an unusual “thyroid cyst”: intrathyroidal parathyroid cyst
TRANSCRIPT
An Unusual “Thyroid Cyst”: IntrathyroidalParathyroid Cyst
Manal Atwan & Runjan Chetty
Published online: 10 May 2011# Springer Science+Business Media, LLC 2011
Introduction
Pathology involving the parathyroid glands most oftenranges from benign (adenoma and hyperplasia) to the veryrare, parathyroid carcinoma. Other pathologic conditionsare decidedly uncommon. Parathyroid glands are a verycommon source of intra-operative frozen sections: for thesurgeon, the challenge lies in identifying, locating anddissecting the parathyroid glands; for the pathologist, thechallenge is to be aware of ectopic locations and unusualpathology associated with the parathyroids in these loca-tions. The case under presentation is unusual not onlybecause of the intrathyroidal location of a parathyroid glandbut also because the ectopic parathyroid gland developed acyst which clinically presented as an intrinsic “thyroid”swelling. While an intrathyroidal location of a parathyroidgland is rare, it is nonetheless, well described, pathologicconditions affecting such ectopically sited glands are rare.
Case Report
A 19-year-old female presented with a 2-month history of left-sided neck lump. External examination revealed a 20×20 mmfirm, non-tender smooth lumpwithin the left lobe of the thyroidgland. An ultrasound scan confirmed the presence of a simple
cyst within the thyroid gland and fine needle aspiration was notattempted. At the patient’s request, a left hemi-thyroidectomywas carried out. The pre-operative serum biochemical markers,including calcium, TSH and phosphate, were all normal. Serumparathyroid hormone was not investigated. Macroscopicexamination of the thyroid lobectomy specimen revealed acystic structure measuring 15 mm in maximal diameter locatedwithin otherwise unremarkable thyroid parenchyma. Thecyst contained small amount of amber-coloured fluid andwas thin-walled.
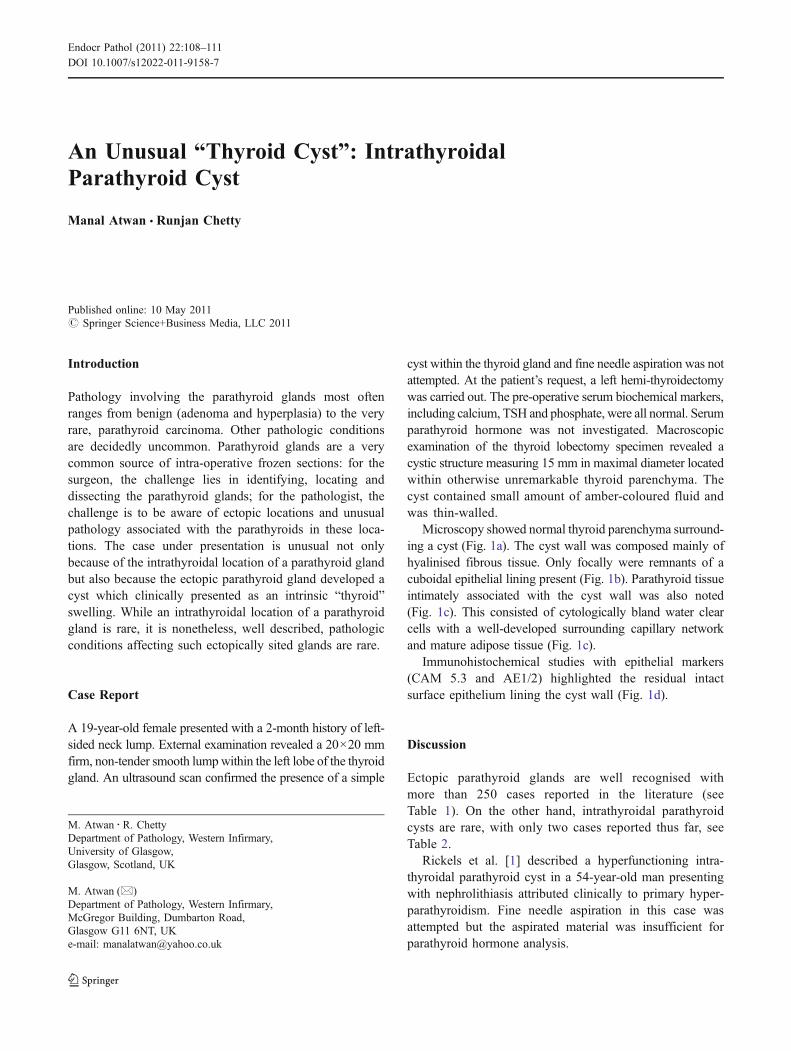
Microscopy showed normal thyroid parenchyma surround-ing a cyst (Fig. 1a). The cyst wall was composed mainly ofhyalinised fibrous tissue. Only focally were remnants of acuboidal epithelial lining present (Fig. 1b). Parathyroid tissueintimately associated with the cyst wall was also noted(Fig. 1c). This consisted of cytologically bland water clearcells with a well-developed surrounding capillary networkand mature adipose tissue (Fig. 1c).
Immunohistochemical studies with epithelial markers(CAM 5.3 and AE1/2) highlighted the residual intactsurface epithelium lining the cyst wall (Fig. 1d).
Discussion
Ectopic parathyroid glands are well recognised withmore than 250 cases reported in the literature (seeTable 1). On the other hand, intrathyroidal parathyroidcysts are rare, with only two cases reported thus far, seeTable 2.
Rickels et al. [1] described a hyperfunctioning intra-thyroidal parathyroid cyst in a 54-year-old man presentingwith nephrolithiasis attributed clinically to primary hyper-parathyroidism. Fine needle aspiration in this case wasattempted but the aspirated material was insufficient forparathyroid hormone analysis.
M. Atwan : R. ChettyDepartment of Pathology, Western Infirmary,University of Glasgow,Glasgow, Scotland, UK
M. Atwan (*)Department of Pathology, Western Infirmary,McGregor Building, Dumbarton Road,Glasgow G11 6NT, UKe-mail: [email protected]
Endocr Pathol (2011) 22:108–111DOI 10.1007/s12022-011-9158-7
Capezzone et al. [2] described a case of ectopicintrathyroid parathyroid cyst with associated papillarymicrocarcinoma of the thyroid in a 29-year-old femalewho was referred for surgery because of a multinodulargoitre. The fluid obtained via fine needle aspiration of thecyst showed elevated parathormone levels. The associationwith papillary microcarcinoma is considered incidental withno causal relationship between the two pathologies. In thiscase, the presence of high concentration of parathyroidhormone in the cyst fluid was suggestive of the diagnosis [2].
Both these cases reiterate the fact that fine needleaspiration can be misleading whether due to difficulty insampling a rather small cyst in an anatomically critical area,or due to insufficient material obtained.
Thus, from the two cases reported, intrathyroidalparathyroid cysts can either be non-functioning or hyper-functioning in which case they may present with the classicprotean symptoms of hyperparathyroidism.
Whilst the clinical differential diagnosis of an anteriorneck swelling includes cystic thyroid neoplasms, branchial
Fig. 1 a Normal thyroid paren-chyma surrounding the cyst wallindicating the intrathyroidallocation of the cyst. b Althoughthe inner lining of the cyst waslargely denuded of epithelium,focally intact cuboidal liningcells were noted. c Ectopicparathyroid tissue intimatelyassociated with the cyst wall.d CAM5.2 highlighting theremnants of an epithelial liningof the cyst wall
Endocr Pathol (2011) 22:108–111 109

cleft cyst and thyroglossal duct cyst, the main differentialdiagnosis based on morphology lies mainly between anintrathyroid parathyroid cyst and yet another rare entity ofcystic intrathyroid parathyroid adenoma. This distinction isdeemed to be very difficult on pure morphological grounds.Generally, a cystic parathyroid lesion together with either amild hyperparathyroidism or slightly elevated calciumlevels would favour a diagnosis of adenoma.
This re-iterates the importance of multidisciplinary teamapproach in such challenging cases. For the pathologistfacing such a situation, multiple tissue sections need to beexamined to detect or exclude a tumour tissue remnant.
There are as few as 200 cases of cystic parathyroidadenomas reported in the literature [3, 4]. These presentclinically as neck swellings, masquerade as thyroid goitreor mediastinal masses. The majority are non-functioning;however, few cases of hyperfunctioning cystic parathyroidadenomas have been reported further complicating theclinical presentation [5]. Rosenberg et al. [6] found thatthe hyperfunctioning cysts were more common in oldermen while there non-functioning counterparts were morecommon in women.
Morphological studies have shown that increased cyto-plasmic lipid content within parathyroid parenchymaindicates functionally suppressed chief cells [7, 8]. Thissupports the finding in our case of a non-functioning andasymptomatic ectopic parathyroid gland consisting of clearchief cells adjacent to and within the cyst wall.
Although the etiological factors contributing to thedevelopment of these cysts are still unclear, a develop-mental hypothesis is well supported by the embryonicmigration access of these glands. It is conceived thatmost cystic parathyroid lesions develop from pre-existingadenomas undergoing infarction or haemorrhage. Thelongstanding compression on the adenomatous parathy-roid tissue by intraluminal fluid or blood may explain theabsence of parathyroid tissue remnant in the wall of the
cyst encountered in our case. It is worth mentioning thatdegenerate changes sometimes admixed with neoplasticparathyroid cells can be seen in the wall of infractedcystic adenomas.
Parathyroid glands first appear during the fifth week ofgestation [8]. The superior parathyroid glands develop as alocalised proliferation in the fourth pharyngeal pouch oneach side and are finally positioned on the posterior aspectof the lateral lobe of the thyroid gland at about the level ofthe isthmus. While the inferior parathyroid glands developin the third pharyngeal pouch and are pulled by thedeveloping thymic diverticulum until they reach theposterior aspect of the lateral lobe of thyroid gland werethey separate completely from the thymus [9–12]. Thesuperior parathyroid glands have a shorter embryonicmigration access, therefore a more constant location.Although the adult position of the parathyroid glands isvariable, a definite pattern of anatomic distribution canbe predicted in relation to their embryonic derivation[13, 14].
What our case highlights is the close associationbetween the ectopic parathyroid cyst and its vascularsupply. The parathyroid glands normally derive theirarterial supply from the superior and inferior thyroidarteries. This raises the hypothetical possibility of acongenital arrest to the migration of the parathyroid glandand its vascular bundle along the branchiopharyngeal arch,followed by cystic degeneration.
Investigations including nuclear imaging scintigraphy,localisation using technetium-99 m sestamibi imaging, fineneedle aspiration cytology and parathyroid hormone mea-surement in aspirated fluid have been attempted. Fineneedle aspiration cytology is invaluable in the diagnosis ofthyroid neoplasms. It is, however, more difficult to interpretin the context of an intrathyroid parathyroid cyst oradenoma. Rossi et al. highlights in his paper [15] the needto distinguish between thyroid follicular neoplasms,
Table 1 Anatomic distribution of ectopic parathyroid glands
Superior parathyroid glands Inferior parathyroid glands
77% Cricothyroid junction posteriorly Most common Between lower pole of thyroid and the thymus
80% above intersection of recurrent laryngeal nerve and inferior thyroid artery 42–61% Lower thyroid or juxtathyroidal
22% Behind upper pole of thyroid Thymic tongue
Rare Retropharyngeal or retrooesophageal, within thyroid parenchyma Uncommon Mediastinal thymus, anterior mediastinum
Citation Presentation Functionality FNAC PTH
Rickels et al. [1] Nephrolithiasis Hyper-functioning Insufficient
Capezzone et al. [2] Multinodular goitre. Non-functioning Raised
Atwan et al. 2011 Thyroid cyst Non-functioning Not attempted
Table 2 Cases of intrathyroidalpaprathyroid cysts
FNAC fine needle aspirationcytology, PTH parathyroidhormone
110 Endocr Pathol (2011) 22:108–111

medullary thyroid carcinoma and non-functioning intra-thyroid parathyroid adenomas, despite the difficultiesencountered in establishing such a diagnosis on purecytologic grounds, as the management of these threeentities is diverse. Non-functioning intrathyroid parathyroidadenomas can be left alone unless atypical features havebeen detected. In contrast, follicular thyroid neoplasms requirea hemithyroidectomy for the assessment of vascular andcapsular invasion and last but not least medullary thyroidcarcinomas are treated by total thyroidectomy and neckdissection. Rossi further discusses in length that no singlecytologic feature per se is diagnostic but the combination ofthese features: pattern, nuclei, nucleoli, cytoplasma, andcolloid will help the cytopathologist in reaching the rightdiagnosis. Immunocytochemistry for parathyroid hormonewill support the diagnosis of an intrathyroid parathyroidadenomas whilst calcitonin positivity is expected in medullarythyroid carcinoma. A high index of clinical suspicion remainsthe gold standard in these challenging and unusual cases.
Currently, there is no consensus on the management ofectopic intrathyroidal parathyroid cysts as these are veryrare cases often incidentally discovered following surgicalintervention. Perhaps a rational approach would be to applysimilar therapeutic guidelines to intrinsic simple benignthyroid cysts.
References
1. Rickels MR, Langer JE, Mandel SJ. Hyperfunctioning intra-thyroidal parathyroid cyst. J Clin Endocrin Metab 2004;89:1051–1052
2. Capezzone M, Morabito E, Belliti P, Giannosio P, de Santis D,Bruno R. Ectopic intrathyroidal non-functioning parathyroid cyst.Endocr Pract 2007;13:56–58.
3. Sen P, Flower N, Papesch M, Davis A, Spedding AV. A benignparathyroid cyst presenting with hoarse voice. The Journal ofLaryngology & Otology 2000; 114(2): 147–148
4. Jha BC, Nagarkar NM, Kochhar S, Mohan H, Dass A. Parathyroidcyst: a rare cause of an anterior neck mass. The Journal ofLaryngology & Otology 1999; 113(1): 73–75 (s)
5. Captain M, Middleton S, Colonel S. Mistaken identity: cysticparathyroid adenoma masquerading as a goitre. The InternetJournal of Surgery™ 2002; ISSN: 1528–8242
6. Rosenberg J, Orlando R, Ludwig M and Pyrtek L. Parathyroidcysts. The American Journal of Surgery 1982;143(4):473–480
7. Futrell JM, Roth SI, Su SPC, Habener JF, Segre GV, Potts JT Jr.Immunocytochemical localisation of parathyroid hormone inbovine parathyroid glands and human parathyroid adenomas.Am J Pathol 1979;94:615–622.
8. Roth SI, Gallagher MJ. The rapid identification of “normal”parathyroid glands by the presence of intracellular fat. Am JPathol 1976; 84: 521–528.
9. Welsh DA. Concerning the parathyroid glands: a critical anatom-ical and experimental study. J Anat Physiol 1998;32:292–307.
10. Gilmour JR. The embryology of the parathyroid glands, thethymus and certain associated rudiments. J Pathol Bacteriol1937;45:507–522.
11. Weller GL. Development of the thyroid, parathyroid and thymusglands in man. Contrib Embryol 1933;24:93–138.
12. Norris EH. The parathyroid glands and the lateral thyroid in man:their morphogenesis, histogenesis, topographic anatomy andprenatal growth, Contrib Embryol 1937;26:247–294.
13. Norris EH. Anatomical evidence of prenatal function of thehuman parathyroid glands. Anat Rec 1946;96:129–142.
14. Nakagarni K, Yamazaki Y, Tounoda Y. An electron microscopicstudy of the human foetal parathyroid gland. Zellforschung1968;85: 89–95.
15. Rossi ED, Mulè A, Zannoni GF, Fadda G. Asymptomatic intra-thyroidal parathyroid adenoma. Report of a case with a cytologicdifferential diagnosis including thyroid neoplasms. Acta Cytol.2004 May-Jun;48(3):437–440
Endocr Pathol (2011) 22:108–111 111