an overview of prognostic factors for long-term survivors of breast cancer
TRANSCRIPT

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 1/22
REVIEW
An overview of prognostic factors for long-term survivorsof breast cancer
Isabelle Soerjomataram Marieke W. J. LouwmanJacques G. Ribot Jan A. RoukemaJan Willem W. Coebergh
Received: 16 February 2007 / Accepted: 20 February 2007 / Published online: 22 March 2007Ó Springer Science+Business Media B.V. 2007
Abstract Background Numerous studies have examined prognosticfactors for survival of breast cancer patients, but relativelyfew have dealt specically with 10+-year survivors. Methods A review of the PubMed database from 1995 to2006 was undertaken with the following inclusion criteria:median/mean follow-up time at least 10 years; overallsurvival and/or disease-specic survival known; and rela-tive risk and statistical probability values reported. Inaddition, we used data from the long-standing EindhovenCancer Registry to illustrate survival probability as indi-cated by various prognostic factors. Results 10-year breast cancer survivors showed 90% 5-year relative survival. Tumor size, nodal status and graderemained the most important prognostic factors for long-term survival, although their role decreased over time.Most studies agreed on the long-term prognostic values of MI (mitotic index), LVI (lymphovascular invasion), Her2-positivity, gene proling and comorbidity for either all or a
subgroup of breast cancer patients (node-positive or neg-ative). The roles of age, socioeconomic status, histologicaltype, BRCA and p53 mutation were mixed, oftendecreasing after correction for stronger prognosticators,thus limiting their clinical value. Local and regionalrecurrence, metastases and second cancer may substantiallyimpair long-term survival. Healthy lifestyle was consis-tently related to lower overall mortality.Conclusions Effects of traditional prognostic factorspersist in the long term and more recent factors need fur-ther follow-up. The prognosis for breast cancer patientswho have survived at least 10 years is favourable and in-creases over time. Improved long-term survival can beachieved by earlier detection, more effective moderntherapy and healthier lifestyle.
Keywords Breast cancer ÁLong-term ÁPrognostic factors ÁSurvival
Introduction
Breast cancer (BC) is the most common cancer amongwomen, with a lifetime risk of up to 12% and a risk of death of up to 5% [ 1]. Its incidence has been increasing butafter a period of continuous rise in many industrializedcountries BC mortality has been stable or has even de-creased in the last 10–15 years [ 2, 3]. The introduction of mass mammographic screening programmes also resultedin earlier detection and diagnosis of small and lessaggressive tumours. This, in combination with therapeuticimprovements, has led to a substantial increase in BCsurvivors over the last few decades (Fig. 1). A long-termsurvivor is commonly dened as a person who is still alive5 years after cancer diagnosis [ 4]. For BC, the relative
I. Soerjomataram ( & ) ÁJ. W. W. CoeberghDepartment of Public Health, Erasmus MC, P.O. Box 2040,Rotterdam 3000 CA, The Netherlandse-mail: [email protected]
I. Soerjomataram ÁM. W. J. Louwman ÁJ. W. W. CoeberghComprehensive Cancer Centre South, P.O. Box 231, 5600 AEEindhoven, The Netherlands
J. G. RibotDepartment of Radiotherapy Catharina Hospital, P.O. Box 1350,5602 ZA Eindhoven, The Netherlands
J. A. RoukemaDepartment of Surgery, St. Elisabeth Hospital, P.O. Box 90151,5000 LC Tilburg, The Netherlands
123
Breast Cancer Res Treat (2008) 107:309–330DOI 10.1007/s10549-007-9556-1

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 2/22

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 3/22
becoming more common with increasing age [ 13]. Com-pared to those without comorbidity whose 5-year relativesurvival was 87%, those with diabetes mellitus or cardio-vascular disease represented 78% and 83% of the respec-tive survival estimates [ 13]. Patients with severecomorbidity exhibited a 2.7–3.4 higher risk of death in10 years compared to those without comorbidity [ 12, 14].
Period of diagnosis Access to care and treatment of BChas improved over time in most industrialized countries,which is reected in the higher long-term survival of BCcases across all age groups and the tumour characteristicsof those diagnosed more recently [ 15–18]. In Finland,relative survival 10 years after diagnosis among patientsyounger than 50 years increased from 49% for thosediagnosed in 1953–1959 to 68% for the 1983–1989 cohort[15]. Furthermore, 60% of node-positive BC patientsdiagnosed in 1978–1979 in Italy survived 10 years orlonger compared to the 50% probability 10-year survivalfor those diagnosed in 1968–1969 [ 17]. In addition, chan-ges in BC diagnosis, e.g. screening[ 19, 20] and betterstaging [ 17], may partly be responsible for the observedincrease in the proportion of survivors.
Time after diagnosis The longer a woman survives BCthe more the prognosis improves, illustrated by conditionalsurvival [ 16, 21]. Probably the subgroup of patients who
survived longer had less aggressive tumours due to a dif-ferent genetic make-up or better life-style. In Australia,79% of women with localized BC survived 10 years afterdiagnosis, yet among those still alive 5 years after diag-nosis 84% had a 10-year survival [ 16]. The respectivevalues for regional vs. advanced BC were 53% and 68%[16]. Unlike other cancers, relative conditional survivalremained stable below 100% after 12 years of survival anddecreased again after about 19 years (Fig. 3) [5]. This maybe a consequence of late recurrences and metastases,second cancers or late side-effects of treatment [ 23].
Socioeconomic status (SES) and race A population-basedstudy of BC patients diagnosed in 1968–1999 in Franceshowed a diminishing role of SES on excess mortalityamong women with BC over these periods [ 24]. Long-termfollow-up studies reported that women with BC from lowsocial classes had a 20–50% poorer survival compared topatients from higher social classes [ 25, 26], although otherscontradicted this [ 27]. Low SES patients were more likelyto be diagnosed at a later stage, had more aggressive tu-mour characteristics and might have received sub-optimaltreatment. However, differences in these prognostic factorsdid not fully explain the variation in survival according tosocial class [ 25]. This is also the case when breast cancersurvival is studied according to race/ethnicity. Ten yearsafter treatment 58% of African Americans were still alivecompared to 66% of the white Americans. After adjustingfor other prognostic factors, 41% excess mortality from allcauses was still observed among African Americans com-pared to caucasians [ 28]. This suggests other residual fac-tors such as lifestyle (higher body weight was observedamong African Americans), comorbidity [ 14], genetics orvariation in the delivery of treatment, which inuenceoutcome beyond variation in tumour aggressiveness [ 29].
Fig. 2 Relative survival of breast cancer patients (n: 13,279)diagnosed in 1990–2002 and followed until 2004, according to ageat diagnosis in southeastern Netherlands
Fig. 3 Conditional 5-year relative survival (calculated using periodanalysis [ 22] of breast cancer patients diagnosed in southernNetherlands in 1985–2002 and followed until 2004, according toage. ( Dashed line ): diagnosed at 25–49 years, ( solid line ): diagnosedat 50–74 years
Breast Cancer Res Treat (2008) 107:309–330 311
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 4/22
Tumour-related characteristics
Tumour size Tumour size is one of the strongest prog-nostic indicators (Fig. 4) [7, 30], even after 20 years of follow-up [ 8, 31]. A larger tumour has been related to morepositive lymph nodes [ 32], thus their interaction furtherinuences the survival from BC. Nonetheless, the inde-
pendence of survival by node status is shown by the lower10-year overall survival rate found for node-negative pa-tients with a tumour of 2–5 cm compared to those with atumour smaller than 1 cm, 66% vs. 79%, respectively [ 33].
Histological type The prognostic value of histologicaltype can be grouped into four: excellent, good, poor andvery poor prognosis [ 34]. BC with an excellent prognosis,such as invasive cribriform, tubular [ 35], tubulo-lobularand mucinous [ 36, 37] showed >80% survival at 10 years[9]. Tubular mixed, mixed ductal with special type, atyp-
ical medullary [ 38] and alveolar lobular carcinoma have agood prognosis with a 60–80% 10-year survival. Thosewith invasive papillary, classic lobular and medullarycancers have a worse prognosis. Finally, 10-year survivalamong those with ductal, solid lobular, mixed ductal andlobular carcinoma is below 50% [ 34]. In most populationsinltrating ductal carcinoma covers about 70% of alldiagnoses [ 36, 39]. Inammatory BC has a particularlypoor prognosis: about 30% survived 10 years [ 40].
Histological grade The most widely used grading sys-
tems are Scarff-Bloom-Richardson classication, Fishergrading nuclear system and Nottingham Combined Histo-logic Grade (NCHG) [ 41]. The validity of grading has beensubjected to inter-observer reproducibility and subjectivity
[42]. However, higher grades have been quite consistentlyassociated with lower long-term survival [ 7, 8, 31, 43–45].Depending on other prognostic factors, such as nodal statusor tumour size [ 46, 47], cumulative survival among pa-tients with the lowest score was 90–94% 10 years afterdiagnosis and 30–78% among those with the highest score[37, 48].
Regional lymph node involvement Lymph node involve-ment is a valuable indicator of long-term survival (Fig. 5)[8, 32]. Node- positive patients have about a 4–8 timeshigher mortality than those without nodal involvement[8, 9, 49]. The more nodes involved the worse the prog-nosis. Prognosis for patients with 10 or more involvedaxillary nodes showed 70% more deaths at 10 years thanfor those with 1–3 involved nodes [ 32]. The survival of node-positive patients improved due to better staging pro-cedures and application of systemic treatment [ 7, 31, 50].
Lymphovascular invasion (LVI) and molecular markers of tumours angiogenesis At the St. Gallen meeting in 2005,LVI was added to the prognostics for node-negative pa-tients [ 51]. Compared to patients having no LVI, a 60%higher BC mortality was observed for node-negative BCpatients having positive LVI [ 52, 53], although others didnot observe the independent role of LVI [ 46, 50]. In thisline of research, studies have also focused on the value of microvessel density [ 44], blood invasion (BVI) [ 54] andmarkers of angiogenesis (VEGFR (vascular endothelial
growth factor receptor), CD105, Tie-2) [ 55, 56] in pre-dicting long-term survival of BC patients, although theresults are still conicting.
Fig. 4 Cumulative survival proportion of breast cancer patientsdiagnosed in southern Netherlands in 1970–1994 and followed until2004, according to tumor size (based on pathological diagnosis). n
tumor size: <2 cm (n: 3263) • tumor size: 2–5 cm (n: 3420) m tumorsize: >5 cm (n: 474) x tumor size: involvement of skin (n: 1133) andunknown/not applicable tumor size: 1410
Fig. 5 Cumulative survival proportion of breast cancer patientsdiagnosed in southern Netherlands in 1970–1994 and followed until2004, according to nodal status (based on pathological diagnosis). n
node negative (n: 4452) • node status: 1–3 positive nodes (n: 3266) m
node status: 4–9 positive nodes (n: 255) x node status: 10+ positivenodes (n: 189), unknown/not applicable node status: 1538
312 Breast Cancer Res Treat (2008) 107:309–330
123
7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 5/22
Grouped prognostic factors Some of the prognosticfactors have been combined into a prognostic index, suchas the TNM classication and also the more current Not-tingham Prognostic Index (NPI), both highly predictive forestimating long-term survival [ 41]. TNM staging consistsof information on primary tumour size, involvement of theregional lymph node and the presence of distant metastasis.
Only 53% of patients with regional or locally advanced BChad survived 10 years after diagnosis compared to 79% of those with localised BC [ 16]. Patients with metastasis(stage: M1) at diagnosis exhibited very poor 10-yearsurvival (3.4%) [ 57].
Tumour size, grade and lymph node status make up theNPI [ 11 , 46, 49]. In a large series of 2879 BC patients,10-year survival proportion was 85% for those with thelowest NPI score and 19% for those with the highest score[11 ].
Recurrence, metastasis and second cancer
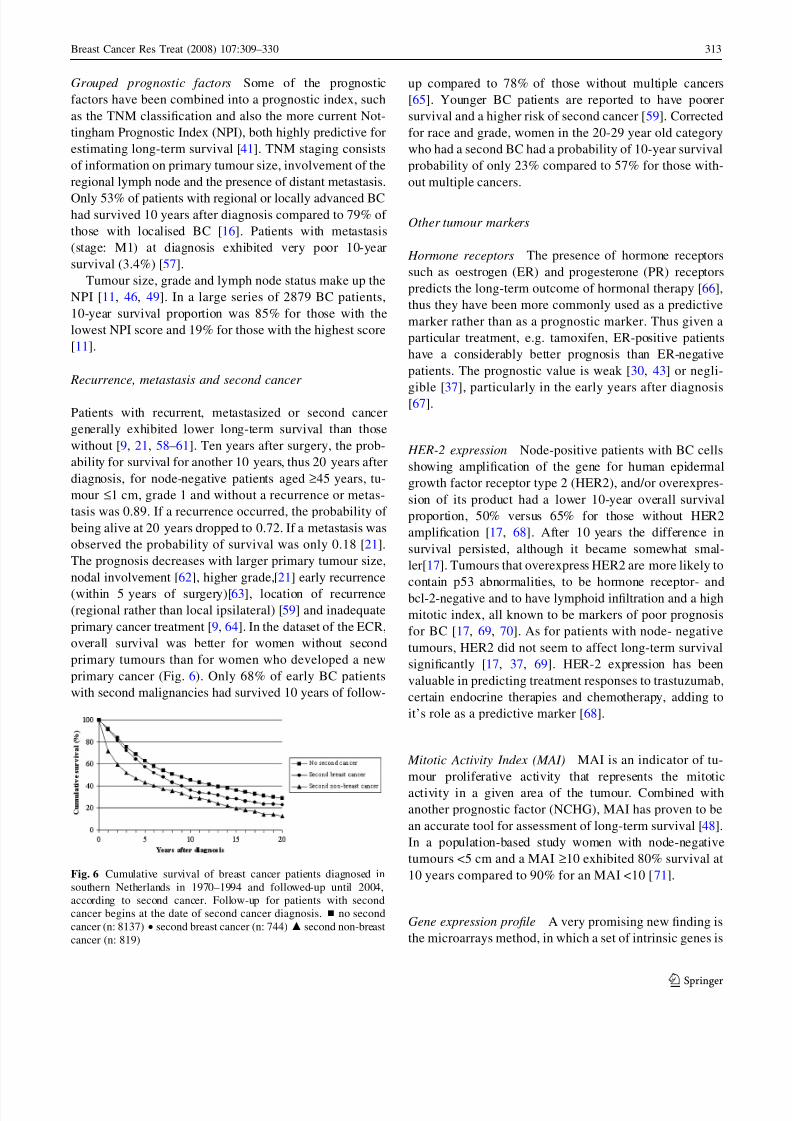
Patients with recurrent, metastasized or second cancergenerally exhibited lower long-term survival than thosewithout [ 9, 21, 58–61]. Ten years after surgery, the prob-ability for survival for another 10 years, thus 20 years afterdiagnosis, for node-negative patients aged ‡ 45 years, tu-mour £ 1 cm, grade 1 and without a recurrence or metas-tasis was 0.89. If a recurrence occurred, the probability of being alive at 20 years dropped to 0.72. If a metastasis wasobserved the probability of survival was only 0.18 [ 21].The prognosis decreases with larger primary tumour size,nodal involvement [ 62], higher grade,[ 21] early recurrence(within 5 years of surgery)[ 63], location of recurrence(regional rather than local ipsilateral) [ 59] and inadequateprimary cancer treatment [ 9, 64]. In the dataset of the ECR,overall survival was better for women without secondprimary tumours than for women who developed a newprimary cancer (Fig. 6). Only 68% of early BC patientswith second malignancies had survived 10 years of follow-
up compared to 78% of those without multiple cancers[65]. Younger BC patients are reported to have poorersurvival and a higher risk of second cancer [ 59]. Correctedfor race and grade, women in the 20-29 year old categorywho had a second BC had a probability of 10-year survivalprobability of only 23% compared to 57% for those with-out multiple cancers.
Other tumour markers
Hormone receptors The presence of hormone receptorssuch as oestrogen (ER) and progesterone (PR) receptorspredicts the long-term outcome of hormonal therapy [ 66],thus they have been more commonly used as a predictivemarker rather than as a prognostic marker. Thus given aparticular treatment, e.g. tamoxifen, ER-positive patientshave a considerably better prognosis than ER-negativepatients. The prognostic value is weak [ 30, 43] or negli-
gible [ 37], particularly in the early years after diagnosis[67].
HER-2 expression Node-positive patients with BC cellsshowing amplication of the gene for human epidermalgrowth factor receptor type 2 (HER2), and/or overexpres-sion of its product had a lower 10-year overall survivalproportion, 50% versus 65% for those without HER2amplication [ 17, 68]. After 10 years the difference insurvival persisted, although it became somewhat smal-ler[ 17]. Tumours that overexpress HER2 are more likely tocontain p53 abnormalities, to be hormone receptor- andbcl-2-negative and to have lymphoid inltration and a highmitotic index, all known to be markers of poor prognosisfor BC [ 17, 69, 70]. As for patients with node- negativetumours, HER2 did not seem to affect long-term survivalsignicantly [ 17, 37, 69]. HER-2 expression has beenvaluable in predicting treatment responses to trastuzumab,certain endocrine therapies and chemotherapy, adding toit’s role as a predictive marker [ 68].
Mitotic Activity Index (MAI) MAI is an indicator of tu-mour proliferative activity that represents the mitoticactivity in a given area of the tumour. Combined withanother prognostic factor (NCHG), MAI has proven to bean accurate tool for assessment of long-term survival [ 48].In a population-based study women with node-negativetumours <5 cm and a MAI ‡ 10 exhibited 80% survival at10 years compared to 90% for an MAI <10 [ 71].
Gene expression prole A very promising new nding isthe microarrays method, in which a set of intrinsic genes is
Fig. 6 Cumulative survival of breast cancer patients diagnosed insouthern Netherlands in 1970–1994 and followed-up until 2004,according to second cancer. Follow-up for patients with secondcancer begins at the date of second cancer diagnosis. n no secondcancer (n: 8137) • second breast cancer (n: 744) m second non-breastcancer (n: 819)
Breast Cancer Res Treat (2008) 107:309–330 313
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 6/22
clustered and segregated into major subgroups; BC with agood and poor prognosis prole is correlated to the prob-ability of distant metastases [ 72] or a tumour with basal orluminal characteristics which are strongly associated withER status [ 73]. In a study of 295 patients diagnosed withstage I or II breast cancer, those classied as having a goodprognosis prole had a 95% overall 10-year survival ratecompared to 55% for those with a poor prole [ 74]. Thisclassication predicted outcome regardless of the nodalstatus, implying that more accurate criteria have becomeavailable for administering adjuvant systemic treatment.
Various molecular markers BRCA1 & 2 mutations wererst identied in 1994 and are BC risk factors for somespecic groups [ 75]. Their role as prognostic indicator forlong-term (more than 10-year) survival has not yet beenestablished. A study of 496 women (median follow-up:116 months), 56 of whom (11%) carried a BRCA1/BRCA2
mutation, showed worse BC-specic survival for womenwith BRCA1 mutations than for those without (62% at10 years versus 86%; P < 0.0001), but not for women withthe BRCA2 mutation [ 76]. However, another study whichcompared patients from BRCA1, BRCA2 and non-BRCA1/2 families as well as sporadic cases did not con-rm the prognostic role of BRCA1/2 [ 77].
Long-term follow-up studies have not demonstrated anindependent effect of p53 mutations on long-term survival.The P53 mutation was related to a poor clinical prole forpatients, hence in multivariate analysis its role on survivaldiminished [ 10, 69, 78, 79].
A high level of tissue urokinase-type plasminogenactivator (uPA) and its inhibitors has been correlated withpoor outcome for node-negative and node-positive patients.Those having the highest level of uPA have a ve timesgreater risk of dying from BC compared to those with thelowest level [ 69]. Other factors such as Ki67 (MIB-1),cathepsin-D, DNA ploidy and S-phase have been suggestedas prognosticators of survival, with conicting results,particularly among long-term survivors. Their use in gen-eral clinical settings is therefore not recommended [ 80, 81].
Miscellaneous
Lifestyle Generally, increased death rates due to BC(13–20%), other causes (49–86%) and all causes(14–70%) have been observed among obese patients[82–85]. Normal body weight tended be more benecialin death from other causes than from BC: [ 83, 84] 9.5%of obese patients died from non-BC causes compared to6.4% and 5.8%, respectively, of the normal or interme-diate groups [ 82]. Obesity was also related to a 2-foldincreased risk of postmenopausal contralateral BC and a
60% higher occurrence of second other cancers [ 84].Therefore, normal weight may reduce the risk of secondpost-menopausal BC, second other cancers and overallmortality [ 83, 84, 86].
Compared with women who engaged in less than 9metabolic equivalent task (MET)-hours per week of activity, women who engaged in 9 or more MET-hours perweek had a 40% lower risk of death from all causes,translating into a 6% absolute (unadjusted) reduction inmortality [ 87], which emphasizes the need to advisephysical activity.
So far, although studies have not convincingly shownthe positive inuence of eating fruit, vegetables and soybean on long-term BC survival [ 85, 88], diets high in fruits,vegetables, legumes, poultry, and sh and a low intake of red meat, desserts and high fat dairy products are likely toprotect against mortality from non-BC causes [ 89].
Modication of BC’s prognostic factors
Various studies have questioned the role of BC risk factorsin determining the biological tumour features as mentionedabove. Indeed, BC risk factors seem to differ according tohistological type, grade, size, nodal status and ER/PRreceptor status [ 90–93]. For example, excessive alcoholintake and obesity increased the risk for the development of ER-positive tumours [ 92, 93]. As for late age at rst full-term birth and obesity are related to an increased risk of large tumours [ 91]. Hence, risk factors for BC may alsoaffect breast biology and clinical behaviour, thus also BC
prognosis.
Changing importance of prognostic factors over timeafter diagnosis
Commonly, the value of prognostic factors decreasesdepending on the length of the follow-up period [ 31, 94].Survival curves according to prognostic factors usuallyshow a large drop in survival for all stages during the rst5 years; afterwards the curve stabilizes. Studies agreed onthe long-lasting inuence of tumour size at diagnosis onsurvival, albeit attenuating over time [ 31, 94, 95]. Grade,nodal status and metastases were also valuable in predict-ing survival up to 20 years after diagnosis [ 31, 95]. Al-though, others have reported that 10 years after diagnosisonly tumour size [ 94] or nodal status [ 8] or old age [ 8]remained as an independent predictor of long-term sur-vival. Similarly, ER/PR status and MAI only had a sig-nicant prognostic role in the rst 5–10 years afterdiagnosis [ 67, 71, 96]. Because even 10 years after BCdiagnosis the probability of survival for BC patients doesnot seem to reach that of the general population, the role of
314 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 7/22
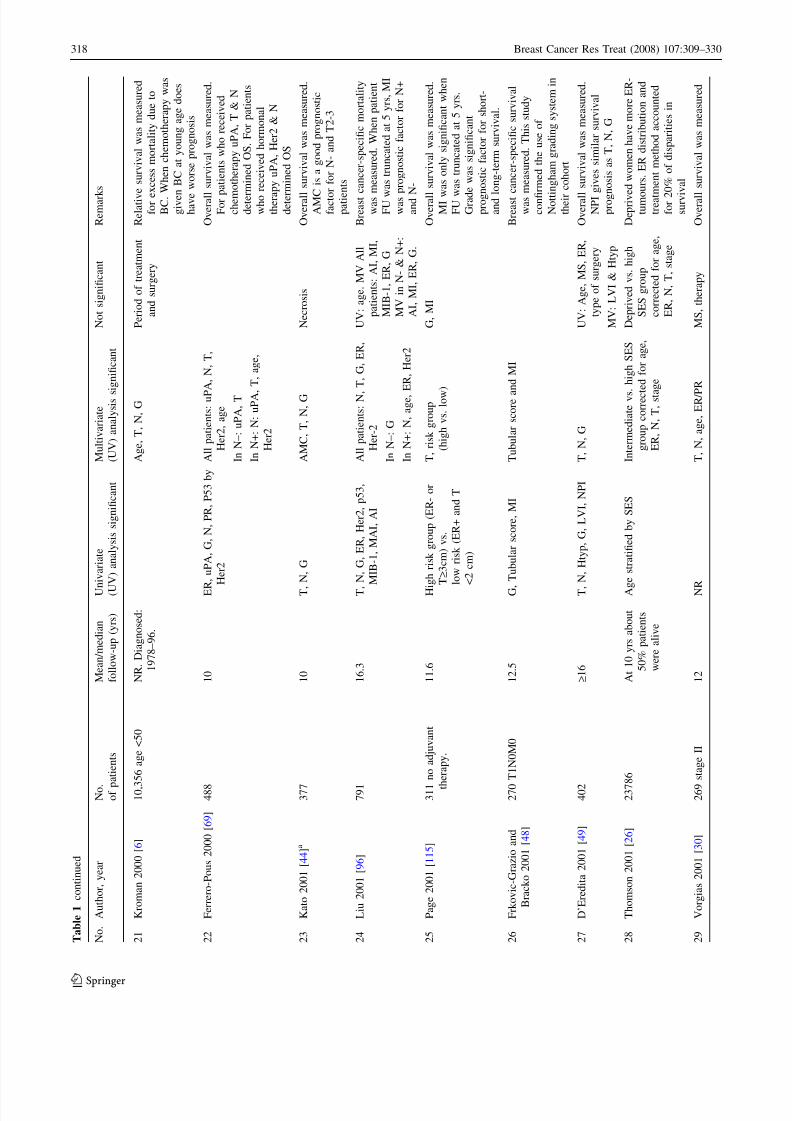
T a
b l e 1
O v e r v i e w o f s t u d i e s r e p o r t i n g l o n g - t e r m p r o g n o s t i c f a c t o r s f o r b r e a s t c a n c e r ( B C ) p a t i e n t s
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
1
H a e r s l e v a n d J a c o b s e n
1 9 9 5 [ 7 0 ] a
4 9 0
1 0 . 6
M S , T , N
, H t y p ,
M I , G
, P R , H
e r 2
A l l p a t i e n t s : N & P R
I n N + : M I & P R
I n N - : M
S & G
H e r 2
O v e r a l l s u r v i v a l w a s m e a s u r e d .
P 5 3 w a s r e l a t e d t o a b s e n c e o f
t u b u l a r f o r m a t i o n , h i g h G
,
E R - n e g a t i v e , h i g h P C N A
( p r o l i f e r a t i n g c e l l n u c l e a r
a n t i g e n ) s c o r e
2
P i e t i l a i n e n 1 9 9 5 [ 1 0 ]
3 9 2
1 1 . 1
P 5 3 , N
, T , H t y p , t u b u l a r
f o r m a t i o n , i n t r a d u c t a l
g r o w t h ,
m a r g i n f o r m a t i o n ,
n e c r o s i s , D N A p l o i d y ,
S - p h a s e f r a c t i o n
A l l p a t i e n t s : N , T , M I
I n N + : T , M I
I n N – : T , p 5 3 , G
O v e r a l l s u r v i v a l w a s m e a s u r e d .
P 5 3 i s r e l a t e d t o y o u n g e r a g e ,
M I , A I , G
, n u c l e a r
p l e o m o r p h i s m
3
H a e r s l e v 1 9 9 5 [ 7 9 ] a
4 9 0
1 1
P C N A
T , G
, P R
H e r 2 & P C N A
( P r o l i f e r a t i n g
c e l l n u c l e a r
a n t i g e n )
O v e r a l l s u r v i v a l w a s m e a s u r e d .
P R w a s o n l y a n i n d e p e n d e n t
f a c t o r i n N - p o s i t i v e p t s . H e r 2
& P C N A w e r e r e l a t e d t o m o r e
p o s i t i v e N
, h i g h e r G , E R - / P R -
n e g a t i v e
4
G a m e l 1 9 9 6 [ 3 9 ]
1 6 3 , 8 0 8
N R
. R a n g e
1 m o s - 1 9 y r s
H i s t o l o g i c a l t y p e
b y s t a g e ( l o c a l i z e d &
r e g i o n a l B C )
B r e a s t c a n c e r s p e c i c s u r v i v a l
w a s m e a s u r e d
5
W e s t 1 9 9 6 [ 1 2 ]
1 1 9 6
N R
. D i a g n o s e d :
1 9 7 3 – 1 9 8 6 .
E n d F U : 1 9 9 4 . C
o m o r b i d i t y
L e v e l o f c o m o r b i d i t y
A d j u s t e d f o r a g e ,
r a c e , s t a g e ,
N , t h e r a p y .
V a l u e s f o r t h e s e
f a c t o r s w e r e n o t
s h o w n
O v e r a l l s u r v i v a l w a s m e a s u r e d .
C h a r l s o n c o m o r b i d i t y i n d e x
w a s u s e d . T h e r e i s n o
d i f f e r e n c e i n t h e s i g n i c a n c e
o f c o m o r b i d i t y o n s u r v i v a l o f
C a u c a s i a n s a n d A f r i c a n
A m e r i c a n ( A A )
6
H a e r s l e v 1 9 9 6 [ 1 1 2 ] a
4 8 7
> 1 0
K i - 6 7 , P C N A
T , G
, P R
K i - 6 7 & P C N A
.
O v e r a l l s u r v i v a l w a s m e a s u r e d .
P R o n l y a n i n d e p e n d e n t f a c t o r
f o r N + p a t i e n t s . K i - 6 7 w a s
r e l a t e d t o T , M I , G
7
N o r t h r i d g e 1 9 9 7 [ 3 6 ]
M u c i n o u s B C : 4 0 8 2 .
I n l t r a t i n g d u c t B C :
1 3 9 , 1 5 4
N R
. D i a g n o s e d :
1 9 7 3 – 1 9 9 0
H T y p , p e r i o d o f d i a g n o s i s ,
S t a g e , G
A g e
B r e a s t c a n c e r s p e c i c s u r v i v a l
w a s m e a s u r e d
8
K o l l i a s 1 9 9 7 [ 1 1 ] a
2 8 7 9 a g e £ 7 0 , T < 5 c m
> 1 0
A g e < 3 5 , N P I
T , G
, N
A g e
O v e r a l l s u r v i v a l w a s m e a s u r e d .
Y o u n g e r t h a n 3 5 y r s h a d
h i g h e r g r a d e , m o r e L V I a n d
w o r s e N P I g r o u p . A f t e r 1 0 y r s
N P I d i d n o t c h a n g e O S
Breast Cancer Res Treat (2008) 107:309–330 315
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 8/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
9
Z a h l a n d T r e t l i 1 9 9 7
[ 9 5 ]
8 8 0 2 a g e < 7 0
D i a g n o s e d :
1 9 6 5 – 7 4 . E n d
F U : 1 9 9 1
S u r v i v a l
c a t e g o r i z e d b y a g e ,
s t a g e a n d
f o l l o w - u p t i m e
E x c e s s h a z a r d f r o m b r e a s t
c a n c e r w a s m e a s u r e d . A f t e r
8 y r s
b e i n g y o u n g e r t h a n
3 5 d o e s n o t i n u e n c e
s u r v i v a l . S t a g e w a s a n
i m p o r t a n t p r o g n o s t i c a t o r u p t o
2 0 y r s
1 0
P i n d e r 1 9 9 8 [ 4 7 ]
4 6 5
1 2
N b y g r a d e ,
T r e a t m e n t b y g r a d e
O v e r a l l s u r v i v a l w a s m e a s u r e d .
T h e s t u d y a i m e d t o c o n r m
v a l u e o f N o t t i n g h a m g r a d i n g
s y s t e m f o r s u r v i v a l . N + G 3
p a t i e n t s b e n e t e d f r o m
p r o l o n g e d c h e m o t h e r a p y
1 1
G a f f n e y 1 9 9 8 [ 1 1 3 ]
B R C A 1 : 3 0
B R C A 2 : 2 0
C o n t r o l : 1 8 2 7 8
B C p t s
B R C A 1 : 9 . 8
B R C A 2 : 7 . 5
C o n t r o l : N R
B R C A 1 v s . B R C A 2
v s . c o n t r o l
O v e r a l l s u r v i v a l w a s m e a s u r e d
C a s e a n d c o n t r o l w e r e m a t c h e d
f o r d a t e o f b i r t h , d a t e o f
d i a g n o s i s a n d t u m o u r s i z e .
P a t i e n t s w i t h B R C A + w e r e
y o u n g e r . P a t i e n t s w i t h B R C A 1
h a d h i g h e r g r a d e
1 2
W o j c i k 1 9 9 8 [ 2 8 ]
6 5 7 7 p a t i e n t s
W h i t e s : 5 8 7 9
A f r i c a n A m e r i c a n ( A A ) :
6 9 8
A t 1 0 y r s 5 9 –
6 7 % p a t i e n t s
w e r e a l i v e
R a c e , G
, N , T ,
s t a g e ,
w a i t i n g t i m e ,
s m o k i n g , b e i n g a w i d o w
,
h a v i n g
o t h e r f a m i l y a s
d e p e n d e n t
R a c e , a g e , s t a g e
U V : a l c o h o l , f a m i l y
h i s t o r y
O v e r a l l s u r v i v a l w a s m e a s u r e d .
A A i s m o r e l i k e l y t o b e
y o u n g e r a t d i a g n o s i s , h a v e
l a r g e r t u m o u r , h i g h e r s t a g e
a n d m o r e l y m p h n o d e s
1 3
M a n s i 1 9 9 9 [ 1 1 4 ]
3 5 0
1 2 . 5
B o n e m a r r o w
m i c r o m e t a s t a s e s
N , T
B o n e m a r r o w
m i c r o m e t a s t a s e s ,
L V I
O v e r a l l a n d b r e a s t c a n c e r -
s p e c i c s u r v i v a l w a s
m e a s u r e d . B o n e m a r r o w
m e t a s t a s e s m a y b e u s e f u l a s
p r o g n o s t i c f a c t o r f o r B C p t s
w i t h o u t i n f o r m a t i o n o n T a n d
N
1 4
K o l l i a s 1 9 9 9 [ 4 6 ] a
3 1 9 T £ 1 c m
> 1 0
G , N , L V
I , N P I
G , N
L V I
O v e r a l l s u r v i v a l w a s m e a s u r e d
1 5
T a b a r 1 9 9 9 [ 4 5 ]
2 4 6 8
N R
. D i a g n o s e d :
1 9 7 7 – 8 5 . E n d
F U : 1 9 9 6
T , N
, G , d e t e c t i o n
m o d e , H T y p
T X N
, a g e * N , H
t y p * N ,
T * N * G
O v e r a l l s u r v i v a l w a s m e a s u r e d .
S c r e e n i n g a r r e s t s d i s e a s e
p r o g r e s s i o n . T u m o u r
p r o g r e s s i o n i s m o r e r a p i d i n
B C p a t i e n t s < 5 0 y r s . O S o f
T 1 a ( 1 – 5 m m ) v s .
T 1 b ( 6 – 1 0 m m ) N S .
316 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 9/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
1 6
H o l m e s 1 9 9 9 [ 8 5 ]
1 9 8 2
1 3 . 1
B M I ‡ 3 0
3 r d t o 5 t h q u i n t i l e
o f p r o t e i n p r o t e i n
i n t a k e a f t e r
d i a g n o s i s , N , T , G
B M I , p r o t e i n i n t a k e
p r i o r d i a g n o s i s , a l c o h o l
i n t a k e
A l l c a u s e m o r t a l i t y w a s
m e a s u r e d . M V f o r B M I w a s
c o r r e c t e d f o r a g e , d i e t
i n t e r v a l , o r a l c o n t r a c e p t i v e
u s e , h o r m o n e r e p l a c e m e n t
t h e r a p y , M S , a g e a t m e n a r c h e ,
a g e t a t b i r t h a n d p a r i t y ,
s m o k i n g , T , G
, N , E R , P R
B M I < 2 1 a n d 1 s t q u i n t i l e o f
p r o t e i n i n t a k e w e r e r e f e r e n c e .
S i g n i c a n t t r e n d o f h i g h e r
m o r t a l i t y f r o m l o w e s t t o
h i g h e s t q u i n t i l e s o f b r e ,
l u t e i n a n d z e a x a n t h i n ,
c a l c i u m a n d p r o t e i n i n t a k e ,
w i t h 1 3 – 3 5 % l o w e s t m o r t a l i t y
i n t h e l o w e s t q u i n t i l e
1 7
N o m u r a 1 9 9 9 [ 5 8 ]
1 8 5 7 < 8 0 y r s
s t a g e I - I I I
1 2
S e c o n d c a n c e r
a n d r e c u r r e n c e
A g e , E R
, N , r e c
u r r e n c e ,
s e c o n d c a n c e r
O v e r a l l s u r v i v a l w a s m e a s u r e d
R e c u r r e n c e i s r e l a t e d t o h i g h e r
s t a g e , y o u n g e r a g e
a t
d i a g n o s i s , H t y p , a n d t h e r a p y .
S e c o n d c a n c e r i s r e l a t e d t o
y o u n g e r a g e . D e a t h r e l a t e d t o
r e c u r r e n c e a n d s e c o n d c a n c e r
i s i n c r e a s e d 1 2 y r s a f t e r
d i a g n o s i s .
1 8
R e e d 1 9 9 9 [ 3 7 ]
6 1 3 T 1 - 2 N 0
1 5 . 5
A g e > 5 0 , T , G
G , T ,
t r e a t m e n t
U V : t r e a t m e n t , E R
,
P R , H
e r 2 , P 5 3
O v e r a l l s u r v i v a l w a s m e a s u r e d .
H e r 2
w a s r e l a t e d t o P R - ,
E R -
n e g a t i v e , P 5 3 , G
. P 5 3 w a s
r e l a t e d t o P R - .
T r e a t m e n t w a s
o v a r i a n & l o c o r e g i o n a l
i r r a d i a t i o n t h a t h a d l o w e r
m o r t a l i t y r a t e
1 9
A e b i 2 0 0 0 [ 7 ]
3 7 0 0 p r e - &
p e r i m e n o p a u s a l
1 2
A g e < 3 5 v s . ‡ 3 5
N , T ,
G , a g e < 3
5 * E R +
A g e , E R
O v e r a l l s u r v i v a l w a s m e a s u r e d .
Y o u n g e r p a t i e n t s w i t h E R +
w h o w e r e n o t a m e n o r r h o e a
h a d a s i g n i c a n t l y s h o r t e r
s u r v i v a l
2 0
F e r r e r o 2 0 0 0 [ 7 8 ]
2 9 7 N -
1 1
T , E R
, P 5 3
T , E R
A g e , P R
, G
B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d . P 5 3 w a s
r e l a t e d t o g r a d e , T , E R -
n e g a t i v e . P 5 3 w a s c o n t i n u o u s
v a r i a b l e
Breast Cancer Res Treat (2008) 107:309–330 317
123
7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 10/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
2 1
K r o m a n 2 0 0 0 [ 6 ]
1 0 , 3 5 6 a g e < 5 0
N R
. D i a g n o s e d :
1 9 7 8 – 9 6 .
A g e , T , N
, G
P e r i o d o f t r e a t m e n t
a n d s u r g e r y
R e l a t i v e s u r v i v a l w a s m e a s u r e d
f o r e x c e s s m o r t a l i t y d u e t o
B C . W h e n c h e m o t h e r a p y w a s
g i v e n B C a t y o u n g a g e d o e s
h a v e w o r s e p r o g n o s i s
2 2
F e r r e r o - P o u s 2 0 0 0 [ 6 9 ] 4 8 8
1 0
E R , u P A , G , N , P R , P 5 3
b y
H e r 2
A l l p a t i e n t s : u P A
, N , T ,
H e r 2 , a g e
I n N – : u P A , T
I n N + : N : u P A , T , a g e ,
H e r 2
O v e r a l l s u r v i v a l w a s m e a s u r e d .
F o r p a t i e n t s w h o r e c e i v e d
c h e m o t h e r a p y u P A , T
& N
d e t e r m i n e d O S . F o r p a t i e n t s
w h o r e c e i v e d h o r m o n a l
t h e r a p y u P A , H
e r 2 & N
d e t e r m i n e d O S
2 3
K a t o 2 0 0 1 [ 4 4 ] a
3 7 7
1 0
T , N
, G
A M C
, T , N
, G
N e c r o s i s
O v e r a l l s u r v i v a l w a s m e a s u r e d .
A M C
i s a g o o d p r o g n o s t i c
f a c t o r f o r N - a n d T 2 - 3
p a t i e n t s
2 4
L i u 2 0 0 1 [ 9 6 ]
7 9 1
1 6 . 3
T , N
, G , E R , H
e r 2 , p 5 3 ,
M I B - 1 , M
A I , A I
A l l p a t i e n t s : N , T , G
, E R ,
H e r - 2
I n N – : G
I n N + : N , a g e ,
E R , H
e r 2
U V : a g e . M V A l l
p a t i e n t s : A I , M I ,
M I B - 1 , E R , G
M V i n N -
& N + :
A I , M I , E R
, G .
B r e a s t c a n c e r - s p e c i c m o r t a l i t y
w a s m e a s u r e d . W h e n p a t i e n t
F U w a s t r u n c a t e d a t 5 y r s , M I
w a s p r o g n o s t i c f a c t o r f o r N +
a n d N -
2 5
P a g e 2 0 0 1 [ 1 1 5 ]
3 1 1 n o a d j u v a n t
t h e r a p y .
1 1 . 6
H i g h r i s k g r o u p ( E R - o r
T ‡ 3 c m ) v s .
l o w r i s k ( E R + a n d T
< 2 c m )
T , r i s k g r o u p
( h i g h v s . l o w )
G , M
I
O v e r a l l s u r v i v a l w a s m e a s u r e d .
M I w a s o n l y s i g n i c a n t w h e n
F U w
a s t r u n c a t e d a t 5 y r s .
G r a d e w a s s i g n i c a n t
p r o g n o s t i c f a c t o r f o r s h o r t -
a n d l o n g - t e r m s u r v i v a l .
2 6
F r k o v i c - G r a z i o a n d
B r a c k o 2 0 0 1 [ 4 8 ]
2 7 0 T 1 N 0 M 0
1 2 . 5
G , T u b u l a r
s c o r e , M I
T u b u l a r s c o r e a n d M I
B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d . T h i s s t u d y
c o n r m e d t h e u s e o f
N o t t i n g h a m g r a d i n g s y s t e m i n
t h e i r c o h o r t
2 7
D ’ E r e d i t a 2 0 0 1 [ 4 9 ]
4 0 2
‡ 1 6
T , N
, H t y p , G
, L V I , N P I
T , N
, G
U V : A g e , M S , E R
,
t y p e o f s u r g e r y
M V : L V I & H t y p
O v e r a l l s u r v i v a l w a s m e a s u r e d .
N P I g i v e s s i m i l a r s u r v i v a l
p r o g n o s i s a s T , N
, G
2 8
T h o m s o n 2 0 0 1 [ 2 6 ]
2 3 7 8 6
A t 1 0 y r s a b o u t
5 0 % p a t i e n t s
w e r e a l i v e
A g e s t r a t i e d b y S E S
I n t e r m e d i a t e v s . h i g h
S E S
g r o u p c o r r e c t e d f o r a g e ,
E R , N , T ,
s t a g e
D e p r i v e d v s . h i g h
S E S g r o u p
c o r r e c t e d f o r a g e ,
E R , N , T ,
s t a g e
D e p r i v e d w o m e n h a v e m o r e E R -
t u m o u r s . E R d i s t r i b u t i o n a n d
t r e a t m e n t m e t h o d a c c o u n t e d
f o r 2 0 % o f d i s p a r i t i e s i n
s u r v i v a l
2 9
V o r g i a s 2 0 0 1 [ 3 0 ]
2 6 9 s t a g e I I
1 2
N R
T , N
, a g e , E R / P R
M S , t h e r a p y
O v e r a l l s u r v i v a l w a s m e a s u r e d
318 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 11/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
3 0
V i n c e n t - S a l o m o n 2 0 0 1
[ 4 3 ]
6 8 5 T £ 3 c m
1 0 . 8
G , N , E R , n e c r o s i s
N , n e c r o s i s ,
G
U V : V a s c u l a r
d e n s i t y , L V I , a g e ,
P R
O v e r a l l s u r v i v a l w a s m e a s u r e d .
I n t r a t u m o r a l v a s c u l a r d e n s i t y
w a s r e l a t e d t o l a r g e r t u m o u r
s i z e a n d h i g h e r g r a d e
3 1
E e r o l a 2 0 0 1 [ 7 7 ]
F a m i l i a l B C : 3 5 9
S p o r a d i c B C : 5 9 5 1 7
N R
D i a g n o s e d :
1 9 5 3 – 1 9 9 5 E n d
F U : 1 9 9 7
S t a g e , a g e , p e r i o d o f B C
d i a g n o s i s , F U
t i m e ( a f t e r
2 a n d 3 y r s o f d i a g n o s i s )
B R C A 1 , B R C A 2
5 - y e a r r e l a t i v e s u r v i v a l w a s
m e a s u r e d f o r e x c e s s m o r t a l i t y
d u e t o B C
3 2
K i t c h e n 2 0 0 1 [ 3 5 ]
9 5 2 0
1 2
T u b u l a r B C t y p e v s . o t h e r
t y p e , b y n o d a l s t a t u s a n d
c h e m o t h e r a p y
O v e r a l l s u r v i v a l w a s m e a s u r e d .
T u b u l a r B C t y p e h a d b e t t e r
p r o g n o s i s t h a n o t h e r t y p e .
T h i s t y p e w a s m o r e l i k e l y t o
h a v e l o w G & E R +
3 3
K a t o 2 0 0 2 [ 5 0 ] a
4 2 2
1 0
P 5 3 , M I , n e c r o s i s , T , N
,
L V I
M I , T , N
U V : A I
O v e r a l l s u r v i v a l w a s m e a s u r e d
I n M V P 5 3 & M I w e r e
i n d e p e n d e n t p r o g n o s t i c f a c t o r s
f o r N - p a t i e n t s o n l y . P 5 3 w a s
r e l a t e d t o M I , A I , n e c r o s i s , G
, T ,
N , E R /
P R
3 4
K a t o 2 0 0 2 [ 5 4 ] a
3 9 8
1 0
B V I , T , N
, G ,
c h e m o t h e r a p y
B V I , T , N
, G ,
c h e m o t h e r a p y
U V : n e c r o s i s
O v e r a l l s u r v i v a l w a s m e a s u r e d
3 5
C o s t a 2 0 0 2 [ 6 7 ]
6 7 0
1 1 . 4
N , T ,
a g e , E R / P R
N , T ,
a g e
M S , E R / P R
B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d . A f t e r 5 y r s o f
F U E R a n d P R w e r e n o t
i n d e p e n d e n t p r o g n o s t i c
f a c t o r s
3 6
M e n a r d 2 0 0 2 [ 1 7 ]
1 9 2 8
D i a g n o s e d i n
1 9 6 8 – 6 9 a n d
1 9 7 8 – 7 9
H e r 2 , N , T ,
M S ,
l y m p h o i d i n l t r a t i o n ,
P R -
G , T ,
N , l y m
p h o i d
i n l t r a t i o n
O v e r a l l s u r v i v a l w a s m e a s u r e d .
H E R - 2 w a s r e l a t e d t o l a r g e
t u m o u r s , h i g h e r G
, l y m p h o i d
i n l t r a t i o n , h i g h e r m i t o t i c
i n d e x , P R -
3 7
V a n d e V i j v e r 2 0 0 2 [ 7 4 ] 2 9 5 a g e < 5 3 , s t a g e I - I I 6 . 7
G e n e p r o l e ( G o o d v s .
b a d p r o g n o s i s ) f o r a l l
p a t i e n t s , N + , N –
G e n e p r o l e , T , N ,
c h e m o t h e r a p y
V I , G
, a g e , h o r m o n a l
t h e r a p y
O v e r a l l s u r v i v a l w a s m e a s u r e d
3 8
V a n ’ t V e e r 2 0 0 2 [ 7 2 ]
1 1 7 a g e < 5 5
N R
B e t t e r c l a s s i c a t i o n o f p a t i e n t s
w i t h h i g h r i s k o f m e t a s t a s i s
a n d i n n e e d o f c h e m o t h e r a p y
Breast Cancer Res Treat (2008) 107:309–330 319
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 12/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
3 9
H a t t e v i l l e 2 0 0 2 [ 2 1 ]
3 1 8 0
1 5 . 8
O S < 5 y e a r : N , G
,
r e c u r r e n c e o r m e t a s t a s i s
O S ‡ 5 y r : G a n d
r e c u r r e n c e
o r m e t a s t a s i s
A g e , T
I f p a t i e n t r e m a i n s w i t h o u t
r e c u r r e n c e o r m e t a s t a s i s ,
e f f e c t o f p r o g n o s t i c f a c t o r s
d e c r e a s e s o v e r t i m e . W i t h
m e t a s t a s e s , t h i s e f f e c t
i n c r e a s e s
4 0
S o t i r i o u 2 0 0 3 [ 7 3 ]
9 9
6 . 1
G e n e p r o l e ( l u m i n a l 1 – 3
v s . b a s a l 1 – 2 & H e r 2
t y p e )
L u m i n a l - l i k e 1 – 3 w a s
p r e d o m i n a n t l y E R + . B a s a l -
l i k e 1 – 2 a n d H e r 2 w a s
p r e d o m i n a n t l y E R -
4 1
D i g n a m 2 0 0 3 [ 8 3 ]
3 3 8 5 N – ,
E R +
1 3 . 8
B M I < 1 8 . 5 a n d B M I ‡ 3 0
h i g h e r t o t a l m o r t a l i t y a n d
o t h e r d e a t h s .
B M I o n
d e a t h s a f t e r B C
e v e n t s .
T o t a l m o r t a l i t y , d e a t h a f t e r B C
e v e n t s a n d o t h e r d e a t h s a s
w e l l a s r e c u r r e n c e r a t e a n d
o c c u r r e n c e o f a s e c o n d c a n c e r
w a s w e r e m e a s u r e d . M V w a s
a d j u s t e d f o r t r e a t m e n t , a g e ,
M S , r a c e , T , E R a n d P R
.
R e f e r e n c e g r o u p w a s B M I
1 8 . 5 – 2 4 . 9 .
4 2
O l i v o t t o 2 0 0 3 [ 5 7 ]
6 2 0 s t a g e I I I B - M
1
> 2 0
S u p r a c l a v i c u l a r B C
,
S t a g e I I I B a n d M 1
O v e r a l l a n d b r e a s t c a n c e r
s p e c i c s u r v i v a l w e r e
m e a s u r e d . P a t i e n t s w i t h
s u p r a c l a v i c u l a r m e t a s t a s e s
h a d s i g n i c a n t l y b e t t e r
s u r v i v a l t h a n p a t i e n t s w i t h
M 1 . S u r v i v a l o f t h e s e p a t i e n t s
r e s e m
b l e s t h a t o f B C s t a g e
I I B . ( F U f o r l i v i n g p a t i e n t s 2 0
y r s , f o r a l l p a t i e n t s 4 . 5 y r s )
4 3
W e i s s 2 0 0 3 [ 3 2 ]
9 0 5 N +
C h e m o t h e r a p y +
2 2 . 6
N + ( N 1 – 3 v s . N 4 – 9 v s .
N > 1 0 ) , a l s o b y
t r e a t m e n t a n d
f o l l o w - u p t i m e
N , T ,
M S
M V : N X T , M S X T ,
a d d i t i o n a l
v i n c r i s t i n e a n d
p r e d n i s o n
O v e r a l l s u r v i v a l w a s m e a s u r e d .
N w a s r e l a t e d t o T . M S w a s
r e l a t e d t o r e c e p t o r s t a t u s
4 4
T a y l o r 2 0 0 3 [ 1 6 ]
5 4 , 2 2 8
A t 1 0 y r s 6 5 %
p a t i e n t s w e r e
a l i v e
P e r i o d o f d i a g n o s i s , s t a g e
b y a g e , F U t i m e b y s t a g e
R e l a t i v e s u r v i v a l w a s m e a s u r e d
f o r e x c e s s m o r t a l i t y d u e t o B C
T h e l o n g e r t h e s u r v i v a l t h e
b e t t e r t h e p r o g n o s i s .
I m p r o v e m e n t i n r e l a t i v e s u r v i v a l
f o r a l l p a t i e n t s a n d a l l s t a g e s
s i n c e 1 9 7 2
320 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 13/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
4 5
D a l e s 2 0 0 4 [ 5 6 ]
9 0 5 a g e d 2 5 – 8 1
1 1 . 7
I n N - : C D 1 0 5 + v e s s e l s . I n
a l l p t s : C D 3 1 , T i e - 2 / T e k
I n a l l p t s : G , C
D 1 0 5
v e s s e l s , E R
I n N – : G , C
D 1 0 5 v e s s e l s ,
P R
I n a l l p t s : T , H t y p ,
C D 3 1 , P R
, a g e . I n
N – : T ,
C D 3 1
v e s s e l s , E R
, a g e
O v e r a l l s u r v i v a l w a s m e a s u r e d .
M V : T i e - 2 / T e k s h o w e d
s i g n i c a n t r o l e f o r p r e d i c t i n g
O S i n a l l p a t i e n t s a n d N -
p a t i e n t s
4 6
B r e n n e r a n d H a k u l i n e n
2 0 0 4 [ 1 5 ]
1 8 , 5 7 8 a g e < 5 0
N R
. D i a g n o s e d :
1 9 5 3 – 1 9 9 9 .
P e r i o d o f d i a g n o s i s ,
s t a g e , s t a g e * p e r i o d , t i m e
a f t e r d i a g n o s i s
I m p r o v e m e n t o f p r o g n o s i s f o r
B C p a t i e n t s y o u n g e r t h a n 5 0
o v e r t h e p a s t d e c a d e s .
R e l a t i v e s u r v i v a l r e m a i n s
l o w e r e d e v e n 4 0 y r s a f t e r
d i a g n o s i s
4 7
R o b s o n 2 0 0 4 [ 7 6 ]
5 8 4 A s h k e n a z i J e w i s h
1 1 6
B R C A 1 , T , N
, E R , a g e ,
c h e m o t h e r a p y
B R C A 1 , T , N , A g e
T a m o k s i f e n ,
B R C A 2
B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d . N o e f f e c t o f
B R C A o n n o n - B C d e a t h .
B R C A 1 o n l y p r e d i c t e d B C
d e a t h
i n p a t i e n t s w i t h o u t
c h e m o t h e r a p y
4 8
C h i a 2 0 0 4 [ 3 3 ]
1 1 8 7 L V I - , N - ,
A d j u v a n t s y s t e m i c
t h e r a p y -
1 0 . 4
T , G
T X G
O v e r a l l a n d b r e a s t c a n c e r
s p e c i c s u r v i v a l w e r e
m e a s u r e d . P a t i e n t s w i t h
h i g h e r g r a d e a n d s i z e h a v e
g r e a t e r c h a n c e t o d i e f r o m
o t h e r & t h o s e w i t h l o w r i s k
d i s e a s e g r e a t e r c h a n c e o f
d e a t h
f r o m B C
4 9
Y o s h i m o t o 2 0 0 4 [ 1 8 ]
1 5 , 4 1 6
N R
. D i a g n o s e d
1 9 4 6 – 2 0 0 1 .
P e r i o d o f d i a g n o s i s
O v e r t h e d e c a d e s , t h e r e w e r e
l e s s e x t e n s i v e s u r g e r y a n d
l y m p h n o d e e x a m i n a t i o n , l e s s
r a d i o t h e r a p y , m o r e c h e m o -
a n d h o r m o n a l t h e r a p y
5 0
H o u t e r m a n 2 0 0 4 [ 1 1 6 ] 5 2 7 a g e ‡ 4 0
4 . 7
C o m o r b i d i t y , N
, T h e r a p y ,
a g e ‡ 7 0 , c o m o r b i d i t y * N
I n a g e < 7 0 : c o m o r b i d i t y , N
I n a g e ‡ 7 0 : c o m o r b i d i t y ,
a g e
I n a g e < 7 0 : t h e r a p y
I n p t s a g e ‡ 7 0 : N
,
t h e r a p y
R e l a t i v e s u r v i v a l w a s m e a s u r e d
f o r e x c e s s m o r t a l i t y d u e t o B C
O l d e r p a t i e n t s w i t h c o m o r b i d i t y
w e r e n o t t r e a t e d d i f f e r e n t l y b u t
h a d a w o r s e p r o g n o s i s
5 1
S c h o p p m a n n 2 0 0 4 [ 5 3 ] 3 7 4
2 2 . 4
L V
I , G , N , T h e r a p y
L V I , G
, N
L M V D ( L y m p h a t i c
M i c r o v e s s e l
D e n s i t y ) , T , H t y p ,
E R , a g e ,
M S
O v e r a l l s u r v i v a l w a s m e a s u r e d .
L V I i s r e l a t e d t o y o u n g
p r e m e n o p a u s a l B C
, l o w e r G
,
N +
Breast Cancer Res Treat (2008) 107:309–330 321
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 14/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
5 2
W a r w i c k 2 0 0 4 [ 3 1 ]
2 2 9 9
> 1 0
G , N , T ,
M e t a s t a s e s
G , N , T ,
M e t a s t a s e s
B r e a s t c a n c e r s p e c i c s u r v i v a l
w a s m e a s u r e d . A l l s t u d i e d
f a c t o r s p r e d i c t e d l o n g - t e r m
s u r v i v a l , b u t t h e i r v a l u e
d e c r e a s e d o v e r t i m e
5 3
B e r c l a z 2 0 0 4 [ 8 2 ]
6 7 9 2
1 4
B M
I 2 5 – 2 9 , B M I ‡ 3 0 l o w e r
o v e r a l l s u r v i v a l
B M I ‡ 3 0
B M I 2 5 – 2 9
O v e r a l l s u r v i v a l a n d a l s o d i s e a s e
f r e e s u r v i v a l w e r e m e a s u r e d .
R e f e r e n c e g r o u p w a s B M I £
2 4 . 9 . M
V a d j u s t e d f o r E R
, T ,
N , M
S , t r e a t m e n t ,
c h e m o t h e r a p y , h o r m o n a l - i n
c o m b i n a t i o n w i t h
c h e m o t h e r a p y
5 4
D i g n a m 2 0 0 5 [ 8 4 ]
4 0 7 7 N - ,
E R -
N R
B M I ‡ 3 5 a n d A A h a d
h i g h e r o v e r a l l m o r t a l i t y
a n d n o n - B C d e a t h
B M I a n d r a c e o n
d e a t h a f t e r B C
e v e n t s
T o t a l m o r t a l i t y , d e a t h a f t e r B C
e v e n t s a n d o t h e r d e a t h s a s
w e l l a s r e c u r r e n c e r a t e a n d
o c c u r r e n c e o f a s e c o n d c a n c e r
w e r e m e a s u r e d . M V w a s
a d j u s t e d f o r t r e a t m e n t , a g e ,
M S , r a c e , T , E R a n d P R
R e f e r e n c e g r o u p w a s B M I £ 2 4 . 9
5 5
H o l m e s 2 0 0 5 [ 8 7 ]
2 9 8 7
9 6 m o n t h s
P h y s i c a l a c t i v i t y
a f t e r
d i a g n o s i s ( M E T ‡ 9 ) o n
B C a n d t o t a l m o r t a l i t y
B r e a s t c a n c e r a n d t o t a l m o r t a l i t y
w e r e m e a s u r e d . M V c o r r e c t e d
f o r a g e , i n t e r v a l b e t w e e n
d i a g n o s i s a n d p h y s i c a l
a c t i v i t y a s s e s s m e n t , s m o k i n g ,
B M I
, M S , h o r m o n e t h e r a p y
u s e , a g e a t r s t b i r t h , p a r i t y ,
e n e r g y i n t a k e , s t a g e a n d
t r e a t m e n t . M E T : m e t a b o l i c
e q u i v a l e n t t a s k h o u r s p e r
w e e k . P a t i e n t s
w i t h B M I ‡ 2 5
a n d m o r e p h y s i c a l a c t i v i t y
b e f o r e d i a g n o s i s t h e r e w a s a
s i g n i c a n t t r e n d f o r l e s s
b r e a s t c a n c e r d e a t h
5 6
R o b s a h m a n d T r e t l i
2 0 0 5 [ 2 7 ]
5 0 4 2
N R
. D i a g n o s e d :
1 9 6 4 – 9 2 . E n d
F U : 1 9 9 2
N R
L o c a t i o n o f h o m e , a g e a t
r s t c h i l d , p h y s i c a l
a c t i v i t y a t w o r k
M V c o r r e c t e d f o r :
a g e , p e r i o d o f
d i a g n o s i s , b i r t h
c o h o r t ,
e d u c a t i o n a l l e v e l B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d . I n c i d e n c e o f
B C i n c r e a s e s w i t h h i g h e r
e d u c a t i o n a l l e v e l , a n d c a s e
f a t a l i t y d e c r e a s e s b y
i n c r e a s i n g e d u c a t i o n l e v e l
322 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 15/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
5 7
V u - N i s h i n o 2 0 0 5 [ 3 8 ]
1 4 9 0 r e c e i v e d b r e a s t -
c o n s e r v i n g t r e a t m e n t
1 3 . 9
M e d u l l a r y B C v s .
o t h e r B C t y p e
O v e r a l l s u r v i v a l w a s m e a s u r e d .
M e d u l l a r y B C t y p e h a d b e t t e r
p r o g n o s i s t h a n o t h e r t y p e .
T h i s t y p e w a s m o r e l i k e l y t o
h a v e E R + , P R + & l e s s
B R C A 1 / 2 m u t a t i o n .
M e d u l l a r y t y p e w a s o n l y a
p r o g n o s t i c f a c t o r f o r t h e r s t
5 y r s
5 8
G a l p e r 2 0 0 5 [ 6 3 ]
2 1 0 2 s t a g e I - I I , 3 1 4 w i t h
l o c a l r e c u r r e n c e ( L R )
1 3 . 1
N R
N o L R t r e a t m e n t , I n v a s i v e
L R , t i m
e ( y r s ) t o l o c a l
r e c u r r e n c e , a g e a t i n i t i a l
B C d i a g n o s i s
T , d e t e c t i o n m e t h o d ,
n u m b e r o f n o d e s
s a m p l e d , E R / P R
,
h i s t o l o g i c a l t y p e ,
G , L V
I , m a r g i n s
M e a s u r e o f s u r v i v a l : d i s t a n t
f a i l u r e , s e c o n d m a l i g n a n c y , o r
d e a t h
P a t i e n t s w i t h a l o n g e r t i m e t o
r e c u r r e n c e h a v e p r o l o n g e d
s u r v i v a l
5 9
V o o g d 2 0 0 5 [ 6 2 ]
2 6 6 B C w i t h L R
1 1 . 2 a f t e r L R f o r
l i v i n g p t s
N R
L o c a t i o n o f L R , s i z e o f L R ,
s k i n i n v o l v e m e n t o f L R
,
N + f o r p r i m a r y t u m o u r
O v e r a l l s u r v i v a l w a s m e a s u r e d .
E a r l y
d e t e c t i o n o f l o c a l
r e c u r r e n c e m a y i m p r o v e t h e
t r e a t m e n t o u t c o m e
6 0
L o u w m a n 2 0 0 5 [ 1 3 ]
8 9 6 6
D i a g n o s e d 1 9 9 5 –
2 0 0 1 . E n d F U :
2 0 0 4
2 o r m o r e c o m o r b i d i t i e s ,
d i a b e t e s m e l l i t u s a n d
p r e v i o u s c a n c e r
P r e v i o u s c a n c e r , C
V D
, D M
,
c e r e b r o v a s c u l a r d i s e a s e ,
d e m e n t i a , 2 o r m o r e
c o m o r b i d i t i e s , s t a g e ,
t r e a t m e n t ( R T , S T ,
a g e )
O v e r a l l a s w e l l a s r e l a t i v e
s u r v i v a l w a s m e a s u r e d f o r
e x c e s s m o r t a l i t y d u e t o B C
P r i m a r y t r e a t m e n t o f B C
p a t i e n t s w i t h s e r i o u s
c o m o r b i d i t y w a s l e s s
e x t e n s i v e t h a n t r e a t m e n t o f
t h o s e
w i t h o u t c o m o r b i d i t y
6 1
T a m m e m a g i 2 0 0 5 [ 1 4 ] 9 0 6
1 0
N u m b e r o f s e v e r e
c o m o r b i d i t i e s , r a c e , t y p e
o f c o m o r b i d i t y
A l l p a t i e n t s : 3 o r m o r e
c o m o r b i d i t i e s a d j u s t e d
f o r s t a g e , a g e , E R ,
s u r g e r y , c h e m o t h e r a p y ,
r a d i o t h e r a p y
O v e r a l l s u r v i v a l w a s m e a s u r e d .
A A h a d m o r e d i a b e t e s a n d
h y p e r t e n s i o n . A f t e r
a d j u s t m e n t f o r t h e s e 2
c o m o r b i d i t i e s d i s p a r i t y
d i s a p p e a r e d
6 2
M e u n i e r - C a r p e n t i e r
2 0 0 5 [ 5 5 ]
9 0 9 / 9 1 8 a g e : 2 5 – 8 1
1 1 . 3
T i e 2
–
U V : V E G F R - 2 ,
V E G F R - 2
O v e r a l l s u r v i v a l w a s m e a s u r e d .
V E G F R - 1 a n d T i e 2 w e r e
r e p o r t e d a s i n d e p e n d e n t
p r o g n o s t i c f a c t o r s c o r r e c t e d
f o r T , G , H
t y p , i n a l l
p a t i e n t s a n d N -
Breast Cancer Res Treat (2008) 107:309–330 323
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 16/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
6 3
T a i 2 0 0 5 [ 4 0 ]
6 1 8 4 I n a m m a t o r y B C
N R
. D i a g n o s e d
1 9 7 3 – 1 9 9 5 .
E n d F U : 2 0 0 0
P e r i o d o f d i a g n o s i s
B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d . P r o g n o s i s h a s
i m p r o v e d o v e r t h e d e c a d e s
d u e t o m o r e a g g r e s s i v e
t h e r a p y
6 4
L o u w m a n 2 0 0 5 [ 7 1 ]
4 9 2 T 1 – 2 N 0
> 1 0 y r s
M A I
O S : a g e , T
B C S : M A I
O S : H T y p , t h e r a p y ,
p e r i o d o f
d i a g n o s i s . B C S :
t h e r a p y , p e r i o d o f
d i a g n o s i s , a g e , T ,
H t y p
O v e r a l l ( O S ) a s w e l l a s r e l a t i v e
s u r v i v a l ( B C S ) w a s m e a s u r e d
f o r e x c e s s m o r t a l i t y d u e t o B C
H i g h e r M A I w a s a s i g n i c a n t
p r o g n o s t i c f a c t o r f o r N – a n d N + ,
b u t o n l y d u r i n g t h e r s t 1 0 y r s
o f F U
6 5
A r r i g a d a 2 0 0 6 [ 8 ]
2 4 1 0 T £ 7 c m N 1 – 2
1 9
T , s k i n x a t i o n , m u s c l e
x a t i o n , G
, N , a g e
T o t a l F U : T , N , G
, a g e < 3 5 ,
a g e ‡ 5 5
F U 0 – 5 y r s : T , N
, G , a g e
‡ 5 5
F U 5 – 1 0 y r s : N , G , a g e
< 3 5 , a g e ‡
5 5
F U 1 0 – 1 5 y r s : N
> 1 0 , a g e
> 5 5 . F U 1 5 – 2 0 y r s : a g e ‡ 6 5
O v e r a l l s u r v i v a l w a s m e a s u r e d .
L o n g - t e r m e f f e c t o f
p r o g n o s t i c f a c t o r s v a n i s h i n g
6 6
N e w m a n 2 0 0 6 [ 2 9 ]
9 0 , 1 2 4 . W h i t e
A m e r i c a n : 7 6 , 1 1 1 .
A A : 1 4 , 0 1 3
A g e , s t a g e , S E S
M e t a - a n a l y s i s . A f r i c a n
A m e r i c a n i s a n i n d e p e n d e n t
p r e d i c t o r o f p o o r o u t c o m e f o r
o v e r a l l s u r v i v a l a n d b r e a s t
c a n c e r s p e c i c m o r t a l i t y
6 7
M e n v i e l l e 2 0 0 6 [ 2 4 ]
4 0 7 , 4 3 5
w o m e n
f o l l o w e d f o r B C
d e a t h ( N : 1 4 0 8 )
W o m e n w h o
d i e d o f B C i n
1 9 6 8 – 9 6
L e v e l o f e d u c a t i o n b y
p e r i o d o f d i a g n o s i s
B r e a s t c a n c e r d e a t h a m o n g
w o m e n w i t h t h e h i g h e s t
e d u c a t i o n c o m p a r e d t o
w o m e n w i t h t h e l o w e s t
e d u c a t i o n i n 1 9 6 8 – 7 4 w a s
0 . 4 3 ; a n d i n 1 9 9 0 – 9 6 : 1 . 1 7
( N S )
6 8
B o u c h a r d y 2 0 0 6 [ 2 5 ]
3 9 2 0 a g e < 7 0
N R
. D i a g n o s e d
i n 1 9 8 0 – 2 0 0 0
S E S
S E S c o r r e c t e d f o r a g e ,
p e r i o d o f d i a g n o s i s ,
m a r i t a l s t a t u s , c o u n t r y
o f
b i r t h , H t y p , E R
,
d e t e c t i o n m e t h o d , s t a g e ,
s e c t o r o f c a r e , t h e r a p y
O v e r a l l s u r v i v a l w a s m e a s u r e d .
L o w e s t S E S h a d l e s s
f r e q u e n t l y s c r e e n - d e t e c t e d
c a n c e r s , l e s s s t a g e I , l e s s
l o b u l a r B C
, l e s s B C T , l e s s
l y m p h n o d e d i s s e c t i o n
324 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 17/22
T a
b l e 1 c o n t i n u e d
N o . A u t h o r , y e a r
N o . o f p a t i e n t s
M e a n / m e d i a n
f o l l o w - u p
( y r s ) U n i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
M u l t i v a r i a t e
( U V ) a n a l y s i s s i g n i c a n t
N o t s i g n i c a n t
R e m a r k s
6 9
S i e g e l m a n n - D a n i e l i
2 0 0 6 [ 1 1 7 ]
9 9 2 , a g e
‡ 7 0
6 . 9
B e i n g i n w h e e l c h a i r , r e n a l
i n s u f c i e n c y , d e m e n t i a ,
C H F , c a r d i a c a r r h y t h m i a ,
D M
, I H D
, o s t e o p o r o s i s ,
P V D
, c e r e b r o v a s c u l a r
d i s e a s e , C O P D
,
P a r k i n s o n ’ s d i s e a s e ,
v a l v u l a r h e a r t d i s e a s e
I n s t a g e 1 A - 2 A : a g e , C H F ,
D M
, P V D
, s t a g e , c a r d i a c
a r r h y t h m i a , P a r k i n s o n ’ s
d i s e a s e , r e n a l
i n s u f c i e n c y
I n s t a g e 2 B - 4 : G , s t a g e ,
N ,
w h e e l c h a i r - b o u n d , r e n a l
i n s u f c i e n c y , C O P D
, a g e ,
D M
S y s t e m i c t h e r a p y
O v e r a l l s u r v i v a l w a s m e a s u r e d .
C H F : C a r d i a c H e a r t F a i l u r e .
D M : D i a b e t e s M e l l i t u s . I H D :
I s c h e m i c H e a r t D i s e a s e . P V D :
P e r i p h e r a l H e a r t D i s e a s e .
C O P D : C h r o n i c O b s t r u c t i v e
P u l m o n a r y D i s e a s e . R o l e o f
c o m o r b i d i t y v a r i e s b y a g e
7 0
P r i t c h a r d 2 0 0 6 [ 6 8 ]
6 3 9 p r e m e n o p a u s a l N + 1 0
H e r 2 a m p l i c a t i o n
H e r 2 c o r r e c t e d f o r a g e , N
,
E R , t y p e
o f s u r g e r y
O v e r a l l s u r v i v a l w a s m e a s u r e d .
T h o s e w i t h a m p l i e d H e r 2
h a v e i m p r o v e d s u r v i v a l w i t h
C E F
7 1
L e e 2 0 0 6 [ 5 2 ]
( A ) A d j u v a n t t h e r a p y – :
9 9 0 . ( B ) A d j u v a n t
t r e a t m e n t + : 1 7 6 5
G r o u p A : 1 3
G r o u p B : 6 . 8 .
L V
I
G r o u p A : T , G , L V I , H t y p
G r o u p B : T , G , L V I ,
c h e m o t h e r a p y , h o r m o n a l
t h e r a p y
B : E R , a g e ,
H t y p
B r e a s t c a n c e r - s p e c i c s u r v i v a l
w a s m e a s u r e d
F o r p a t i e n t s w i t h o u t a d j u v a n t
t r e a t m e n t , r o l e o f G i n s u r v i v a l
w a s h i g h e r i n t h e r s t 5 y r s .
R o l e o f H t y p w a s n o t s i g n i c a n t
f o r t h e r s t 5 y r s o f F U
a
i n d i c a t e s t h e o v e r l a p p i n g p a t i e n t s
u s e d b y t h e s a m e a u t h o r t o a n s w e r a n o t h e r r e s e a r c h q u e s t i o n ; y r s : y e a r s ; U V : U n i v a r i a t e a n a l y s i s . M V : M u l t i v a r i a t e a n a l y s i s . M S : M e n o p a u s a l S t a t u s ; T :
T u m o u r s i z e ; N : N o d a l i n v o l v e m e n t ; H t y p : H i s t o l o g i c a l t y p e ; M I : M i t o t i c I n d e x ; G : G r a d e ; P R : P r o g e s t e r o n e R e c e p t o r s t a t u s ; E R : O e s t r o g e n R e c e p t o r s t a t u s ; P C N A : p r o l i f e r a t i n g c e l l n u c l e a r
a n t i g e n ; m o s : m o n t h s ; N R : N o t R e p o r t e d ; A A : A f r i c a n A m e r i c a n ; a g e : i s i n y e a r a n d i n d i c a t e a g e a t p r i m a r y b r e a s t c a n c e r u n l e s s o t h e r w i s e s t a t e ; N P I : N o t t i n g h a m
P r o g n o s t i c I n d e x ; L V I :
L y m p h o v a s c u l a r I n v a s i o n ; ( P r o g n o s t i c f a c t o r ) * ( P r o g n o s t i c f a c t o r ) : i n t e r a c t i o n b e t w e e n t w o f a c t o r s ; B M I : B o d y M a s s I n d e x ; A M C : A v e r a g e M i c r o v e s s e l C o u n t ; M A I : M i t o t i c A c t i v i t y I n d e x ;
A I : A p o p t o s i s I n d e x ; F U : F o l l o w - u p ; S E S : S o c i o e c o n o m i c S t a t u s ; B V I : B l o o d v e s s e l I n v a s i o n ; L M V D : L y m p h a t i c M i c r o v e s s e l D e n s i t y ; L R : l o c a l r e c u r r e n c e ; C V D : C a r d i o v a s c u l a r D i s e a s e ;
D M : D i a b e t e s M e l l i t u s ; R T : r a d i o t h e r a p y ; S T : S y s t e m i c t h e r a p y ; V E G F R : V a s c u l a r E n d o t h e l i a l G r o w t h F a c t o r R e c e p t o r ; O S : O v e r a l l s u r v i v a l ; B C S : B r e a s t C a n c e r S p e c i c S u r v i v a l ; N S : n o t
s i g n i c a n t ; C H F : C a r d i a c H e a r t F a i l u r e ; I H D : I s c h e m i c H e a r t D i s e a s e . P V D : P e r i p h e r a l H e a r t D i s e a s e . C O P D : C h r o n i c O b s t r u c t i v e P u l m o n a r y . C E F : c y c l o p h o s p h a m i d e , e p i r u b i c i n a n d
u o r o u r a c i l
Breast Cancer Res Treat (2008) 107:309–330 325
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 18/22
T a
b l e 2
S e l e c t e d p r o g n o s t i c f a c t o r s f o r l o n g - t e r m o v e r a l l m o r t a l i t y o f b r e a s t c a n c e r ( B C ) p a t i e n t s
P a t i e n t g r o u p s b a s e d
H a z a r d r a t i o ( H R ) f o r
o v e r a l l f o l l o w - u p o r
s u r v i v a l p r o b a b i l i t y ( S )
1 0 y e a r s a f t e r d i a g n o s i s
M o r p h o l o g y b a s e d
H a z a r d r a t i o ( H R ) f o r
o v e r a l l f o l l o w - u p o r
s u r v i v a l p r o b a b i l i t y
( S ) 1 0 y e a r s a f t e r
d i a g n o s i s
M o l e c u l a r b a s e d
H a z a r d r a t i o ( H R ) f o r
o v e r a l l f o l l o w - u p o r
s u r v i v a l p r o b a b i l i t y
( S ) 1 0 y e a r s a f t e r
d i a g n o s i s
A g e a t d i a g n o s i s [ 8 ]
H R :
L y m p h n o d e s t a t u s [ 3 1 ]
H R :
H E R 2 [ 6 9 ]
H R :
< 3 5 v s . 3 5 – 4 4
1 . 4 ( P : 0 . 0 7 )
N ‡ 1 v s . N 0
2 . 4 ( 1 . 9 – 2 . 9 )
> 5 0 0 v s . £ 5 0 0
1 . 8 2 ( 1 . 1 – 2 . 9 )
4 5 – 5 4 v s . 3 5 – 4 4
1 . 1 ( n s )
M e t a s t a s e s v s . N 0
2 2 . 7 3 ( 1 6 . 1 – 3 2 . 2 )
O n l y i n n o d e - p o s i t i v e
5 5 – 6 4 v s . 3 5 – 4 4
2 . 0 ( P : 0 . 0 0 0 )
6 5 – 7 5 v s . 3 5 – 4 4
2 . 5 ( P : 0 . 0 0 0 )
P e r i o d o f d i a g n o s i s [ 1 6 ]
R e l a t i v e s u r v i v a l b :
T u m o u r s i z e ( m m ) [ 3 1 ]
H R :
C e l l p r o l i f e r a t i o n i n d e x
H R :
1 9 7 2 – 1 9 7 6
5 9 %
T 1 0 – 1 4 v s . T 1 – 9
1 . 2 ( 0 . 8 – 1 . 9 )
( M A I )
1 9 7 7 – 1 9 8 6
6 4 %
T 1 5 – 1 9 v s . T 1 – 9
1 . 7 ( 1 . 1 – 2 . 6 )
> 1 0 v s . £ 1 0 [ 1 0 ]
1 . 0 2 ( 1 . 0 0 – 1 . 0 3 )
1 9 8 7 – 1 9 9 1
7 0 %
T 2 0 – 2 9 v s . T 1 – 9
2 . 5 ( 1 . 6 – 3 . 9 )
O n l y i n n o d e - p o s i t i v e
p a t i e n t s
T 3 0 – 4 9 v s . T 1 – 9
3 . 8 ( 2 . 4 – 6 . 0 )
T ‡ 5 0 v s . T 1 – 9
4 . 6 ( 2 . 9 – 7 . 6 )
T i m e a f t e r d i a g n o s i s [ 1 6 ]
R e l a t i v e s u r v i v a l :
T u m o u r g r a d e [ 4 4 ]
H R :
G e n e e x p r e s s i o n p r o l e [ 7 4 ]
S :
0 v s . 5 y r s a f t e r d i a g n o s i s
I I v s . I
2 . 5 ( 1 . 0 – 6 . 1 )
5 5 % v s . 9 5 %
R e g i o n a l B C
7 9 % v s . 8 4 %
I I I v s . I
5 . 7 ( 2 . 6 – 1 2 . 4 )
P o o r v s . g o o d s i g n a t u r e f
L o c a l l y a d v a n c e d B C
5 3 % v s . 6 8 %
S o c i o e c o n o m i c s t a t u s [ 2 6 ]
H R :
T u m o u r t y p e [ 3 4 ]
S :
E R / P R s t a t u s [ 3 0 ]
H R :
I n t e r m e d i a t e v s . a f u e n t
1 . 2 ( 1 . 0 – 1 . 4 )
P o o r v s . e x c e l l e n t d , e
< 5 0 % v s . > 8 0 %
P o s i t i v e v s . n e g a t i v e
0 . 3 8 ( 0 . 0 2 – 1 . 0 6 )
D e p r i v e d v s . a f u e n t
1 . 2 ( 0 . 9 9 – 1 . 5 3 )
L i f e s t y l e
H R :
B o d y M a s s I n d e x
< 2 1 v s . 2 9 + k g / m
2
1 . 4 ( 0 . 9 7 – 2 . 0 0 ) [ 8 5 ] c
P h y s i c a l a c t i v i t y
< 3 v s . 2 3 . 9 M E T - h / w k a
0 . 5 6 ( 0 . 4 – 0 . 8 ) [ 8 7 ]
H R : H a z a r d r a t i o c a l c u l a t e d w i t h i n m u l t i v a r i a t e a n a l y s i s o f b r e a s t c a n c e r p a t i e n t s f o l l o w e d f o r a m e d i a n / m e a n o f 1 0 y e a r s o r l o n g e r a
M e t a b o l i c e q u i v a l e n t t a s k h o u r s p e r w e e k ; b
E s t i m a t e s
t a k e n f r o m g r a p h ; c
H i g h e r a l c o h o l i n t a k e n o s i g n i c a n t e f f e c t o n m o r t a l i t y . S i g n i c a n t t r e n d o f h i g h e r m o r t a l i t y f o r l o w e s t c o m p a r e d t o h i g h e s t q u i n t i l e s o f b r e , l u t e i n
a n d z e a x a n t h i n , c a l c i u m
& p r o t e i n i n t a k e ; d
B e c o m e s l a r g e r a s n u m b e r s o f i n v o l v e d l y m p h n o d e s i n c r e a s e s [ 8 ] ; e
E x c e l l e n t p r o g n o s i s : t u b u l a r , i n v a s i v e c r i b r i f o r m , m
u c i n o u s , t u b u l o l o b u l a r . P o o r p r o g n o s i s : m i x e d
l o b u l a r , s o l i d l o b u l a r , d u c t a l a n d m i x e d d u c t a l l o b u l a r ; f
u n a d j u s t e d e s t i m a t e s
326 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 19/22
other prognostic factors in determining survival for long-term survivors still needs to be determined.
The role of early detection
Increased awareness among women and improvement indiagnostic procedures have enabled earlier and better
detection of BC. Trials on population screening have re-ported 21–29% reduction in BC mortality for women in-vited for screening within 14–16 years of follow-up [ 19,97]. Screening identied tumours at an early stage conse-quently, survival improved [ 98, 99]. Screening also iden-tied patients with slowly growing tumours who mightreceive unnecessarily aggressive cancer treatment. Thus,Joensuu et al. [ 100 ] examined recurrence rates among pa-tients detected by screening compared to those detectedoutside screening. After adjusting for tumour aggressive-ness (tumour size, nodal status, grade, age, treatment, PRstatus, HER-2), hence eliminating bias towards detection of
indolent cancers (length bias), the benet of screening forthe prognosis for BC patients remained evident.[ 100 ] Thissuggests that other factors explain the indolent behaviourof BC detected by screening. Hence, until this factor isestablished, detection mode should probably be consideredas a prognostic factor and thus be taken into account inpatient management.
The role of treatment
Improvement in BC treatment has undoubtedly also in-creased the long-term survival of BC patients [ 101 ], as
reected by the improved overall survival across all BCstages [ 16]. Using historical data from population-basedstudies in periods when effective treatment was not avail-able, it was estimated that without treatment only 4% of BC patients would survive 10 years or longer [ 102 ]. BCtreatment guidelines have been modied continuously inthe last 28 years, tailored to most of the prognosticatorsmentioned earlier [ 51]. Effectiveness of various treatmentmodalities has been summarized by others who concludethat radiation, chemotherapy and hormonal therapy mayreduce long-term mortality by up to 57% [ 66, 103 –105 ].Emerging new therapeutic approaches using a monoclonal
antibody directed against HER-2 have yielded improvedshort-term survival for advanced stage [ 106 ] as well asoperable BC patients [ 107 ]. Quality of treatment asindicated by loco-regional failure [ 108 ], surgeon workload[109 ] or hospital volume [ 110 ], may affect survivalalthough its role on long-term survival still needs conr-mation. In conclusion, on the one hand we have observed ashift in stage towards less aggressive cancers; on the otherhand, better and more (systemic) treatment has becomeavailable, leading to improved survival for BC patients.
Conclusion
The prognosis of BC has become relatively good, with cur-rent 10-year relative survival about 70% in most westernpopulations [ 16, 111 ], especially if up-to-date statisticalmethod such as the period analyses is used [ 111 ] (Table 1).Even better, the longer patients survive their BC the higher
their survival chance [ 16]. Our review shows conventionalprognostic factors of survival, such as tumour size, lymphnode status and grade, remain the most important determi-nants of 10-year survival for BC patients (Table 2). Moststudies agreed on the value of MAI and LVI for prediction of long-term survival. The inuence of host factors includingage, race/ethnicity or socio-economic factors and tumour-related factors such as histological type and angiogenesisdiminishes after correction for other factors. For most recentmarkers such as Her2, gene proling, p53 mutation and uPAlevel longer follow-up is needed. Recurrence, metastasesanda second cancer double the burden of disease thus increaserisk of mortality. Similarly, co-occurrence with other dis-eases is in no doubt decrease survival.
Healthier lifestyle generally increases long-term sur-vival. Modiable risk factors (such as alcohol consumptionand obesity) not only affect incidence but also tumour’clinical behaviour and thus survival.
Although a lot is known about the prognosis for BCpatients, effect of traditional prognostic factors appears toattenuate over time, leaving room for studies on the role of other and newer factors for long-term survival.
References
1. Parkin DM, Bray F, Ferlay J et al (2005) Global cancer statis-tics, 2002. CA Cancer J Clin 55:74–108
2. Sant M, Aareleid T, Berrino F et al (2003) EUROCARE-3:survival of cancer patients diagnosed 1990–94-results andcommentary. Ann Oncol 14(Suppl 5):v61–118
3. Botha JL, Bray F, Sankila R et al (2003) Breast cancer incidenceand mortality trends in 16 European countries. Eur J Cancer39:1718–1729
4. ACS: Cancer facts and gures 2005. Atlanta, 20055. Janssen-Heijnen MLG, Louwman WJ, van de Poll-Franse LV
et al (2005) Van meten naar weten. 50 jaar kankerregistratie.Integraal Kankercentrum Zuid (IKZ), Eindhoven, 104 pp
6. Kroman N, Jensen MB, Wohlfahrt J et al (2000) Factors inu-encing the effect of age on prognosis in breast cancer: popula-tion based study. BMJ 320:474–478
7. Aebi S, Gelber S, Castiglione-Gertsch M et al (2000) Is che-motherapy alone adequate for young women with oestrogen-receptor-positive breast cancer? Lancet 355:1869–1874
8. Arriagada R, Le MG, Dunant A et al (2006) Twenty-ve yearsof follow-up in patients with operable breast carcinoma: corre-lation between clinicopathologic factors and the risk of death ineach 5-year period. Cancer 106:743–750
9. Fisher ER, Anderson S, Tan-Chiu E et al (2001) Fifteen-yearprognostic discriminants for invasive breast carcinoma: National
Breast Cancer Res Treat (2008) 107:309–330 327
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 20/22
Surgical Adjuvant Breast and Bowel Project Protocol-06.Cancer 91:1679–1687
10. Pietilainen T, Lipponen P, Aaltomaa S et al (1995) Expressionof p53 protein has no independent prognostic value in breastcancer. J Pathol 177:225–232
11. Kollias J, Elston CW, Ellis IO et al (1997) Early-onset breastcancer—histopathological and prognostic considerations. Br JCancer 75:1318–1323
12. West DW, Satariano WA, Ragland DR et al (1996) Comorbidityand breast cancer survival: a comparison between black andwhite women. Ann Epidemiol 6:413–419
13. Louwman WJ, Janssen-Heijnen ML, Houterman S et al (2005)Less extensive treatment and inferior prognosis for breast cancerpatient with comorbidity: a population-based study. Eur JCancer 41:779–785
14. Tammemagi CM, Nerenz D, Neslund-Dudas C et al (2005)Comorbidity and survival disparities among black and whitepatients with breast cancer. JAMA 294:1765–1772
15. Brenner H, Hakulinen T (2004) Are patients diagnosed withbreast cancer before age 50 years ever cured? J Clin Oncol22:432–438
16. Taylor R, Davis P, Boyages J (2003) Long-term survival of women with breast cancer in New South Wales. Eur J Cancer39:215–222
17. Menard S, Balsari A, Casalini P et al (2002) HER-2-positivebreast carcinomas as a particular subset with peculiar clinicalbehaviors. Clin Cancer Res 8:520–525
18. Yoshimoto M, Tada K, Hori H et al (2004) Improvement in theprognosis of Japanese breast cancer patients from 1946 to2001–an institutional review. Jpn J Clin Oncol 34:457–462
19. Nystrom L, Andersson I, Bjurstam N et al (2002) Long-termeffects of mammography screening: updated overview of theSwedish randomised trials. Lancet 359:909–919
20. Otto SJ, Fracheboud J, Looman CW et al (2003) Initiation of population-based mammography screening in Dutch munici-palities and effect on breast-cancer mortality: a systematicreview. Lancet 361:1411–1417
21. Hatteville L, Mahe C, Hill C (2002) Prediction of the long-termsurvival in breast cancer patients according to the presentoncological status. Stat Med 21:2345–2354
22. Brenner H, Gefeller O, Hakulinen T (2004) Period analysis for’up-to-date’ cancer survival data: theory, empirical evaluation,computational realisation and applications. Eur J Cancer40:326–335
23. Hooning MJ, Aleman BM, van Rosmalen AJ et al (2006) Cause-specic mortality in long-term survivors of breast cancer: a 25-year follow-up study. Int J Radiat Oncol Biol Phys 64:1081–1091
24. Menvielle G, Leclerc A, Chastang JF et al (2006) Socialinequalities in breast cancer mortality among French women:disappearing educational disparities from 1968 to 1996. Br JCancer 94:152–155
25. Bouchardy C, Verkooijen HM, Fioretta G (2006) Social class is
an important and independent prognostic factor of breast cancermortality. Int J Cancer 119(5):1145–115126. Thomson CS, Hole DJ, Twelves CJ et al (2001) Prognostic
factors in women with breast cancer: distribution by socioeco-nomic status and effect on differences in survival. J EpidemiolCommunity Health 55:308–315
27. Robsahm TE, Tretli S (2005) Weak associations between soci-odemographic factors and breast cancer: possible effects of earlydetection. Eur J Cancer Prev 14:7–12
28. Wojcik BE, Spinks MK, Optenberg SA (1998) Breast carcinomasurvival analysis for African American and white women in anequal-access health care system. Cancer 82:1310–1218
29. Newman LA, Grifth KA, Jatoi I et al (2006) Meta-analysis of survival in African American and white American patients withbreast cancer: ethnicity compared with socioeconomic status. JClin Oncol 24:1342–1349
30. Vorgias G, Koukouras D, Paleogianni V et al (2001) Prognosticsignicance of factors affecting disease free interval and overallsurvival for Stage II breast cancer in Greece. A multivariatecohort study. Eur J Obstet Gynecol Reprod Biol 95:100–104
31. Warwick J, Tabar L, Vitak B et al (2004) Time-dependent ef-fects on survival in breast carcinoma: results of 20 years of follow-up from the Swedish Two-County Study. Cancer100:1331–1336
32. Weiss RB, Woolf SH, Demakos E et al (2003) Natural history of more than 20 years of node-positive primary breast carcinomatreated with cyclophosphamide, methotrexate, and uorouracil-based adjuvant chemotherapy: a study by the Cancer andLeukemia Group B. J Clin Oncol 21:1825–1835
33. Chia SK, Speers CH, Bryce CJ et al (2004) Ten-year outcomesin a population-based cohort of node-negative, lymphatic, andvascular invasion-negative early breast cancers without adjuvantsystemic therapies. J Clin Oncol 22:1630–1637
34. Galea MH, Blamey RW, Elston CE et al (1992) The Notting-ham Prognostic Index in primary breast cancer. Breast CancerRes Treat 22:207–219
35. Kitchen PR, Smith TH, Henderson MA et al (2001) Tubularcarcinoma of the breast: prognosis and response to adjuvantsystemic therapy. ANZ J Surg 71:27–31
36. Northridge ME, Rhoads GG, Wartenberg D et al (1997) Theimportance of histologic type on breast cancer survival. J ClinEpidemiol 50:283–290
37. Reed W, Hannisdal E, Boehler PJ et al (2000) The prognosticvalue of p53 and c-erb B-2 immunostaining is overrated forpatients with lymph node negative breast carcinoma: a multi-variate analysis of prognostic factors in 613 patients with afollow-up of 14–30 years. Cancer 88:804–813
38. Vu-Nishino H, Tavassoli FA, Ahrens WA et al (2005) Clini-copathologic features and long-term outcome of patients withmedullary breast carcinoma managed with breast-conservingtherapy (BCT). Int J Radiat Oncol Biol Phys 62:1040–1047
39. Gamel JW, Meyer JS, Feuer E et al (1996) The impact of stageand histology on the long-term clinical course of 163,808patients with breast carcinoma. Cancer 77:1459–1464
40. Tai P, Yu E, Shiels R et al (2005) Short- and long-term cause-specic survival of patients with inammatory breast cancer.BMC Cancer 5:137
41. Harris JR, Lippman ME, Morrow M et al (2004) Diseases of thebreast 3rd edn. Philadelphia, Lippincott Williams & Wilkins
42. Gilchrist KW, Kalish L, Gould VE et al (1985) Interobserverreproducibility of histopathological features in stage II breastcancer. An ECOG study. Breast Cancer Res Treat 5:3–10
43. Vincent-Salomon A, Carton M, Zafrani B et al (2001) Longterm outcome of small size invasive breast carcinomas inde-pendent from angiogenesis in a series of 685 cases. Cancer
92:249–25644. Kato T, Kameoka S, Kimura T et al (2001) Angiogenesis as apredictor of long-term survival for 377 Japanese patients withbreast cancer. Breast Cancer Res Treat 70:65–74
45. Tabar L, Duffy SW, Vitak B et al (1999) The natural history of breast carcinoma: what have we learned from screening? Cancer86:449–462
46. Kollias J, Murphy CA, Elston CW et al (1999) The prognosis of small primary breast cancers. Eur J Cancer 35:908–912
47. Pinder SE, Murray S, Ellis IO et al (1998) The importance of thehistologic grade of invasive breast carcinoma and response tochemotherapy. Cancer 83:1529–1539
328 Breast Cancer Res Treat (2008) 107:309–330
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 21/22
48. Frkovic-Grazio S, Bracko M (2002) Long term prognostic valueof Nottingham histological grade and its components in early(pT1N0M0) breast carcinoma. J Clin Pathol 55:88–92
49. D’Eredita G, Giardina C, Martellotta M et al (2001) Prognosticfactors in breast cancer: the predictive value of the NottinghamPrognostic Index in patients with a long-term follow-up thatwere treated in a single institution. Eur J Cancer 37:591–596
50. Kato T, Kameoka S, Kimura T et al (2002) p53, mitosis,apoptosis and necrosis as prognostic indicators of long-termsurvival in breast cancer. Anticancer Res 22:1105–1112
51. Goldhirsch A, Glick JH, Gelber RD et al (2005) Meetinghighlights: international expert consensus on the primary ther-apy of early breast cancer 2005. Ann Oncol 16:1569–1583
52. Lee AH, Pinder SE, Macmillan RD et al (2006) Prognosticvalue of lymphovascular invasion in women with lymph nodenegative invasive breast carcinoma. Eur J Cancer 42:357–362
53. Schoppmann SF, Bayer G, Aumayr K et al (2004) Prognosticvalue of lymphangiogenesis and lymphovascular invasion ininvasive breast cancer. Ann Surg 240:306–312
54. Kato T, Kameoka S, Kimura T et al (2002) Blood vessel inva-sion as a predictor of long-term survival for Japanese patientswith breast cancer. Breast Cancer Res Treat 73:1–12
55. Meunier-Carpentier S, Dales JP, Djemli A et al (2005) Com-parison of the prognosis indication of VEGFR-1 and VEGFR-2and Tie2 receptor expression in breast carcinoma. Int J Oncol26:977–984
56. . Dales JP, Garcia S, Carpentier S et al (2004) Long-termprognostic signicance of neoangiogenesis in breast carcinomas:comparison of Tie-2/Tek, CD105, and CD31 immunocyto-chemical expression. Hum Pathol 35:176–183
57. Olivotto IA, Chua B, Allan SJ et al (2003) Long-term survivalof patients with supraclavicular metastases at diagnosis of breastcancer. J Clin Oncol 21:851–854
58. Nomura Y, Tsutsui S, Murakami S et al (1999) Prognostic im-pact of second cancer on the survival of early breast cancerpatients. Int J Oncol 14:1103–1109
59. Raymond JS, Hogue CJ (2006) Multiple primary tumours inwomen following breast cancer, 1973–2000. Br J Cancer94:1745–1750
60. Kollias J, Ellis IO, Elston CW et al (2001) Prognostic signi-cance of synchronous and metachronous bilateral breast cancer.World J Surg 25:1117–1124
61. Wapnir IL, Anderson SJ, Mamounas EP et al (2006) Prognosisafter ipsilateral breast tumor recurrence and locoregionalrecurrences in ve National Surgical Adjuvant Breast and BowelProject node-positive adjuvant breast cancer trials. J Clin Oncol24:2028–2037
62. Voogd AC, van Oost FJ, Rutgers EJ et al (2005) Long-termprognosis of patients with local recurrence after conservativesurgery and radiotherapy for early breast cancer. Eur J Cancer41:2637–2344
63. Galper S, Blood E, Gelman R et al (2005) Prognosis after localrecurrence after conservative surgery and radiation for early-
stage breast cancer. Int J Radiat Oncol Biol Phys 61:348–35764. Habel LA, Shak S, Jacobs MK et al (2006) A population-basedstudy of tumor gene expression and risk of breast cancer deathamong lymph node-negative patients. Breast Cancer Res 8:R25
65. Obedian E, Fischer DB, Haffty BG (2000) Second malignanciesafter treatment of early-stage breast cancer: lumpectomyand radiation therapy versus mastectomy. J Clin Oncol 18:2406–2412
66. Early Breast Cancer Trialists’ Collaborative Group (2005) Ef-fects of chemotherapy and hormonal therapy for early breastcancer on recurrence and 15-year survival: an overview of therandomised trials. Lancet 365:1687–1717
67. Costa SD, Lange S, Klinga K et al (2002) Factors inuencingthe prognostic role of oestrogen and progesterone receptor levelsin breast cancer—results of the analysis of 670 patients with11 years of follow-up. Eur J Cancer 38:1329–1334
68. Pritchard KI, Shepherd LE, O’Malley FP et al (2006) HER2 andresponsiveness of breast cancer to adjuvant chemotherapy. NEngl J Med 354:2103–2111
69. Ferrero-Pous M, Hacene K, Bouchet C et al (2000) Relationshipbetween c-erbB-2 and other tumor characteristics in breastcancer prognosis. Clin Cancer Res 6:4745–4754
70. Haerslev T, Jacobsen GK, Zedeler K (1995) Proliferating cellnuclear antigen (PCNA) and c-erbB-2 oncoprotein in breastcarcinoma with correlations to histopathological parameters andprognosis. Oncol Rep 2:99–105
71. Louwman WJ, van Beek MW, Schapers RF et al (2005) Long-term survival of T1 and T2 lymph node-negative breast cancerpatients according to mitotic activity index: a population-basedstudy. Int J Cancer 118(9):2310–2314
72. van ’t Veer LJ, Dai H, van de Vijver MJ et al (2002) Geneexpression proling predicts clinical outcome of breast cancer.Nature 415:530–536
73. Sotiriou C, Neo SY, McShane LM et al (2003) Breast cancerclassication and prognosis based on gene expression prolesfrom a population-based study. Proc Natl Acad Sci USA100:10393–10398
74. van de Vijver MJ, He YD, van’t Veer LJ et al (2002) A gene-expression signature as a predictor of survival in breast cancer.N Engl J Med 347:1999–2009
75. Miki Y, Swensen J, Shattuck-Eidens D et al (1994) A strongcandidate for the breast and ovarian cancer susceptibility geneBRCA1. Science 266:66–71
76. Robson ME, Chappuis PO, Satagopan J et al (2004) A combinedanalysis of outcome following breast cancer: differences insurvival based on BRCA1/BRCA2 mutation status and admin-istration of adjuvant treatment. Breast Cancer Res 6:R8–R17
77. Eerola H, Vahteristo P, Sarantaus L et al (2001) Survival of breast cancer patients in BRCA1, BRCA2, and non-BRCA1/2breast cancer families: a relative survival analysis from Finland.Int J Cancer 93:368–372
78. Ferrero JM, Ramaioli A, Formento JL et al (2000) P53 deter-mination alongside classical prognostic factors in node-negativebreast cancer: an evaluation at more than 10-year follow-up.Ann Oncol 11:393–397
79. Haerslev T, Jacobsen GK (1995) An immunohistochemicalstudy of p53 with correlations to histopathological parameters,c-erbB-2, proliferating cell nuclear antigen, and prognosis. HumPathol 26:295–301
80. Mirza AN, Mirza NQ, Vlastos G et al (2002) Prognostic factorsin node-negative breast cancer: a review of studies with samplesize more than 200 and follow-up more than 5 years. Ann Surg235:10–26
81. Fitzgibbons PL, Page DL, Weaver D et al (2000) Prognosticfactors in breast cancer. College of American Pathologists
Consensus Statement 1999. Arch Pathol Lab Med124:966–7882. Berclaz G, Li S, Price KN et al (2004) Body mass index as a
prognostic feature in operable breast cancer: the InternationalBreast Cancer Study Group experience. Ann Oncol 15:875–884
83. Dignam JJ, Wieand K, Johnson KA et al (2003) Obesity,tamoxifen use, and outcomes in women with estrogen receptor-positive early-stage breast cancer. J Natl Cancer Inst 95:1467–1476
84. Dignam JJ, Wieand K, Johnson KA et al (2006) Effects of obesity and race on prognosis in lymph node-negative, estrogen
Breast Cancer Res Treat (2008) 107:309–330 329
123

7/30/2019 An Overview of Prognostic Factors for Long-term Survivors of Breast Cancer
http://slidepdf.com/reader/full/an-overview-of-prognostic-factors-for-long-term-survivors-of-breast-cancer 22/22
receptor-negative breast cancer. Breast Cancer Res Treat97(3):245–254
85. Holmes MD, Stampfer MJ, Colditz GA et al (1999) Dietaryfactors and the survival of women with breast carcinoma.Cancer 86:826–835
86. Byers T, Sedjo RL (2006) A weight loss trial for breast cancerrecurrence: pre-menopausal, post-menopausal, both, or neither?Cancer Causes Control 17:1–3
87. Holmes MD, Chen WY, Feskanich D et al (2005) Physicalactivity and survival after breast cancer diagnosis. JAMA293:2479–2486
88. Brown JK, Byers T, Doyle C et al (2003) Nutrition and physicalactivity during and after cancer treatment: an American CancerSociety guide for informed choices. CA Cancer J Clin53:268–291
89. Kroenke CH, Fung TT, Hu FB et al (2005) Dietary patternsand survival after breast cancer diagnosis. J Clin Oncol23:9295–9303
90. Colditz GA (2005) Estrogen, estrogen plus progestin therapy,and risk of breast cancer. Clin Cancer Res 11:909s–917s
91. Garcia-Closas M, Brinton LA, Lissowska J et al (2006) Estab-lished breast cancer risk factors by clinically important tumourcharacteristics. Br J Cancer 95:123–129
92. Suzuki R, Rylander-Rudqvist T, Ye W et al (2006) Body weightand postmenopausal breast cancer risk dened by estrogen andprogesterone receptor status among Swedish women: a pro-spective cohort study. Int J Cancer 119:1683–1689
93. Suzuki R, Ye W, Rylander-Rudqvist T et al (2005) Alcohol andpostmenopausal breast cancer risk dened by estrogen andprogesterone receptor status: a prospective cohort study. J NatlCancer Inst 97:1601–1608
94. Takeuchi H, Baba H, Kano T et al (2005) The time-relatedchanges of the importance of prognostic factors in breast cancer.A sequential multivariate analysis of 1423 Japanese patients.Breast Cancer Res Treat 94:273–278
95. Zahl PH, Tretli S (1997) Long-term survival of breast cancer inNorway by age and clinical stage. Stat Med 16:1435–1449
96. Liu S, Edgerton SM, Moore DH 2nd et al (2001) Measures of cell turnover (proliferation and apoptosis) and their associationwith survival in breast cancer. Clin Cancer Res 7:1716–1723
97. Alexander FE, Anderson TJ, Brown HK et al (1999) 14 years of follow-up from the Edinburgh randomised trial of breast-cancerscreening. Lancet 353:1903–1908
98. Tabar L, Yen MF, Vitak B et al (2003) Mammography servicescreening and mortality in breast cancer patients: 20-yearfollow-up before and after introduction of screening. Lancet361:1405–1410
99. Shen Y, Yang Y, Inoue LY et al (2005) Role of detectionmethod in predicting breast cancer survival: analysis of randomized screening trials. J Natl Cancer Inst 97:1195–1203
100. Joensuu H, Lehtimaki T, Holli K et al (2004) Risk for distantrecurrence of breast cancer detected by mammography screen-ing or other methods. JAMA 292:1064–1073
101. Peto R, Boreham J, Clarke M et al (2000) UK and USA breastcancer deaths down 25% in year 2000 at ages 20–69 years.Lancet 355:1822
102. Johnstone PA, Norton MS, Riffenburgh RH (2000) Survival of patients with untreated breast cancer. J Surg Oncol 73:273–277
103. Fisher B, Jeong JH, Bryant J et al (2004) Treatment of lymph-node-negative, oestrogen-receptor-positive breast cancer:long-term ndings from National Surgical Adjuvant Breast andBowel Project randomised clinical trials. Lancet 364:858–868
104. Clarke M, Collins R, Darby S et al (2005) Effects of radio-therapy and of differences in the extent of surgery for earlybreast cancer on local recurrence and 15-year survival: anoverview of the randomised trials. Lancet 366:2087–2106
105. Fisher B, Jeong JH, Anderson S et al (2004) Treatment of axillary lymph node-negative, estrogen receptor-negative breastcancer: updated ndings from National Surgical AdjuvantBreast and Bowel Project clinical trials. J Natl Cancer Inst96:1823–1831
106. Hurley J, Doliny P, Reis I et al (2006) Docetaxel, cisplatin, andtrastuzumab as primary systemic therapy for human epidermalgrowth factor receptor 2-positive locally advanced breast cancer.J Clin Oncol 24:1831–1838
107. Romond EH, Perez EA, Bryant J et al (2005) Trastuzumab plusadjuvant chemotherapy for operable HER2-positive breast can-cer. N Engl J Med 353:1673–1684
108. Ernst MF, Voogd AC, Coebergh JW et al (2004) Using loco-regional recurrence as an indicator of the quality of breast cancertreatment. Eur J Cancer 40:487–493
109. Stefoski Mikeljevic J, Haward RA, Johnston C et al (2003)Surgeon workload and survival from breast cancer. Br J Cancer89:487–491
110. Simunovic M, Rempel E, Theriault ME et al (2006) Inuence of hospital characteristics on operative death and survival of patients after major cancer surgery in Ontario. Can J Surg49:251–258
111. Houterman S, Janssen-Heijnen ML, van de Poll-Franse LV et al(2006) Higher long-term cancer survival rates in southeasternNetherlands using up-to-date period analysis. Ann Oncol17(4):709–712
112. Haerslev T, Jacobsen GK, Zedeler K (1996) Correlation of growth fraction by Ki-67 and proliferating cell nuclear antigen(PCNA) immunohistochemistry with histopathological parame-ters and prognosis in primary breast carcinomas. Breast CancerRes Treat 37:101–113
113. Gaffney DK, Brohet RM, Lewis CM et al (1998) Responseto radiation therapy and prognosis in breast cancer patientswith BRCA1 and BRCA2 mutations. Radiother Oncol47:129–136
114. Mansi JL, Gogas H, Bliss JM et al (1999) Outcome of primary-breast-cancer patients with micrometastases: a long-term follow-up study. Lancet 354:197–202
115. Page DL, Gray R, Allred DC et al (2001) Prediction of node-negative breast cancer outcome by histologic grading andS-phase analysis by ow cytometry: an Eastern CooperativeOncology Group Study (2192). Am J Clin Oncol 24:10–18
116. Houterman S, Janssen-Heijnen ML, Verheij CD et al (2004)Comorbidity has negligible impact on treatment and complica-tions but inuences survival in breast cancer patients. Br J
Cancer 90:2332–2337117. Siegelmann-Danieli N, Khandelwal V, Wood GC et al (2006)Breast cancer in elderly women: outcome as affected by age,tumor features, comorbidities, and treatment approach. ClinBreast Cancer 7:59–66
330 Breast Cancer Res Treat (2008) 107:309–330