anabolic exercise in haemodialysis patients: a randomised controlled pilot study
TRANSCRIPT

ORIGINAL ARTICLE
Anabolic exercise in haemodialysis patients: a randomisedcontrolled pilot study
Danielle L. Kirkman & Paul Mullins &
Naushad A. Junglee & Mick Kumwenda &
Mahdi M. Jibani & Jamie H. Macdonald
Received: 14 October 2013 /Accepted: 4 March 2014# Springer-Verlag Berlin Heidelberg 2014
AbstractBackground The anabolic response to progressive resistanceexercise training (PRET) in haemodialysis patients is unclear.This pilot efficacy study aimed to determine whether high-intensity intradialytic PRET could reverse atrophy and conse-quently improve strength and physical function inhaemodialysis patients. A second aim was to compare anyanabolic response to that of healthy participants completingthe same program.Methods In a single blind controlled study, 23 haemodialysispatients and 9 healthy individuals were randomly allocated toPRET or an attention control (SHAM) group. PRET complet-ed high-intensity exercise leg extensions using novel equip-ment. SHAM completed low-intensity lower body stretchingactivities using ultra light resistance bands. Exercises werecompleted thrice weekly for 12 weeks, during dialysis in thehaemodialysis patients. Outcomes included knee extensor
muscle volume by magnetic resonance imaging, knee exten-sor strength by isometric dynamometer and lower body testsof physical function. Data were analysed by a per protocolmethod using between-group comparisons.Results PRET elicited a statistically and clinically significantanabolic response in haemodialysis patients (PRET—SHAM,mean difference [95 % CI]: 193[63 to 324]cm3) that was verysimilar to the response in healthy participants (PRET—SHAM, 169[−41 to 379]cm3). PRET increased strength inboth haemodialysis patients and healthy participants. In con-trast, PRET only enhanced lower body functional capacity inthe healthy participants.Conclusions Intradialytic PRET elicited a normal anabolicand strength response in haemodialysis patients. The lack ofa change in functional capacity was surprising and warrantsfurther investigation.
Keywords Weight lifting .Wasting syndrome . Chronickidney failure . Haemodialysis
1 Introduction
Muscle atrophy is frequently observed with haemodialysis(HD) affecting 18–80 % of patients [1–5]. Muscle wastingin this population is a noteworthy problem as it independentlypredicts morbidity and mortality [6]. Strong positive correla-tions have been revealed between muscle quantity andstrength, oxygen extraction at the muscle and functional ca-pacity in HD patients [2, 3, 7, 8], suggesting that musclewasting also reduces physical functioning. Thus, musclewasting indirectly affects quality of life (QoL).
Disuse remains a consistently cited mechanism of atrophy[5] that is rarely addressed by standard routine care. Progres-sive resistance exercise training may be a safe, cost-effective,anabolic intervention, having already been implemented in
D. L. Kirkman :N. A. Junglee : J. H. MacdonaldSchool of Sport, Health and Exercise Sciences, Bangor University,Bangor, Wales, UK
D. L. Kirkman :N. A. Junglee :M. M. JibaniDepartment of Nephrology, Gwynedd Hospital, Betsi CadwaladrUniversity Health Board, Bangor, Wales, UK
P. MullinsBangor Imaging Centre, School of Psychology, Bangor University,Bangor, Wales, UK
M. KumwendaDepartment of Nephrology, Glan Clywd Hospital, Betsi CadwaladrUniversity Health Board, Bangor, Wales, UK
D. L. Kirkman (*)College of Health Sciences, Department of Kinesiology and AppliedPhysiology, University of Delaware, 504 S College Ave, Newark,DE 19716, USAe-mail: [email protected]
J Cachexia Sarcopenia MuscleDOI 10.1007/s13539-014-0140-3

other catabolic diseases [9, 10]. However, despite positivelyaffecting anabolic markers such as mitochondrial biogenesis,skeletal muscle mRNA, muscle IGF-1 protein and musclefibre cross-sectional area across all stages of chronic kidneydisease [11, 12] in HD patients, the efficacy of resistanceexercise on muscle quantity, as assessed using recommendednutritional endpoints [13], remains uncertain. Previously, onlytwo intradialytic resistance exercise interventions have shownbeneficial effects on muscle atrophy [14, 15] whilst the ma-jority of studies have failed to elicit an anabolic response inthis patient population [15–17].
The reason for this discouraging lack of an anabolic responseto resistance exercise inHDpatients is unclear [5]. Unfortunately,previous resistance exercise interventions have generally lackedattributes (such as sufficient overload and progression) necessaryto elicit an anabolic effect [18, 19]. Thus, before resistanceexercise can be investigated further as an adjunctive therapy forHD patients, a program meeting the guidelines deemed mosteffective for anabolism must be implemented. Alternatively, HDpatients present with hypogonadism [20], insulin resistance [21]and a perturbed insulin-like growth factor/growth hormone axis[22], all of which are required to activate signalling pathwaysresponsible for protein synthesis. Thus, a comparison betweenthe anabolic response in HD patients and healthy controls wouldalso be beneficial.
Consequently, the aim of this study was to determine whethera novel intradialytic progressive resistance exercise training tech-nique, ensuring sufficient overload and progression for anabo-lism, could safely reverse atrophy and improve muscle strengthand physical function in HD patients. A secondary aim was tocompare any anabolic response to that of healthy participantscompleting the same program. It was hypothesised that progres-sive resistance exercise training would significantly increasemuscle volume, strength and physical function in HD patientsas compared to an attention control group, and that this responsewould be similar to that observed in healthy participants.
2 Methods
2.1 Study design
In this two-centre, single blind, pre-test post-test, controlledtrial (clinicaltrials.gov: NCT01007838), participants were ran-domly allocated to receive progressive resistance exercisetraining (PRET) or a sham exercise attention control interven-tion (SHAM) using opaque envelopes in a 1:1 manner, strat-ified by disease, gender and centre (by DK).
2.2 Participants
Ethical approval was provided by Betsi Cadwaladr UniversityHealth Board Ethics Committee and Bangor University.
Participants provided written informed consent. Haemodialysispatients were recruited from two renal units in NorthWales, UK.Inclusion criteria required patients to be diagnosed with stage 5chronic kidney disease receiving HD three times per week.Patients were excluded if they were below 18 years of age, hadreceived HD <3 months, required support for ambulation of>50m, presentedwith haemoglobin levels <11 g dL−1, presentedwith neuromuscular or catabolic conditions, received any ana-bolic treatment in the preceding 3 months, had any uncontrolledmedical condition, presented with contraindications to take partin exercise or were unable to provide consent.
Sedentary healthy participants were recruited from theNorth Wales community using posters placed in communitycentres. Participants were excluded if their general practitionerdeemed the participant to have a contraindication to exercise,had suffered from a catabolic condition or received an ana-bolic or exercise intervention in the preceding 3 months.
2.3 Intervention
PRET groups completed a 12-week resistance training pro-gram three times per week, during routine HD sessions for thepatients and during university visits for the healthy partici-pants. Each session involved a leg press exercise using equip-ment (Fitness Systems, Bolton, UK) designed to fit to the endof a dialysis chair (Stephen H Anatomical New, GardhenBilance, Italy). As obtaining large training loads using tradi-tional plate loading machines was unsafe and impractical inthe renal unit, leg press equipment was designed to utilise aseries of resistance bands providing a maximum resistanceequivalent to 200 kg. During training, participants completedthree sets of eight to ten repetitions at 80 % of their predicted1RM (determined from an assessment of their 5RM [23] toreduce the risk of injury associated with 1RM testing in thispopulation [24]) with 2-min rest period between sets. Basedon resistance exercise biology, this protocol is recommendedfor muscle hypertrophy [18, 19]. When 10–12 repetitionscould be completed at a rating of perceived exertion below15 (hard), 1RM was re-determined and the training loadincreased accordingly.Weekly training volumewas calculatedas kg per lift × lifts per session × sessions per week. TheSHAM group carried out a series of unprogressive stretchesusing an ultra-light Thera-Band (Hygenic Corporation, Ak-ron, Ohio).
2.4 Outcomes
Outcome measures were assessed pre and post the 12 weekintervention by assessors blinded to group allocation.
Thigh muscle volume The primary outcome measure wasthigh muscle volume determined by magnetic resonance im-aging. T1 and T2 images were obtained in the axial plane from
J Cachexia Sarcopenia Muscle

the femoral tibial joint line to the top of the femoral head (3TPhilips Achieva; Philips Healthcare, Best, The Netherlands).The image parameters were as follows: T1 acquisition matrixof 236×236, FOV 475×475×198, voxel size 2×2 mm2, TE2.3 ms, TR 4ms, slice thickness 5mm, acquisition time 3min.The muscle cross-sectional area of 12 evenly spaced axialslices [25] was determined using image processing software(version 4.x, Osirix, Pixmeo, Geneva). The truncated coneformula was applied to calculate muscle volume. The test re-test reliability of this protocol expressed as a coefficient ofvariation (CV) was 1.5 % with an interclass correlation(ICC3,k) of 0.997.
Muscle strength Isometric bilateral knee extensor strengthwas measured using an isometric chair (Bodycare Products,Southam, UK) equipped with a load cell (615S, TedeaHuntleigh, Vishay, Basingstoke, UK), resolved and convertedto force in Newtons by a data acquisition and analysis system(PowerLab 16SP; AD Instruments PTY, Colorado Springs,CO). Three maximal voluntary contractions were performedwith a minute rest between each. The highest value was usedfor analysis. The ICC3,k of this was reported as 0.960 (26).
Physical function Physical function tests included the 30-s sitto stand test, a measure of lower body strength (ICC3,k=0.89);the 8-ft get up and go test, a measure of speed and agility(ICC3,k=0.95) and the 6-min walk test, a measure of aerobiccapacity (ICC3,k=0.94) [27].
Harms Information on harms was collected at the beginningand end of each session via interview and, in HD patients, bychecking dialysis treatment records. Specifically, informationon musculoskeletal injuries, cardiovascular events, acute hy-potension and hypertension and access complications wererecorded.
Unexpected and serious harms were collected as they oc-curred, during the trial period only. Decisions about whetherevents were attributable to the intervention were made by un-blinded clinicians.
Quality of life Preliminary data on self-reported quality of life(QoL) were obtained using the Short Form-36 version 2 (SF-36v2) questionnaire [28].
2.5 Statistical analysis
Data were analysed using the Statistical Package for the SocialSciences (version 18; IBM, New York, USA) with statisticalsignificance set at p≤0.05. Weekly training volumes in thePRET groups were compared using a repeated measuresanalysis of variance. For the primary outcome of musclevolume, a minimum important clinical change over 12 weekswas set as 75 cm3, which over a year would equate to a change
of 10 % of thigh muscle volume in healthy individuals. Formuscle volume, knee extensor strength, physical function andQoL data, comparisons of the response between groups wereof primary interest to this efficacy study. Therefore, indepen-dent t tests on change scores were used, analysing data on aper protocol basis. Effect sizes (d) were also calculated forthese comparisons using Cohen’s method, and can beinterpreted as small (0.3), medium (0.5) or large (0.8) [29].Differences in the change scores between groups, along withthe 95 % confidence intervals for these differences were alsocalculated. This three-step approach ensured that the responsecould be compared (i) between PRET and SHAM within theHD patients, (ii) between PRETand SHAMwithin the healthyparticipants and (iii) between HD patients and healthy partic-ipants within the PRET group. Data on harms and compliancewere presented descriptively.
3 Results
3.1 Participants, compliance and training volume
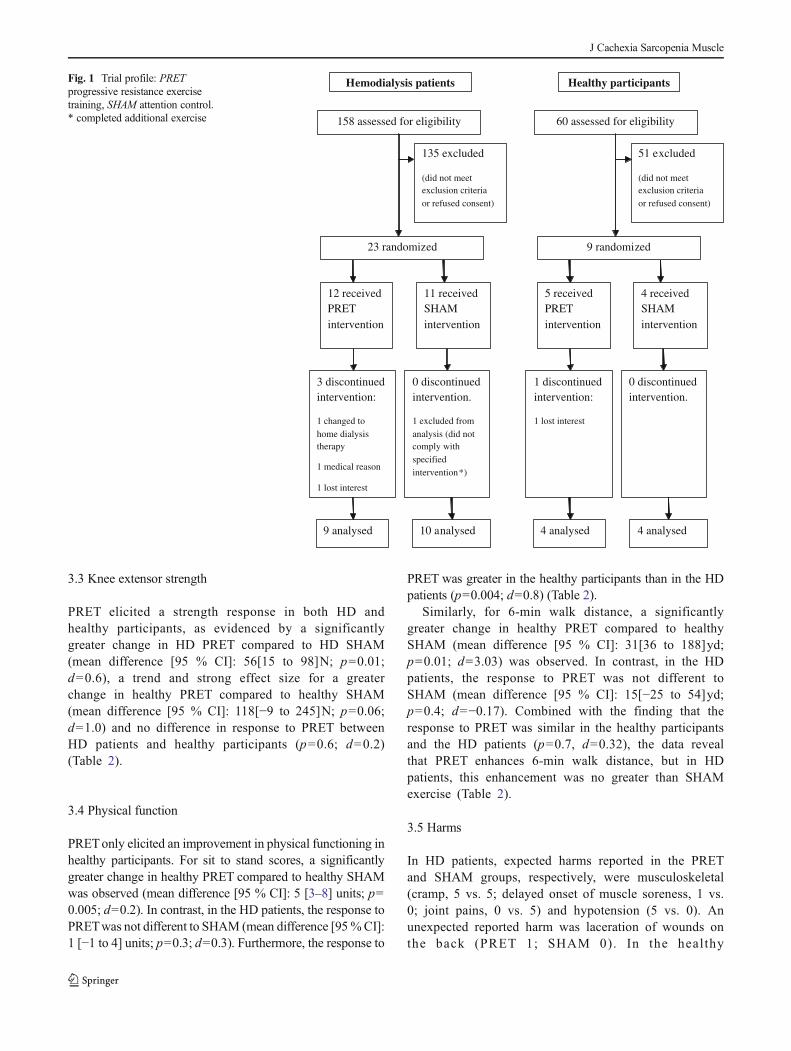
Participant flow through the study is presented in Fig. 1.Participant characteristics are presented in Table 1. There wereno statistical differences between HD patients and healthycontrols for age and body mass index. All HD patient baselinehaematology, biochemistry and dialysis data were within renalassociation recommended ranges (Table 1).
In the PRET groups, training volumes significantly increasedto a similar extent in HD and healthy participants, as evidencedby a significant main effect of time (p=0.03, Fig. 2), a non-significant group × time interaction (p=0.3) and a non-significantmain effect of group (p=0.2). Compliance to PRETwas similarin both HD patients and healthy participants with 94±3 and 93±3 % of training sessions completed, respectively. Reasons formissing any of the 324 offered exercise sessions in theHDPRETgroup were illness (14 sessions), scheduling issues (2 sessions)and dialysis equipment problems (2 sessions). Reasons for miss-ing any of the 180 offered exercise sessions in the healthy PRETgroupwere holidays (8 sessions) and unexplained nonattendance(4 sessions).
3.2 Thigh muscle volume
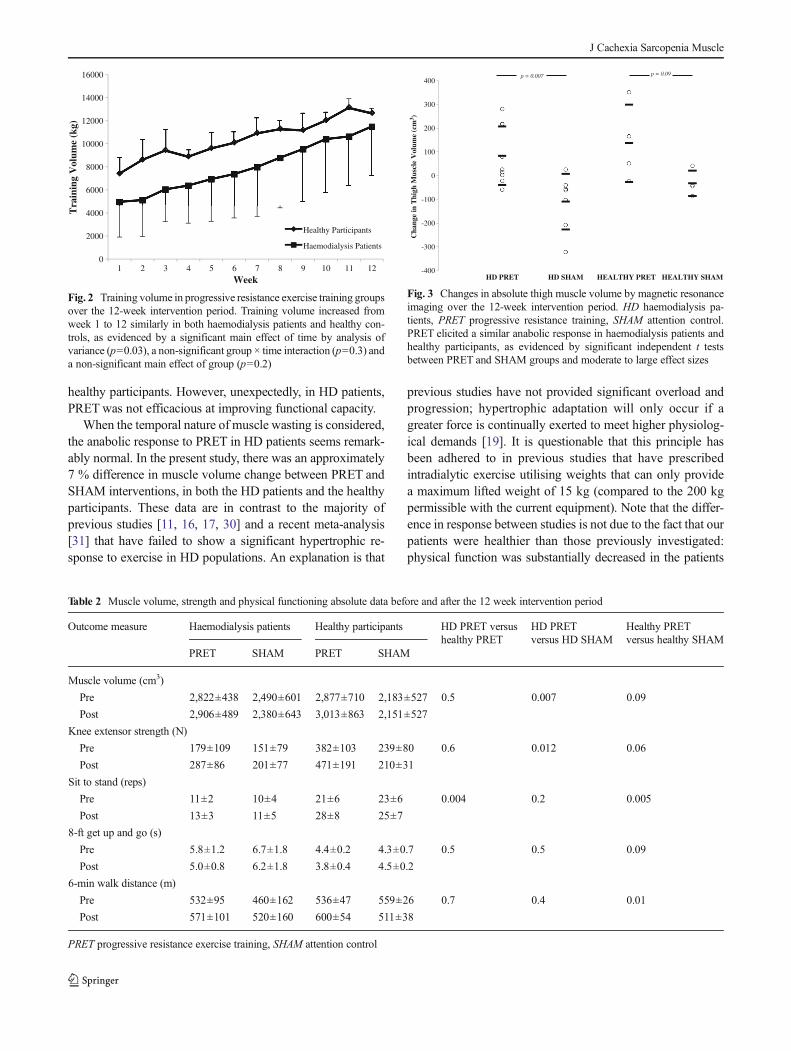
PRET elicited an anabolic response in both HD and healthyparticipants, as evidenced by a clinically and significantlygreater change in HD PRET compared to HD SHAM (meandifference [95 % CI]: 193[63 to 324]cm3; p=0.007; d=0.4), atrend and strong effect size for a greater change in healthyPRET compared to healthy SHAM (mean difference [95 %CI]: 169[−41 to 379]cm3, p=0.1; d=0.2) and no difference inresponse to PRET between HD patients and healthy partici-pants (p=0.5; d=0.1) (Table 2 and Fig. 3).
J Cachexia Sarcopenia Muscle
3.3 Knee extensor strength
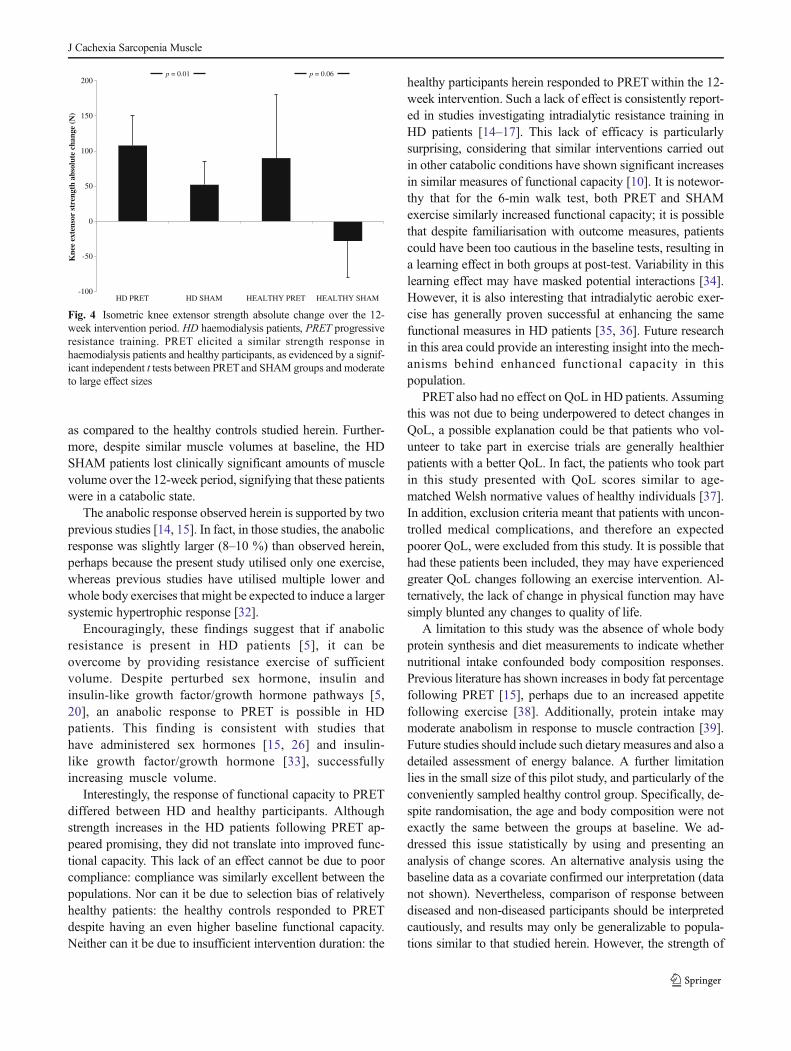
PRET elicited a strength response in both HD andhealthy participants, as evidenced by a significantlygreater change in HD PRET compared to HD SHAM(mean difference [95 % CI]: 56[15 to 98]N; p=0.01;d=0.6), a trend and strong effect size for a greaterchange in healthy PRET compared to healthy SHAM(mean difference [95 % CI]: 118[−9 to 245]N; p=0.06;d=1.0) and no difference in response to PRET betweenHD patients and healthy participants (p=0.6; d=0.2)(Table 2).
3.4 Physical function
PRETonly elicited an improvement in physical functioning inhealthy participants. For sit to stand scores, a significantlygreater change in healthy PRET compared to healthy SHAMwas observed (mean difference [95 % CI]: 5 [3–8] units; p=0.005; d=0.2). In contrast, in the HD patients, the response toPRETwas not different to SHAM (mean difference [95%CI]:1 [−1 to 4] units; p=0.3; d=0.3). Furthermore, the response to
PRET was greater in the healthy participants than in the HDpatients (p=0.004; d=0.8) (Table 2).
Similarly, for 6-min walk distance, a significantlygreater change in healthy PRET compared to healthySHAM (mean difference [95 % CI]: 31[36 to 188]yd;p=0.01; d=3.03) was observed. In contrast, in the HDpatients, the response to PRET was not different toSHAM (mean difference [95 % CI]: 15[−25 to 54]yd;p=0.4; d=−0.17). Combined with the finding that theresponse to PRET was similar in the healthy participantsand the HD patients (p=0.7, d=0.32), the data revealthat PRET enhances 6-min walk distance, but in HDpatients, this enhancement was no greater than SHAMexercise (Table 2).
3.5 Harms
In HD patients, expected harms reported in the PRETand SHAM groups, respectively, were musculoskeletal(cramp, 5 vs. 5; delayed onset of muscle soreness, 1 vs.0; joint pains, 0 vs. 5) and hypotension (5 vs. 0). Anunexpected reported harm was laceration of wounds onthe back (PRET 1; SHAM 0). In the healthy
Hemodialysis patients Healthy participants
4 analysed 4 analysed
1 discontinued intervention:
1 lost interest
0 discontinued intervention.
5 received PRETintervention
4 received SHAM intervention
9 randomized
51 excluded
(did not meet exclusion criteria or refused consent)
9 analysed 10 analysed
3 discontinued intervention:
1 changed to home dialysis therapy
1 medical reason
1 lost interest
0 discontinued intervention.
1 excluded from analysis (did not comply with specified intervention*)
12 received PRETintervention
11 received SHAM intervention
23 randomized
135 excluded
(did not meetexclusion criteria or refused consent)
60 assessed for eligibility158 assessed for eligibility
Fig. 1 Trial profile: PRETprogressive resistance exercisetraining, SHAM attention control.* completed additional exercise
J Cachexia Sarcopenia Muscle
participants, only one musculoskeletal harm was report-ed (delayed onset of muscle soreness) in the PRETgroup (Fig. 4).
3.6 Quality of life
PRET had positive efficacy in the healthy participants onbodily pain and social functioning domains, but this was notthe case in the HD patients (% change scores below; absolutedata not shown). Specifically, PRET elicited a large and sig-nificant improvement in bodily pain in healthy participants(PRET, +34±5 %; SHAM, −3±16 %; p=0.005; d=2.4) butnot in HD patients (PRET, 0±15 %; SHAM, +2±15 %; p=0.1; d=0.1). PRET also elicited a large significant improve-ment in social functioning in the healthy participants (PRET, +23±20 %; SHAM, −9±19 %; p=0.05; d=1.4) but not in HDpatients (PRET, p=+7±18 %; SHAM, −1.5±8 %; p=0.2; d=0.3). PRET had no efficacy on change scores for physical
function (p=0.1), role limitation due to physical problems (p=0.5), general health (p=0.3), vitality (p=0.44) and role limi-tation due to emotional problems (p=0.4) in either the healthyparticipants or HD patients.
4 Discussion
The aim of this randomised controlled pilot efficacy study wasto implement an intradialytic exercise program that met re-quired resistance exercise training principles to reverse muscleatrophy in HD patients. A secondary aim was to compare theanabolic response in HD patients to healthy controls. Usingnovel equipment allowing adequate overload and progression,12 weeks of high-intensity PRET elicited a clinically impor-tant and statistically significant anabolic response and strengthincrease in HD patients that was similar to that observed in
Table 1 Baseline characteristics of all groups
Characteristic Haemodialysis patients Healthy participants p
PRET SHAM PRET SHAM HD PRET versushealthy PRET
HD SHAM versushealthy SHAM
Age (years) 48±18 58±15 50±15 40±17 0.8 0.06
Body mass index (kg m2-1)§ 25±3 26±5 30±7 25±5 0.08 0.5
Gender (Male/Female) 7/2 6/4 2/2 0/4
Comorbid conditions
HypertensionDiabetesMyocardial infarction
5 4 1 1
0 2 0 0
0 3 1 0
Number on medications
Beta blockersAce inhibitorsAngiotensin receptor blockersCalcium channel blockersAlpha blockersBenzodiazepinesErythropoiesis stimulating agents
5 2 1 0
3 4 0 0
0 0 0 0
2 5 0 0
1 2 0 0
0 4 0 1
6 7 0 0
Aetiology of HD
GlomerulonephritisInfective/obstructiveHereditaryUncertain
4 51 1
1 0
3 4
Dialysis vintage (months) 46±54 66±47Kt/Vurea 1.34±0.13 1.50±0.24
Haemoglobin (g dL−1) 11.7±1.8 12.1±2.1
Albumin 41±3 42±3
Serum bicarbonate (mmol L−1) 22.4±3.2 22.5±2.7
Serum potassium (mmol L−1) 4.8±1.0 5.0±0.6
HD haemodialysis, PRET progressive resistance exercise training, SHAM attention control
J Cachexia Sarcopenia Muscle
healthy participants. However, unexpectedly, in HD patients,PRET was not efficacious at improving functional capacity.
When the temporal nature of muscle wasting is considered,the anabolic response to PRET in HD patients seems remark-ably normal. In the present study, there was an approximately7 % difference in muscle volume change between PRET andSHAM interventions, in both the HD patients and the healthyparticipants. These data are in contrast to the majority ofprevious studies [11, 16, 17, 30] and a recent meta-analysis[31] that have failed to show a significant hypertrophic re-sponse to exercise in HD populations. An explanation is that
previous studies have not provided significant overload andprogression; hypertrophic adaptation will only occur if agreater force is continually exerted to meet higher physiolog-ical demands [19]. It is questionable that this principle hasbeen adhered to in previous studies that have prescribedintradialytic exercise utilising weights that can only providea maximum lifted weight of 15 kg (compared to the 200 kgpermissible with the current equipment). Note that the differ-ence in response between studies is not due to the fact that ourpatients were healthier than those previously investigated:physical function was substantially decreased in the patients
0
2000
4000
6000
8000
10000
12000
14000
16000
1 2 3 4 5 6 7 8 9 10 11 12
Tra
inin
g V
olum
e (k
g)
Week
Healthy Participants
Haemodialysis Patients
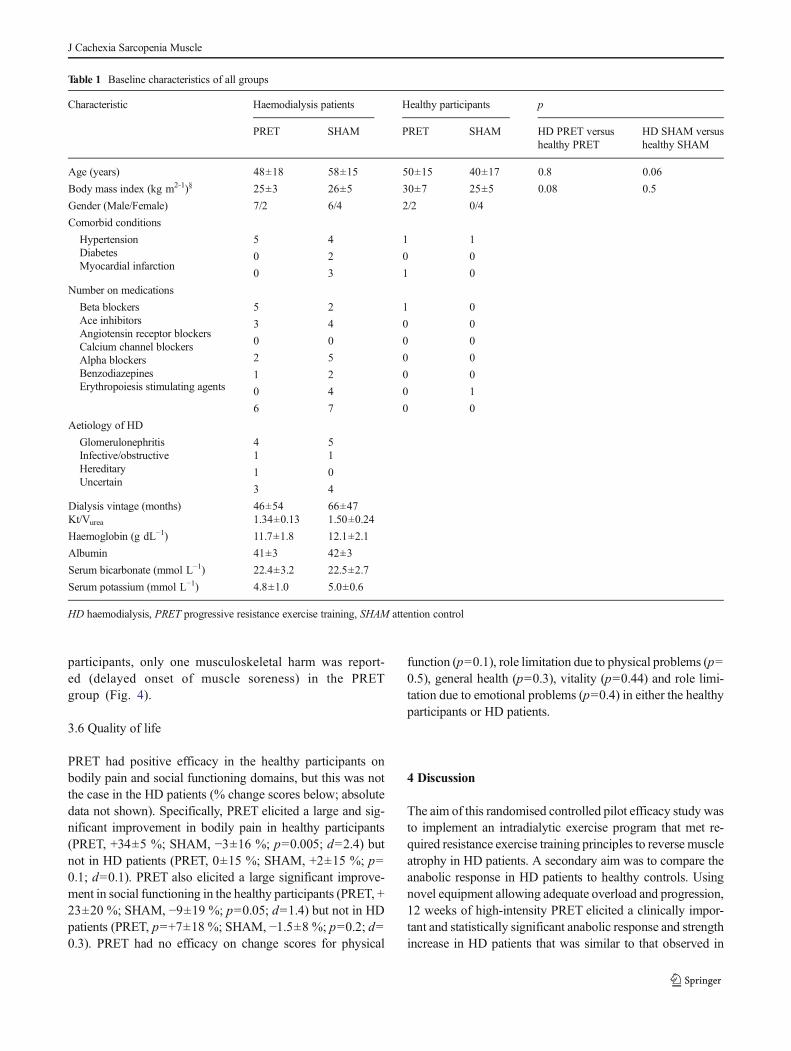
Fig. 2 Training volume in progressive resistance exercise training groupsover the 12-week intervention period. Training volume increased fromweek 1 to 12 similarly in both haemodialysis patients and healthy con-trols, as evidenced by a significant main effect of time by analysis ofvariance (p=0.03), a non-significant group × time interaction (p=0.3) anda non-significant main effect of group (p=0.2)
Table 2 Muscle volume, strength and physical functioning absolute data before and after the 12 week intervention period
Outcome measure Haemodialysis patients Healthy participants HD PRET versushealthy PRET
HD PRETversus HD SHAM
Healthy PRETversus healthy SHAM
PRET SHAM PRET SHAM
Muscle volume (cm3)
Pre 2,822±438 2,490±601 2,877±710 2,183±527 0.5 0.007 0.09
Post 2,906±489 2,380±643 3,013±863 2,151±527
Knee extensor strength (N)
Pre 179±109 151±79 382±103 239±80 0.6 0.012 0.06
Post 287±86 201±77 471±191 210±31
Sit to stand (reps)
Pre 11±2 10±4 21±6 23±6 0.004 0.2 0.005
Post 13±3 11±5 28±8 25±7
8-ft get up and go (s)
Pre 5.8±1.2 6.7±1.8 4.4±0.2 4.3±0.7 0.5 0.5 0.09
Post 5.0±0.8 6.2±1.8 3.8±0.4 4.5±0.2
6-min walk distance (m)
Pre 532±95 460±162 536±47 559±26 0.7 0.4 0.01
Post 571±101 520±160 600±54 511±38
PRET progressive resistance exercise training, SHAM attention control
-400
-300
-200
-100
0
100
200
300
400
Cha
nge
in T
high
Mus
cle
Vol
ume
(cm
3 )
HD PRET HD SHAM HEALTHY PRET HEALTHY SHAM
p = 0.007 p = 0.09
Fig. 3 Changes in absolute thigh muscle volume by magnetic resonanceimaging over the 12-week intervention period. HD haemodialysis pa-tients, PRET progressive resistance training, SHAM attention control.PRET elicited a similar anabolic response in haemodialysis patients andhealthy participants, as evidenced by significant independent t testsbetween PRET and SHAM groups and moderate to large effect sizes
J Cachexia Sarcopenia Muscle
as compared to the healthy controls studied herein. Further-more, despite similar muscle volumes at baseline, the HDSHAM patients lost clinically significant amounts of musclevolume over the 12-week period, signifying that these patientswere in a catabolic state.
The anabolic response observed herein is supported by twoprevious studies [14, 15]. In fact, in those studies, the anabolicresponse was slightly larger (8–10 %) than observed herein,perhaps because the present study utilised only one exercise,whereas previous studies have utilised multiple lower andwhole body exercises that might be expected to induce a largersystemic hypertrophic response [32].
Encouragingly, these findings suggest that if anabolicresistance is present in HD patients [5], it can beovercome by providing resistance exercise of sufficientvolume. Despite perturbed sex hormone, insulin andinsulin-like growth factor/growth hormone pathways [5,20], an anabolic response to PRET is possible in HDpatients. This finding is consistent with studies thathave administered sex hormones [15, 26] and insulin-like growth factor/growth hormone [33], successfullyincreasing muscle volume.
Interestingly, the response of functional capacity to PRETdiffered between HD and healthy participants. Althoughstrength increases in the HD patients following PRET ap-peared promising, they did not translate into improved func-tional capacity. This lack of an effect cannot be due to poorcompliance: compliance was similarly excellent between thepopulations. Nor can it be due to selection bias of relativelyhealthy patients: the healthy controls responded to PRETdespite having an even higher baseline functional capacity.Neither can it be due to insufficient intervention duration: the
healthy participants herein responded to PRETwithin the 12-week intervention. Such a lack of effect is consistently report-ed in studies investigating intradialytic resistance training inHD patients [14–17]. This lack of efficacy is particularlysurprising, considering that similar interventions carried outin other catabolic conditions have shown significant increasesin similar measures of functional capacity [10]. It is notewor-thy that for the 6-min walk test, both PRET and SHAMexercise similarly increased functional capacity; it is possiblethat despite familiarisation with outcome measures, patientscould have been too cautious in the baseline tests, resulting ina learning effect in both groups at post-test. Variability in thislearning effect may have masked potential interactions [34].However, it is also interesting that intradialytic aerobic exer-cise has generally proven successful at enhancing the samefunctional measures in HD patients [35, 36]. Future researchin this area could provide an interesting insight into the mech-anisms behind enhanced functional capacity in thispopulation.
PRETalso had no effect on QoL in HD patients. Assumingthis was not due to being underpowered to detect changes inQoL, a possible explanation could be that patients who vol-unteer to take part in exercise trials are generally healthierpatients with a better QoL. In fact, the patients who took partin this study presented with QoL scores similar to age-matched Welsh normative values of healthy individuals [37].In addition, exclusion criteria meant that patients with uncon-trolled medical complications, and therefore an expectedpoorer QoL, were excluded from this study. It is possible thathad these patients been included, they may have experiencedgreater QoL changes following an exercise intervention. Al-ternatively, the lack of change in physical function may havesimply blunted any changes to quality of life.
A limitation to this study was the absence of whole bodyprotein synthesis and diet measurements to indicate whethernutritional intake confounded body composition responses.Previous literature has shown increases in body fat percentagefollowing PRET [15], perhaps due to an increased appetitefollowing exercise [38]. Additionally, protein intake maymoderate anabolism in response to muscle contraction [39].Future studies should include such dietary measures and also adetailed assessment of energy balance. A further limitationlies in the small size of this pilot study, and particularly of theconveniently sampled healthy control group. Specifically, de-spite randomisation, the age and body composition were notexactly the same between the groups at baseline. We ad-dressed this issue statistically by using and presenting ananalysis of change scores. An alternative analysis using thebaseline data as a covariate confirmed our interpretation (datanot shown). Nevertheless, comparison of response betweendiseased and non-diseased participants should be interpretedcautiously, and results may only be generalizable to popula-tions similar to that studied herein. However, the strength of
-100
100
-50
50
200
150
0
Kne
e ex
tens
or s
tren
gth
abso
lute
cha
nge
(N)
p = 0.01 p = 0.06
HD PRET HD SHAM HEALTHY PRET HEALTHY SHAM
Fig. 4 Isometric knee extensor strength absolute change over the 12-week intervention period. HD haemodialysis patients, PRET progressiveresistance training. PRET elicited a similar strength response inhaemodialysis patients and healthy participants, as evidenced by a signif-icant independent t tests between PRETand SHAM groups and moderateto large effect sizes
J Cachexia Sarcopenia Muscle

including this comparison group is that for the first time, itallows such comparisons to be made.
In conclusion, using novel intradialytic equipment to allowadequate overload, PRET was safe and increased musclevolume and strength in HD patients. A similar anabolic re-sponse to PRET was observed in HD patients and healthyparticipants, precluding assumptions of anabolic resistance toexercise in this patient population. While reversing musclewasting is theoretically beneficial for reducing morbidity andmortality, the lack of efficacy on functional capacity wassurprising and warrants further investigation.
Acknowledgments We acknowledge Loretta Davies, Nicola Carey,Hannah Lowther and Ruth Glover for invaluable help with data collec-tion. This study was supported by unrestricted grants from the NorthWestWales National Health Service Trust Endowment Fund and by NorthWales National Health Service Trust Research and Development-CentralArea.
Authorship The authors certify that they comply with the ethicalguidelines for authorship and publishing of the Journal of Cachexia,Sarcopenia and Muscle 2010; 1:7–8 (von Haehling S, Morley JE, CoatsAJ, and Anker SD).
Conflicts of interest The authors declare that they have no conflict ofinterest.
References
1. Sakkas GK, Ball D, Mercer TH, Sargeant AJ, Tolfrey K, Naish PF.Atrophy of non-locomotor muscle in patients with end-stage renalfailure. Nephrol Dial Transplant. 2003;18:2074–81.
2. Johansen KL, Shubert T, Doyle J, Soher B, Sakkas GK, Kent-BraunJA. Muscle atrophy in patients receiving hemodialysis: effects onmuscle strength, muscle quality, and physical function. Kidney Int.2003;63:291–7.
3. Macdonald JH, Phanish MK, Marcora SM, Jibani M, BloodworthLLO, Holly JMP, et al. Muscle insulin-like growth factor status, bodycomposition, and functional capacity in hemodialysis patients. J RenNutr. 2004;14:248–52.
4. Workeneh BT,MitchWE. Review of muscle wasting associated withchronic kidney disease. Am J Clin Nutr. 2010;91:1128S–32.
5. Mak RH, Ikizler TA, Kovesdy CP, Raj DS, Stenvinkel P, Kalantar-Zadeh K. Wasting in chronic kidney disease (vol 2, pg 9, 2011). JCachexia Sarcopenia Muscle. 2011;2:119.
6. Huang CX, Tighiouart H, Beddhu S, Cheung AK, Dwyer JT,Eknoyan G, et al. Both low muscle mass and low fat are associatedwith higher all-cause mortality in hemodialysis patients. Kidney Int.2010;77:624–9.
7. Marrades RM, Roca J, Campistol JM, Diaz O, Barbera JA,Torregrosa JV, et al. Effects of erythropoietin on muscle O2 transportduring exercise in patients with chronic renal failure. J Clin Invest.1996;97:2092–100.
8. Cheema B, Abas H, Smith B, O’Sullivan AJ, Chan M, PatwardhanA, et al. Investigation of skeletal muscle quantity and quality in end-stage renal disease. Nephrology (Carlton). 2010;15:454–63.
9. Singh MAF, Ding WJ, Manfredi TJ, Solares GS, O’Neill EF,Clements KM, et al. Insulin-like growth factor I in skeletal muscleafter weight-lifting exercise in frail elders. Am Physiol EndocrinolMetab. 1999;277:E135–43.
10. Lemmey AB, Marcora SM, Chester K, Wilson S, Casanova F,Maddison PJ. Effects of high-intensity resistance training in patientswith rheumatoid arthritis: a randomized controlled trial. ArthritisRheum. 2009;61:1726–34.
11. Kopple JD, Wang H, Casaburi R, Fournier M, Lewis MI, Taylor W,et al. Exercise in maintenance hemodialysis patients induces tran-scriptional changes in genes favoring anabolic muscle. J Am SocNephrol. 2007;18:2975–86.
12. Balakrishnan VS, Rao M, Menon V, Gordon PL, Pilichowska M,Castaneda F, et al. Resistance training increases muscle mitochondri-al biogenesis in patients with chronic kidney disease. Clin J Am SocNephrol. 2010;5:996–1002.
13. Senior JR, Maroni BJ. Working group session report: chronic renaland gastrointestinal disease. J Nutr. 1999;129:313S–4.
14. Chen JL, Godfrey S, Ng TT,Moorthi R, Liangos O, Ruthazer R, et al.Effect of intra-dialytic, low-intensity strength training on functionalcapacity in adult haemodialysis patients: a randomized pilot trial.Nephrol Dial Transplant. 2010;25:1936–43.
15. Johansen KL, Painter PL, Sakkas GK, Gordon P, Doyle J, Shubert T.Effects of resistance exercise training and nandrolone decanoate onbody composition and muscle function among patients who receivehemodialysis: a randomized, controlled trial. J Am Soc Nephrol.2006;17:2307–14.
16. Cheema B, Abas H, Smith B, O’Sullivan A, ChanM, Patwardhan A,et al. Randomized controlled trial of intradialytic resistance trainingto target muscle wasting in ESRD: the progressive exercise foranabolism in kidney disease (PEAK) study. Am J Kidney Dis.2007;50:574–84.
17. Cheema B, Abas H, Smith B, O’Sullivan A, ChanM, Patwardhan A,et al. Progressive exercise for anabolism in kidney disease (PEAK): arandomized, controlled trial of resistance training during hemodialy-sis. J Am Soc Nephrol. 2007;18:1594–601.
18. Spiering BA, Kraemer WJ, Anderson JM, Armstrong LE, Nindl BC,Volek JS, et al. Resistance exercise biology: manipulation of resis-tance exercise programme variables determines the responses ofcellular and molecular signalling pathways. Sports Med.2008;38:527–40.
19. Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C,Feigenbaum MS, et al. Joint position statement: progression modelsin resistance training for healthy adults. Med Sci Sports Exerc.2002;34:364–80.
20. Albaaj F, Sivalingham M, Haynes P, McKinnon G, Foley RN,Waldek S, et al. Prevalence of hypogonadism in male patients withrenal failure. Postgrad Med J. 2006;82:693–6.
21. Mak RH. Insulin and its role in chronic kidney disease. PediatrNephrol. 2008;23:355–62.
22. Mak RH, Cheung WW, Roberts Jr CT. The growth hormone-insulin-like growth factor-I axis in chronic kidney disease. Growth HormIGF Res. 2008;18:17–25.
23. Bryzycki M. Strength testing-predicting a one-rep max from a reps-to-fatigue. J Phys Edu Recreat Dance. 1993;64:88–90.
24. Painter PL, Krasnoff JB. End stage metabolic disease: renal failureand liver failure. In: Durstine JL, Moore GE, Painter PL, Roberts SO,editors. ACSM’s exercise management for persons with chronicdiseases and disabilities. 3rd ed. Champaign, IL: Human Kinetics;2009. p. 175–82.
25. Tracy BL, Ivey FM, Metter EJ, Fleg JL, Siegel EL, Hurley BF. Amore efficient magnetic resonance imaging-based strategy for mea-suring quadriceps muscle volume. Med Sci Sports Exerc.2003;35:425–33.
26. Macdonald JH, Marcora SM, Jibani MM, Kumwenda MJ, AhmedW, Lemmey AB. Nandrolone decanoate as anabolic therapy inchronic kidney disease: a randomized phase II dose-finding study.Nephron Clin Pract. 2007;106:125–35.
27. Rikili R, Jones C. Senior fitness test manual. Champaign, IL: HumanKinetics; 2001.
J Cachexia Sarcopenia Muscle

28. Ware JE, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B,Maruish ME. User’s manual for the SF-36v2 health survey.QualityMetric: Lincoln, RI; 2007.
29. Cohen J. Statistical power analysis for the behavioural sciences.Hillsdale: Lawrence Erlbaum Associates; 1988.
30. Headley S, GermainM,Mailloux P,Mulhern J, Ashworth B, Burris J,et al. Resistance training improves strength and functional measuresin patients with end-stage renal disease. Am J Kidney Dis.2002;40:355–64.
31. Heiwe S, Jacobson SH. Exercise training for adults with chronickidney disease. Cochrane Database Syst Rev. 2011;10:CD003236.
32. Hansen S, Kvorning T, Kjaer M, Sjogaard G. The effect of short-termstrength training on human skeletal muscle: the importance of phys-iologically elevated hormone levels. Scand J Med Sci Sports.2001;11:347–54.
33. Dong J, Ikizler TA. New insights into the role of anabolic interven-tions in dialysis patients with protein energy wasting. Curr OpinNephrol Hypertens. 2009;18:469–75.
34. Hopkins WG. Measures of reliability in sports medicine and science.Sports Med. 2000;30:1–15.
35. Cheema BSB, Smith BCF, Singh MAF. A rationale for intradialyticexercise training as standard clinical practice in ESRD. Am JKid Dis.2005;45:912–6.
36. Macdonald JH, Marcora SM, Jibani M, Phanish MK, Holly J,Lemmey AB. Intradialytic exercise as anabolic therapy inhaemodialysis patients—a pilot study. Clin Physiol Funct Imaging.2005;25:113–8.
37. Burholt V, Nash P. Short form 36 (SF-36) health survey questionnaire:normative data for wales. J Public Health (Oxf). 2011;33:587–603.
38. Hopkins M, Jeukendrup A, King NA, Blundell JE. The relationshipbetween substrate metabolism, exercise and appetite control doesglycogen availability influence the motivation to eat, energy intakeor food choice? Sports Med. 2011;41:507–21.
39. Burd NA, Wall BT, van Loon LJC. The curious case of anabolicresistance: old wives’ tales or new fables? J Appl Physiol.2012;112:1233–5.
J Cachexia Sarcopenia Muscle