an unusual malignant thyroid nodule: coexistence of epithelioid angiosarcoma and follicular variant...
TRANSCRIPT

An Unusual Malignant Thyroid Nodule: Coexistenceof Epithelioid Angiosarcoma and FollicularVariant Papillary Thyroid Carcinoma
Mehmet Kefeli & Ozgur Mete
# Springer Science+Business Media New York 2013
Case History
A 40-year-old man noticed a large lump on his left anteriorneck. He underwent repeated fine needle aspiration biopsiesthat were nondiagnostic. There was no previous exposure toionizing radiation or known family history of thyroid cancer.He had a suppressed thyroid stimulating hormone and de-veloped progressive clinical evidence of hyperthyroidism.Thyroid autoantibodies were negative. A thyroid scan dem-onstrated a large cold nodule in the left thyroid. Heunderwent total thyroidectomy.
What is Your Diagnosis? Figure Composite (Figs. 1 and 2)
Clinicopathological Diagnosis: Thyroid Angiosarcomaarising in Follicular Variant Papillary Thyroid Carcinoma
Gross examination of the thyroid confirmed an encap-sulated 7.0 cm nodular lesion in the left lobe. Onhistological examination, this nodule exhibited exten-sive central necrosis surrounded by a rim of viable
neoplastic tissue with minimal capsular invasion. Theviable neoplastic tissue displayed two distinct compo-nents consisting of proliferating epithelioid endothelialcells and follicular epithelial cells (Fig. 1). The follic-ular epithelial proliferation exhibited diagnostic nuclearfeatures of papillary thyroid carcinoma characterized bynuclear membrane irregularities that result in loss ofnuclear roundness in enlarged nuclei (Fig. 1a and b).The second component intermingled with papillary thy-roid carcinoma consisted of anastomosing vascularchannels lined by epithelioid endothelial cells, as wellsolid areas where vascular differentiation was observed(Fig. 1c and d.) The endothelial cells displayed en-larged pleomorphic nuclei, prominent nucleoli, and in-creased mitotic activity (6/10 HPF) including atypicalfigures, consistent with epithelioid angiosarcoma(Fig. 1d). No giant cell change was identified. Thesarcoma component was negative for thyroglobulin,TTF-1, HBME-1, chromogranin-A and calcitonin, andwas positive for factor VIII (diffuse), CD34 (diffuse),CD31 (diffuse), vimentin (diffuse), AE1/AE3, andCK19 (very focal; Fig. 2). The differentiated thyroidcarcinoma component was diffusely positive for thyro-globulin, TTF-1, CK19, AE1/AE3, and vimentin(focal), and was negative for HBME-1, CD34, CD31,factor VIII, chromogranin-A, and calcitonin (Fig. 2).While the MIB-1 LI and p53 expression were 60 and70 % in the sarcoma component, respectively; thesewere 3 and 5 % in the papillary carcinoma, respective-ly. An incidental 0.1 cm papillary microcarcinoma wasalso noted in the right lobe. In summary, this represent-ed an angiosarcoma arising in a follicular variant pap-illary thyroid carcinoma. The absence of other primary
Dr. Kefeli is currently working at the Department of Pathology,Ondokuz Mayis University, Faculty of Medicine, Samsun, Turkey. Hewas involved in this study during his endocrine pathology observershipat University Health Network.
M. Kefeli :O. Mete (*)Department of Pathology, University Health Network,200 Elizabeth Street, 11th floor, Toronto, ON M5G 2C4, Canadae-mail: [email protected]
O. MeteDepartment of Laboratory Medicine and Pathobiology, Universityof Toronto, Toronto, ON, Canada
Endocr PatholDOI 10.1007/s12022-013-9243-1
angiosarcoma on subsequent clinical and radiological inves-tigation excluded the possibility of metastatic angiosarcoma.We suggested that follicular destruction due to mass effectcontributed to our patient’s hyperthyroidism.
Comment
Angiosarcomas are often seen in the skin and superficial softtissue of the head and neck region, especially in elderlypatients with chronic sun damage. Visceral angiosarcomashave been described in many organs including lung, liver,kidney, ovary, testis, and breast, and some of them arelinked to previous irradiation [1, 2]. Primary thyroidangiosarcomas are rare neoplasms and have been describedin the setting of long-standing endemic goiters due to iodinedeficiency [1, 3, 4]. The current case is an unusual exampleof the spectrum of vascular endothelial proliferations of thethyroid gland. Similar to the presented case, angiosarcomaarising in a well-differentiated thyroid carcinoma (follicularcarcinoma) has been described in a 64-year-old man with a4.8-cm nodule [3].
Nodules with previous fine-needle aspirations oftenshow regions of degeneration associated with fibrosisand granulation tissue-like endothelial proliferations [4,5]. Reactive endothelial proliferations can be observedin long-standing goiter; they can display random cyto-logical atypia at sites of degeneration, but often lack ananastomosing vascular growth pattern [4]. Rarely, hem-angiomas similar to those of other locations are seen inthe thyroid gland. The diagnostic workup of a malignantneoplasm with angiomatoid components requires the
distinction of angiosarcoma from other primary malig-nant thyroid neoplasms with angiomatoid features in-cluding medullary thyroid carcinoma (positive for TTF-1, CEA, calcitonin, and general neuroendocrinemarkers), paraganglioma (positive for tyrosine hydroxy-lase and general neuroendocrine markers) and anaplasticthyroid carcinoma (can be positive for keratins andTTF-1), as well as from metastatic sarcomas withangiomatoid features. While the hypothesis that malig-nant neoplasms exhibiting dual differentiation still needsfurther clarification, pathologists have long believed thatmost cases reported as thyroid angiosarcoma were inreality anaplastic thyroid carcinomas with angiomatoidfeatures [1]. In fact, this view is no longer acceptedwhen evidence of endothelial differentiation is provenby positivity for CD31, CD34, or factor VIII-relatedantigen, or by ultrastructural evidence, e.g., Weibel–Palade bodies [1]. One should also be aware that allangiosarcomas may express low-molecular weight kera-tins; however, cytokeratin expression is exclusively seenin epithelioid angiosarcomas [2].
In summary, vascular endothelial proliferations of thethyroid gland encompass a spectrum of morphologicalchanges including granulation tissue-like vascular prolifer-ations, reactive endothelial hyperplasia at sites of degenera-tion as well as neoplastic endothelial proliferations. Whilevascular endothelial proliferations may occur in the back-ground of benign follicular nodular disease, one shouldremember that they can also arise in a well-differentiatedthyroid carcinoma. An immunopanel that includes markersof vascular endothelial differentiation should be used tosolve this quandary.
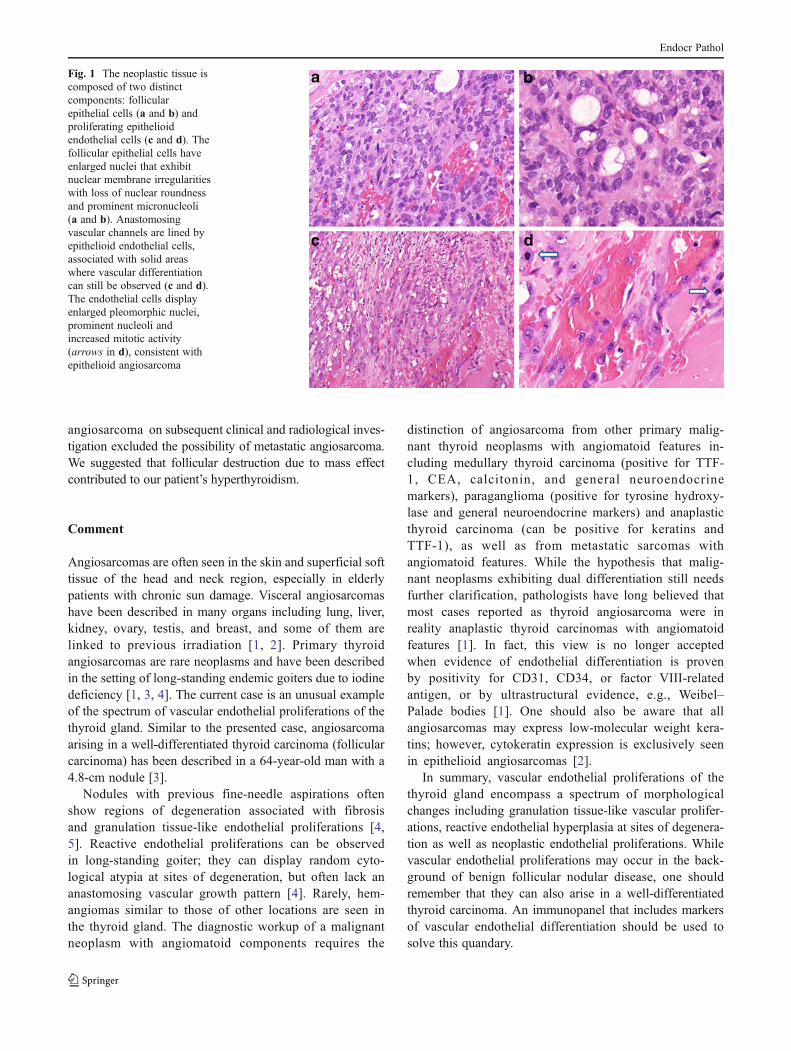
Fig. 1 The neoplastic tissue iscomposed of two distinctcomponents: follicularepithelial cells (a and b) andproliferating epithelioidendothelial cells (c and d). Thefollicular epithelial cells haveenlarged nuclei that exhibitnuclear membrane irregularitieswith loss of nuclear roundnessand prominent micronucleoli(a and b). Anastomosingvascular channels are lined byepithelioid endothelial cells,associated with solid areaswhere vascular differentiationcan still be observed (c and d).The endothelial cells displayenlarged pleomorphic nuclei,prominent nucleoli andincreased mitotic activity(arrows in d), consistent withepithelioid angiosarcoma
Endocr Pathol

References
1. DeLellis RA, Lloyd RV, Heitz PU, Eng C, eds. WorldHealth Organization classification of tumours. Pathologyand genetics of tumours of endocrine organs: IARC Press,Lyon, 2004.
2. Folpe AL, Inwards CY. Bone and soft tissue pathology. Elsevier,Philadelphia, 2010.
3. Kim NR, Ko YH, Sung CO. A case of coexistent angiosarcoma andfollicular carcinoma of the thyroid. J Korean Med Sci 18(6): 908–13;2003.
4. Papotti M, Arrondini M, Tavaglione V, Veltri A, Volante M. Diag-nostic controversies in vascular proliferations of the thyroid gland.Endocr Pathol 19(3): 175–183, 2008.
5. Sapino A, Papotti M, Macrì L, Satolli MA, Bussolati G.Intranodular reactive endothelial hyperplasia in adenomatous goitre.Histopathol 26(5):457–462, 1995.
Fig. 2 a The angiosarcoma component is negative for TTF-1 whereasthe papillary carcinoma is positive for TTF-1. b Thyroglobulin is positivein papillary carcinoma and is negative in the angiosarcoma component. cAE1/AE3 is positive in angiosarcoma. dCD31 highlights the two distinct
components. e Angiosarcoma is strongly positive for CD31. f CD34stains only the normal endocrine vascular network in the papillary carci-noma component. g The angiosarcoma has intense p53 expression,whereas the papillary carcinoma (h) is negative for p53
Endocr Pathol