anaesthetic considerations for cleft surgeries
TRANSCRIPT

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 1/67
ANAESTHETIC CONSIDERATIONS
FOR CLEFT SURGERIES
SNIGDHA PADDALWAR
JNMC,DMIMS
WARDHA

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 2/67
INTRODUCTION
Ever since John Snow published in the lancet 1847, thefirst report of giving ether to a 7 year old boy for cleft liprepair, anesthesiologist's have been striving to perfectthe safety of anaesthesia in craniofacial surgeries.
Cleft lip and palate - commonest craniofacialabnormalities.
Facial disfigurement - Huge impact on life of an
individual/family Surgery-Anatomically corrects deformity
Augments dento-alveolar growth
Restores normal palatal function and self confidence
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 3/67
INTRODUCTION (CONTD)
Safe surgical repair
R equires a team approach.
µthe difference to thesurgeon, between doing acleft palate operation witha thoroughly experienced anaesthetist and aninexperienced one, is the
difference between pleasure and pain! ¶
-Quoted by a surgeon in 1912
ANAESTHETIST
PAEDIATRICIAN
SURGEON

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 4/67
INTRODUCTION (CONTD)
The optimum anaesthetic management depends
on
1.Age of the patient
2.Associated abnormalities
3.Availability of
Intraoperative monitoring equipment
Anaesthetic drugs
Expertise Level of postoperative care
Availability of equipments/devices for difficult airway

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 5/67
INTRODUCTION (CONTD)
The majority of anaesthetic morbidity relates to
Establishment of difficult airway
Protection and maintenance of airway
Co morbidities
Associated syndromes
Sharing area of intervention with the surgeon
Non availability of nasal route
Paediatric age group Postoperative complications
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 6/67
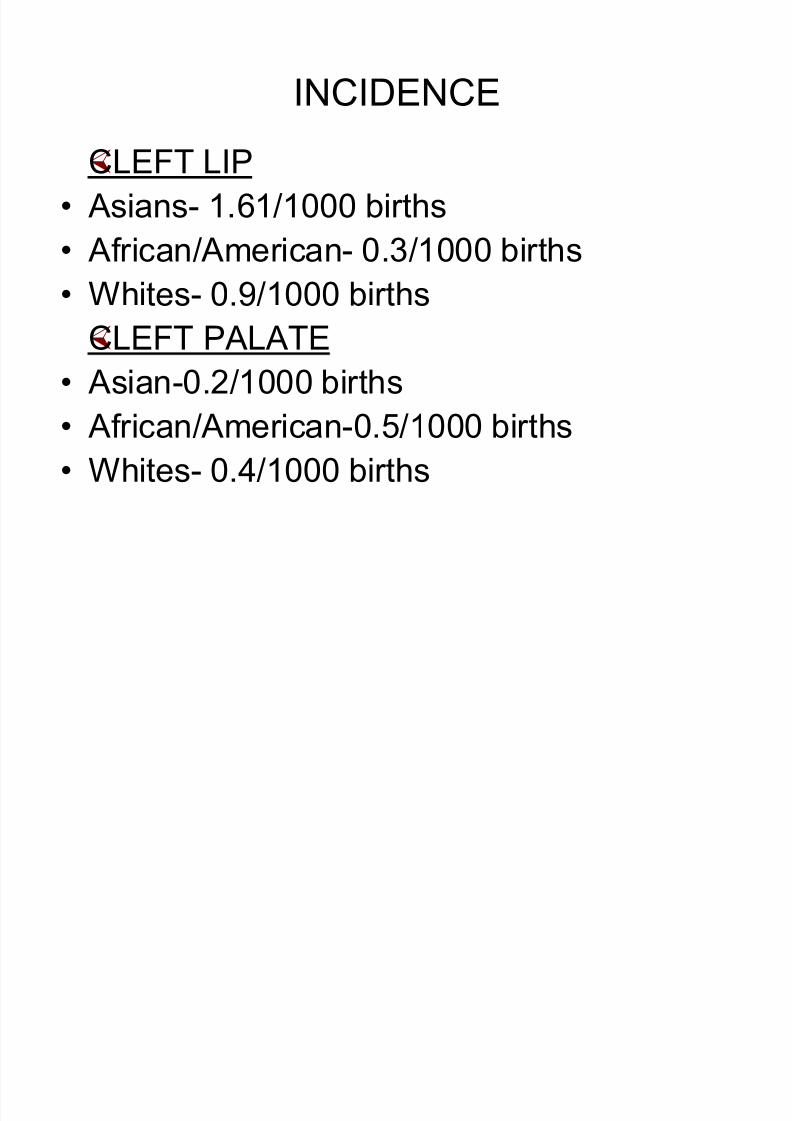
INCIDENCE
CLEFT LIP
Asians- 1.61/1000 births
African/American- 0.3/1000 births
Whites- 0.9/1000 births
CLEFT PALATE
Asian-0.2/1000 births
African/American-0.5/1000 births
Whites- 0.4/1000 births

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 7/67
INCIDENCE
Cleft palate more in females than males
Combination of cleft lip/palate-more in males
Cleft lip more in males
Left sided common as compared to right
Many complex classifications have been devised
cleft can involve the lip, alveolus, hard palateand / or soft palate
Complete or Incomplete,
Unilateral or Bilateral.
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 8/67
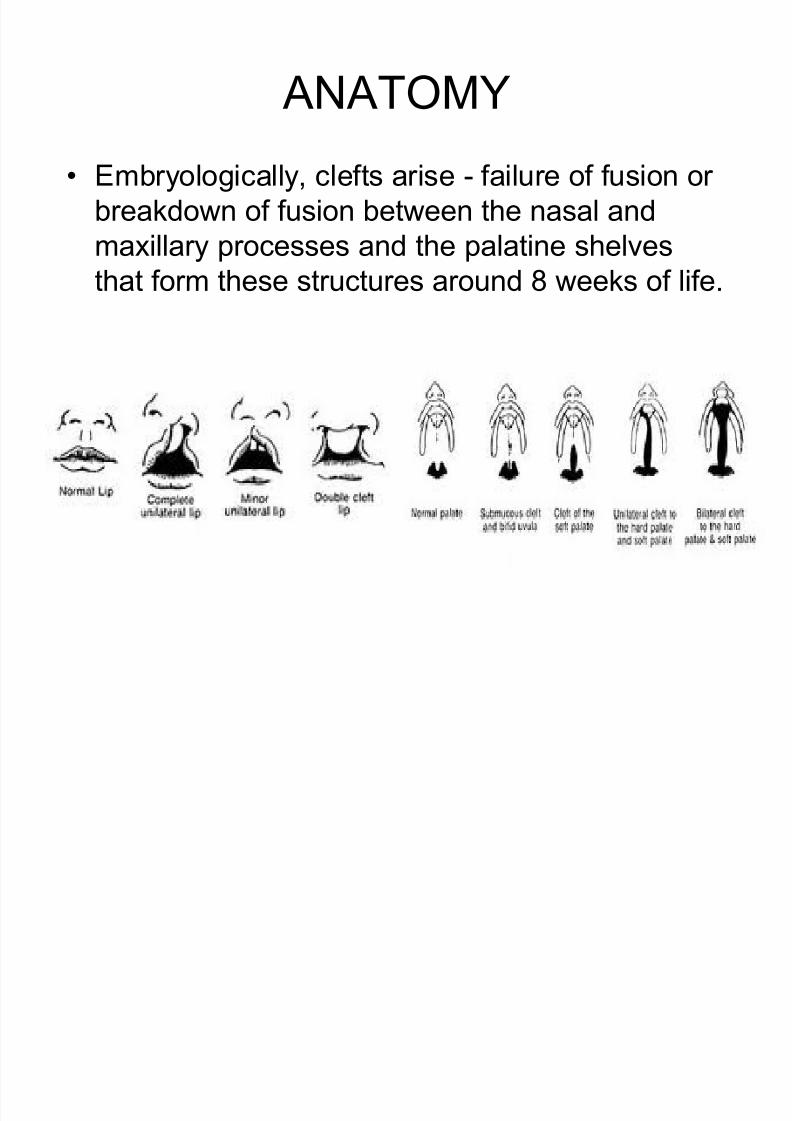
ANATOMY
Embryologically, clefts arise - failure of fusion or
breakdown of fusion between the nasal and
maxillary processes and the palatine shelves
that form these structures around 8 weeks of life.
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 9/67
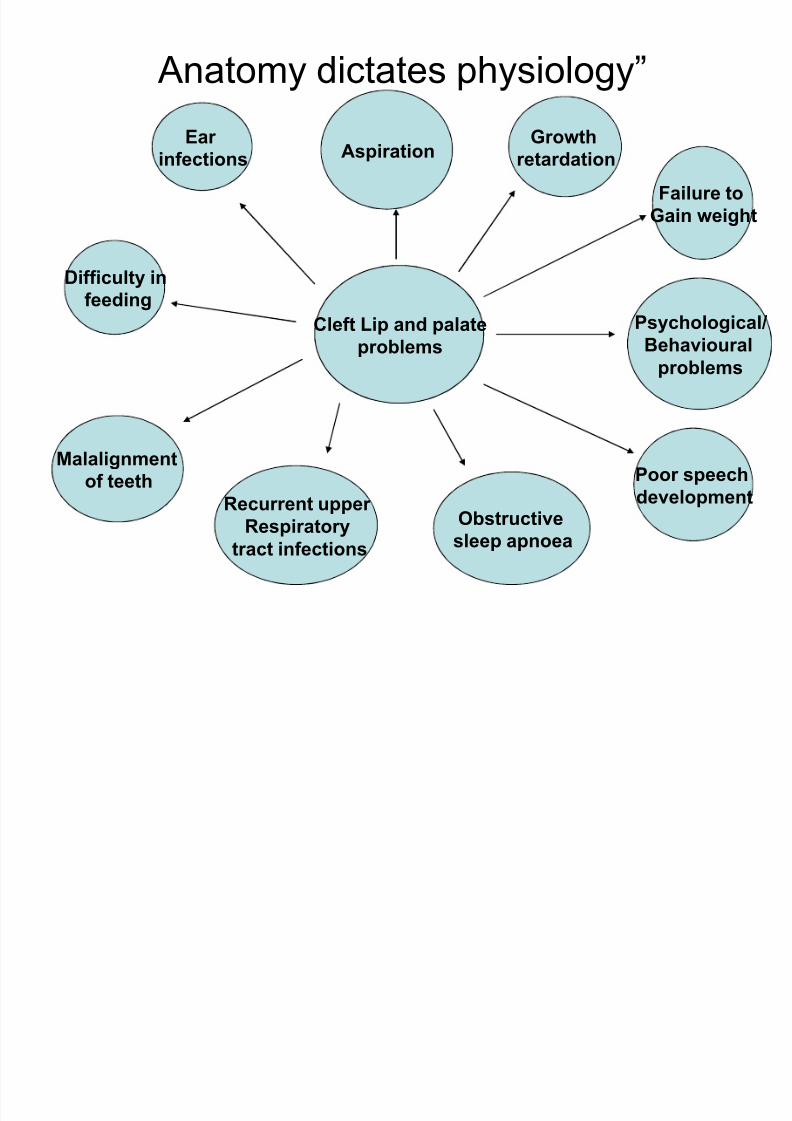
³ Anatomy dictates physiology´
Cleft Lip and palate
problems
Failure to
Gain weight
Poor speech
development
Malalignment
of teeth
Difficulty infeeding
Ear infections
Recurrent upper
Respiratory
tract infections
GrowthretardationAspiration
Obstructive
sleep apnoea
Psychological/
Behavioural
problems

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 10/67
TIMING OF SURGICAL REPAIR
Surgical repair of a cleft lip - 3 months onwards
of age for cosmetic reasons
Trend to operate in the neonatal period in
Western countries. (lip adhesion)
Correcting the defect early ± popular with
parents as it facilitates bonding and feeding.
Late repair- Anaesthesia relatively safe Drawbacks- Negative impact on growth and
development
Speech, hearing, psychology and performance
at school

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 11/67
TIMING OF SURGICAL REPAIR
Cleft palate repair - Balance between poor facial growth with an early repair/ poor speechdevelopment with a repair after the age of 1
year. Usually done ± after 6 months of age in
developed countries.
Cleft lips and palates - often done much later in
developing countries due to non availability of atrained anesthesiologist
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 12/67
PREOPERATIVE EVALUATION
In collaboration with a paediatrician Standard preoperative history
Thorough examination
Special care to assess A detailed family history
Birth history
Allergy to drugs Previous exposure to
anaesthesia

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 13/67
PREOPERATIVE EVALUATION
(CONTD)
Peculiarity of the defect
Previous repairs done
Associated anomalies and problems Associated complications
Psychological issues
DETAILED AND THOROUGHEVALUATION OF AIRWAY
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 14/67
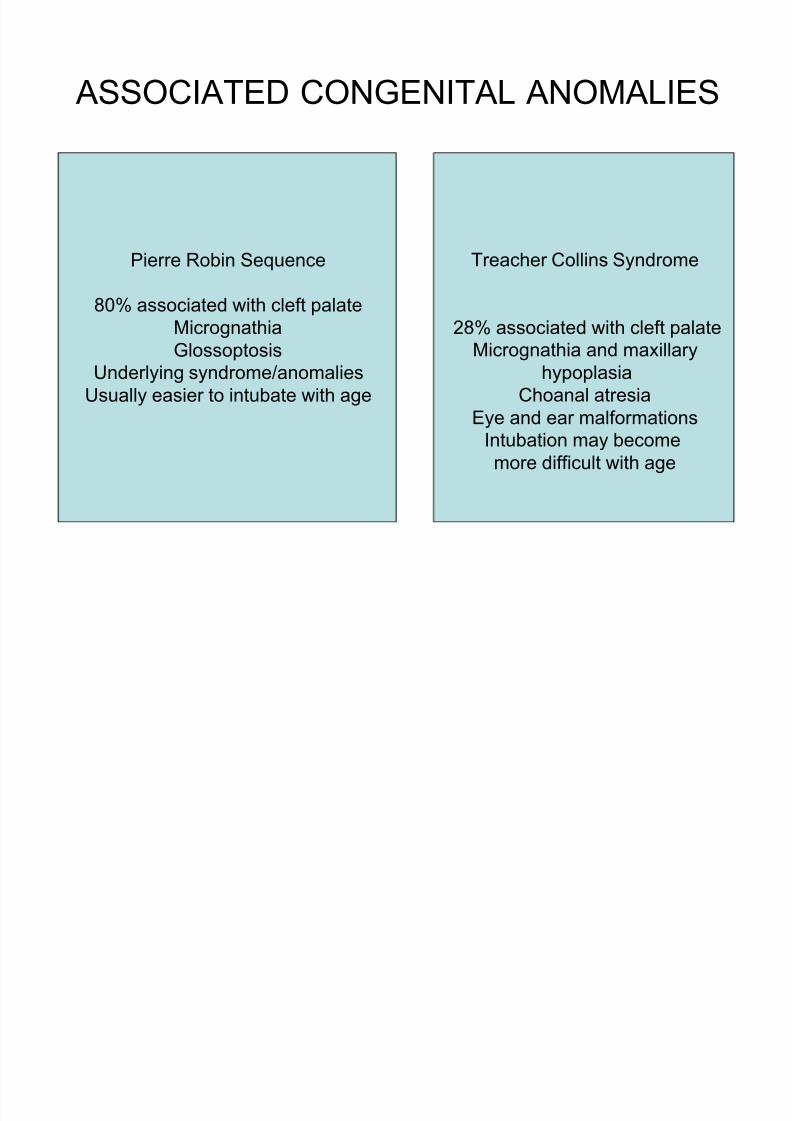
ASSOCIATED CONGENITAL ANOMALIES
Pierre Robin Sequence
80% associated with cleft palate
Micrognathia
Glossoptosis
Underlying syndrome/anomalies
Usually easier to intubate with age
Treacher Collins Syndrome
28% associated with cleft palate
Micrognathia and maxillary
hypoplasia
Choanal atresia
Eye and ear malformationsIntubation may become
more difficult with age

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 15/67
PIERRE ROBIN SYNDROME

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 16/67
TREACHER COLLINS SYNDROME

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 17/67
ASSOCIATED SYNDROMES(CONTD)
Hemifacial Microsomia
Hemifacial
and mandibular hypoplasia
Cervical spine abnormalities
Ear and eye abnormalities
Intubation may become
more difficult with age
Velocardiofacial Syndrome
Microcephalymicrostomia
Flat nasal bridge
small ears
short stature
Immune deficiency
congenital cardiac disease
Laryngeal anomalies
tracheal anomalies

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 18/67
ASSOCIATED SYNDROMES(CONTD)
Stickler Syndrome
Progressive connective
tissue disorder
Micrognathia and
flat face
Eye, ear and joint
abnormalitiesCongenital cardiac disease
Down Syndrome
Microstomia
relative macroglossia
Epicanthic folds
simian crease
Congenital cardiac
disease Atlantoaxial subluxation
and instability
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 19/67
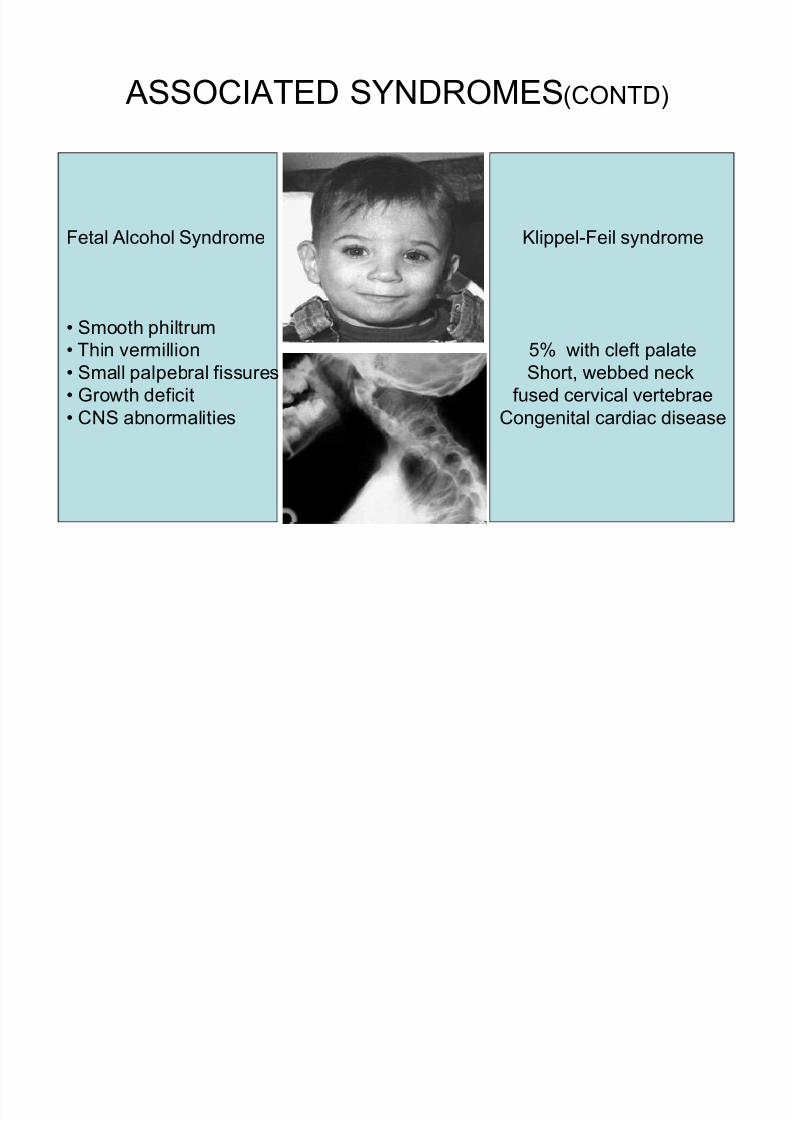
ASSOCIATED SYNDROMES(CONTD)
Fetal Alcohol Syndrome
Smooth philtrum
Thin vermillion
Small palpebral fissures
Growth deficit
CNS abnormalities
Klippel-Feil syndrome
5% with cleft palate
Short, webbed neck
fused cervical vertebrae
Congenital cardiac disease

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 20/67
PAEDIATRIC AGE-GROUP
Different airway anatomy
Obligate nose breathers
Immature organ functions
Less organ reserve
Reduced cardiac calcium stores
Meticulous fluid balance Immature temperature regulation
Susceptibility to depressant effects of anaesthetic drugs

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 21/67
CHRONIC RHINORRHOEA
.
Common in children with cleft palate
Reflux into the nose during feeds.
Distinguish from active infection - surgery can bepostponed
Preoperative antibiotics - low grade nasal infections
1) Reduces - frequency of postoperative pyrexial illnesses.
2) Reduces - post op respiratory complications
3) Prevents spread of infection intracranially-handling of tissues in the vicinity of cranium
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 22/67
UPPER RESPIRATORY TRACT
INFECTION
ALWAYS INFORM THE SURGEON OF INCREASED
RISKS
Decision to proceed with surgery/anaesthesia-depends
on various factors Can be a prodrome of a serious illness/simple viral
infection
Child with URI-increased risk of Atelectasis
Laryngospasm
Bronchospasm
Postintubation croup
Pneumonia
Episodes of Desaturation

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 23/67
CHRONIC UPPER AIRWAY
OBSTRUCTION
Parents will give H/O
Snoring or obvious airway obstruction during
sleep.
Apnoea during feeds
Prolonged feeding time
Failure to thrive due to an inability to coordinate
feeding and breathing at the same time. Afraid of letting the child sleep alone
Child sleeps comfortably when prone

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 24/67
OBSTRUCTIVE SLEEP APNOEA SYNDROME
Disorder of breathing during sleep
Chronic upper airway obstruction/intermittent
complete obstruction
Abnormality of central respiratory control.
Risk factors-craniofacial abnormalities,
neuromuscular abnormality, adenotonsillar
hypertrophy
Sensitive to respiratory depressant effects of anaesthetic agents, benzodiazepines, opioids
Prone for cor pulmonale, post operative apnoea
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 25/67
RIGHT VENTRICULAR HYPERTROPHY
COR PULMONALE
Results from recurrent hypoxia due to airway
obstruction
Highly sensitive to fluid load
Avoid hypoxia, hypercarbia, acidosis and
hypothermia
Keep ionotropes ready Avoid causes increasing sympathetic activity

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 26/67
NUTRITION AND HYDRATION
Potential difficulty with feeding ± Assess
State of hydration
Overall growth
Nutritional anemia
³Haemoglobin concentration-as a guide´
Physiological anaemia - between 3 and 6
months of age. Ideally Hb >10g/dl.
Malnutrition and anaemia-delay wound healing
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 27/67
RULE OF µTEN¶
A patient with
1) Hb- 10gm%
2) WBC count </= 10,000/cumm3) Weight > 10 pounds
4) Age > 10 weeks

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 28/67
INVESTIGATIONS
Laboratory work - CBC, platelets, PT/PTT (for cleftpalate repair), KFT, LFT
CXR/ECG not necessary if the history and heart/lung
exam - normal
Consider bank blood availability - large cleftpalate repairs
Complete cardiac evaluation ± associated cardiacdefects
Relevant radiographs ± evaluation of airway

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 29/67
PREOPERATIVE PREPARATION
Desired goals
Afebrile
Optimal cardio respiratory condition
URI resolved as much as possible Banked blood arranged - if required
NPO status as per protocol
Informed consent for the surgical procedure obtained bysurgeon
Discussion of general anesthesia, including potentialrisks and complications, by the anesthesiologist withpatient's parents

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 30/67
PREOPERATIVE PREPARATION(CONTD)
NPO status for elective cases
2 hours - clear liquids (water, apple juice)
for all ages
4 hours - solids and milk/formula up to 6
months old
6 hours for solids, non-clear liquids for all
children 6 months or older

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 31/67
PREFERRED SCHEDULE
Youngest and smallest patients - early in theday.
Cleft palates, revisions, and other difficultcases earlier than others
Avoid being overenthusiastic while postingcases-per day/surgeon/2-3 cases
Remember-Anaesthetic morbidity increases asduration of period under anaesthesiaincreases

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 32/67
PREMEDICATION
Oral midazolam 0.25-0.5 mg/kg 1/2 hour prior to
induction if >8 kg; otherwise, no premedication.
Recognize that premedication may cause the
patient to be drowsy
To be given in preanaesthesia care unit
preferably with child in mothers lap
Should be avoided in patients comingfor secondary repairs like Abbe flap,
pharyngoplasty, tongue flap etc
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 33/67
PREPARATION OF ANESTHETIC
EQUIPMENT
Full vaporizer
Functioning suction machine/
catheters Full oxygen tanks
ECG and pulse oximetry
Capnography (end-tidal co2) if available
Temperature-monitoring device Appropriate circuit to give positive pressure
ventilation (circle or Jackson-Rees)

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 34/67
PREANAESTHETIC PREPARATION(CONTD)
Appropriate sizes of blood pressure cuffs, ETT(RAE) south pole, largyngoscope blades,masks, Oral/Nasal airways, LMA.
Secure 22 / 20G IV catheters 60 drop/cc IV tubing buretrol chamber drip
(Paediatric)
Lactated Ringers or Normal Saline IV solutions
Warm blankets Anesthetic record with continuous recording of
vital signs (every 5 minutes or less)

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 35/67

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 36/67
INTRAOPERATIVE MEDICATIONS
Inhalational agent
Sevoflurane
HalothaneIsoflurane
Muscle relaxants
Succinyl choline
Vecuronium
Atracurium
RocuroniumIV induction agent
Propofol
Thiopental
Ketamine
Antisialogogue, vagolytic
Atropine
Glycopyrrolate
AntibioticAnalgesics
Fentanyl
morphine
Reversal agents
Edrophonium
NeostigmineNaloxone

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 37/67
INTRAOPERATIVE MEDICATIONS
Rectal acetaminophen
Steroids
(1 or 2 doses only)
Bronchodilators
Aminophylline
Terbutaline
Albuterol inhaler
Resuscitation medications
Epinephrine
AtropineCalcium
Bicarbonate
Glucose
Banked blood

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 38/67
INDUCTION OF ANAESTHESIA
VARIOUS METHODS
FOR
INDUCTION OF
ANAESTHESIA
Inhalational mask
inductionwith spontaneous
ventilation and IV after
Loss of
consciousness
IV induction if child is older
and cooperative
IM induction if child uncooperative
and apprehensive
INHALATION
INDUCTIONWITH
IV SECURED, IN
DIFFICULT AIRWAY

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 39/67
INTUBATION AND MAINTENANCE
Assure ability to ventilate by mask withoutmuscle relaxants
Intubation after Preoxygenation with 100% O2
ETT size - air leak at 15-30 cm H2O pressure Observe and auscultate
Equal bilateral chest movement
Presence of end-tidal CO2
Secure ET tube properly
Maintenance-O2/N2O/inahlational agent

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 40/67

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 41/67

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 42/67
INTRAOPERATIVE MAINTENANCE
Beware of ETT movement during
patient's head is being positioned
retractors are being placed.
Beware of tube occlusion if mouth retractor is opened completely.
Beware of throat pack placement and assure removal beforeextubation
Recommend intraoperative suture tag placement on side of patient'scheek and assign OR personnel to remind of throat packplacement/removal

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 43/67
TUBE PLACEMENT

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 44/67
HANDING OVER
Handing over the patient to the surgeon
Crucial step- as anesthesiologist now losesdirect access to the airway
Ensure Correct placement/fixation of ET tube
Access to IV line
Fixation of monitoring leads
Proper and tight connections of breathing circuit
Optimum position of the patient

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 45/67
INTRAOPERATIVE MAINTENANCE(contd)
Prefer inhalational agent and O2/N2O or O2/air
for maintenance
Record vital signs (BP, HR, RR, O2 sat, Temp,
and ET CO2 if avail.) every 5 minutes
Carefully monitor intraoperative blood loss, fluid
administration and urine output for prolongedsurgeries
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 46/67
ADRENALINE INFILTRATION
Local anaesthetic with adrenaline infiltration
Should be done carefully after negative
aspiration
Dose 10microgm/kg
If infiltration causes tachycardia
Hypovolemia/Hypercapnia
Light plane of anaesthesia Inhalational agents sensitize myocardium to
exogenous catecholamines

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 47/67
COMPLICATIONS
General anaesthesia ±can cause life threateningcomplications
Common in infants and neonates
Careful selection of patients
Anticipation of problems
Thorough preparation to handle the difficulties
Early recognition
Prompt treatment Inform and discuss with surgeon
As far as possible follow protocols

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 48/67
INTRAOPERATIVE COMPLICATIONS
Inability to secure airway
Airway trauma
Desaturation
Surgeon and anaesthetist share the area of intervention
Kinking of tube
Tube dislocation/disconnection
Tube block
Accidental extubation

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 49/67
INTRAOPERATIVE COMPLICATIONS(CONTD)
Hypothermia
Excessive bleeding
Hypercapnia
Hypoxia
Equipment failure
Drug allergies
Cardiac Arrythmias
Hypotension
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 50/67
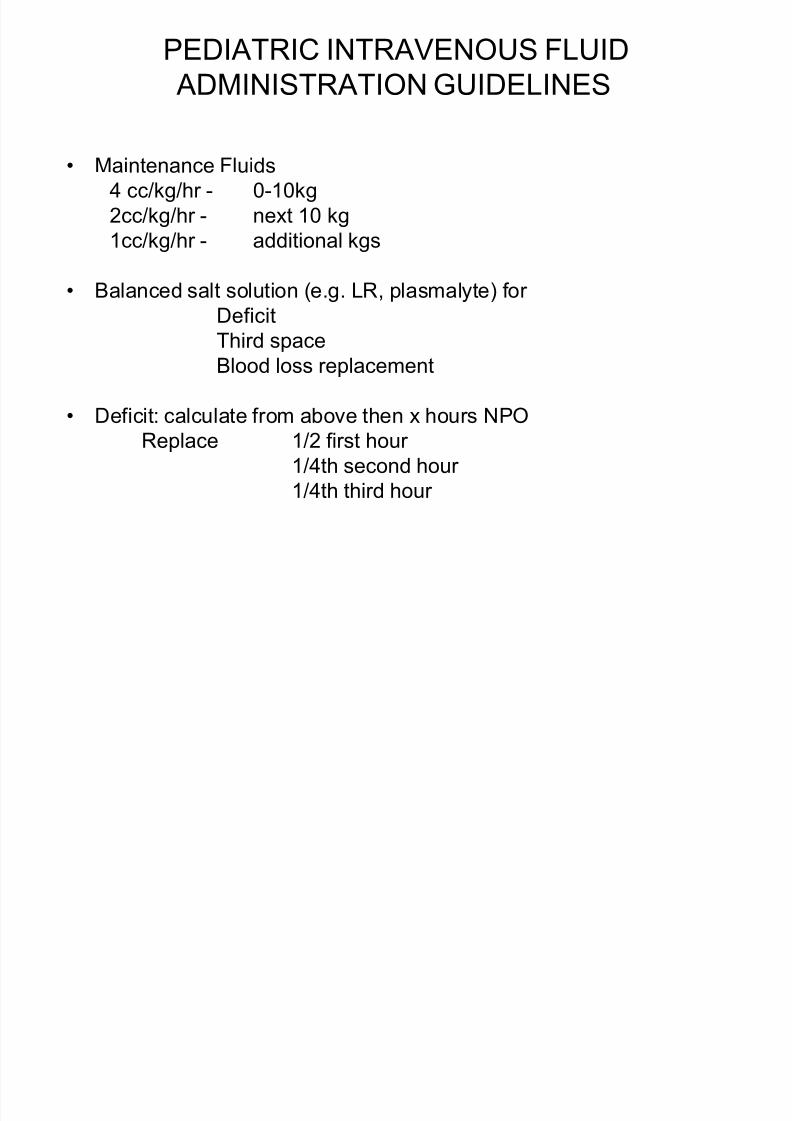
PEDIATRIC INTRAVENOUS FLUID
ADMINISTRATION GUIDELINES
Maintenance Fluids
4 cc/kg/hr - 0-10kg
2cc/kg/hr - next 10 kg
1cc/kg/hr - additional kgs
Balanced salt solution (e.g. LR, plasmalyte) for Deficit
Third space
Blood loss replacement
Deficit: calculate from above then x hours NPOReplace 1/2 first hour
1/4th second hour
1/4th third hour

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 51/67
PEDIATRIC INTRAVENOUS FLUID
ADMINISTRATION GUIDELINES
Third Space Losses
2-4 cc/kg/hr minor procedure (lip scar revision)
4-6 cc/kg/hr moderate procedure (bilateral lip repair)
8-10cc/kg/hr major procedure (large cleft palate repair)
Blood Loss
Replace 3x blood loss with balanced salt solution
10cc/kg/hr PRBCs raises HCT 5%
Estimated Blood Volume
Infant 80 ml/kg1-3 years 75 ml/kg
3-6 years 70 ml/kg
>6 years 65 ml/kg
A well-hydrated patient will have less post operative nausea

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 52/67
EXTUBATION IN OR
Ensure
Throat pack removed
Remove throat pack before surgeon places suture for- Abbe flap,tongue flap
Placement of tongue suture (post-palate/pharyngoplasty) No bleeding
Strong suction available
Patient breathing 100% O2 spontaneously
No residual narcotization/neuromuscular block
Oxygen saturation >97% or better
Surgeon should be present scrubbed and immediately available inOR
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 53/67
EXTUBATION IN OR
Tracheostomy instrument tray available
Gently suction anterior nares, oropharynx if possible-but beware suture lines and wounds
As far as possible-surgeon should perform suctioning
Patient should be
awake
opening eyes
spontaneous purposeful movement
able to open mouth and/or cough Retain ability to give 100% O2 by positive pressure mask
Instrument table remains set up

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 54/67
EXTUBATION
Consider delayed extubation
Suspecting airway edema
Pulmonary edema Severe Bronchospasm
Impossible to re-intubate e.g abbe flap,
pharyngeal flap, tongue flap Hemodynamic instability

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 55/67
COMPLICATIONS DURING EXTUBATION
Laryngospasm
Bronchospasm
Hypoxia
Arrythmias Bleeding
Airway obstruction
Hypothermia
Residual anaesthetic drug effects
Need to reintubate
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 56/67
TRANSPORT OF PATIENTS
Patient fully conscious
Responding well to verbal commands
Hemodynamically stable
Ensure haemostasis Spontaneously breathing well
Maintaining SpO2>97% on
room air
Transport in lateral position
Accompanied by anaesthetist
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 57/67
TRANSPORT TO
PACU
Handing over to ICU personnel
with detailed intraop information
Clear and detailed post operativeinstructions
Attach to monitors immediately
O2 by mask Parents to be involved in post op care

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 58/67
POST OP OBSERVATION
Nurse in lateral position with head low
Vital signs ± stable
Strict vigilance for airway and breathing
No evidence of bleeding.
Vital signs and wound check- every hour or more frequently for the first twelve
hours.
Adequate pain relief Treat nausea/vomiting

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 59/67
POST OPERATIVE CARE
Clear liquids PO to be offered initially
Increase oral intake as per tolerance
Intravenous fluids - continue until the patient is takingliquids well orally.
Recommend high visibility bed
Patient: nurse ratio at least 3:1
Established Emergency protocol
Monitor and treat problems as they arise
Chain of communication and command clearlydelineated

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 60/67
POST OPERATIVE PAIN CONTROL
Intravenous opioids
Oral analgesics-NSAIDS
Rectal suppositories
Infraorbital nerve block
Local anaesthetic with adrenaline infiltration
locally

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 61/67
POST OPERATIVE MANAGEMENT
Ability to access anesthesiologist andsurgeon for airway management postoperatively if needed
Surgeon immediately available to answer and address questions regardingpostoperative wound care and drainage
Family of patient to be fully informed of allperioperative events, including success or failure of procedure performed.
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 62/67
POST OPERATIVE CARE
TRAINED
NURSE
ANAESTHETIST
PARENTS
SURGEON
PATIENT
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 63/67
POST OPERATIVE COMPLICATIONS
Airway obstruction ± blood/secretions/tongue fall/airwayedema
Periodic suctioning
Ensure proper position
Ensure tongue suture in place
Nebulisation and hydration
Post operative apnoea-commonly seen in infants
Keep equipment for mask ventilation ready Avoid opioids
Strict SpO2 monitoring (sleeping pulse oximetry)

8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 64/67
POST OPERATIVE COMPLICATIONS(CONTD)
Desaturation- Easy respiratory fatigability
Nose block
Hypoventilation residual effects of
anaesthetic drugs Bleeding
Hyper/hypothermia
Pulmonary edema
Accidental extubation
Aspiration
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 65/67
CONCLUSION
Anaesthesia for cleft lip and palate repair with hospital-based cleft care team is relatively safe
Recommend general anaesthesia for most cases
Local anaesthesia for smaller defects in older
children/adults
Anaesthetist should be
Trained in Paediatric anaesthesia and PALS
Able to manage difficult airway
Able to manage post operative complications Able to understand pathophysiology of clefts, associated
complications, disorders especially syndromic patients
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 66/67
CONCLUSION (CONTD)
A well trained, skilled and coordinated team with good
communication and with implementation of
recommended protocols can provide safe
anaesthesia/surgery to this subset of children, making
and engraving this experience as a smooth sail not onlyfor the patients but also for the parents
8/3/2019 Anaesthetic Considerations for Cleft Surgeries
http://slidepdf.com/reader/full/anaesthetic-considerations-for-cleft-surgeries 67/67