the canine was displaced on the palatal
side, close to the midline. Using fixed multibracketedappliances, she had aligned and leveled the teeth tocreate space in the appropriate location. The patientwas then referred to an oral and maxillofacial surgeonfor surgical exposure. The surgeon reflected a palatalflap, removed bone on that side of the incisors, butfailed to find the canine. He then sutured the flapback to its former place and sent the patient back tothe orthodontic practitioner, who consulted with oneof the authors (A.B.). Figure 2 shows the aligned andleveled dentition at the consultation visit. It also showsthe iatrogenic periodontal defect on the palatal side ofthe left central incisor, caused by the futile surgicalexposure.

Table III. Correctives measures taken in the revised treat-ment
Corrective measure Number of teeth
Surgical
Expose in revised (correct) location 2
Reexpose to bond attachments 3
Reexpose to change the direction of ligatures 7
Reexpose to remove soft tissue 4
Luxation 7
Total number of teeth reoperated 22
Expose teeth not previously exposed 2
Orthodontic
Apply traction when it had not been
applied before
4
Reevaluate position and change direction
of traction
15
Reinforce anchorage 18
Create space 2
American Journal of Orthodontics and Dentofacial Orthopedics Becker, Chaushu, and Chaushu 747Volume 137, Number 6
Comparing these pictures with the initial clinicalphotographs shows how this stage of treatment hadeliminated the clinical signs that were present initially,which should have indicated to the practitioner andthe surgeon that the impacted canine was on the labialside. Moreover, this could have been positively con-firmed by using the vertical parallax method of diagno-sis, from the plane radiographic panoramic and anteriorocclusal views that had been commissioned at the outset(Fig 1).
Before the recommencement of treatment, a CBCTimage (Fig 3) was taken to diagnose or negate any path-ologic changes from the earlier orthodontic and surgicalprocedures and to accurately locate the tooth in 3 di-mensions, along its entire length. The canine was ex-posed on the labial side (Fig 4, A) and aligned in thenormal way with 2-stage traction—first to the labial(Fig 4, B) and then to the distal—to circumnavigatethe root of the lateral incisor. The clinical and pano-ramic views at 5 years posttreatment show the align-ment achieved and the similarity between the treatedand untreated sides (Fig 5, A, B, and D). However, thepalatal gingival defect from the first surgical procedureremained (Fig 5, C).
For patient 23, the diagnosis of severe incisor rootresorption was missed. Based on the clinical examina-tion and a panoramic view, the first practitioner had di-agnosed bilaterally impacted canines, with the rightcanine palatally and the left canine labially displaced(Fig 6). Surgical exposure was attempted after 15months of active orthodontic treatment with fixed multi-bracketed appliances, during which the teeth had beenaligned and leveled. No new radiographs were takenat this stage.
It was only at the time of surgery that the surgeonnoted severe root resorption of the adjacent incisorsand recorded the condition both photographically andradiographically (Fig 7). He nevertheless bonded at-tachments to the canines, closing the surgical flap andreferring the patient to an author (S.C.).
A CBCT image was used to evaluate and confirm theseverity and form of incisor root loss (Fig 8). Reopera-tion was indicated, especially for the palatal rightcanine, to redirect the ligature wires that had initiallybeen drawn in the direction of the canine’s final anddesired location (Fig 9). This was done to permit thecanine to be moved away from the incisors in the firststage. Figure 10 shows the final alignment of bothcanines and the radiographic view of the incisor areaat 24 months posttreatment. The extent of root resorp-tion, the regeneration of bone, and a distinct laminadura around each tooth can be clearly seen.
DISCUSSION
The prevalence of canine impaction in the generalpopulation of most Western countries has been vari-ously described as between 0.92% and 2.4%.10-14
Since this problem is a local etiologic factor leadingto malalignment and malocclusion of the teeth, it mustbe assumed that in any orthodontic practice there willbe a disproportionately larger number of patients whosuffer from this anomaly. Many will be treatedsuccessfully, but, as can be seen in this study, someclinicians will fail to resolve the impaction in at least1 patient and will find it necessary to either refer thepatient elsewhere to improve the chances of success oradvise extraction. This appears to have no relationshipto whether the clinician has had orthodontic specialisttraining or has many years of clinical experience.However, by its very nature, our sample wasunquestionably biased, since affected patients will beusually treated by specialists, and most generalistswill not undertake cases of this nature. Nevertheless,this study demonstrates that many specialists areinadequately equipped to diagnose the anomaly andfrequently become aware of the problem only whentreatment for the overall malocclusion is well advanced.
Furthermore, although the treatments we analyzedhad included all the elements needed for a successfultreatment, including orthodontics and surgical exposurein every patient, with the exception of 2 patients, theyhad all failed. The orthodontic treatment for these 2 pa-tients had been expected to cause the autonomous erup-tion of the teeth, without the need for surgery, whenadequate space was provided. Even the waiting periodsof 36 and 54 months had been insufficient to generate

Fig 1. Patient 6: pretreatment views.
Fig 2. Patient 6: clinical views at the referral consultation.
Fig 3. Patient 6: CBCT images. A, Paraxial view (vertical slice) through the central incisor; B, axialview (horizontal slice).
748 Becker, Chaushu, and Chaushu American Journal of Orthodontics and Dentofacial Orthopedics
June 2010
autonomous eruption. This indicates questionable judg-ment in the assessment of the patients in general anda lack of appreciation of the potential complexity ofthe problem in the treatment plan.
Advancing age has been shown to reduce the chan-ces of orthodontic resolution of impacted teeth, specif-
ically in the fourth decade of life and beyond.15-17 Inour sample, only 1 patient (25) was over 30 years ofage, and both maxillary canines were ankylotic andcould not be moved.
The initial location for 34 of the 37 impacted teethin this sample had been determined with plane film
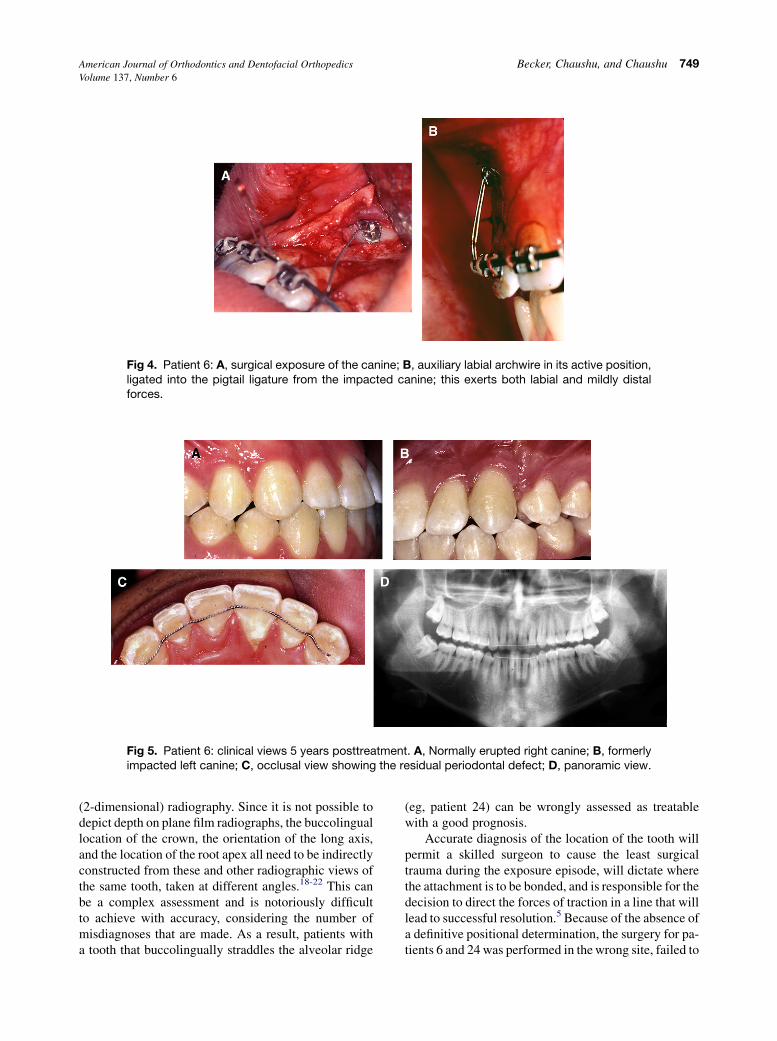
Fig 4. Patient 6: A, surgical exposure of the canine; B, auxiliary labial archwire in its active position,ligated into the pigtail ligature from the impacted canine; this exerts both labial and mildly distalforces.
Fig 5. Patient 6: clinical views 5 years posttreatment. A, Normally erupted right canine; B, formerlyimpacted left canine; C, occlusal view showing the residual periodontal defect; D, panoramic view.
American Journal of Orthodontics and Dentofacial Orthopedics Becker, Chaushu, and Chaushu 749Volume 137, Number 6
(2-dimensional) radiography. Since it is not possible todepict depth on plane film radiographs, the buccolinguallocation of the crown, the orientation of the long axis,and the location of the root apex all need to be indirectlyconstructed from these and other radiographic views ofthe same tooth, taken at different angles.18-22 This canbe a complex assessment and is notoriously difficultto achieve with accuracy, considering the number ofmisdiagnoses that are made. As a result, patients witha tooth that buccolingually straddles the alveolar ridge
(eg, patient 24) can be wrongly assessed as treatablewith a good prognosis.
Accurate diagnosis of the location of the tooth willpermit a skilled surgeon to cause the least surgicaltrauma during the exposure episode, will dictate wherethe attachment is to be bonded, and is responsible for thedecision to direct the forces of traction in a line that willlead to successful resolution.5 Because of the absence ofa definitive positional determination, the surgery for pa-tients 6 and 24 was performed in the wrong site, failed to

Fig 6. Patient 23: pretreatment views.
750 Becker, Chaushu, and Chaushu American Journal of Orthodontics and Dentofacial Orthopedics
June 2010
locate the tooth, and, because of the rummaging search,inflicted considerable and superfluous surgical trauma.
The other important entity that is difficult to diag-nose from plane film radiographs is resorption of theroots of teeth adjacent to the impacted tooth.23-26 Afacially or palatally aberrant tooth is depictedsuperimposed on the root of a lateral or central incisorin the buccolingual plane. Thus, the most likely site tobe affected on the incisor is the labial or lingualaspect of the root, facing and close to the canine.25
Any consequent flaw in the integrity of the root of thetooth will become visible only on a panoramic or peri-apical film when resorption has affected the continuityof the mesiodistal profile of the root and only whenthis is not obscured by the superimposed images.
The ultimate answer to all of these potential prob-lems lies in the intelligent use of CBCT. It delineatesimpacted teeth clearly, in 3 planes of space and in rela-tion to their surrounding structures, both dental and non-dental. Furthermore and in contrast with plane filmradiography, CBCT is free of projection distortion andeliminates the superimposition of neighboring teeth.27-29
For the amount of information that it provides, thedosage of ionizing radiation is low, and the method ishighly cost-effective, recommending it as a routinediagnostic aid in the proposed treatment of all but themost superficial of impacted teeth.27
Since the positional diagnoses of the impacted teethin the sample were almost exclusively made on the basisof plane film radiography, that was at least partiallybecause several patients were treated some years ago,before the introduction of CBCT. Even now, many prac-
titioners are unaware of this modality and its advan-tages, or consider it superfluous. In the reevaluation ofthe patients, CT was used in only 10, since the resthad been reviewed some years earlier. In any suchreevaluation of a failed case today, CBCT would beconsidered a mandatory prerequisite.
For both labially and palatally displaced canines,the direct path to their rightful place in the arch is fre-quently impeded by the root of the lateral incisor or,occasionally, even the central incisor. Therefore, todraw the canine in a direct line to this prepared spaceinevitably brings it into direct contact with the incisorroot. In the simpler cases, a minor amount of angularinterference can be overcome by an increase in thetraction force, but movement of the impacted toothwill be resisted to a greater or lesser extent. Increasingthe force will increase the load on the anchor unitsand lead to loss of anchorage. Furthermore, it mightcause incisor root resorption or exacerbate a processthat had been present before treatment—a conditionfound in 66.7% of the lateral incisors and 11.1% ofthe central incisors in patients with maxillary canineimpaction.28
To eliminate this potential source of failure, traction in2 separate stages and in 2 directions should be started.30,31
The first stage is to move the impacted tooth away fromthe root of the incisor and into a location where thetooth has a direct path to its place in the arch. Fora palatal canine, this is usually in a slightly palatal butmainly vertically downward direction. Once clear, thetooth can then be drawn buccally, with a simple labialtipping movement toward the labial archwire. Neither of

Fig 7. Patient 23: records taken during the first surgical procedure. A, Right canine (palatal); B, leftcanine (buccal); C and D, right and left periapical radiographs.
Fig 8. Patient 23: paraxial views from CBCT. A, Right; B, left.
American Journal of Orthodontics and Dentofacial Orthopedics Becker, Chaushu, and Chaushu 751Volume 137, Number 6
these movements causes much danger of loss ofanchorage, and there is no reason to expect resorption ofthe roots of the adjacent incisors.
In terms of mechanotherapy, the second componentof this 2-stage movement is simple to design and mighttake the form of an elastic tie or an auxiliary superelasticlabial archwire.5 However, the first stage of the 2-stagemovement requires inventiveness and initiative from theoperator in designing a custom-built auxiliary springthat will cause movement in the desired direction,neither along nor toward an archwire.31-33
In most of these cases, the actual amount of move-ment, tipping or bodily, is taxing on dental anchorage.Accordingly, before the clinician’s attention turns tothe resolution of the impacted tooth, he or she should
create a composite anchor unit involving all availableerupted teeth in the same jaw and, often, in the oppositejaw as well. This is most conveniently done by using aslarge a base arch as will fill the slots of the brackets onall other teeth, with or without intermaxillary elastics.With the advent of temporary anchorage devices inroutine orthodontic treatment, consideration should begiven to their use in many of these cases.34,35 Anindependent implant system for traction of the caninecan be designed and used before or parallel to theregular orthodontic appliances that will be used forthe overall malocclusion.35 In our sample, for failure as-sociated with loss of anchorage in 18 canines, each ofthe above remedies was variously used in the revisedtreatments, as indicated.

Fig 9. Patient 23: clinical view of the right canine. A, At the referral consultation; B, during the repeatsurgery to redirect the ligature through palatal tissue; C, traction is applied from a custom built aux-iliary archwire with a loop spring to erupt the palatal impacted right canine through the palatal mucosaand away from the resorbed right lateral incisor root; D, the same auxiliary archwire has a secondloop to erupt the labially impacted left canine away from the resorbed left lateral incisor root.
Fig 10. Patient 23: clinical views 2 years posttreatment. A, Right canine; B, left canine; C and D, rightand left periapical radiographs.
752 Becker, Chaushu, and Chaushu American Journal of Orthodontics and Dentofacial Orthopedics
June 2010
Ankylosis of the impacted tooth is often an ortho-dontist’s blanket diagnosis to cover all failed cases.However, as we have seen in this study, several of thoseteeth responded to orthodontic force that was appropri-
ately applied, in terms of force level and direction.Nevertheless, there was a relatively high incidence ofankylosis, which might appear to be difficult to explain,since the incidence of ankylosis of impacted canines in

American Journal of Orthodontics and Dentofacial Orthopedics Becker, Chaushu, and Chaushu 753Volume 137, Number 6
young patients is extremely low.36,37 Ankylosis andexternal resorption have been reported as sequelae oforthodontic movement of impacted teeth whendamage is caused to the periodontal ligament byligating the teeth around the neck with a lasso wire.38
Similarly, an overly ambitious exposure might denudethe root surface, or the surgeon might push an elevatorinto the periodontal attachment of the tooth to ‘‘loosenup’’ the tooth, thereby injuring the cementum layer.The orthophosphoric acid etchant, in liquid form, canalso seep into this area and produce chemical traumato the cementum. These incidental and seemingly inno-cent addenda could cause an ankylosis or a cervical rootresorption lesion of the impacted tooth; either will ef-fectively stop all further orthodontic movement of thattooth.5,39
Surgical luxation with appropriate traction was suc-cessful in 3 of the 7 teeth that had the procedure. There-fore, this procedure can be offered to the patient, eventhough its outcome is questionable and has never beenaddressed in the literature.
Before these patients were referred for review oftheir failed treatments, 15 had already undergone 2.5years or more of active orthodontic treatment withappliances; 6 others had passed the 1-year mark. Thenew treatment added a further considerable period oftime to the task of attempting to achieve success inwhat was, in essence, the treatment of a single tooth—and not all these attempts were successful.
CONCLUSIONS
There are many aspects and minutiae involved in thetreatment of impacted maxillary canines that, singly ortogether, can lead to failure of the overall aim of theexercise. This study has shown that failure in this typeof treatment is all too frequent for the following reasons.
1. Diagnosis of the location of the tooth and its imme-diate relationship with the roots of the adjacentteeth is generally treated with cavalier and oftennegligent simplicity, even though modern technol-ogy has provided the tools to achieve this with greataccuracy in all 3 dimensions.
2. With inappropriate positional diagnosis, it followsthat traction will be applied in the wrong direction.
3. A lack of appreciation of the considerable anchor-age requirements of the case and the need to exploitall available means of enhancing them will inevita-bly lead to inefficient mechanotherapy and unnec-essarily longer treatment.
4. Ankylosis might have afflicted the impacted tootheither a priori or as the result of the earlier surgicalor orthodontic maneuvers.
From this platform, we issue a cri de coeur toencourage the teaching of this subject as a separateentity in graduate orthodontic programs in which it isconspicuously absent at this time.
REFERENCES
1. Wolf JE, Mattila K. Localization of impacted maxillary canines
by panoramic tomography. Dentomaxillofac Radiol 1979;8:
85-91.
2. Jacobs S. Exercises in the localisation of unerupted teeth. Aust
Orthod J 1987;10:33-5, 58-60.
3. Chaushu S, Chaushu G, Becker A. The use of panoramic radio-
graphs to localize displaced maxillary canines. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 1999;88:511-6.
4. Kokich VG, Mathews DP. Surgical and orthodontic management
of impacted teeth. Dent Clin North Am 1993;37:181-204.
5. Becker A. The orthodontic treatment of impacted teeth. London:
Informa UK Ltd; 2007.
6. Chaushu S, Becker A, Zeltser R, Branski S, Vasker N, Chaushu G.
Patients perception of recovery after exposure of impacted teeth:
a comparison of closed- versus open-eruption techniques. J Oral
Maxillofac Surg 2005;63:323-9.
7. Becker A, Kohavi D, Zilberman Y. Periodontal status following
the alignment of palatally impacted canine teeth. Am J Orthod
1983;84:332-6.
8. Vermette ME, Kokich VG, Kennedy DB. Uncovering labially
impacted teeth: apically positioned flap and closed-eruption
techniques. Angle Orthod 1995;65:23-32.
9. Crescini A, Nieri M, Buti J, Baccetti T, Pini Prato GP. Orthodontic
and periodontal outcomes of treated impacted maxillary canines.
Angle Orthod 2007;77:571-7.
10. Dachi SF, Howell FV. A survey of 3,874 routine full-month radio-
graphs. II. A study of impacted teeth. Oral Surg Oral Med Oral
Pathol 1961;14:1165-9.
11. Thilander B, Jakobsson SO. Local factors in impaction of maxil-
lary canines. Acta Odontol Scand 1968;26:145-68.
12. Kramer RM, Williams AC. The incidence of impacted teeth. A
survey at Harlem hospital. Oral Surg Oral Med Oral Pathol
1970;29:237-41.
13. Ericson S, Kurol J. Longitudinal study and analysis of clinical
supervision of maxillary canine eruption. Community Dent Oral
Epidemiol 1986;14:172-6.
14. Sacerdoti R, Baccetti T. Dentoskeletal features associated with
unilateral or bilateral palatal displacement of maxillary canines.
Angle Orthod 2004;74:725-32.
15. Harzer W, Seifert D, Mahdi Y. The orthodontic classification of
impacted canines with special reference to the age at treatment,
the angulation and dynamic occlusion. Fortschr Kieferorthop
1994;55:47-53.
16. Becker A, Chaushu S. Success rate and duration of orthodontic
treatment for adult patients with palatally impacted maxillary
canines. Am J Orthod Dentofacial Orthop 2003;124:509-14.
17. Zuccati G, Ghobadlu J, Nieri M, Clauser C. Factors associated
with the duration of forced eruption of impacted maxillary
canines: a retrospective study. Am J Orthod Dentofacial Orthop
2006;130:349-56.
18. Hunter SB. The radiographic assessment of the unerupted maxil-
lary canine. Br Dent J 1981;150:151-5.
19. Ericson S, Kurol J. Radiographic examination of ectopically
erupting maxillary canines. Am J Orthod Dentofacial Orthop
1987;91:483-92.

754 Becker, Chaushu, and Chaushu American Journal of Orthodontics and Dentofacial Orthopedics
June 2010
20. Jacobs SG. Localization of the unerupted maxillary canine: how
to and when to. Am J Orthod Dentofacial Orthop 1999;115:
314-22.
21. Mason C, Papadakou P, Roberts GJ. The radiographic localization
of impacted maxillary canines: a comparison of methods. Eur J
Orthod 2001;23:25-34.
22. Armstrong C, Johnston C, Burden D, Stevenson M. Localizing
ectopic maxillary canines—horizontal or vertical parallax? Eur
J Orthod 2003;25:585-9.
23. Ericson S, Kurol J. Resorption of maxillary lateral incisors caused
by ectopic eruption of the canines. A clinical and radiographic
analysis of predisposing factors. Am J Orthod Dentofacial Orthop
1988;94:503-13.
24. Ericson S, Kurol PJ. Resorption of incisors after ectopic erup-
tion of maxillary canines: a CT study. Angle Orthod 2000;70:
415-23.
25. Becker A, Chaushu S. Long-term follow-up of severely resorbed
maxillary incisors after resolution of an etiologically associated
impacted canine. Am J Orthod Dentofacial Orthop 2005;127:
650-4.
26. Falahat B, Ericson S, Mak D’Amico R, Bjerklin K. Incisor root
resorption due to ectopic maxillary canines. Angle Orthod
2008;78:778-85.
27. Chaushu S, Chaushu G, Becker A. The role of digital volume to-
mography in the imaging of impacted teeth. World J Orthod 2004;
5:120-32.
28. Walker L, Enciso R, Mah J. Three-dimensional localization of
maxillary canines with cone-beam computed tomography. Am J
Orthod Dentofacial Orthop 2005;128:418-23.
29. Liu DG, Zhang WL, Zhang ZY, Wu YT, Ma XC. Localization of
impacted maxillary canines and observation of adjacent incisor
resorption with cone-beam computed tomography. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 2008;105:91-8.
30. Becker A, Zilberman Y. The palatally impacted canine: a new
approach to treatment. Am J Orthod 1978;74:422-9.
31. Kornhauser S, Abed Y, Harari D, Becker A. The resolution of
palatally impacted canines using palatal-occlusal force from
a buccal auxiliary. Am J Orthod Dentofacial Orthop 1996;
110:528-34.
32. Jacoby H. The ‘‘ballista spring’’ system for impacted teeth. Am J
Orthod 1979;75:143-51.
33. Orton HS, Garvey MT, Pearson MH. Extrusion of the ectopic
maxillary canine using a lower removable appliance. Am J Orthod
Dentofacial Orthop 1995;107:349-59.
34. Park HS, Kwon OW, Sung JH. Micro-implant anchorage for
forced eruption of impacted canines. J Clin Orthod 2004;38:
297-302.
35. Chaushu S, Chaushu G. Lingual appliances, implants and
impacted teeth. In: Becker A, editor. The orthodontic treatment
of impacted teeth. London: Informa UK Ltd; 2007. p. 229-38.
36. Caminiti MF, Sandor GK, Giambattistini C, Tompson B. Out-
comes of the surgical exposure, bonding and eruption of 82
impacted maxillary canines. J Can Dent Assoc 1998;64:572-4.
576-9.
37. Szarmach IJ, Szarmach J, Waszkiel D. Complications in the
course of surgical-orthodontic treatment of impacted maxillary
canines. Adv Med Sci 2006;51(Suppl 1):217-20.
38. Boyd RL. Clinical assessment of injuries in orthodontic move-
ment of impacted teeth. I. Methods of attachment. Am J Orthod
1982;82:478-86.
39. Heithersay GS. Invasive cervical resorption: an analysis of poten-
tial predisposing factors. Quintessence Int 1999;30:83-95.