an update and baseline data from the phase 2/3 gain trial
TRANSCRIPT

1
April 2021
An update and baseline data from the Phase 2/3 GAIN trial of COR388 (atuzaginstat) a novel bacterial virulence factor inhibitor for the treatment of Alzheimer’s Disease
Michael Detke, MD PhD1, Shirin Kapur, PhD1, Marwan Sabbagh, MD2, Mark Ryder, DMD3, Ira Goodman, MD4, Debasish Raha, PhD1, Florian Ermini, PhD1, Mai Nguyen, PhD1, Ursula Haditsch, PhD1, Joanna Bolger1, Dave Hennings, PhD1,
Kim Perry, PhD5, Casey Lynch1, Hatice Hasturk, DDS, PhD6, Leslie J. Holsinger, PhD1, Stephen Dominy, MD1
(1) Cortexyme, South San Francisco, CA; (2) Cleveland Clinic, Las Vegas, NV; (3) UCSF, San Francisco, CA; (4) Bioclinica, Orlando, FL; (5) Innovative Analytics, Portage, MI; (6) Forsyth Forsyth Institute, Cambridge, MA

2
Certain information contained in this presentation and statements made orally during this presentation relate to or are based on studies, publications, surveys and
other data obtained from third-party sources and Cortexyme's own internal estimates and research. While Cortexyme believes these third-party sources to be
reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness
of, any information obtained from third-party sources. While Cortexyme believes its internal research is reliable, such research has not been verified by any
independent source. This presentation contains information that is highly confidential and/or privileged. The information is intended only for the use of individuals
or entities to which it is addressed. If you are not the intended recipient, you are hereby notified that any reliance, disclosure, copying, distribution, or taking of any
action on the contents of this material is strictly prohibited. This presentation contains forward-looking statements. Forward-looking statements are neither
historical facts nor assurances of future performance. Instead, they are based on Cortexyme's current beliefs, expectations and assumptions regarding the future
of its business, its future plans and strategies, its clinical results and other future conditions. All statements other than statements of historical facts contained in
this presentation, including statements regarding future results of operations and financial position, business strategy, current and prospective markets or
products, clinical activities, regulatory approvals, degree of market acceptance, and plans and objectives of management for future operations, are forward-
looking statements. The words "may," "will," "should," "expect," "plan," "anticipate," "could," "intend," "target," "project," "estimate," "believe," "predict,"
"potential" or "continue" or the negative of these terms or other similar expressions are intended to identify forward-looking statements, although not all forward-
looking statements contain these identifying words. The forward-looking statements in this presentation represent Cortexyme' views as of the date of this
presentation. Although Cortexyme believes the expectations reflected in such forward-looking statements are reasonable, it can give no assurance that such
expectations will prove to be correct. Accordingly, readers are cautioned not to place undue reliance on these forward-looking statements. Except as required by
applicable law, Cortexyme do not plan to publicly update or revise any forward-looking statements contains herein, whether as a result of any new information,
future events, changed circumstances or otherwise. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-
looking statements. New risk factors and uncertainties may emerge from time to time, and it is not possible to predict all risk factors and uncertainties. There can
be no assurance that the opportunity will meet your investment objectives, or that you will receive a return of all or part of such investment. Investment results may
vary significantly over any given time period. The appropriateness of a particular investment or strategy will depend on an investor's individual circumstances and
objectives. We recommend that investors independently evaluate specific investments and strategies.
Disclaimer

3
Disclosures
Drs. Sabbagh, Goodman, Hasturk, Perry and Ryder are consultants for Cortexyme,
compensated for their time (no stock/options).
All other authors are full-time employees of Cortexyme and holders of Cortexyme
stock/options.
Most of the work presented here was funded by Cortexyme, Inc.
4
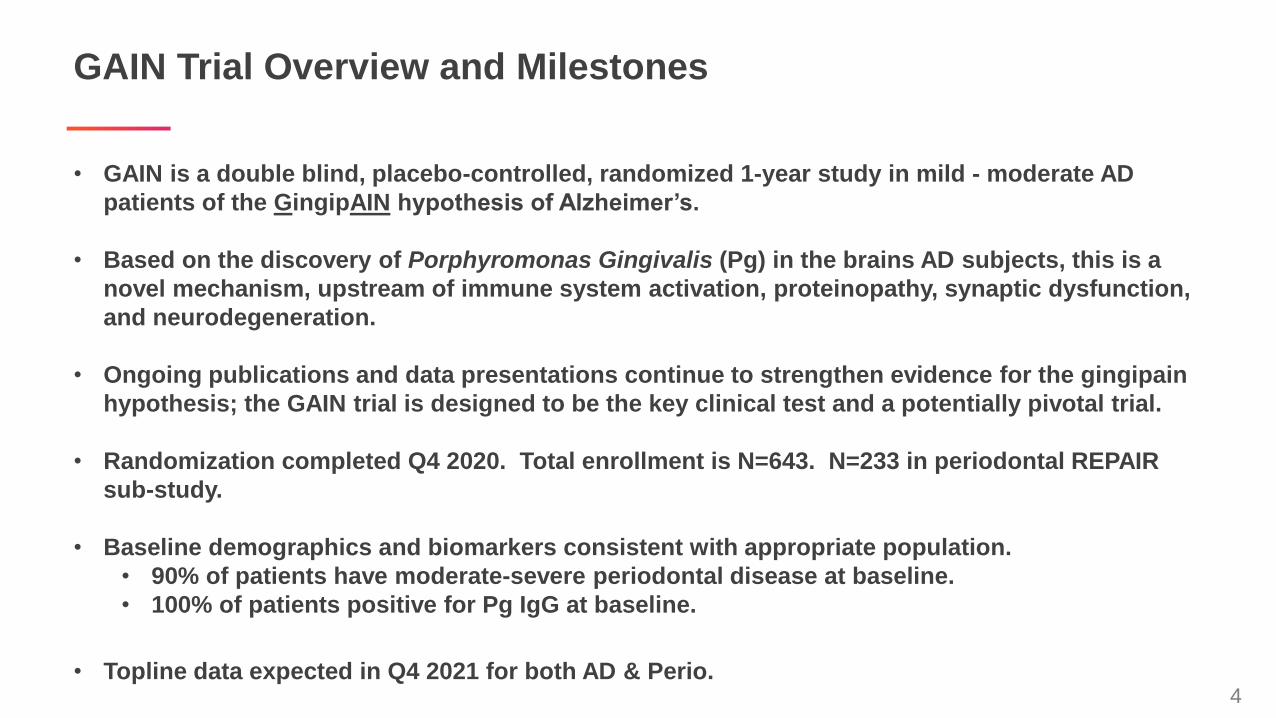
GAIN Trial Overview and Milestones
• GAIN is a double blind, placebo-controlled, randomized 1-year study in mild - moderate AD
patients of the GingipAIN hypothesis of Alzheimer’s.
• Based on the discovery of Porphyromonas Gingivalis (Pg) in the brains AD subjects, this is a
novel mechanism, upstream of immune system activation, proteinopathy, synaptic dysfunction,
and neurodegeneration.
• Ongoing publications and data presentations continue to strengthen evidence for the gingipain
hypothesis; the GAIN trial is designed to be the key clinical test and a potentially pivotal trial.
• Randomization completed Q4 2020. Total enrollment is N=643. N=233 in periodontal REPAIR
sub-study.
• Baseline demographics and biomarkers consistent with appropriate population.
• 90% of patients have moderate-severe periodontal disease at baseline.
• 100% of patients positive for Pg IgG at baseline.
• Topline data expected in Q4 2021 for both AD & Perio.

5
NeurodegenerationTau fragmentation
ApoE fragmentation
Lysosomal dysfunction
P. gingivalisinfection
Braininfiltration
Gingipain
(protease virulence factor)
secretion
Aging
Genetic risk (ApoE4,
TLR4, CR1, TREM2)
Trauma
Bacterial load
Host responseAmyloid beta production
Microglia activation
Neuroinflammation
Complement induction
Inflammasome
Bacterial Brain Infiltration Triggers Alzheimer’s Pathology

6
Seminal Discovery: P. gingivalis Found in Brains of >90% of AD Patients
Source: Collaboration with University of Auckland/ Neurovalida ****p<0.0001, Dominy et al. Science Advances, 2019
Immunohistochemistry
of middle temporal
gyrus microarray
Tau load(normalized to control)
100
10
1
0.1
Age-matched
ControlsAlzheimer’s
Arg
inin
e g
ingip
ain
load
(norm
aliz
ed t
oco
ntr
ol)
Arg
inin
e g
ingip
ain
load
(norm
aliz
ed t
oco
ntr
ol)
10
1
0.1
****
0.001 0.01 0.1 1 10 100 1000
Gingipain load correlates to symptoms and pathology

7
Evidence of Causation: Oral Pg Infection Induces AD Pathology in Mice
*p< 0.05,**p<0.01, ***p<0.001, ****p<0.001, *****p<0.001
Source: Adapted from Ilievski, et al. Chronic oral application of a periodontal pathogen results in brain inflammation, neurodegeneration and amyloid beta production in wild type
mice PLOS: One 2018
Mic
rog
lia
/fi
eld
Activated Microglia
Cont. Inf.
14
12
10
8
6
4
2
0
**
#p
Ta
u/
fie
ld
Tau Tangle-Like Neurons
Cont. Inf.
*****14
12
10
8
6
4
2
0
P.g
ing
iva
lis
16
SR
NA
co
pie
s/
5F
FP
E
P. Gingivalis Infiltrates the
Brain
Cont. Inf.
10
8
6
4
2
0
x10
****
Re
lati
ve
TN
Fa
lph
ag
en
e
ex
pre
ss
ion
Neuroinflammation
Cont. Inf.
10
8
6
4
2
0
**
Am
ylo
idb
eta
Pla
qu
es
/fi
eld
Amyloid Beta Plaques
*****
Cont. Inf.
6
5
4
3
2
1
%In
tac
t
ne
uro
ns
/fi
eld
Neurodegeneration
Cont. Inf.
100
80
60
40
20
10
0
**********
■ CA1
■ DG
Brain pathology at 22 weeks post oral infection of wild type mouse with P. gingivalis

8
Atuzaginstat Acts Upstream of Alzheimer’s Induced Pathology
Source: Cortexyme atuzaginstat (COR388) dose response study, Mean +/- SEM *p< 0.05,**p<0.01, ***p<0.001, Science Advances, 2019
Week 1 2 3 4
56 7 8 9 10
0COR388 10 or 30 mg/kg po 2x/day
3x oral P.g. / week
Infected Inf + COR388
Copy
#/
100
ng
DN
A
Inte
rneuro
ns
/m
m3
pg
/m
gP
rote
in
pg
/m
gP
rote
in
0
2,000
4,000
6,000
***
0
2,000
4,000
6,000
8,000
10,000
*
0.00
0.05
0.10
0.15
0.20
***
0.0
0.5
1.0
1.5
2.0
2.5
**
Infected Inf + COR388
Infected Inf + COR388
Infected Inf + COR388
Efficacious in wild type mouse model for sporadic Alzheimer’s disease

9
Atuzaginstat Showed Favorable Trends on Multiple Cognitive Measures
Source: Cortexyme MAD study: *p< 0.05, ***p<0.001
MM
SE
Sco
re
Days of treatment
CA
NTA
Bco
mp
osite
(Zscore
)
Days of treatment Pro
po
rtio
nP
rep
ositio
n:to
talco
nte
nt
Days of treatment
COR388 (n=6) Placebo (n=3)
28-day Phase 1b MAD study in AD patients

10
Days of treatment
%o
fb
aselin
ele
vel
*
0 10 20 30
130
120
110
baseline
90
80
70
60
days
**
%o
fb
aselin
ele
vel
Atuzaginstat Target Engagement of Key Endpoints
Source: Cortexyme ApoE and MAD study: *p< 0.05, ** p< 0.01
Placebo (n=2)COR388 (n=4)
0 28
Placebo (n=2)COR388 (n=6)
28-day Phase 1b MAD study in AD patients
11
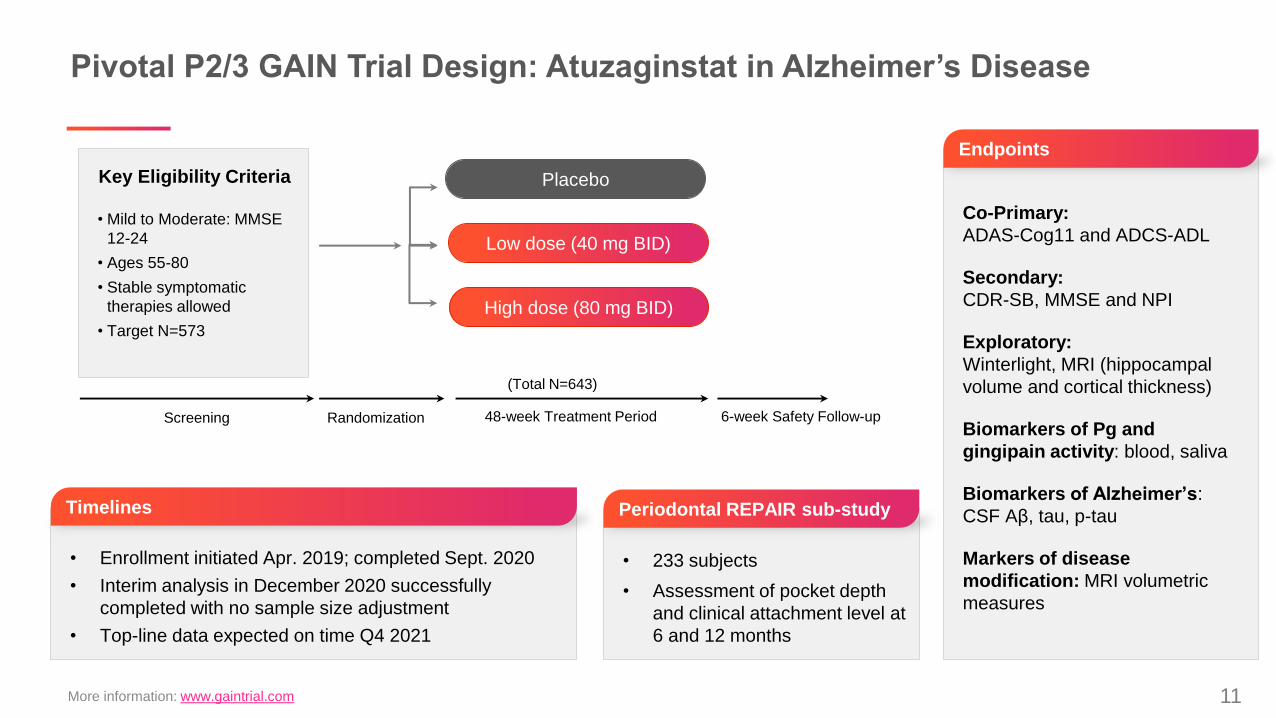
Pivotal P2/3 GAIN Trial Design: Atuzaginstat in Alzheimer’s Disease
• Mild to Moderate: MMSE
12-24
• Ages 55-80
• Stable symptomatic
therapies allowed
• Target N=573
RandomizationScreening
Co-Primary:
ADAS-Cog11 and ADCS-ADL
Secondary:
CDR-SB, MMSE and NPI
Exploratory:
Winterlight, MRI (hippocampal
volume and cortical thickness)
Biomarkers of Pg and
gingipain activity: blood, saliva
Biomarkers of Alzheimer’s:
CSF Aβ, tau, p-tau
Markers of disease
modification: MRI volumetric
measures
Endpoints
Key Eligibility Criteria
• Enrollment initiated Apr. 2019; completed Sept. 2020
• Interim analysis in December 2020 successfully
completed with no sample size adjustment
• Top-line data expected on time Q4 2021
• 233 subjects
• Assessment of pocket depth
and clinical attachment level at
6 and 12 months
Timelines Periodontal REPAIR sub-study
Placebo
Low dose (40 mg BID)
48-week Treatment Period
(Total N=643)
More information: www.gaintrial.com
High dose (80 mg BID)
6-week Safety Follow-up

12
GAIN Baseline Demo: Population and Stratification as Expected
Parameter Overall (N=643)
Age at Informed Consent (years) 69.1 (55 – 80)
Sex
Male 278 (43%)
Female 365 (57%)
Race and Ethnicity
Black or African American 42 (7%)
White, Hispanic or Latino 68 (11%)
White, Not Hispanic/Latino 505 (79%)
Other 10 (2%)
Missing 18 (3%)
Parameter Overall (N=643)
Region
North America 447 (70%)
Europe 196 (30%)
MMSE, n (%)
Moderate >=12 to <=18 324 (50%)
Mild >=19 to <=24 319 (50%)
ApoE4 (Stratum), n (%)
ApoE4 Positive 414 (64%)
non-ApoE4 229 (36%)
Cholinesterase Inhibitor/Memantine Use
Yes 476 (74%)
No 167 (26%)

13
Biomarker Highlights: Baseline CSF Ab 42/40, Tau and P-Tau
Approximately 84% of GAIN subjects have CSF markers characteristic of Alzheimer’s Disease diagnosis

14
Over 90% of GAIN Subjects in the Periodontal REPAIR
Sub-Study Have Moderate to Severe Periodontal Disease at Baseline
Diagnosis based on Pocket depth and Clinical attachment loss measures (N=233)
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
% o
f s
ub
jec
ts
N o n e -
M i l d
M o d e r a t e -
S e v e r e
0
4
8
1 2
1 6
2 0
2 4
2 8
3 2
Nu
mb
er
of t
ee
th
N o n e -
M i l d
M o d e r a t e -
S e v e r e
Diagnosis based on PD and CAL Number of teeth

15
100% of subjects analyzed have P. gingivalis specific IgG
in plasma at baseline indicating systemic infection
100% of GAIN subjects have
evidence of systemic P. gingivalis
exposure and 78% have IgG
antibody titers that correlate with
periodontal disease. N=638.
Offenbacher et al, J Periodontology 2007 Oct; 78(10):1911-25

16
Summary
• Data continue to accumulate supporting the gingipain hypothesis of Alzheimer’s, periodontal
disease and other degenerative disorders
• The GAIN trial, designed to be a key clinical proof of concept and potentially pivotal trial, is
fully enrolled
• Baseline data* support that this is an appropriate population for testing atuzaginstat for AD
• Demographics
• Aβ, Total tau and p-Tau 181 in CSF
• Pg antibodies in serum
• Periodontal disease data in a sub study
• Topline data will be reported by Q4 2021
• Alzheimer’s Disease
• Periodontal Disease
17
Acknowledgements
Cortexyme team
Stephen Dominy, MDCasey Lynch, MSLeslie Holsinger, PhDDave Hennings, PhDJoanna BolgerShirin Arastu-Kapur, PhDMai Nguyen, PhDDebashish Raha, PhDFlorian Ermini, PhD Ursula Haditsch, PhDSean BroceTheresa Roth
Clinical Investigators in Phase 1 & Clinical Advisors
Merce Boada, MD, PhDMark Brody, MDJeffrey Cummings, MDMartin Farlow, MDIra Goodman, MDHatice Hasturk, DDS, PhDClive Holmes, PhDLouis Kirby, MDThomas Laughren, MDDavid Munoz, MDMark Ryder, DMD
Marwan Sabbagh, MDPhilip Scheltens, MD, PhDLon Schneider, MD, MSEric Siemers, MDMarwan Sabbagh, MDPierre Tariot, MDStephen Thien, MD

18
THANK YOU