“an evidence-based guideline of using music therapy for managing pain...
TRANSCRIPT

Abstract of thesis entitled
“An Evidence-based Guideline of Using Music
Therapy for Managing Pain in Adults with
Cancer”
Submitted by
Li Yim Yim
for the degree of Master of Nursing
at The University of Hong Kong
in August 2012
Pain is a common problem that affects nearly all cancer patients
(Kwekkeboom, 2008). There are various factors that constitute suffering to cancer
patients. Apart from physical pain, cancer patients usually experience emotional
crisis and spiritual struggles (Magill, 2008).
Music therapy is believed to be one of the most effective treatments for
cancer patients. It provides a holistic care to patients with cancer. It will not only
manage the physical sensation, but also address the psychological, social and
spiritual parts of the patients (Magill, 2009). Although current studies have

suggested the benefits of using music therapy in reducing pain for cancer patients,
it is not a common practice in Hong Kong.
As the administration rate of music therapy relies heavily on the knowledge
of the nurses (Kwekkeboom, 2008). Therefore, this paper aims at providing
evidence on the use of music therapy. In the hope of a clinical guideline, it can
increase the administration rate of music therapy for cancer pain management in
clinical setting.
Apart from the clinical guideline, an implementation and evaluation plan on
music therapy will also be discussed in this paper. There will be a full description
from preparation to evaluation. Nurses can make use of this reference guide to
provide music therapy for their cancer patients in respect to pain management.

An Evidence-based Guideline of Using Music
Therapy for Managing Pain in Adults with Cancer
by
Li Yim Yim
B.Nurs. H.K.U.
A thesis submitted in partial fulfillment of the requirements for
the degree of Master of Nursing
at The University of Hong Kong.
Aug 2012
i
Declaration
I declare that this thesis represents my own work, except where due
acknowledgment is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualification.
Signed……………………………………………………………….
Li Yim Yim

ii
Acknowledgement
I would like to express my heartfelt gratitude to my supervisor Dr. Sharron
Leung. She has provided me a lot of support and inspirations all along my
dissertation. Whenever I got problems concerning the dissertation, she was always
there. Without her guidance, I could not be able to finish my dissertation so
successfully.
Besides, I would like to express my sincere thanks to my family members
especially Mr. Yeung Chun Hoi who had been so patient and generous during
these two years.
Last but not least, I would also like to say thank you to my lovely classmates
especially Ar Yu and Kennis who had been very kind and helpful.

iii
Contents
Declaration …………………………………………………….……………..…...……….i
Acknowledgement ………………………………………….………………………..……ii
Table of Contents ………………………………………………...………………..........iii
Lists of appendices…………………….………………………….…………………….....v
Chapter 1 Introduction
Background ……………………………………..…………..…………….…1
Affirming Needs ……………………………...…………………...…………4
Objectives of Dissertation ……..………..……………….………..…………7
Research Question ……………………………...……………………………7
Significance ……………………………….…………….……………..…….7
Chapter 2 Critical Appraisal
Searching Strategies ………………..…………………………..…………...9
Summary of Data ……………..……………………………………………11
Synthesis of Data ……………..………………………….………...……….15
Recommendation ………………..………………………………………….23
Conclusion …………………..……………………………………………...24
Chapter 3 Implementation Potential
Setting and Target Audience ….…………….…….………………………..25
Transferability of Findings .....………….……………….…………….……26
Feasibility…………………………………………………………………...29
Cost-benefit Ratio ………………....……………………...………………..33
Conclusion …………………….……………………………………………37
Chapter 4 Evidence-based Practice Guideline ……………………………….38

iv
Chapter 5 Implementation Plan
Stakeholders ……………………………………………………..…………44
Communication Plan ………………………………………….……………46
Communication Process ……………………………………………………48
Pilot Test …………………………………………………………….……..51
Chapter 6 Evaluation Plan
Outcome Evaluation ……………….………………………….……………56
Process Evaluation …………………………………………………………57
Chapter 7 Conclusion …………………..…………………………...…………61
Appendices ………………………………………………………………………63
References ……………………………………………..……………………….109

v
Appendices
Appendix I
Searching History …………………………………...………………...……63
Appendix II
Table of Evidence ……………………………………………………….…64
Appendix III
CASP Evaluation ……………………………………..……………………72
Appendix IV
Summary Table of the Sampled Studies …….……….....……..………...…88
Appendix V
Recommendation Table of the Sampled Studies …………….…..…..…….90
Appendix VI
Quality Assessment Summary of the Sampled Studies ……………………91
Appendix VII
Material and Non-material Cost …………..……………………………..…92
Appendix VIII
Benefits of Implementing Music Therapy ………………..………..………93
Appendix IX
Cost-benefits Ratio for Implementation of Music Therapy …...…………...94
Appendix X
Level of Evidence (SIGN) …………………………………………………95
Appendix XI
Grade of Recommendation (SIGN) …………..……………………………96
Appendix XII
音樂治療紀錄表 (第一部份) …………………..………………..…..……97

vi
音樂治療意見調查表 (第二部份) ………………………………..………98
Appendix XIII
Music Intervention Evaluation Form (Part 1) …………….………………100
Survey on Music Intervention (Part 2) …………………….….…………..101
Appendix XIV
Staff Self-evaluation Survey on Music Intervention …………..………….103
Appendix XV
Quiz On Music Intervention ………………………………..………..…....105
Appendix XVI
Doctors’ Perspective Survey on Music Intervention ……….…………….106
Appendix XVII
Eligibility Checklist for Music Intervention ………..………………….…107
Appendix XVIII
Time Table for Music Intervention ……………….………………………108

1
Chapter 1 Introduction
Pain is a common problem that affects nearly all cancer patients (Kwekkeboom,
2008). As pointed out by Catane et al. (2006), every one out of two cancer patients
will suffer from psychiatric disorders. Further pointed out by Huang et al. (2010),
about 38% of the newly diagnosed cancer patients and 81% of terminal cancer
patients report pain. In fact, cancer pain can occur in any stages of the illness (Skyes
et al., 2003). Untreated pain can cause depression, anxiety, hopelessness and even
desire to die (Huang et al., 2010). In the view of promoting a better well being, a
multidisciplinary approach for pain control should be allocated to cancer patients.
Background
The Prevalence and Incidence of Cancer in Hong Kong
According to the Hong Kong Cancer Registry, there were 24635 new cases
identified in 2008. Nowadays, male and female counterparts in Hong Kong are
expected to have an average age of 79.6 and 86.1 respectively. Further revealed by
Catane et al., (2006), the incident rate of cancer for people with age of 75 or above is
relatively high. With an increased life expectancy, more people are expected to suffer
from cancer which means cancer pain will be one of the major problems that medical
professionals need to tackle with in the coming and near future.

2
Pain Management in Hong Kong and its Adverse Effects
Pain is defined as a combination of physiological, affective, cognitive, emotional
and behavioral experience (Kwekkeboom, 2008). In Hong Kong, cancer pain is
usually treated by pharmacologic method which may be only effective in targeting
physical sensation part of pain (Catane, et al., 2006). However, other parts like social,
emotional and behavioral functioning of the individuals may be neglected
(Kwekkeboom, 2008). Furthermore, the use of analgesic would lead to a lot of side
effects on top of its advantages.
The Raise of Non-pharmacologic Method
On the other hand, there is an increasing number of studies examined the effect
of non-pharmacologic method in treating pain. The use of non-pharmacologic method
provides a multidisciplinary approach of care which addresses different needs in
respect to physical, emotional, cognitive and spiritual components of the patient
(Huang et al., 2010). However, the administration rate of the identified
evidence-based practice relies heavily on the knowledge of nurses to the specific area
(Kwekkeboom, 2008). Hence, the purpose of this research is to translate the best
evidence into a clinical guideline where nurses can use it to implement music therapy
on adult cancer patients.

3
The Definition of Cancer Pain
Cancer pain is defined as a combination of physiological, cognitive, emotional
and behavioral experience (Kwekkeboom et al., 2008). As cancer pain constitutes
different dimensions, it is usually referred as ‘total pain’.
Cancer pain can be attributed by cancer itself, cancer related treatments and
diagnostic procedures or cancer caused disability (Skyes et al., 2003). The perception
of pain is subjective. It can be affected by ones’ mood, morale, culture and ethnicity
(Skyes et al., 2003). Cancer pain can be further featured as acute or chronic pain.
The definition of acute pain.
Acute pain is usually associated with invasive diagnostic procedures
(Margoles and Weiner, 2010). For instance, bone marrow biopsy or fine needle
aspiration is inevitable in the diagnosis of solid tumors (Shabanloei et al., 2010).
The definition of chronic pain.
Chronic pain is defined as intermittent pain or continuous pain that lasts for
more than 3 - 6 months (Margoles and Weiner, 2010). Chronic pain in cancer
patients can be aroused from tumor itself like tissue inflammation, necrosis,
obstructed lymphatic and blood vessels, distended organs or edema (Huang et al.,

4
2010). It can also come from cancer accompanied treatments like radiation
therapy, chemotherapy or surgeries.
The treatment options for cancer pain.
Recent statistics revealed that 60% of the cancer patients suffering from
more than one type of pain (Catane et al., 2006). No matter the patient suffers
from acute or chronic pain, pharmacologic method is the dominant pain
treatment in Hong Kong. However, the use of analgesic can cause serious
negative impacts.
Commonly used pain medication comprises of Nonsteroidal
Anti-inflammatory Drugs (NSAID) and opioidal analgesic. For incidence,
NSAID may cause epigastric upset and risk of severe renal toxicity. In addition,
opioidal analgesic could cause nausea and vomiting, drowsiness, constipation
and respiratory depression (Catane et al., 2006). Therefore, it provokes the
need of non-pharmacologic method in treating pain for adult cancer patients.
Affirming Needs
Pain is a common problem that experienced by almost all cancer patients but
cannot be completely treated by medications. In contrast, non-pharmacologic
interventions could provide a more comprehensive approach in treating different

5
dimensions of pain. For instance, non-drug method can affect ones’ mood, emotional
response to pain, pain behavior and perceptions of personal control over pain
(Kwekkeboom, 2008).
Types of Non-pharmacologic Interventions
There are numerous types of non-drug interventions. Some of the most popular
interventions include music therapy, guided imagery, relaxation and distraction
(Bardia et al., 2006).
Music therapy entails the use of different kinds of musical pieces. On the other
hand, guided imagery refers to the use of imagery to affect one’s physical, emotional,
or spiritual state (Bardia et al., 2006). In addition, relaxation most likely involves
muscle relaxation. Last but not least, distraction derives a focus of attention where
undesirable condition can be escaped (Kwekkeboom, 2003).
On the whole, music therapy is selected because it can provide a comprehensive
approach in treating different dimensions of pain. How music affects each dimension
component of pain will be explained in the following paragraphs.
The effect of music on psychological and physical sensation of pain.
Music therapy itself can act as a ‘relaxation’ and ‘distraction’ tool.
According to Kwekkeboom (2003), music can withdraw a patient’s attention to
pain which shows similar effect to distraction. In addition, music can stimulate
6
the brain to reduce the level of stress hormones and exert a positive impact on
emotions where anxiety can be reduced (Kwekkeboom, 2003).
The effect of music on social and cognitive dimension of pain.
Pleasurable emotion allows patients to express their feeling which in term
will improve their communication between family members and health care
providers (Magill, 2008). Further pointed out by Kwekkeboom (2003), music
therapy can also relieve the feeling of hopelessness and ameliorate perception of
pain control.
Definition of music therapy.
According to the American Music Therapy Association, music therapy is
defined as “the clinical and evidence-based use of music intervention to
accomplish individualized goals within a therapeutic relationship by a
credentialed professional” (Pawuk & Schumacher, 2010). Many previous studies
have indicated a positive effect for its implementation on pain relief (Li et al,
2011). It is a save, convenient and cost effective treatment for relieving pain and
anxiety (Nguyen, Hellstrom & Bentgson, 2010). It can be directly administered
by nurses without the need to have a physician order.

7
Objectives of the Dissertation
1. To conduct a translational research on the effectiveness of music therapy in
reducing pain for adult cancer patient.
2. To perform a critical appraisal on the identified studies.
3. To extract evidence from the identified studies so as to develop a clinical
guideline on pain management for adult cancer patients in respect to the use of
music.
4. To discuss the implementation potential and evaluation plan for music therapy on
ward setting level.
Research Question
What is the effectiveness of music therapy in reducing pain for adult cancer
patients in Hong Kong?
Significance
Pain is a significant problem that affects nearly all cancer patients (Kwekkeboom,
2008). An effective intervention in pain management will be beneficial to patients,
nurses and institutions.
From the Patient Point of View
Music therapy provides a comprehensive approach for treating different
dimensions of pain. Music has been proven to be effective in reducing physical

8
sensation of pain (Huang et al., 2010). Besides, social functioning can be improved as
a result of better communication (Magill, 2008). In addition, psychological tension
can be relieved with a reduction of stress hormone (Kwekkeboom, 2003). Lastly,
cognitive behavior can be changed as a result of better control on pain perception
(Kwekkeboom, 2003).
From the Nurse Point of View
An effective pain management can reduce the demand of nursing care. Music
therapy is easy, safe and convenient to carry out (Nguyen, Hellstrom & Bentgson,
2010). It can be directly administered by nurses without the need to have a physician
order.
From the Institution Point of View
Implementation of music therapy is not expensive. It can thus save the medical
resources so that any extra resources can be spent on other areas in need. Lower
admission rate can also be achieved due to better pain management.

9
Chapter 2 Critical Appraisal
The translational research starts with keyword search from various databases. In
this chapter, there will be a detailed description on the searching process from
identifying keywords to the selection of potential studies. The identified studies will
be further rated according to their level of evidence while valuable data extracted
from the selected studies will be used for synthesis.
Searching Strategies
Identification of Studies
The first step was to identify keywords related to the translational research. The
keywords included ‘music’, ‘music therapy’, ‘pain’, ‘cancer’ and ‘neoplasms’. A total
of four electronic databases were used to search for potential studies on 17th
of August
in 2011. The databases used were MEDLINE, CINAHL, Pubmed and British Nursing
Index. The literature search was conducted in each of the above databases by using
the identified keywords both separately and in combination with each other. Only
English journals within 10 years of publishing will be accepted.
Inclusion Criteria
The studies selected should include:
1. Male or female patients

10
2. Age 18 or above
3. Either suffering from acute or chronic pain
4. Either use active or passive form of music therapy for pain management
Exclusion Criteria
All qualitative studies, pilot studies, editorials and author’s opinion will be
excluded.
Search Result
After the searching processes with its restriction on the inclusion and exclusion
criteria, there were a total of 67 potential articles identified from the four databases.
These articles were then screened with title and abstract. All duplicated articles were
deleted. After that, the reference lists of the relevant articles were further screened to
search for any potential useful studies. Two articles were extracted from the reference
list of the selected literatures. Finally, a total of eight studies were selected for this
literature review. Appendix I showed the searching history of the same set of
keywords in respect to different databases.
Data Extraction and Quality Assessment of the Sampled Studies
The eight sampled studies were extracted and data were recorded in the form of
table of evidence. Critical Appraisal Skills Programme [CASP] (2006) was used to
perform the quality assessments of the selected studies. After that, the level of

11
evidence of the sampled articles will be rated according to the Scottish Intercollegiate
Guidelines Network [SIGN] (2008). The table of evidence and the table of quality
assessment are shown in Appendix II-III.
Summary of Data
Types of Study
Appendix IV and V summarized the data of the eight studies in a table form. The
eight sampled studies were published between 2003 and 2011. Six of them were
randomized controlled trials (Allred et al., 2010; Clark et al., 2006; Huang et al., 2010;
Kwekkeboom, 2003; Li et al., 2011; Nilsson et al., 2003). The remaining two samples
were quasi-experimental pretest posttest studies (Good & Abn, 2008; Shabanloei et al.,
2010)
Sample Size
For those six sampled randomized controlled trial studies, the sample size varied
from 58 to 151 (Allred et al., 2010; Clark et al., 2006; Huang et al., 2010;
Kwekkeboom, 2003; Li et al., 2011; Nilsson et al., 2003). For the two
quasi-experimental pretest posttest studies, the sample size lied between 50 and 73
(Good & Abn, 2008; Shabanloei et al., 2010).
12
Patient’s Characteristics
RCT studies.
Four out of six RCT studies included patient with a diagnosis of cancer
(Clark et al., 2006; Huang et al., 2010; Kwekkeboom, 200; Li et al., 2011). The
stage of cancers varied from stage 1-4. The remaining two RCT studies focused
on patients undergoing Arthroplasty or day case surgeries (Allred et al., 2010;
Nilsson et al., 2003). All of the six studies were given with either active or
passive music therapy with or without words.
Quasi-experimental pretest posttest studies.
One study recruited samples undergoing for gynecologic surgery (Good &
Abn, 2008). Another one study included patient receiving bone marrow biopsy
and aspiration (Shabanloei et al., 2010). Both of the studies were given with
passive music therapy with or without words (Good & Abn, 2008; Shabanloei et
al., 2010).
Intervention
RCT studies.
Li et al. (2011) examined the effect of passive music therapy on
postoperative pain and chemotherapy. Besides, Allred et al. (2010) and Nilsson et
al. (2003) observed the effect of passive music on intra and postoperative pain.

13
On the other hand, Clark et al. (2006) investigated the effect of active music on
chemotherapy while Huang et al. (2010) inspected the effect of passive music on
usual cancer pain. Last but not least, Kwekkeboom (2008) compared the effect of
music and distraction on procedural pain. All of the above studies had compared
the effect of active or passive music therapy to a control group (Allred et al.,
2010; Clark et al., 2006; Huang et al., 2010; Kwekkeboom, 2003; Li et al., 2011;
Nilsson et al., 2003).
Quasi-experimental pretest posttest studies.
Good & Abn (2008) studied the effect of Korean and American Music on
women after gynecologic surgery. On the other hand, Shabanloei et al. (2010)
examined the effect of passive music in patients undergoing bone marrow biopsy
and aspiration.
Time of Data Collection
Participants in six studies were followed up and data was collected on a daily
basis (Allred et al., 2010; Good & Abn, 2008; Huang et al., 2010; Kwekkeboom, 2003;
Nilsson et al., 2003; Shabanloei et al., 2010). While in other two studies, participants
were followed up and data was collected on a weekly basis (Clark et al., 2006; Li et
al., 2011).

14
Outcome Measures for Pain
There were totally three different types of pain scales used in the sampled studies
including Numeric Rating Scale (NRS), Visual Analog Scale (VAS) and Short-Form
of McGill Pain Questionnaire (SF-MPQ). Clark et al. (2006) solely used NRS for the
measurement of pain intensity. On the other hand, Good & Abn (2008) used VAS for
pain measurement. Three studies measured the level of pain with both the Numeric
Rating Scale and Visual Analog Scale (Huang et al., 2010; Kwekkeboom, 2003;
Shabanloei et al., 2010). In addition, Allred et al. (2010) used the SF-MPQ and VAS
as the pain scales. Lastly, Li et al. (2011) used only SF-MPQ for pain measurement.
Effect of music on pain.
Active music therapy.
There was a reduction on pain level for cancer patient during radiation
therapy but it was not statistically significant with p value > 0.05 (Clark et al.,
2006).
Passive music therapy.
Four RCTs and two quasi-experimental pretest posttest studies showed a
significant reduction in pain for music group with respect to intra and post
operation, chemotherapy, usual pain and bone marrow biopsy. (Allred et al.,
2010; Huang et al., 2010; Li et al., 2011; Nilsson et al., 2003; Good & Abn, 2008;

15
Shabanloei et al., 2010). On the other hand, Clark et al. (2006) and Kwekkeboom
(2003) showed no significant difference in pain level between the music group
and control group.
Drop Out Rate
The drop out rate of the 6 RCTs varied from 0 – 12.5% while the drop out rate of
the two quasi-experimental studies was zero.
Synthesis of Data
A summary for the synthesis of the quality assessment of the eight sampled
studies was listed in Appendix VI. All the sampled studies had asked a clearly-focused
question on the effect of music therapy in either acute or chronic pain. This included
studies to examine the effect of music on medical procedures, radiation or
chemotherapy, intra or post-operation or usual pain.
Besides, six out of eight studies were designed appropriately with a
randomization. The remaining two articles used the pretest posttest study designs. All
these eight studies were rated in respect to their level of evidence (High, Medium or
Low) according to the Scottish Intercollegiate Guidelines Network (SIGN). Several
factors like the probability of bias, significance, reliability and application of the
evidence will be considered in the rating.

16
Level of Evidence
High level of evidence.
According to Scottish Intercollegiate Guidelines Network (2008), high level
of evidence refers to studies which ‘fulfilled all or almost of the criteria’. In
addition, conclusion drawn from these studies or review with high level of
evidence are thought to be very unlikely to alter (Scottish Intercollegiate
Guidelines Network, 2008). From the eight sampled studies, one randomized
controlled trial was rated as high level of evidence (Nilsson et al., 2003). This
study would be given a “1++” sign to indicate for high level of evidence.
Bias was unlikely to happen.
In this study, both the control group and experimental groups were well
balanced. Besides, the randomization was done by using a computer-generated
list which could minimize selection bias. In addition, double blinding method
was used in this study to reduce observer bias. Furthermore, all participants in
the study were followed up and data was collected on a daily basis in the same
way which could reduce performance bias. Last but not least, the sample size
was calculated based on a power of 80% at the 5% level of significance. The
final sample size was further augmented from forty to fifty to allow a drop rate
of 20% in each group. The sample size was more than enough so that the play of

17
chance bias would be excluded.
All participants who entered the study were accounted for its conclusion.
Neither the intervention group could get a control group option nor could
the control group get an intervention group option. All participants in the study
were followed up. The drop out rate was zero. The participants were analyzed by
the group that they were originally allocated to eliminate intention-to-treat
analysis.
Significance and reliability.
P value and 95% confidence interval were used in this study to present the
result. Both the intervention groups and control group had a p value smaller than
0.05 which meant the result was significant. The pain level of the study was
measured by Numeric Rating Scale with reliability and validity tested. Therefore,
the information provided was precise and reliable.
Application of the evidence.
The study contains applicable evidence to my proposed research setting
which would benefit cancer patients who will be undergoing surgeries. Our
current practice of pain management may be changed as a result of the trial
(Nilsson et al., 2003).

18
Medium level of evidence.
According to Scottish Intercollegiate Guidelines Network (2008), medium
level of evidence referred to studies with some of the criteria fulfilled. In addition,
“Those criteria that have not been fulfilled or not adequately described are thought
unlikely to alter the conclusion” (Scottish Intercollegiate Guidelines Network,
2008, p.55). For those studies which are considered as medium level of evidence,
a “1 +” or “1 –” sign would be used for indication.
From the eight sampled studies, five randomized controlled trials were
considered as medium level of evidence because the identified studies would only
fulfill some of the requirements as listed (Allred et al., 2010; Clark et al., 2006;
Huang et al., 2010; Li et al., 2011; Kwekkeboom, 2003).
Bias was unlikely to happen.
Four out of the five studies contained well balanced control and intervention
groups with stratification (Allred et al., 2010; Clark et al., 2006; Huang et al.,
2010; Li et al., 2011). Three sampled studies mentioned the method for
randomization (Clark et al., 2006; Huang et al., 2010; Li et al., 2011). Two of
them used minimization programme (Clark et al., 2006; Huang et al., 2010). On
the other hand, the remaining one study used randomization code generated by
computers to allocate participants into the control and intervention group.

19
Appropriate randomization method helped to reduce selection bias.
Two out of five studies used a single blinded method with only staff is
blinded during the research to minimize observer bias (Huang et al., 2010; Li et
al., 2011). All the five studies examined the effect of music with respect to
different situations, participants blinding was actually quite difficult.
All the participants were followed up and data was collected in the same
way. Therefore, performance bias could be minimized.
Only one study recruited a small amount of sample (Kwekkeboom, 2003).
Three of the studies recruited samples more than one hundred with effective
sample size calculated by power analysis (Allred et al., 2010; Huang et al., 2010;
Li et al., 2011). All those three articles designed to have a power of 80% at the
5% level of statistical significance. On the whole, most articles recruited enough
number of participants in order to reduce the play of chance bias (Allred et al.,
2010; Huang et al., 2010; Li et al., 2011).
Low drop out rate.
All of the participants who entered the trial were accounted for the
conclusion in the five studies (Allred et al., 2010; Clark et al., 2006; Huang et al.,
2010; Li et al., 2011; Kwekkeboom, 2003). Neither the participants in
intervention group could get a control group option nor could the control group

20
participants get an intervention group treatment. The drop out rate of the five
studies varied from 0 – 12.5 % (Allred et al., 2010; Clark et al., 2006; Huang et
al., 2010; Li et al., 2011; Kwekkeboom, 2003). Three studies had zero percent
drop out rate (Allred et al., 2010; Clark et al., 2006; Kwekkeboom, 2003). Two
studies had a drop out rate less than thirteen percent (Huang et al., 2010; Li et al.,
2011). Overall, the drop out rate was low.
Significance and reliability.
Two of the five studies were precise enough to make a decision. P value was
used to present the result with 95% confidence interval provided (Huang et al.,
2010; Li et al., 2011). Both of the studies were statistically significant with p
value < 0.05. On the other hand, two studies with p value provided but
confidence interval was missing (Allred et al., 2010; Clark et al., 2006). Both the
studies had a p value > 0.05 which represented insignificant result.
All the five studies used validated and reliable tools for pain intensity
measurement. Clark et al. (2006) solely used NRS for the measurement of pain
intensity. Two studies measured the level of pain with both the Numeric Rating
Scale and Visual Analog Scale (Huang et al., 2010; Kwekkeboom, 2003).
Besides, Allred et al. (2010) used the SF-MPQ and VAS as the pain scales. Lastly,
Li et al. (2011) used only SF-MPQ for pain.

21
All the studies above contains applicable evidence to my proposed research
setting which would benefits cancer patients who will be undergoing surgeries,
radiation therapy or chemotherapy, invasive medical procedures and complaining
usual cancer pain. Our current practice of pain management may be changed as a
result of the trial (Allred et al., 2010; Clark et al., 2006; Huang et al., 2010; Li et
al., 2011; Kwekkeboom, 2003).
Low level of evidence.
According to Scottish Intercollegiate Guidelines Network (2008), low level
of evidence referred to those studies which fulfilled few or none of the criteria. In
addition, conclusions drawn from those studies are likely or very likely to alter
(Scottish Intercollegiate Guidelines Network, 2008). A “2 ++” sign will be used
to indicate for studies with low level of evidence.
From the eight sampled studies, two of them were regarded as low level of
evidence (Good & Abn, 2008; Shabanloei et al., 2010). They were rated as low
level of evidence because they achieved only a few criteria listed.
Both of the studies had a quasi-experimental pretest posttest design,
randomization was not available. As a result, there was a high chance of selection
bias.
Both of the studies did not mention about the blinding method. This would

22
increase the risk to bias.
All of the participants who entered the trial were accounted for the
conclusion. Neither the participants in intervention group could get a control
group option nor could the control group participants get an intervention group
treatment. The drop rate was zero in both studies.
All the participants were followed up and data was collected in the same way.
Therefore, performance bias could be minimized.
Good & Abn (2008) provided information on calculation of effective size
with power set at 80% but Shabanloei et al. (2010) did not. Both of the studies
may not be precise enough to make a decision. For incidence, only p value was
provided in the two studies without the provision of confidence interval. Both of
the study results were statistically significant with p value < 0.05.
Both the studies used reliable and validate measurement tool for pain
intensity. Good & Abn (2008) used VAS for pain measurement. On the other hand,
Shabanloei et al. (2010) measured the level of pain with both the Numeric Rating
Scale and Visual Analog Scale.
Both the studies above had some results applicable to my proposed research
setting. Therefore, the current practice may be changed as a result of the studies.

23
Recommendation
Based on the findings of the selected studies, there are several recommendations
regarding the use of music therapy on pain management of adult cancer patients.
There were six out of eight studies supported that music therapy was effective in
treating either acute or chronic pain experienced by cancer patient. Therefore, the
use of music therapy should be highly encouraged among cancer patients. (Allred et
al., 2010; Clark et al., 2006; Huang et al., 2010; Kwekkeboom, 2003; Li et al., 2011;
Nilsson et al., 2003). Since the identified studies were carried out in both Western and
Eastern countries, the result of the studies were highly generalizable.
All the selected studies stated the need of an informed consent before initiation
of music. It should thus consider as a routine practice to get the consent from the
patient before any music therapy sessions.
Both Huang et al., (2010) and Li et al., (2011) had highlighted the importance of
considering cultural background for the selection of music. It should be noted that
cultural preference of the patients should be valued.
Although there is no restriction on the tempo of the music, three out of eight
studies suggested that music at a tempo of 60-80 beats per minute was preferable than
others as it can provide a sedative effect (Allred et al., 2010; Huang et al., 2010;
Nilsson et al., 2003).

24
Concerning the duration and frequency of music therapy, three out of eight
studies suggested that at least one music session which lasts for about twenty to thirty
minutes should be provided to patient with respect to either acute or chronic pain
(Allred et al., 2010; Huang et al., 2010; Li et al., 2011).
No matter the music was song with or without words, it had shown a significant
reduction on the pain level of the patient after the music therapy. Three studies
explained that words inside the song may have special meaning to patient (Good &
Abn, 2008; Huang et al., 2010; Li et al., 2011). On the other hand, song without words
can prevent patient from focusing on the words which may affect the effectiveness of
music (Allred et al., 2010; Shabanloei et al., 2010). Therefore, patient’s preference is
rather important.
Conclusion
There were a total of eight studies including six randomized controlled trial and
two quasi-experimental pretest posttest studies which were reviewed in this paper.
The quality of the sampled studies was assessed. Important data synthesized from the
selected studies will be useful to develop the clinical guideline on the use of music
therapy for pain management on adult cancer patients in the later chapter.

25
Chapter 3 Implementation Potential
The above chapters have presented a general idea on the benefits and
effectiveness of music therapy on pain management in adult cancer patients. In order
to implement the innovation into real clinical settings, a thorough assessment on
transferability, feasibility and cost/benefit ratio must be carried out.
Setting and Target Audience
Characteristics of the Target Setting
Music therapy is proposed to be carried out in the mixed ward of St. Paul’s
Hospital (SPH). SPH is 1 of the 13 private hospitals in Hong Kong. It is located on
the Hong Kong Island. It provides a total of 361 beds. The ward units are divided into
General Ward, Paediatric Ward, Nursery, Intensive Care Unit, Triage Ward and Day
Centre. Under General Ward, it is furthered subdivided into surgical, medical and
mixed wards. Patients are admitted to different ward units with respect to their
conditions and room rate. In the Mixed Ward of SPH, there will be both medical and
surgical cases regardless of different sexes.
Target Audience
Both male and female adult cancer patients (age 18 or above) who suffer from
acute or chronic pain will be eligible for the intervention. They can be patients
diagnosed with various types and stages of cancers. According to the Hong Kong

26
Cancer Registry, the most common sites of cancers for both sexes are lung,
colorectum, breast, liver, prostate, stomach, nasopharynx, non-melanoma skin,
Non-Hodgkin's lymphoma and Corpus uteri. This cancer site ranking was also
applicable to the Mixed Ward of SPH. Concerning the definition of acute and chronic
pain, it is already well defined in Chapter 1.
Transferability of Findings
Transferability refers to whether the findings of the selected studies can be
transferred to my own working environment. In order to utilize the findings of the
selected studies, comparison on similarities in terms of demographic factors,
philosophy of care, number of patient beneficial from the intervention and time
consumption on implementation and evaluation have to be assessed thoroughly.
Characteristics of the Selected Studies
There were both Asian and Western studies selected for the translational research.
Demographic factors like gender, marital status, religion, employment and education
level were well considered in these selected studies. Other than that, the selected
studies had recruited patients with various types of cancer and stages. In order to
investigate the effect of music on different perspectives of pain, studies with both
diagnostic and treatment procedures were included as well.

27
Similarities between the Selected Studies and Current Clinical Settings
The findings of the selected studies are highly comparable to the target audience
of my own working environment. Initially, cancer patients of 18 above with different
nationality and background from all over the world could be admitted to the mixed
ward of SPH. They can be patients suffered from different types and stages of cancer.
Some of them may admit due to diagnostic procedures like bone marrow or tissue
biopsy while others may come for surgery or even chemotherapy.
Philosophy of Care
Coherently, SPH shares similar philosophy of care to music intervention. The
first mission of SPH is to provide a high standard of service by restoring health and
providing tender loving care to patient. The notion of music therapy is similar. It aims
at providing a comprehensive care for cancer patients physically, psychologically and
socially.
From physical point of view, music therapy can reduce pain effectively through
distraction (Kwekkeboom, 2003). Socially, music can improve communication
between patients and others (Magill, 2008). This is because music can induce
pleasurable emotion which allows patients to express their feeling. Psychologically,
music can stimulate the brain to reduce the level of stress hormones and exert a
positive impact on emotions. Thus, music can enhance mood and relieve anxiety

28
(Kwekkeboom, 2003).
The second mission of SPH is to treat all patients equally regardless of their
colour, race or creed in the name of Lord Jesus Christ. Similarly, music is a universal
language. It shares common languages across different cultures and ethic groups.
Number of Patients Benefited from the Innovation
According to the Hong Kong Cancer Registry, there were 24635 new cases
identified in 2008. Undoubtedly, both the prevalence and incidence are in an
increasing trend. Recently, it is estimated that there are 45 new admissions per month
related to either cancer treatments or accompanied diagnostic procedures in my
working place. Further stated in Kwekkeboom (2008), nearly all cancer patients
experience pain at some point from their illness. Therefore, there will be large enough
proportion of patients benefited from the innovation.
Required Materials for Music Therapy
According to Nguyen, Hellstrom& Bentgson (2010), music therapy is a save,
convenient and cost effective treatment for relieving both pain and anxiety. Most
preferably, it can be directly administered by nurses without the need to have a
physician order. Moreover, only simple materials are needed to carry out the
innovation. This includes a set of earphones, a sound player and a database for
selection of music. In fact, the benefits of the innovation might even double here in

29
SPH. This is because all the materials needed to implement the innovation are readily
usable except lacking a music library for the provision of music.
Time Consumption on Implementation and Evaluation
All nurses including Nursing Officer (NO), Registered Nurse (RN) and Enrolled
Nurse (EN) will be fully responsible for the implementation. Generally speaking, it
does not take long to implement music therapy. It takes about 30 minutes for nurses to
carry out assessment and education. Each session of music therapy will last less than
30 minutes while the main process is determined by patients themselves. Patients are
free to initiate and terminate the intervention at any point of time. However, music
intervention should be provided for at least 5 minutes in procedural pain and 20-30
minutes for chronic pain in order to obtain a therapeutic effect (Allred et al., 2010;
Huang et al. 2010; kewekkboom.2003; Li et al. 2011). Finally, the evaluation part will
spend less than five minute through completing a set of questionnaire.
Feasibility
Feasibility refers to whether music intervention is feasible to be carried out in my
own clinical setting. Several factors needed to be considered for feasibility and each
factor will be discussed in the following paragraphs. The identified factors included
freedom to implement, interference to current staff, availability of administrative
support and resources, requirement on staff training and special skills as well as

30
presence of clinical tools for evaluation.
Freedom to Implement
On one hand, music therapy provides autonomy for nurses as it can be initiated
without physician’s order. On the other hand, it provides another treatment option for
cancer patients in terms of pain management. Under all circumstances, patients have
the right to receive or stop the innovation at any time point.
Interference to Current Staff
Workload will be slightly increased at the beginning because assessment and
education takes time. However, the overall workload will be decreased. Currently,
pharmacologic approach is the main management for cancer patients in my own
clinical setting. In many occasions, pain medication will be given to patient upon their
requests. When they experience pain, they will use the call bell very frequently on
requesting pain medication. As a result of that, a lot of man power is squandered in
answering the call bells. Even worse, when the current available analgesic cannot
relieve pain satisfactorily, nurses also need to call the doctor upon request of pain
medication. However, it usually takes time for doctors to answer back for medication
prescription. Therefore, the implementation of music therapy actually brings prompt
relieve to patients through a better and efficient care provided by nurses.

31
Availability of Administrative Support
SPH has done a lot of innovations after decanting to a new block (A block). One
of the breakthroughs is the implementation of SAP system. Each patient is now
entitled with a so called ‘bed side terminal’ where they can watch TV programmes,
listen to the radio and assess to the internet. Recently, the hospital has also
emphasized the importance of evidence based practice. Therefore, any evidence based
innovation which would bring benefits to the patients will be always welcomed by the
hospital.
Requirement of Special Skills and Staff Training
Unlike aseptic techniques or other critical nursing care, music therapy does not
require special skills. However, basic training for staff is needed. In general, most of
my colleagues showed little knowledge on music therapy. Thus, staff training is
crucial. It is proposed that two training sessions will be given to ward nurses. Each
training session takes about 2 hours. The first training session is an introductive
course where fundamental knowledge like definition, benefits and intervention
guideline on music therapy will be provided. The second training session emphasizes
application where different case scenarios will be demonstrated. A question and
answer session will also be available in the second training session so that frontline
staff can share their problems concerning the innovation.

32
Availability of Equipment
Some equipment needed to be prepared in order to implement music therapy in
the ward setting level. This includes a set of earphones, a sound player and a database
for music selection. Concerning the earphones, it is already available for every
inpatient. This is because each new admission under SPH is supplied with an
Admission Kit. Inside the Admission Kit, there is a disposable set of earphones inside.
In addition, patients would use the Bed-Side Terminal as the sound player for music.
In order to increase the selection choices of music, it is proposed that a music library
should be purchased. Congruously, Naxos Music Library will be the choice as it
provides a variety of music like Classical, Jazz, World, Classic Rock, Nostalgia music
and Opera. There are more than 60000 CDs available from their database. What is
more the Naxos Music Library can be set up easily without the need of special
software. Patient can assess to the database easily through the bed-side terminal. Most
importantly, it is not expensive. It cost only about USD 200 for annual subscription
per account. The account can be used by different patients from the whole hospital.
Presence of Tools for Clinical Evaluation
Numeric Rating Scale will be used for the evaluation of pain level. It is one of
the most common scales which showed both reliability and validity for measurement
of pain intensity. It contains a 0-10 scale where 0 = no pain and 10 = most pain

33
experienced (Clark et al., 2006).
Cost-benefit Ratio
A balance between the cost and benefit must be strived in order to implement
music intervention successfully. Ideally, benefit of the innovation should exceed the
cost of putting the innovation into practice. In the following paragraphs, both benefit
and cost will be discussed.
Risk of Continuing Current Practice
Up till now, pharmacologic approach is the dominant pain management for adult
cancer patients in my working place. As analgesic can cause intolerance, it will cause
exaggerative use of pain medication easily. Besides, analgesic could lead to a lot of
side effects. Common side effects include drowsiness and constipation (Details
concerning the side effects of analgesic were stated in Chapter 1). Because analgesic
targets on reducing physical sensation of pain, psychological and social function of
cancer patient is often neglected.
Benefits of Music Therapy
Music is effective in reducing pain. Music therapy itself can act as a ‘relaxation’
and ‘distraction’ tool. According to Kwekkeboom (2003), music can withdraw a
patient’s attention to pain. In addition, music can stimulate the brain to reduce the
level of stress hormones and exert a positive impact on emotions where anxiety can be

34
reduced (Kwekkeboom, 2003). Apart from that, pleasurable emotion aroused by
music allows patients to express their feeling which in term will improve their
communication between family members and health care providers (Magill, 2008).
Further pointed out by Kwekkeboom (2003), music therapy can also relieve the
feeling of hopelessness and ameliorate perception of pain control.
Potential Benefits Brought by Music Therapy
From the patient point of view.
Music therapy provides a multidisciplinary approach for pain management in
adult cancer patients. Patient will get more satisfaction towards the hospital with
respect to reduced pain and anxiety level. Improved mood also encourage patient
to share their feeling with others so that normal social life functioning of the
patients can be maintained. Better pain control will also reduce the length of
hospitalization which in turn helps patient to save money. As a whole, the quality
of life of cancer patient can be enhanced.
From the nurse point of view.
As music therapy can be initiated by nurses themselves without the need of
physician’s order, nurses can enjoy a higher autonomy for clinical practice. If
there is adequate pain control measures for patients, the frequency of call bells and
phone orders for pain medication prescription can be reduced. Thus, the overall

35
demand of work will be decreased. Coherently, good reputation of the hospital
could increase occupancy so that staff bonus could be assured.
From the hospital point of view.
Music intervention shares similar mission and philosophy of care to SPH
where ‘high standard of service’ can be achieved through it implementation.
Besides, effective and innovative evidence based practice would also live up the
hospital reputation and act as a role model to other hospitals in Hong Kong.
Cost for Implementation of Music Therapy
There is material cost as well as non-material cost for the implementation of
music therapy. (Details on material and non-material cost will be shown on Appendix
VII)
Material cost.
The implementation of music bears some material cost. Firstly, a music
library needs to be purchased for the provision of musical pieces. The annual
subscription cost of Naxos Music Library per account is USD 200. It is estimated
two new cancer cases will be admitted each day. It is better to spare 5 accounts for
Naxos Music Library as patient will be staying in the hospital for 2 days on
average. Therefore, a total of 5 accounts will be needed which cost USD 1000
annually (approximately HKD 7800). In addition, printing cost for each set of
36
assessment and evaluation forms will be rated about $0.3. The printing cost for
training materials charged about $2 per nurse. As stationery, earphones and sound
player are readily usable from the hospital, no extra cost will be charged.
Non-material cost.
Manpower and venue for holding the training sessions are the main
non-material cost for carrying out music intervention. On average, the monthly
salary of a nurse working in a mixed ward is $29117. An hourly salary is
approximately $ 165.4. Each nurses needs to attend a 4 hour training session
which will cost about $661.6. There will be a total of 17 nurses attending the
training sessions. It will cost about $11247.2. In addition, there will be altogether
4 training session provided by a RN. The total spending on providing training will
be rated $1363.2. On the other hand, no extra cost will be charged on venue as
venue for holding the training session is readily available from the hospital once
approval can be made.
Cost-benefits ratio on implementation of music.
Generally, the medication expense on pain control per patient is about
$78.3/day. Patients’ hospitalization will be shortened if pain control is satisfactory.
The expenses staying one more day in a mixed ward will charge about $2400
including doctor’s fee and room charges. Therefore, a patient needs to spend more

37
than $2400 for each extra day staying in the hospital can be saved (Details on the
calculation of cost/benefit ratio will be shown on Appendix VIII and Appendix
IX).
Conclusion
Transferability, feasibility, and cost for music implementation are well discussed
in this chapter. It is noted that music therapy is highly transferable, feasible and cost
effective. Music therapy shares similar target population and philosophy of care to
current clinical setting. It is also predicted that there will be also large enough
population of patients benefited from the intervention. Overall, music intervention can
reduce the workload of nurses. On the other hand, it provides a comprehensive care to
patients. It helps patients physically, socially and psychologically. From the institution
point of view, the mission of ‘providing a high standard of service’ can be achieved by
providing music therapy. Moreover, the cost of continuing current practice largely
exceeds the cost of implementing new innovation. Thus, it is worth putting music
therapy as another pain management option for patients, nurses as well as the
institution.

38
Chapter 4 Evidence Based Practice Guideline
In the above chapter where transferability, feasibility and cost and benefits were
thoroughly discussed, it is noted that music therapy is a cost effective treatment for
pain management in adult cancer patients. As stated before, the administration rate of
non-pharmacologic method relies heavily on the knowledge of the nurses
(Kwekkeboom, 2008). In the view of promoting this innovative intervention to the
daily ward practice, it is of ultimate importance to develop an evidence based practice
guideline.
Details of the Guideline
Title
The title will be “A guideline for the use of music therapy for managing cancer
pain in adult patients.”
Aim
The purpose is to guide nurses on the use of music therapy for relieving cancer
pain in adult patients
Objectives
The objectives of the evidence based practice guideline are:
1. To reduce pain in different types of cancer patients
2. To encourage the use of music therapy through EBP
39
Target Population
Music therapy will be provided to both male and female cancer patients whom
are admitted to the mixed ward of St. Paul’s Hospital. The inclusion criteria are:
1. Patient of age 18 or above
2. Who experience acute or chronic pain
3. Without hearing deficit and
4. Cognitive impairment
Keys to the Quality of Recommendation
Both the level of evidence and the grade of recommendation will follow the
suggestions given by Scottish Intercollegiate Guidelines Network [SIGN] (2008). The
grade of recommendation will be ranging from A to D which will be stated at the end
of each recommendation. For detailed description on the level of evidence and the
grade of recommendation, please refer to Appendix X and Appendix XI. It is noted
that the recommendation guideline will comprise of five parts:
1. Assessment
2. Preparation
3. Selection of Music
4. Duration and Frequency of Music Therapy and
5. Evaluation

40
Assessment.
Recommendation 1.0.
The hearing ability and cognitive state of clients should be assessed for
the eligibility of music intervention. (A)
Patient with hearing deficit or cognitive impairment may not be able to
reflect the effectiveness of music therapy (Allred et al., 2010; Clark et al.,2006;
Huang et al., 2010; Kwekkeboom et al., 2003; Nilsson et al., 2003). (1+)
Preparation.
Recommendation 2.0.
Informed consent needs to be obtained before the music intervention.
(A)
It is because some people just simply do not like music or allergic to music
(Li et al., 2011) (1+); some of them may not be able to focus on music (Huang et
al., 2010) (1+) while others may not see music as a therapy to reduce pain (Good
& Abn, 2008). (2++)
Recommendation 3.0.
Patient needs to put on headphones when listening to the selected
music. (A)
Use of earphones can prevent outside environment from disturbing the

41
patient (Li et al., 2011; Nilsson et al., 2003). (1+; 1++) It can also help the
patient to concentrate on hearing the music (Huang et al., 2010). (1+)
Recommendation 4.0.
Patients have to rest on bed during the innovation and avoid
interruptions. (A)
There are 6 out of 8 selected studies showed a significant reduction on pain
when having an intervention on bed (Allred et al., 2010; Good & Abn, 2008;
Huang et al., 2010; Li et al., 2011; Nilsson et al, 2003). (1+; 2++; 1+; 1+; 1++)
Selection of music.
Recommendation 5.0.
Use patient’s preferred music. (A)
Individually chosen music is familiarized, liked and has meaning for patient
(Good & Abn, 2008). (2++) Apart from that, liked and culturally familiarized
music can distract patient from pain and relax patient more (Huang et al., 2010;
Li et al., 2011). (1+)
Recommendation 6.0.
The tempo of music is better at 60-80 beats/min. (A)
The identified tempo can provide a sedative effect and decrease the chance
of increasing the heart rate by entrainment (Allred et al., 2010; Huang et al.,

42
2010; Shabanloei et al., 2010). (1+; 1+; 2++) It can also produce a calming effect
and an increased sense of well being (Allred et al., 2010). (1+)
Recommendation 7.0.
The music piece can be song with or without words. (A)
With lyrics.
The words inside the song may have special meaning to patient (Good &
Abn, 2008; Huang et al., 2010; Li et al., 2011). (2+; 1+; 1+)
Without words.
This can avoid patient from focusing on the words which may affect the
effectiveness of music (Allred et al., 2010; Shabanloei et al., 2010). (1+; 2+)
Duration and frequency of music therapy.
Chronic pain.
Recommendation 8.0.
Two sessions of music therapy with 20- 30 minutes duration should be
provided each day (morning and evening). (A)
Appropriateness of the duration of music therapy is well supported (Allred et
al., 2010; Huang et al. 2010; Li et al. 2011). (1+)
43
Acute pain.
Recommendation 9.0.
Music therapy is provided during the procedure. (B)
It can significantly relieve pain and anxiety through cognitive behavioral
interventions. It can distract patient’s attention to pain (Kwekkeboom, 2003;
Shabanloei et al., 2010). (1+; 2++)
Evaluation.
Recommendation 10.0.
A post-intervention assessment should be done immediately after the
innovation. (A)
It can effectively reveal the absolute effect of music intervention on pain
relieve right after the intervention (Allred et al., 2010; Clark et al., 2006; Good &
Abn, 2008; Huang et al., 2010; Kwekkeboom, 2003; Li et al., 2011; Nilsson et al.,
2003; Shabanloei et al., 2010). (1++; 2++)

44
Chapter 5 Implementation Plan
After formulating the intervention protocol, now it comes to the implementation
plan. Clinically, it is not easy to put a new intervention into practice. Staff resistance
is one of the crucial concerns in implementing a new protocol. Thus, a thorough
planning is needed well before to overcome any expected and unexpected obstacles.
Undoubtedly, implementation plan set a good framework for the whole process.
Communication allows stakeholders to raise their concerns and problems regarding
the new intervention so that the interest and benefit of each party can be strived. In the
following paragraphs, the communication plan with different stakeholders, the flow of
communication and the process of communication will be discussed.
Stakeholders
Stakeholders refer to those people whom may be affected by the innovation
(Burns and Grove, 2005). Each stakeholder plays an important role to the project.
Their decision is the key success to the innovation. Through their support and
participation, valuable data and information can be gathered to refine the guideline.
The stakeholder identified in this innovation includes the Hospital Administrative
Director, Senior Nursing Officer (SNO), Nursing Officer (NO), Nurses (Registered
Nurse and Enrolled Nurse), Vice Medical Superintendent, Residential and Visiting
Doctors as well as patients.

45
The Role of Nursing Officer and Senior Nursing Officer
The nursing officer is an experienced nurse who has a lot of experience in
carrying out new innovation. She is the key person to identify potential problems in
this project. She also has to predict feasibility by balancing the cost and benefits of the
intervention. Last but not least, the NO needs to set timeframe for each process so that
the innovation can be carried out in a proposed period of time. On the other hand, the
SNO needs to in charge of the whole project.
The Role of Vice Medical Superintendent
Vice Medical Superintendent is the doctor responsible for administration medical
issues in respect to doctors. In this innovation, he is accountable to promote the new
innovation to both Residential and Visiting doctors. He is the key person to initiate
changes to doctors.
The Role of Hospital Administrative Director
Hospital Administrative Director is the key person to make approval regarding to
establishment of new measures. Hospital benefit is his key interest. He will be
accountable for balancing the cost and benefits bringing from the new intervention.
Besides, he is also accountable to compare the vision between the hospital and new
innovation to make sure there is no discrepancy.

46
Communication Plan
The communication plan describes the communication between the proposer and
the stakeholders. The objective of communication is to get support from different
stakeholders and to get funding from the administrative hierarchy. Therefore, the aims
and objectives of the new innovation should be explained to the identified
stakeholders clearly.
Communication with Nursing Officer (NO)
In order to make the innovation successful, we need to gain support from the
identified stakeholders. The proposer of the project will first approach to the Nursing
Officer through RNIC-NO handover. Nursing officer in SPH is responsible for
management of identified ward. There will be a 15 minutes handover time each day
for the Registered Nurses in Charge to report any big issues concerning the ward to
the Nursing Officer. The proposer will make use of the 15 minutes handover time to
give a brief presentation to the Nursing Officer. The presentation should be short and
precise. The idea of the innovation should be explained to the NO clearly with
benefits of the innovation highlighted. Without the endorsement of NO, the
innovation cannot be further delivered to the higher hierarchy of the hospital.
The Establishment of Innovation Committee
Three RNs will be selected by the NO to form the innovation committee. The
47
innovation committee takes active role in provoking the need of change to current
practice with evidence. Apart from that, they need to foresee obstacles and figure out
solutions in respect to the new innovation. Last but not least, they are also responsible
to present the innovation to different hierarchy mentioned above.
Communication with Higher Administrative Hierarchy
An innovation presentation which emphasizes strong evidence support practice
and potential benefits will be given to SNO through the regular ward meeting by the
innovation committee. Thereafter, a similar presentation will be held during the
regular IC meeting in order to gain the approval from the Hospital Administrative
Director.
When the project is approved by the Hospital Administrative Director, it is high
time to introduce the innovation to the Vice Medical Superintendent via the regular
multidiscipline meeting. In SPH, the Vice Medical Superintendent is the team leaders
of the Residential Doctors. The innovation can be further spread to the frontline staff
and patients once the Vice Medical Superintendent nods with the innovation.
After getting the approval from upper hierarchy and support from various
identified stakeholders, there will be a 2 weeks time exchange period for questions
and data collection before the pilot test. In the exchange period, stakeholders are free
to raise their comments and concerns regarding the new innovation.

48
Communication Process
The communication process is divided into three stages: initiation, facilitation
and sustaining phase. Each of process is in identical importance which will be
discussed below.
Initiation
The proposer starts the initiation by sharing the experience of managing cancer
pain of adult patients with the NO. During the meeting, the proper will present the
idea of alternative treatment (music therapy), its effectiveness and benefits, the role of
implementing evidence-based practice in promoting nursing care standard, as well as
the problem of continuing current practice. After that, the innovation committee
which comprised of 3 RNs will be formed under the selection of NO.
The role of innovation committee.
The key role of the innovation committee is to provoke the need of change
to current practice with evidence. The NO of the innovation committee will
present the proposed innovation to the leaders identified above during routine
meeting where questions and concerns can be raised from the floor. The
innovation committee will collect the information and use valuable data to
reformulate the evidence-based guideline. Undoubtedly, a well structured and
detailed guideline can promote the use of the intervention.

49
Before implementing the innovation, proper education and training are
needed. The innovation committee will provide 2 training sessions (each session
takes 2 hour) to each nurse to ensure competency. When putting the innovation
into practice, the innovation committee also needs to monitor and audit the
frontline staff to evaluate effectiveness. Definitely, there will be numerous
problems encountered when putting a new innovation into real practice. The
innovation committee is expected to figure out appropriate solution with respect
to the identified problems.
Facilitation
After getting a good start, it comes to facilitation. In order to gain a success,
support from different parties is needed.
Ways to get support from frontline staff.
Without the support from frontline staff, the innovation cannot put into
practice. There will be a 5-10 minutes information sharing session during the
handover time from an A shift to a P shift. The information session will persist
for a week time in order to let all nurses to know about the new innovation.
During the information session, a leaflet attached with the training session
timetable will be distributed to nurses. The website address for online forum
discussion will also be printed in the leaflet. The online forum provides a good

50
channel for frontline staff to raise their comment, concern and problems about
the new intervention.
Ways to get support from doctors.
Visiting Doctors and Residential Doctors.
A detailed information booklet will be sent to doctor’s clinic. Undoubtedly,
the doctors will be willing to introduce the new innovation to patient if it is not
expensive and effective. Therefore, data on cost per patient and effectiveness of
the music intervention will be highlighted in the booklet. At the back of the
booklet, a survey will be attached (Please refer to Appendix XVI for details). The
visiting doctors are free to express their idea concerning the new innovation.
Similarly, the booklet will be also sent to the residential doctors through personal
hospital email account.
Ways to get support from patients.
Music intervention for pain management is a new term to most of the patients.
Therefore, adequate propaganda is needed. Free leaflet can be obtained from the
leaflet boxes in the Outpatient Department and all general wards. Posters will also
be put up on the notice board. Information on the new intervention can also be
acquired from the Hospital Monthly Newsletter and Hospital Webpage.
51
Sustaining
The sustaining phase is about the maintenance of the innovation. In order to keep
the new innovation flow continuously, nurse compliance should be maintained. The
effectiveness of the music intervention can be shown by comparing statistics on
complaints and satisfaction for pain management between current practice and
innovation through charts. Positive reinforcement will therefore be obtained from
sharing these successful stories to frontline nurses during the handover time and
regular ward meeting. In addition, nurses’ compliance can be measured through
documentation and auditing. Certificate will be awarded to the ward with highest
compliance to appreciate their efforts.
Pilot Test
Pilot test is carried out before large scale of implementation of music therapy to
all general wards. The pilot test is used to test for feasibility, transferability and
acceptability of music therapy. Besides, any unexpected problems or misconception
can be checked out during the pilot test. Other than that, data collected from the pilot
test will be useful to refine the original protocol. Thus, it can increase the probability
of success towards the new innovation. The details of the pilot test will be discussed
in the following paragraphs.

52
Setting
The pilot test will be implemented on a 19 bed semi-private mixed ward in St.
Paul’s Hospital.
Study Design and Samples
Quasi-experimental study design will be used for the pilot test which measures
the pain level of the patient before and after the test. The patients are recruited
through convenience sampling.
Sample Size
With reference to the sample size calculation in the Evaluation (please refer to
Chapter 6 for details), 40 patients are needed for the pilot test. Assuming around 7
patients will be recruited each week, it takes about 6 weeks to recruit all the patients
needed.
Inclusion Criteria for the Patients
Cancer patients who satisfy the following criteria will be recruited for the study.
1. Age 18 or above
2. Suffer from either chronic or acute pain
3. Able to speak Cantonese or English
4. Without hearing deficit and cognitive impairment

53
Education and Training to Ward Nurses
The pilot test will be carried out by the innovation committee (RNs x 3) and the
nurses (RNs x 7and ENs x 8) working in the A19 ward unit. Two 2 hour training
sessions will be provided before the pilot test. The first training session is an
introductive course where fundamental knowledge like definition, benefits and
intervention guideline on music therapy will be provided. The second training
emphasizes application where different case scenarios will be demonstrated. A
question and answer session will also be available in the second training so that
frontline staff can share their problems concerning the innovation.
Procedure.
When new cancer patients are admitted to the ward A19, responsible nurses
will screen for the eligibility of the patients towards the intervention. Only
patients who can fulfill the above inclusion criteria will be invited for the study.
Patients who agree to use music therapy for pain control need to sign a consent
form before the intervention. After that, a 15 minutes introductive course will be
given to patients on the use of bedside terminal, knowledge on the selection of
music from Naxos Music Library and briefing on Post Intervention Evaluation
Form. Patient is required to rate their pain level before and after the each music
therapy session. On the discharge day, invited patient is required to complete the

54
whole pile of Intervention Evaluation Form. The way to complete the
Intervention Evaluation Form on the discharge day is to encourage patients to
give comments on the arrangement for the whole process rather than on a daily
basis.
Assess for feasibility.
The availability of equipment and resources can be predicted through the
pilot test. The equipment needed for music intervention includes a set of
earphones, a sound player and a database for music selection. Both the earphones
and sound player are readily usable in SPH. The only concern is about the
database (Naxos Music Library). For instance, questions concerning the number
of subscriptions needed, convenience and accessibility of the database can be
tested out via pilot test.
Assess for acceptability and nurses compliance.
Each patient is asked to rate their satisfaction concerning the new
innovation in the survey. On the other hand, ward nurses are asked to fill in
another set of survey to check for their acceptability, level of workload,
competence, compliance and comments regarding music intervention (For details
of the evaluation form, please refer to Appendix XII-XIV).
55
Review the pilot test for further improvement.
The pilot test takes six weeks time to complete for the whole process. Data
collected from the pilot test is useful for future practice. The results of the pilot
test will be useful to predict the effectiveness, cost and benefits of the innovation.
In addition, problems raised and comments collected from the pilot study will
also be used to refine the protocol. Other than that, the pilot test can act as a good
buffer to test for feasibility, acceptability (patients and nurses) as well as the
compliance of nurses towards the new innovation. Thus, pilot test increase the
probability of success towards the new innovation.

56
Chapter 6 Evaluation Plan
The aim of evaluation is to review the effectiveness of the innovation. It provides
good evidence to stakeholders on how the innovation is processing and its outcome
effectiveness. In the following paragraphs, evaluation on outcome and process will be
discussed.
Outcome Evaluation
Patient’s Pain Level
Patient needs to complete the whole pile of Music Intervention Evaluation Form
on the discharge day. The Music Intervention Evaluation Form consists of two parts
(Appendix XIII). The first part contains the pain level rating of patients and their
blood pressure before and after the intervention. The second part is patients’ survey on
music intervention. In the survey, invited patients are asked about their comments and
satisfaction towards music intervention
Outcome Measures
Patient’s Pain Level is measured by Numeric Rating Scale (NRS) before and
after the intervention. The NRS is a common measurement for pain which shows
good reliability and validity (Clark et al., 2006). In the Intervention Evaluation Form,
patient is asked to rate the pain level before and after the intervention in a 0-10 scale
where 0 is equal to no pain and 10 is equal to most pain experienced.

57
Process Evaluation
Nurses’ Compliance and Knowledge
Nurses compliance can be checked by documentation auditing through the
Eligibility Checklist for Music Intervention and Staff Self-Evaluation Survey on
Music Intervention (Please refer to Appendix XVII and Appendix XIV for details). In
addition, nurses’ knowledge can be tested through quiz and returned skill
demonstration to the innovation committee. Only multiple choice questions will be
asked in the quiz (Please refer to Appendix XV for details). Nurses need to achieve
100% of the total marks in order to get a pass. For those who failed the quiz, a half
hour revision class will be provided. The failure will need to retake the quiz again.
Other than quiz, an anonymous self-evaluation survey will be distributed to the nurses
to ask about their competence, compliance and confidence in implementing the new
innovation. The self-evaluation survey is a 5 point graded scale survey where 1 =
totally disagree and 5 = totally agree. When the staff completed the survey, they
should return the survey to the collection box in Ward A19.
Cost and Benefit of the Hospital
The new innovation could shorten the length of hospitalization for patients. On
the other hand, it can live up the reputation of the hospital through enhanced nursing
care. Thus, higher hospital admission rate can be achieved due to better quality of care.

58
Actual statistical data can be obtained from the Monthly Admission Statistics.
Nature and Number of Client Involved
The inclusion criteria will be same as those stated in the pilot test. For those
patients who are not able to consent, have vision problem, hearing deficit or cognitive
impairment will be excluded from the study. In performing the statistical analysis, a
two-tailed t test will be used to see whether there is a reduction in pain level for
cancer patients. The sample size of the patient is calculated base on Russ Lenth
(2010). By using 5% margin of error and 80% power, the effective sample size is 126.
Assuming there is a 20 % drop rate which is common in the private hospital. Finally,
158 patients are needed for the study. Approximately, there are 7 eligible patients
each week, it takes 23 weeks to recruit all the samples. Therefore, the intervention
period will continue for about 6 month’s time.
Data Analysis
The main objective is to measure the pain level of the patient. The data collected
will be analyzed by the Statistical Package for Social Science (SPSS) Version 19. A
two paired t-test will be performed to test for significance.
Effectiveness of the innovation.
Pain level of the patients.
Patient’s pain level will be measured by the Numeric Rating Scale. Both the

59
baseline pain level before the intervention and pain level after the intervention will
be measured. The innovation is regarded as effective if 80% of the recruited
patients report less pain after the use of music therapy.
Nurses’ knowledge and compliance.
It should be noted that both the knowledge and compliance of nurses will
pose a great impact on the effectiveness of the innovation. Knowledge has a direct
impact on confidence. Nurses will implement the new innovation if they are
confident to do so. Therefore, nurses’ knowledge should be tested after the
training. The introductory course is said to be effective only if 95% of the ward
nurses passed the quiz. In order to get a pass for the quiz, nurses have to answer
all questions correctly.
On the other hand, even the innovation is evidently shown to be effective, if
nurses are not willing to provide the innovation to the patient, music therapy is
useless to the patients. Therefore, nurses’ compliance should be tested through an
anonymous self evaluation survey and documentation auditing. The compliance
will be considered as satisfactory only if 80% or above of the wards nurses are
compliant to the new innovation.
In the anonymous self-evaluation survey, ward nurses were free to express
their concerns and comments towards the new intervention. The survey will be

60
distributed to the ward nurses after one week implementation of the new
innovation. The survey will be redistributed again after one month’s time to see
whether there is any difference and change in existing problems concerning the
new practice.
Cost and benefit of the hospital.
The new innovation brings a win-win situation to both the patients and the
hospital. On one hand, the new innovation can shorten the hospitalization of the
patient and reduce the cost per patient per day. In addition, when the patients are
more satisfied with the hospital service, there will be less complaints and less
demand on nursing care for pain medication.
On the other hand, with promoted quality of nursing care, it can live up the
reputation of the hospital. The innovation is said to be effective if the hospital
admission rate and patient’s satisfaction is increased as well as staff input to
respond call bells for pain medication is reduced.
The effectiveness of the outcome can be measured through the above
evaluation. Data from the evaluation can provide good evidence on the
effectiveness of music intervention. Thus, it can give valuable information on
actual cost and benefits of the new innovation to each of the identified
stakeholder.

61
Chapter 7 Conclusion
Pain is known as one of the most horrible experience to most of the cancer
patients. No matter they are undergoing diagnostic tests or receiving treatment, pain
seems unavoidable. Cancer pain itself actually has many different dimensions other
than only physical part of it. Emotional upset and social dysfunction can also cause
pain to them. It raises the need of a multidisciplinary care approach to management
the pain of cancer patients.
Lately, a lot of large scale researches have been done to test for the efficacy of
music intervention on pain management of cancer patients. Nowadays, music
intervention has become one of the most common non-pharmacologic practices in
Western Countries. In deep, most of the identified sample studies in this translational
research had also indicated a positive effect of music therapy on reducing pain for
cancer patients.
Despite the fact that music is believed to be safe, inexpensive and easy to carry
out, it is not a common practice for pain management in Hong Kong. Many factors
determine the administration rate of music intervention. Common barriers to music
intervention are knowledge deficit and lack of evidence based practice guideline.
Thus, this paper was intended to provide an evidence based practice guideline for

62
ward nurses to implement music therapy on adult cancer patients in respect to pain
management.
The evidence based guideline was developed according to the best evidence
extracted from the identified studies. Transferability, feasibility, and cost for music
implementation were well examined in the previous chapters to ensure its application
to the real clinical setting.
Due to high prevalence of cancer incidents, it is believed that there will be large
enough proportion of patients benefited from the proposed music intervention. It is
hoped that this translational research can increase the awareness of ward nurses so as
to make music intervention as one of the active pain managements for adult cancer
patients.

63
Item Electronic Databases
Medline via
Ovid
CINAHL
via
EBSCOhost
Pubmed British Nursing
Index
Search Date 17/8/2011 17/8/2011 17/8/2011 17/8/2011
1. Music or Music. mp.
or Music Therapy or
Music Therapy. mp.
12414 118 13289 378
2. Cancer. mp. or
Neoplasms. mp.
927156 3491 2550736 11488
3. Pain or Pain. mp. 381861 2811 473708 6145
1 + 2 +3 56 5 76 6
Limit to Recent 10 Years
+
Limit to English
+
Eliminate Pilot and Preliminary Studies
+
Eliminate Duplication With Other Databases
+
Screen Reference Lists of the Relevant Studies
Total 8
Appendix I: Searching History

64
Bibliographic
Citation
Study
Design
Evidence
Level
Number of Patients
and Subject Characteristics
Intervention Comparison Length of
Follow Up
Outcome Measure Result
Allred, K.D.,
Byer. J.F. &
Sole, M. L.
(2010).
RCT 1 + - A total of 56 participants
Control group n = 28
Music group n = 28
- Participants were
1. Male or Female aged
from 18 -60 years
who
2. undergoing Total Knee
Arthroplasty (TKA)
- Music group
would hear
music for 20
minutes before
ambulation
- The music piece
with tempo 60 –
80 beats per
minute
- Rest for 20
minutes
before
ambulation
One day - The pain intensity
was measured by
McGill Pain
Questionnaire
Short Form
(MPQ-SF) and
Visual Analog
Scale
- Anxiety level was
measured by
Visual Analog
Scale
- Statistically insignificant
between control group
and music group in pain
and anxiety level.
- Significant reduction in
pain and anxiety level
between time T1 and T2
& T2 and T3 within
groups.
- Reduction in pain and
anxiety level within
groups was reduced in a
larger proportion to
control group.
Comment: Pain and anxiety level were statically insignificant between control and music groups. However, there was a larger reduction in pain and anxiety level within music group.
This suggested that music was more effective in reducing pain and anxiety before ambulation than rest alone. Music is suggested to use as a routine care plan for patients who are
undergoing TKA.
Appendix II: Table of Evidence

65
Bibliographic
Citation
Study
Design
Evidence
Level
Number of Patients
and Subject
Characteristics
Intervention Comparison Length of
Follow Up
Outcome Measure Result
Clark, M.,
Isaacks-Downton,
G., Wells, N.,
Redlin.-Frazier,
S., Eck, C.,
Hepworth, J. T.,
& Chakravarthy,
B. (2006).
RCT 1+ - A total of 63 cancer
patients were
recruited
- They were patients
who need to do
radiation therapy in a
comprehensive cancer
centre in VA
Music group: n = 35
Control group: n =28
- Music group was interviewed
by a music therapist
- During the interview,
participants would select
preferred music styles for use
as relaxation or distraction
- The music therapist would use
the interview to identify music
types that might be effective
- Listen to identified music
during RT
- The control
group would
receive usual
care without
exposure to a
music
therapist
- Ranged
from 1-7
weeks
relied on
the course
of radiation
therapy
1. Emotional distress
was measured by
a. Validate scale
b. Distress numeric
rating scale
(NRS)
2. Anxiety and
depression was
measured by Hospital
Anxiety and
Depression Scale
3. Fatigue was measured
by Profile of Mood
States Fatigue
- Music group had
1. Lower level of
anxiety
2. Lower level of
distress
- No significant
difference
between the music
group and control
group in
1. Depression
2. Fatigue
3. Pain
Comment: Music was found to be effective in reducing pain in other studies but not significant in this study. In fact, most of the sample here did report lower level of pain at baseline. This
might suggest that music would be more effective in patient who had certain level of pain intensity. This study had raised a very good suggestion which further research should be focused
more on the dose of music in order to provide optimal effect for the patients.
Appendix II: Table of Evidence
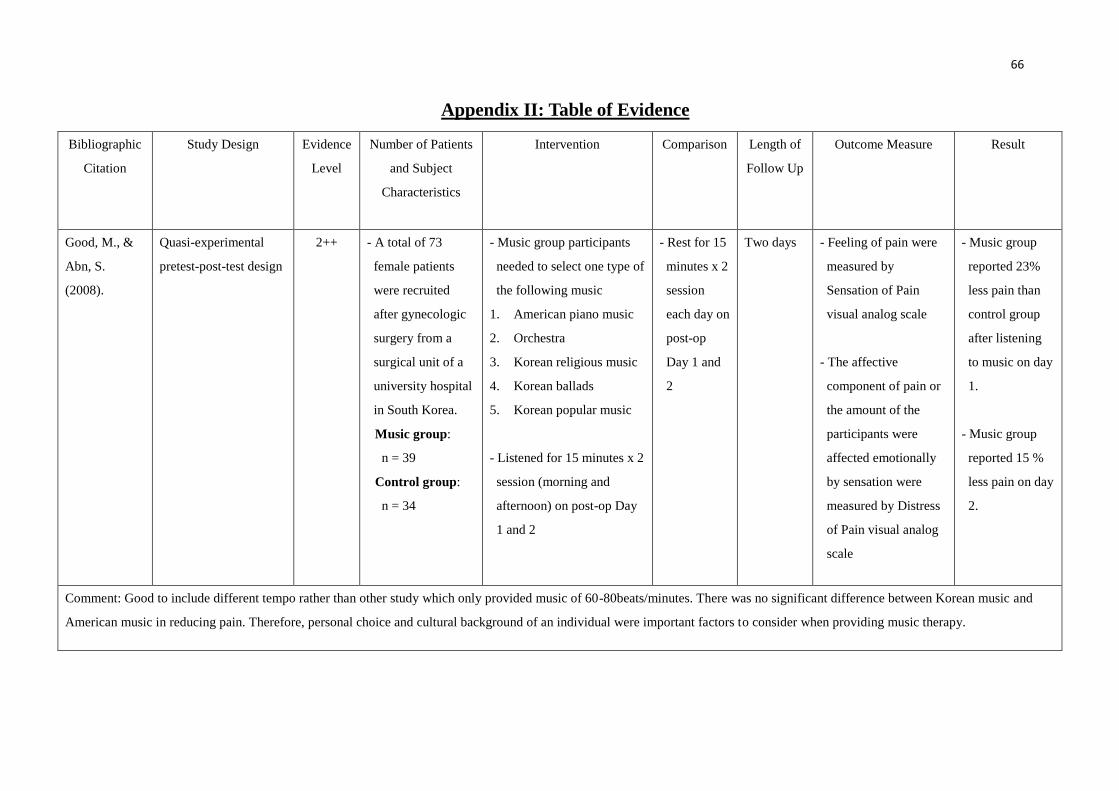
66
Bibliographic
Citation
Study Design Evidence
Level
Number of Patients
and Subject
Characteristics
Intervention Comparison Length of
Follow Up
Outcome Measure Result
Good, M., &
Abn, S.
(2008).
Quasi-experimental
pretest-post-test design
2++ - A total of 73
female patients
were recruited
after gynecologic
surgery from a
surgical unit of a
university hospital
in South Korea.
Music group:
n = 39
Control group:
n = 34
- Music group participants
needed to select one type of
the following music
1. American piano music
2. Orchestra
3. Korean religious music
4. Korean ballads
5. Korean popular music
- Listened for 15 minutes x 2
session (morning and
afternoon) on post-op Day
1 and 2
- Rest for 15
minutes x 2
session
each day on
post-op
Day 1 and
2
Two days - Feeling of pain were
measured by
Sensation of Pain
visual analog scale
- The affective
component of pain or
the amount of the
participants were
affected emotionally
by sensation were
measured by Distress
of Pain visual analog
scale
- Music group
reported 23%
less pain than
control group
after listening
to music on day
1.
- Music group
reported 15 %
less pain on day
2.
Comment: Good to include different tempo rather than other study which only provided music of 60-80beats/minutes. There was no significant difference between Korean music and
American music in reducing pain. Therefore, personal choice and cultural background of an individual were important factors to consider when providing music therapy.
Appendix II: Table of Evidence

67
Bibliographic
Citation
Study
Design
Evidence
Level
Number of Patients
and Subject Characteristics
Intervention Comparison Length
of
Follow
Up
Outcome Measure Result
Huang, S.T.,
Good, M. and
Zauszniewski,
J.A. (2010)
RCT 1++ - A total of 482 patients
assessed.
Control group n= 64
Music group n= 65
- Various type of cancer
patients (stage 1 - 4) were
recruited from two large
medical centers in
Kaohsiung City, Southern
Taiwan
- A 30 minutes
of self chosen
music will be
given to the
Music group
- Rest for 30
min (but they
will be given a
30 min of self
chosen music
in order to
blind them and
for
demoralization
after the 30
min rest)
Two days - Pain intensity was measured by numeric
rating scale in respect to
1. cancer pain
2. 24-h usual, least, and worst pain
3. analgesic “in effect” at the time of
testing,
- Compare severity of pain by visual analog
scale(from 0-10)
0 = no pain at all
10 = worst pain experienced
- Music group
had less posttest
pain than
control group
- Music group
scored average
1.5 units less
sensation of
pain than
control group
Comment: Good to involve patient with different types of cancer with stages 1 to 4. Music was significant in reducing pain in this study. Therefore, music could be effective in reducing pain
for different types of cancer from stage 1-4. However, only those participants who complain pain level of ≥3/10 will be included. It caused special caution when interpreting the intervention
for patients with mild pain.
Appendix II: Table of Evidence

68
Bibliographic
Citation
Study
Design
Evidence
Level
Number of Patients
and Subject Characteristics
Intervention Comparison Length of
Follow
Up
Outcome Measure Result
Kwekkeboom,
K.L. (2003)
RCT 1+ - A total of 60 patients who
were undergoing invasive
medical procedures were
recruited.
Music group: n = 24
Distraction group: n = 14
Control group: n= 20
-Music group:
1. Selected a compact
disc of their preferred
style of music
2. Listened to music 5-15
minutes before the
procedure till end
- Distraction group:
1. Selected their choice
of a book on tape
2. Listened to music 5-15
minutes before the
procedure till end
3. A short quiz would be
given to ensure
attention to the story
- Rested quietly
before and
during the
procedure
One day - Pain intensity
1. Measured by
numeric rating scale
2. From 0-10
0 = no pain at all
10 = worst pain
experienced
- Anxiety
1. Measured by
Speilberger
State-Trait Anxiety
Inventory-state
portion (STAI-s)
- No significant
difference
between the
music group
and distraction
group in pain
and anxiety
Comment: The result was not consistent with other study where music therapy is effective in reducing pain and anxiety level. It raised good suggestion that music and distraction should be
used to reduce pain before the procedure. Sample size was too small that results were not generalizable.
Appendix II: Table of Evidence

69
Bibliographic
Citation
Study
Design
Evidence
Level
Number of Patients
and Subject
Characteristics
Intervention Comparison Length of Follow Up Outcome Measure Result
Li, X.M., Yan,
H., Zhou, K.N.,
Dang, S.N.,
Wang, D.L. &
Zhang, Y.P.
(2011)
RCT 1+ - A total of 120 patients
were included
Control group : n =60
Music group: n = 60
- All are female patients
1. Aged between 25 –
65 years who
2. Needed to have
radical mastectomy
Music group:
- Listened to music
twice a day
- 30 minutes for
each session
- Once in the early
morning
( 6am-8am)
- Once in the
evening
(9pm – 11 pm)
- With routine
nursing care (With
PCA)
- With routine
nursing care
only (With
PCA)
- Hospital stay for
13.6 +/- 2.0 days
- Two chemotherapy
periods for 18.9 +/-
7.1 days
Pain is measured
by
1. McGill Pain
Questionnaire
(SFMPQ)
2. Visual
Analogue
Scale
3. Present Pain
Intensity
- Music therapy
reduces three main
pain scores
( PRI-total, VAS
and PPI)
significantly
Comment: Large sample size of RCT provide high level of evidence. The study result was consistent with other study where music therapy is effective in reducing pain. The study
design was similar to current clinical setting where result can be generalized.
Appendix II: Table of Evidence
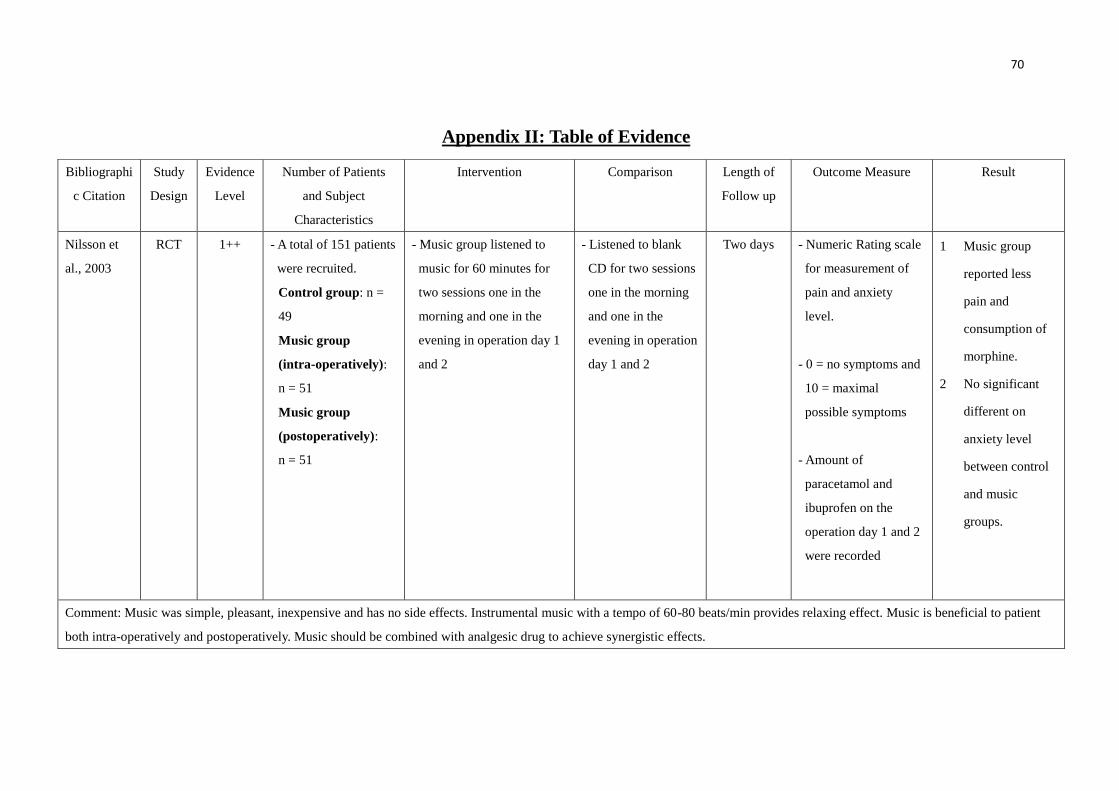
70
Bibliographi
c Citation
Study
Design
Evidence
Level
Number of Patients
and Subject
Characteristics
Intervention Comparison Length of
Follow up
Outcome Measure Result
Nilsson et
al., 2003
RCT 1++ - A total of 151 patients
were recruited.
Control group: n =
49
Music group
(intra-operatively):
n = 51
Music group
(postoperatively):
n = 51
- Music group listened to
music for 60 minutes for
two sessions one in the
morning and one in the
evening in operation day 1
and 2
- Listened to blank
CD for two sessions
one in the morning
and one in the
evening in operation
day 1 and 2
Two days - Numeric Rating scale
for measurement of
pain and anxiety
level.
- 0 = no symptoms and
10 = maximal
possible symptoms
- Amount of
paracetamol and
ibuprofen on the
operation day 1 and 2
were recorded
1 Music group
reported less
pain and
consumption of
morphine.
2 No significant
different on
anxiety level
between control
and music
groups.
Comment: Music was simple, pleasant, inexpensive and has no side effects. Instrumental music with a tempo of 60-80 beats/min provides relaxing effect. Music is beneficial to patient
both intra-operatively and postoperatively. Music should be combined with analgesic drug to achieve synergistic effects.
Appendix II: Table of Evidence

71
Bibliographic
Citation
Study Design Evidence
Level
Number of Patients
and Subject
Characteristics
Intervention Comparison Length of
Follow Up
Outcome Measure Result
Shabanloei, R.,
Golchin, M.,
Efanhani, A.,
Dolatkhan, R.,
&Rasoulian, M.
(2010).
Quasi-experimental
pre-test post test design
2 ++ - A total of 100
participants
Control group n = 50
Music group n = 50
- Participants were
1. Aged from 18 -60
years who
2. Undergo bone
marrow biopsy and
aspiration
- Music group would
hear music for 10 -
20 minutes during
the procedure.
- Three music piece
of temp with 70 –
80 beats per minute
1. Canon in D
major
2. Lover Story
3. Dance of the
Iguana
- Rest during
the procedure
One day - The pain and
anxiety level was
measured by
Spielberger
Stat-Trait
Anxiety
Inventory
(STAI).
- Music group
showed less pain
and anxiety.
Comment: The result of this study was consistent with other study that music would be effective in reducing pain and anxiety. It was good to study the effect of music on bone marrow
biopsy and aspiration as they are common procedures that encountered in clinical setting. However, only three types of music were provided here for selection. This may limit the effect
of music.
Appendix II: Table of Evidence

72
Appendix III: CASP Evaluation
Screening Questions Answer
1. Did the study ask a clearly-focused question? Yes.
2. Was this a randomized Controlled trial (RCT)
and was it appropriately so?
Yes.
3. Were participants appropriately allocated to
intervention and control groups?
Yes.
- There was no significant difference between the
control group and music group.
- The sample size of control group and music
group was similar.
4. Were participants, staff and study personnel
‘blind’ to participants’ study group?
Can’t tell.
- There is no information provided from the test
about blinding.
5. Were all of the participants who entered the
trial accounted for at its conclusion?
Yes.
- There is no intervention group participants got a
control group option or vice versa.
- There is no loss to follow up.
- All participants were analyzed by the groups they
originally allocated.
6. Were the participants in all groups followed up
and data collected in the same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to
minimize the play of chance?
Yes.
- The effective sample size was calculated at a
power of 80 % at a 5% level of significance.
8. How are the results presented and what is the
main result?
- The results are presented as a measurement of
anxiety and pain level.
- Statistically insignificant between control group
and music group in pain and anxiety level.
- Significant reduction in pain and anxiety level
between time T1 and T2 & T2 and T3 within
Allred, K.D., Byer. J.F. & Sole, M. L. (2010). The effect of music on postoperative pain and anxiety.
Pain Management Nursing, 11 (1), 15-25.

73
groups.
- Reduction in pain and anxiety level within
groups was reduced in a larger proportion to
control group.
9. How precise are these results? - Only p value is reported. The result may not be
precise enough to make a decision.
10. Were all important outcomes considered so the
results can be applied?
Yes.
- The study was similar to my clinical setting.
- Music improved general mood and reduced the
consumption of opioid.
- Music therapy was suggested as a routine plan
for patients undergoing Total Knee Arthroplasty.
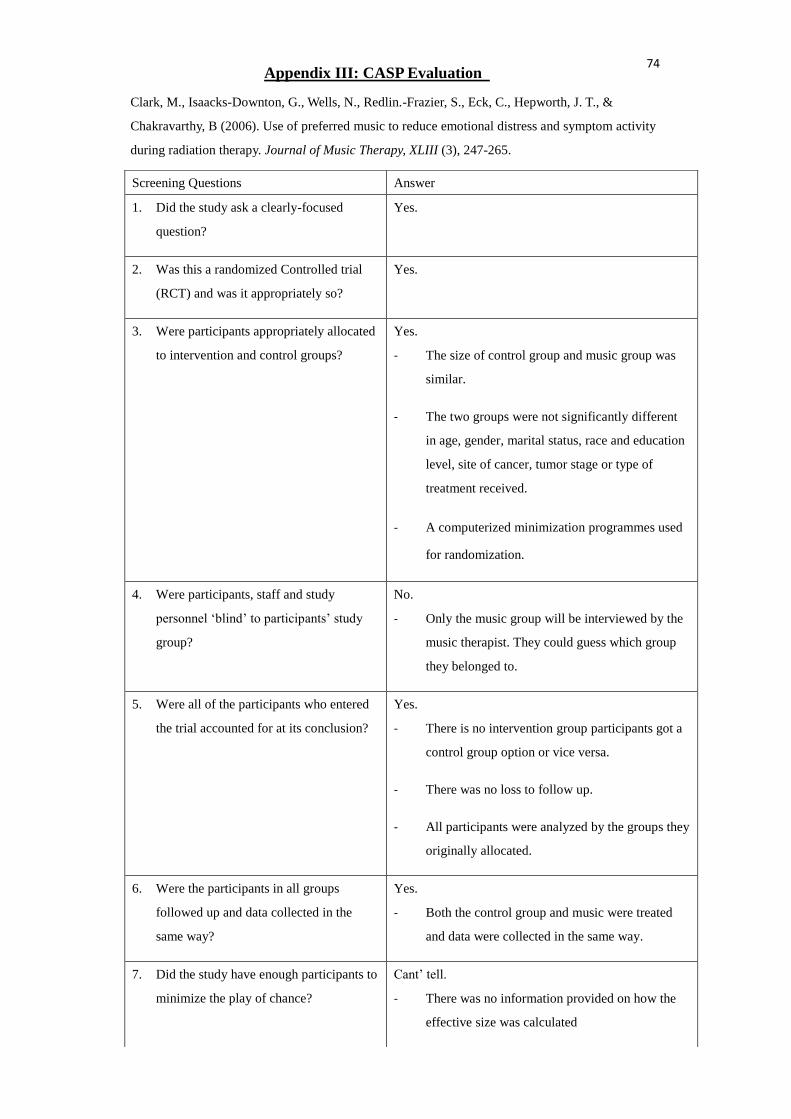
74
Appendix III: CASP Evaluation
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized Controlled trial
(RCT) and was it appropriately so?
Yes.
3. Were participants appropriately allocated
to intervention and control groups?
Yes.
- The size of control group and music group was
similar.
- The two groups were not significantly different
in age, gender, marital status, race and education
level, site of cancer, tumor stage or type of
treatment received.
- A computerized minimization programmes used
for randomization.
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
No.
- Only the music group will be interviewed by the
music therapist. They could guess which group
they belonged to.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
Yes.
- There is no intervention group participants got a
control group option or vice versa.
- There was no loss to follow up.
- All participants were analyzed by the groups they
originally allocated.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to
minimize the play of chance?
Cant’ tell.
- There was no information provided on how the
effective size was calculated
Clark, M., Isaacks-Downton, G., Wells, N., Redlin.-Frazier, S., Eck, C., Hepworth, J. T., &
Chakravarthy, B (2006). Use of preferred music to reduce emotional distress and symptom activity
during radiation therapy. Journal of Music Therapy, XLIII (3), 247-265.

75
8. How are the results presented and what is
the main result?
- The anxiety, depression, distress now, fatigue
and pain now were measured at baseline,
Mid-RT and End of RT.
- Music group had a lower level in distress and
anxiety.
- No significant difference between the music
group and control group in depression, fatigue
and ‘pain now’.
9. How precise are these results? - Only p value was provided. It may not precise
enough to make a decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- It tried to examine the effect of music in anxiety,
depression, distress level, pain and fatigue where
all these dependent variable were important
indicators for cancer patients during RT.
- It was consistent with other study that music
could reduce anxiety and distress level.
- The study had pin pointed the dose effect of
music. In order to optimize the effect of music,
patients are advised to listen to music 5 times per
week.

76
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized controlled trial
(RCT) and was it appropriately so?
No.
3. Were participants appropriately allocated
to intervention and control groups?
Yes.
- There is no significant difference between the
control and music group in pre-test sensation and
distress scores or on employment status, income
or marital status.
- The sample size of control group and music
group was similar.
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
Can’t tell.
- There was no information provided from the test
about blinding.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
Yes.
- There was no intervention group participants got
a control group option or vice versa.
- There was no loss to follow up.
- All participants were analyzed by the groups they
originally allocated.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to
minimize the play of chance?
Yes.
- The effective sample size was calculated at a
power of 80 % at a 5% level of significance.
Appendix III: CASP Evaluation
Good, M., & Abn, S. (2008). Korean and American music reduces pain in Korean women after gynecologic
surgery. Pain Management Nursing, 9(3), 96-103.

77
8. How are the results presented and what is
the main result?
- The results were presented as a measurement of
anxiety and pain level.
- Music group reported 23% less pain than control
group on day1 and 17% on day 2.
9. How precise are these results? - Only p value was reported.
- The result may not be precise enough to make a
decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- The study was similar to my clinical setting.
- Different from other studies, it proposed that fast
pace of music can also provide significant effect
on pain relief.
- Rather, patient’s choice and cultural background
should be considered.
- Music therapy is a non-invasive, inexpensive and
safe intervention for relieving pain and anxiety.
- No matter the individual, nurses and institution
will be beneficial from the intervention.

78
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized controlled trial
(RCT) and was it appropriately so?
Yes.
3. Were participants appropriately allocated
to intervention and control groups?
Yes.
- The sample size of music group and control
group were similar.
- There was no significant difference between the
groups in age, gender, height, weight, martial
status, religion and education level.
- A computerized minimization program and
stratification were used for randomization.
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
No.
- Only participants were blinded from the study.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
Yes.
- There is no intervention group participants got a
control group option or vice versa.
- There was no loss to follow up.
- All participants were analyzed by the groups they
originally allocated.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to
minimize the play of chance?
Yes.
- The effect size was calculated by power analysis.
8. How are the results presented and what is
the main result?
- The pain intensity in music group was mild while
the pain intensity in control group was moderate.
- Music group had less posttest pain than control
group. Music group scored average 1.5 unites
Appendix III: CASP Evaluation
Huang, S.T., Good, M. & Zauszniewski, J.A. (2010). The effectiveness of music in relieving pain in
cancer patients: a randomized controlled trial. International Journal of Nursing Studies, 47, 1354-1362.

79
less sensation of pain than control group
9. How precise are these results? - Both p value and 95% confidence interval were
provided.
- It would be precise enough to make a decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- This study was carried in Taiwan which has
similar culture to Hong Kong.
- The result was generalizable because different
demographic and cancer characteristics were
studied to exclude bias.
- The outcome would be beneficial to patient,
health care professional and policy maker.
- From the patient point of view, music can act as
an alternative method for reducing pain.
- From the health care professional point of view,
music is easy, safe and easy to carry out
- From the policy maker point of view, music is
inexpensive and medical resources can be saved.

80
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized controlled trial
(RCT) and was it appropriately so?
Yes.
3. Were participants appropriately allocated
to intervention and control groups?
No.
- The randomization procedure was not mentioned
here.
- The group size of each group was not very
balanced
- The distraction group has a smaller sample size
than music and control group.
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
No.
- Only participants were blinded to the study.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
No.
- Data from two participants were excluded
because experimental conditions had been
contaminated.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to
minimize the play of chance?
No.
- The effective sample size calculation was not
mentioned here.
- The sample size was quite small in each group
especially in the distraction group.
8. How are the results presented and what is
the main result?
- The pain level was measured before the
procedure, during the procedure and after the
procedure in each of the group while the anxiety
level was measured only before and after the
procedure.
Appendix III: CASP Evaluation
Kwekkeboom, K.L. (2003). Music versus distraction for procedural pain and anxiety in patients with cancer. Online
Nursing Forum, 30 (3), 433-440
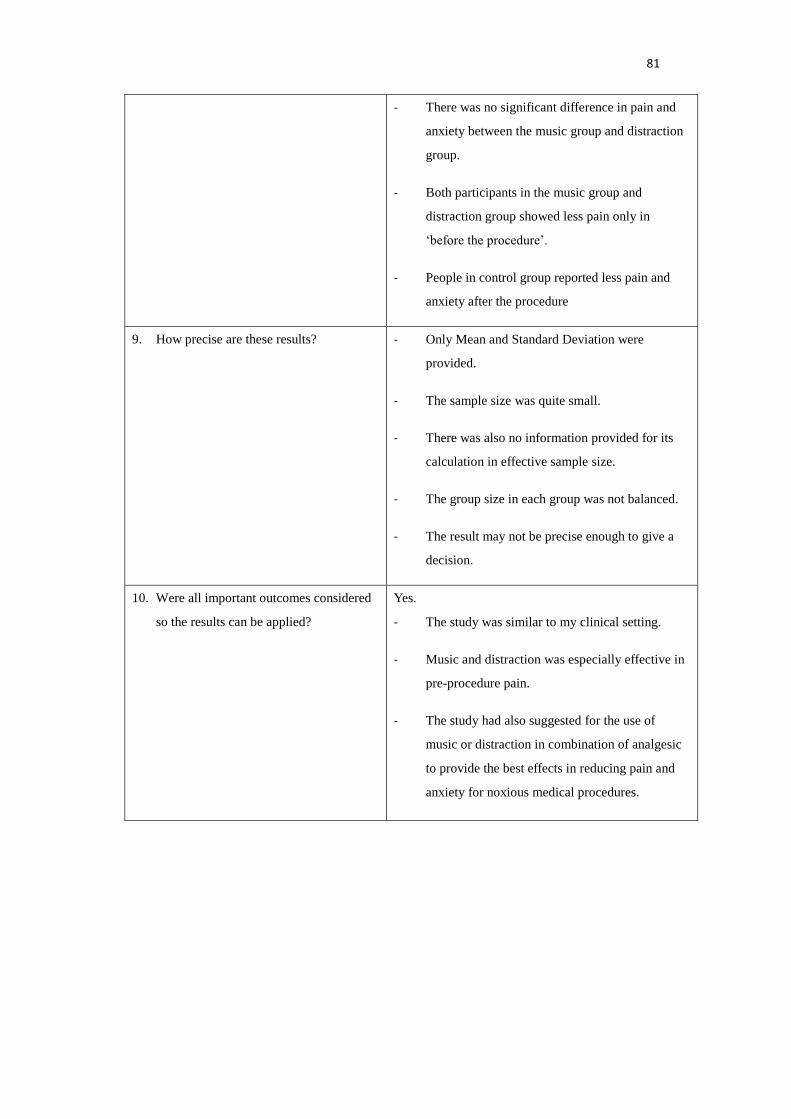
81
- There was no significant difference in pain and
anxiety between the music group and distraction
group.
- Both participants in the music group and
distraction group showed less pain only in
‘before the procedure’.
- People in control group reported less pain and
anxiety after the procedure
9. How precise are these results? - Only Mean and Standard Deviation were
provided.
- The sample size was quite small.
- There was also no information provided for its
calculation in effective sample size.
- The group size in each group was not balanced.
- The result may not be precise enough to give a
decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- The study was similar to my clinical setting.
- Music and distraction was especially effective in
pre-procedure pain.
- The study had also suggested for the use of
music or distraction in combination of analgesic
to provide the best effects in reducing pain and
anxiety for noxious medical procedures.

82
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized controlled trial
(RCT) and was it appropriately so?
Yes.
3. Were participants appropriately allocated
to intervention and control groups?
Yes.
- The randomization was generated by computer
software.
- The music group and control group were well
balanced
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
No.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
No.
- There were 6 patients lost to follow up in the
music group and 9 patient lost to follow up in the
control group.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music group were
reviewed at the same time intervals.
7. Did the study have enough participants to
minimize the play of chance?
Yes.
- The sample size was calculated based on the
change in PRI-total score which needed to recruit
100 patients with 50 in each group.
- The sample size was further augmented to 120
patients to allow drop rate of 20%.
8. How are the results presented and what is
the main result?
- The results are presented as a measurement with
mean and standard deviation provided.
- Music therapy reduces three main pain scores
(PRI-total, VAS and PPI) significantly.
Li, X.M., Yan, H., Zhou, K.N., Dang, S.N., Wang, D.L. & Zhang, Y.P. (2011) Effects of music
therapy on pain among female breast cancer patients after radical mastectomy: results from a
randomized controlled trial. Breast Cancer Res Treat, 128, 411-419.
Appendix III: CASP Evaluation
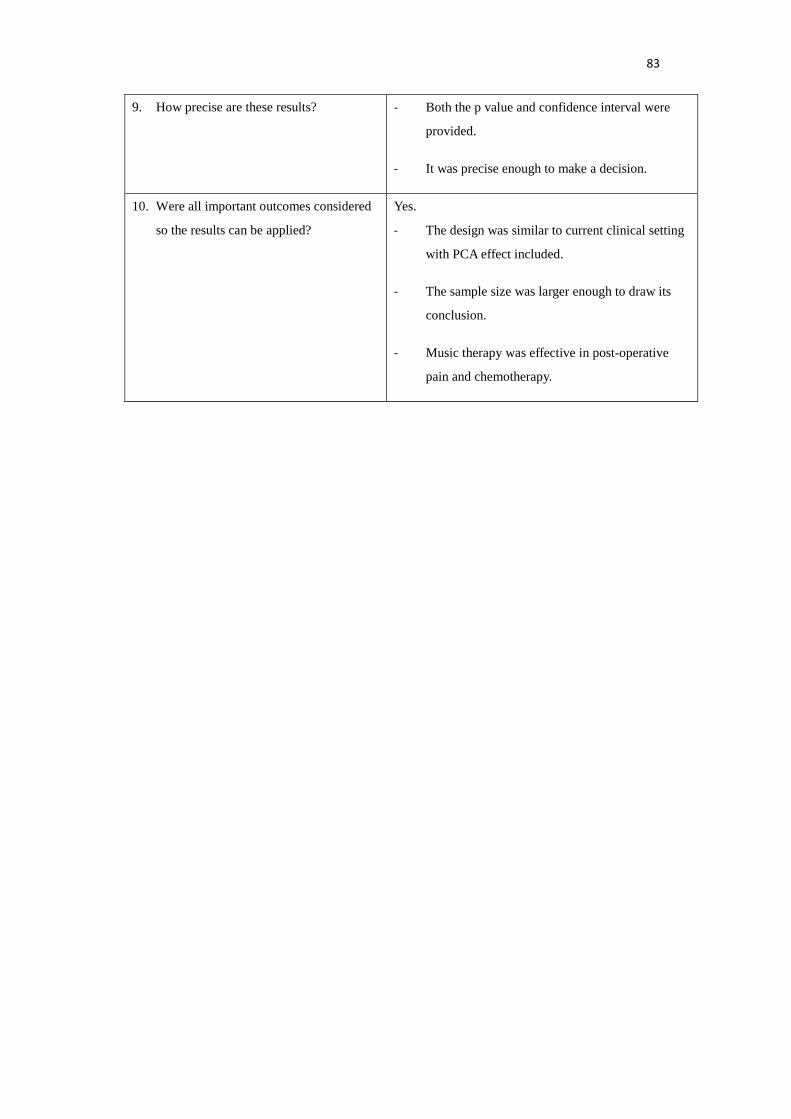
83
9. How precise are these results? - Both the p value and confidence interval were
provided.
- It was precise enough to make a decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- The design was similar to current clinical setting
with PCA effect included.
- The sample size was larger enough to draw its
conclusion.
- Music therapy was effective in post-operative
pain and chemotherapy.

84
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized controlled trial
(RCT) and was it appropriately so?
Yes.
3. Were participants appropriately allocated
to intervention and control groups?
Yes.
- Randomization was done by using a
computer-generated list.
- The control group and intervention groups were
well balanced.
- There is no significant difference between the
control and music group in demographics,
pre-operative anxiety, anaesthetic and surgical
factors.
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
Yes.
- The anaesthetist, nurse anaesthetist, surgeon and
operation room nurses and post-anaesthesia care
unit personal were blinded to the selection.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
Yes.
- There is no intervention group participants got a
control group option or vice versa.
- There is no loss to follow up.
- All participants were analyzed by the groups they
originally allocated.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to Yes.
- The effective sample size was calculated at a
Appendix III: CASP Evaluation
Nilsson, U., Rawal, N. & Unosson, M. A comparison of intra-operative or postoperative exposure
to music –a controlled trial of the effects on postoperative pain. Anaesthesia, 58, 699-703.

85
minimize the play of chance? power of 80 % at a 5% level of significance.
8. How are the results presented and what is
the main result?
- The results are presented as a measurement level
of anxiety, pain, nausea and fatigue.
- Music group participants had a lower level of
pain and anxiety.
9. How precise are these results? - Both p value and 95% confidence interval were
provided.
- It would be precise enough to make a decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- The study was similar to my clinical setting.
- Benefits of music therapy had considered.
- Music was simple, pleasant, inexpensive and has
no side effects.
- Instrumental music with a tempo of 60-80
beats/min provides relaxing effect.
- Music is beneficial to patient both
intra-operatively and postoperatively.
- Music should be combined with analgesic drug
to achieve synergistic effects.

86
Shabanloei, R., Golchin, M., Efanhani, A., Dolatkhan, R., & Rasoulian, M. (2010). Effects of music
therapy on pain and anxiety in patients undergoing bone marrow biopsy and aspiration. Association of
Operating Room Nurse Journal, 91 (6), 746-751.
Screening Questions Answer
1. Did the study ask a clearly-focused
question?
Yes.
2. Was this a randomized controlled trial
(RCT) and was it appropriately so?
No.
3. Were participants appropriately allocated
to intervention and control groups?
Yes.
- There is no significant difference between the
control and music group. -The size of control and
music group is equal.
4. Were participants, staff and study
personnel ‘blind’ to participants’ study
group?
Can’t tell.
- There is no information provided from the test
about blinding.
5. Were all of the participants who entered
the trial accounted for at its conclusion?
Yes.
- There is no intervention group participants got a
control group option or vice versa.
- There is no loss to follow up.
- All participants were analyzed by the groups they
originally allocated.
6. Were the participants in all groups
followed up and data collected in the
same way?
Yes.
- Both the control group and music were treated
and data were collected in the same way.
7. Did the study have enough participants to
minimize the play of chance?
Can’t tell.
- The sample size of each group contained 50
participants.
- However, there was no information how the
sample size collected.
8. How are the results presented and what is
the main result?
- The results are presented as a measurement of
anxiety and pain level.
- Lower level of anxiety and pain intensity were
reported in the music group with p value < 0.05.
Appendix III: CASP Evaluation

87
9. How precise are these results? - Only p value is reported. The result may not be
precise enough to make a decision.
10. Were all important outcomes considered
so the results can be applied?
Yes.
- The study was similar to my clinical setting.
- Music therapy is a non-invasive, inexpensive and
safe intervention for relieving pain and anxiety.
- No matter the individual, nurses and institution
will be beneficial from the intervention.

88
Article Type of Study Number
of Patients
Patient’s characteristics Intervention Comparison Length of
Follow Up
Outcome
Measure
Effect Size
Allred et al.
(2010)
RCT 56 Patient undergoing TKA Music therapy Rest Daily Pain intensity
(VAS +
SFMPQ)
Significant difference in pain
within groups with p= 0.001 and
0.000
Clark et al.
(2006)
RCT 63 Cancer patient undergoing
radiation therapy
Music therapy Rest Weekly Pain intensity
(NRS)
No significant difference
Good & Abn
(2008)
Quasi-
experimental
pretest posttest
73 Women undergoing
Gynecologic Surgery
American music
or Korean music
Rest Daily Pain intensity
(VAS)
Music group experience
significant less pain level p <
0.05
Huang et al.
(2010)
RCT 129 Cancer patients with usual
pain
Music therapy Rest Daily Pain intensity
(NRS +VAS)
Music group experience less
pain with p < 0.001
Appendix IV: Summary Table of the Sampled Studies

89
Kwekkeboom
(2003)
RCT 58 Cancer patient undergoing
invasive medical
procedure
Music therapy or
distraction
therapy
Rest Daily Pain intensity
(NRS +
VAS)
No significant difference
Li et al. (2011)
RCT 120 Female cancer patient
undergoing radical
mastectomy +
chemotherapy
Music therapy Rest Weekly Pain intensity
(VAS +
SFMPQ)
Music group reported less pain
with p < 0.001
Nilsson et al.
(2003)
RCT 151 Patient undergoing day
case surgery
(inguinal hernia repair or
varicose vein surgery)
Music therapy Rest Daily Pain intensity
(NRS)
Music group reported less pain
with p < 0.001
Shabanloei et
al. (2010)
Quasi-
experimental
pretest posttest
100 Patient undergoing bone
marrow biopsy and
aspiration
Music therapy Rest Daily Pain intensity
(NRS +
VAS)
Significant difference in pain
with p = 0.000

90
Article Self Selected
Music from
Repertoire List
Music Provided by
Music Therapist
Type of Music
a. With
b. Without lyrics
Tempo
a. 60 - 80 beats/min
b. 80 - 110 beats/min
Cultural
Background
Duration of Each
Session
Frequency
Allred et al. (2010) √ X b a N/A 20 minutes 2 times/day
Clark et al. (2006)
√ √ N/A N/A N/A Start to finish
except on the 5 min
of radiation therapy
5 times /week
Good & Abn (2008) √ X a + b a + b √ 15 minutes 2 times/day
Huang et al. (2010) √ X b a √ 30 minutes N/A
Kwekkeboom (2003) √ X a+ b N/A N/A 5-15 minutes During procedure
Li et al. (2011) √ X a + b N/A √ 30 minutes 2 times/day
Nilsson et al. (2003) √ X b a N/A 60 minutes 2 times/day
Shabanloei et al. (2010) √ X b a N/A 10-20 minutes During procedure
Appendix V: Recommendation Table of the Sampled Studies

91
Quality Assessment of those 8 Sampled Studies
/Focused questions
Allred et al.
(2010)
Clark et al.
(2006)
Good and Abn
(2008)
Huang et al.
(2010)
Kwekkeboom
(2003)
Li et al.
(2011)
Nilsson et al.
(2003)
Shabanloei
et al. (2010)
Did the study ask a clearly-focused
question?
Yes Yes Yes Yes Yes Yes Yes Yes
Was this a randomized controlled trial
(RCT) and was it appropriately so?
Yes Yes No Yes Yes Yes Yes No
Were participants appropriately allocated to
intervention and control groups?
Yes Yes Yes Yes No Yes Yes Yes
Were participants, staff and study personnel
“blind” to participants’ study group?
Can’t tell No Can’t tell No No No Yes Can’t tell
Were all of the participants who entered the
trial accounted for its conclusion?
Yes Yes Yes Yes No No Yes Yes
Were the participants in all groups followed
up and data collected in the same way?
Yes Yes Yes Yes Yes Yes Yes Yes
Did the study have enough participants to
minimize the play of chance?
Yes Can’t tell Yes Yes No Yes Yes Can’t tell
Were these results precise enough to make a
decision?
No No No Yes No Yes Yes No
Were all important outcomes considered so
the results can be applied?
Yes Yes Yes Yes Yes Yes Yes Yes
Level of evidence 1+ 1+ 2++ 1+ 1- 1+ 1++ 2++
Appendix VI: Quality Assessment Summary of the Sampled Studies
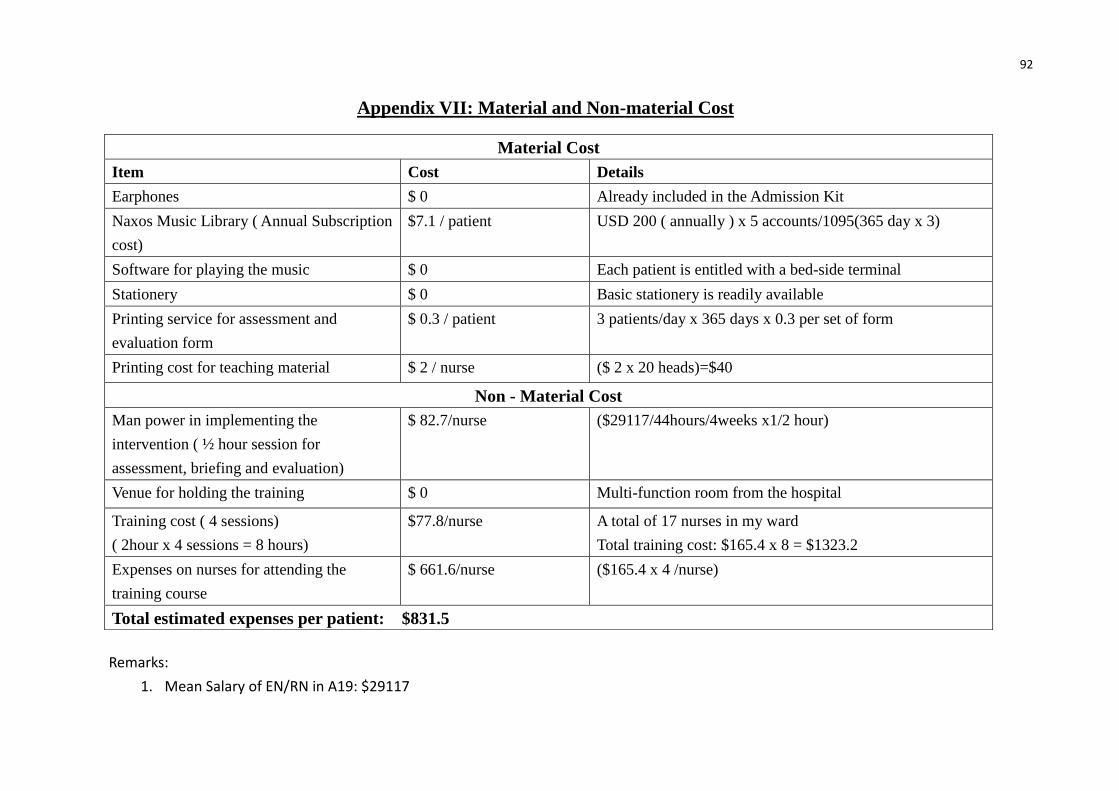
92
Material Cost
Item Cost Details
Earphones $ 0 Already included in the Admission Kit
Naxos Music Library ( Annual Subscription
cost)
$7.1 / patient USD 200 ( annually ) x 5 accounts/1095(365 day x 3)
Software for playing the music $ 0 Each patient is entitled with a bed-side terminal
Stationery $ 0 Basic stationery is readily available
Printing service for assessment and
evaluation form
$ 0.3 / patient 3 patients/day x 365 days x 0.3 per set of form
Printing cost for teaching material $ 2 / nurse ($ 2 x 20 heads)=$40
Non - Material Cost
Man power in implementing the
intervention ( ½ hour session for
assessment, briefing and evaluation)
$ 82.7/nurse ($29117/44hours/4weeks x1/2 hour)
Venue for holding the training $ 0 Multi-function room from the hospital
Training cost ( 4 sessions)
( 2hour x 4 sessions = 8 hours)
$77.8/nurse A total of 17 nurses in my ward
Total training cost: $165.4 x 8 = $1323.2
Expenses on nurses for attending the
training course
$ 661.6/nurse ($165.4 x 4 /nurse)
Total estimated expenses per patient: $831.5
Appendix VII: Material and Non-material Cost
Remarks:
1. Mean Salary of EN/RN in A19: $29117

93
Item Saved money per patient/per day
Decreased expenses on pain medication $78.3
(Panadol extend 1 tab TID)
(Arcoxia 120mgQD)
(Nexium 20mg QD)
Decreased length of stay ( = decreased hospital charges) $1200
Decreased doctors’ fee $1200
Total $2478.3
Appendix VIII: Benefits of Implementing Music Therapy

94
Cost/ per patient Benefit/ per patient
Material Cost = $ 9.4 Decreased hospital charge and doctor’s fee = $ 2400
Non-material Cost = $ 822.1 Decrease expenses on medication = 78.3
$ 831.5 $2478.3
Net gain = Total potential benefits - Total estimated expenses = $2478.3 – $831.5 = $1646.8
Appendix IX: Cost-benefits Ratio for Implementation of Music Therapy
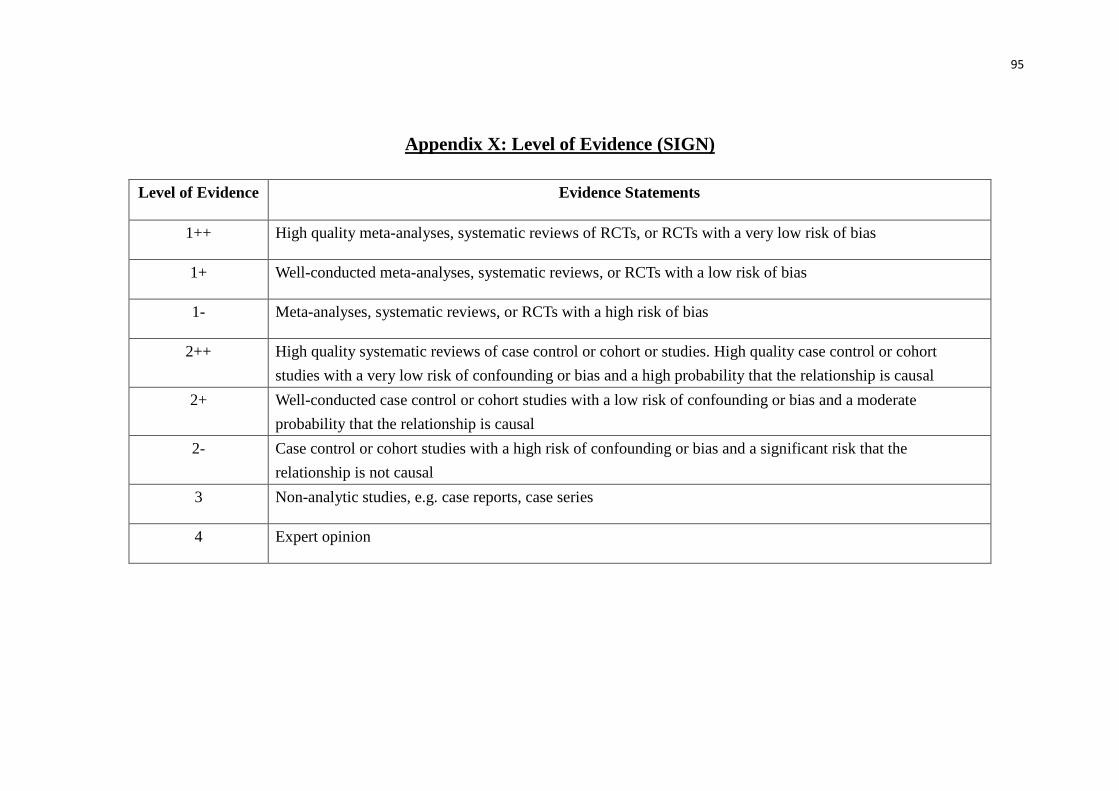
95
Appendix X: Level of Evidence (SIGN)
Level of Evidence Evidence Statements
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies. High quality case control or cohort
studies with a very low risk of confounding or bias and a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a moderate
probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the
relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion

96
Appendix XI: Grade of Recommendation (SIGN)
Grade Statements
A At least one meta-analysis, systematic review of RCTs, or RCT rated as 1++and directly applicable to the target
population; or
A body of evidence consisting principally of studies rated as 1+, directly applicable to the target population,
and demonstrating overall consistency of results
B A body of evidence including studies rated as 2++, directly applicable to the target population, and
demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to the target population and demonstrating
overall consistency of results; or Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
RT Recommended best practice based on the clinical experience of the guideline development group

97
Appendix XII: 音樂治療紀錄表
日期: 時間:
血壓 (由護士或健康服務助理填寫) 治療前: ______________mmHg
治療後: ______________mmHg
痛楚程度:
0 – 10 scale
0 = 完全沒有痛
10 = 最痛
(請在適當方格內加上√)
治療前:
1 2 3 4 5
6 7 8 9 10
治療後:
1 2 3 4 5
6 7 8 9 10
日期: 時間:
血壓 (由護士或健康服務助理填寫) 治療前: ______________mmHg
治療後: ______________mmHg
痛楚程度:
0 – 10 scale
0 = 完全沒有痛
10 = 最痛
(請在適當方格內加上√)
治療前:
1 2 3 4 5
6 7 8 9 10
治療後:
1 2 3 4 5
6 7 8 9 10
日期: 時間:
血壓 (由護士或健康服務助理填寫) 治療前: ______________mmHg
治療後: ______________mmHg
痛楚程度:
0 – 10 scale
0 = 完全沒有痛
10 = 最痛
(請在適當方格內加上√)
治療前:
1 2 3 4 5
6 7 8 9 10
治療後:
1 2 3 4 5
6 7 8 9 10
第一部份

98
Appendix XII: 音樂治療意見調查表
請在適當方格內加上√
1. 你喜歡音樂治療嗎?(1 = 非常不喜歡,5 = 非常喜歡)
1 2 3 4 5
2. 你覺得音樂治療對減低痛楚有療效嗎?(1 = 非常不同意,5 = 非常同意)
1 2 3 4 5
3. 如果將來感到痛楚,你會再次選擇音樂治療嗎?
(1 = 一定不會,5 = 一定會)
1 2 3 4 5
4. 當你接受音樂治療時,有沒有受到周圍環境噪音滋擾?
(1 = 從不,5 = 經常)
1 2 3 4 5
5. 你認為醫院是否一個提供音樂治療的好地方?
(1 = 非常不同意,5 = 非常同意)
1 2 3 4 5
6. 你覺得十五分鐘時間的指引輔導是否足夠?
(1 = 非常不足,5 = 非常足夠)
1 2 3 4 5
7. 你覺得 Naxos Music Library 能否提供足夠的音樂類型讓你選擇?
(1 = 非常不足,5 = 非常足夠)
1 2 3 4 5
8. 你覺得登入 Naxos Music Library 容易嗎?(1 = 非常困難,5 = 非常容易)
1 2 3 4 5
第二部份

99
9. 當你在接受音樂治療期間遇到問題時,你得到足夠的幫助嗎?
(1 = 非常不足,5 = 非常足夠)
1 2 3 4 5
10. 你會將音樂治療介紹給其他人嗎?( 1 = 一定不會,5 = 一定會)
1 2 3 4 5
11. 整體來說,你滿意是次住院的安排嗎?( 1 = 非常不滿,5 = 非常滿意)
1 2 3 4 5
12. 其他意見及建議
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________

100
Appendix XIII: Music Intervention Evaluation Form
Date: Time:
Blood Pressure (To be competed by nurse
or HCA)
Before: ________________mmHg
After: _________________mmHg
Pain Level:
0 – 10 scale
0= no pain at all
10= most pain experienced
(Please √ as appropriate)
Before:
1 2 3 4 5
6 7 8 9 10
After:
1 2 3 4 5
6 7 8 9 10
Date: Time:
Blood Pressure (To be competed by nurse
or HCA)
Before: ________________mmHg
After: _________________mmHg
Pain Level:
0 – 10 scale
0= no pain at all
10= most pain experienced
(Please √ as appropriate)
Before:
1 2 3 4 5
6 7 8 9 10
After:
1 2 3 4 5
6 7 8 9 10
Date: Time:
Blood Pressure (To be competed by nurse
or HCA)
Before: ________________mmHg
After: _________________mmHg
Pain Level:
0 – 10 scale
0= no pain at all
10= most pain experienced
(Please √ as appropriate)
Before:
1 2 3 4 5
6 7 8 9 10
After:
1 2 3 4 5
6 7 8 9 10
Part 1: Pain Level

101
Appendix XIII: Survey on Music Intervention
Please √ as appropriate
1. Did you like Music Intervention? (1 = extremely dislike, 5 = extremely like)
1 2 3 4 5
2. Do you think music intervention is useful in reducing pain?
(1 = totally disagree, 5 = totally agree)
1 2 3 4 5
3. Will you select music intervention again when you experience pain in the
future? (1 = very unlikely, 5 = very likely)
1 2 3 4 5
4. Was there any noise in the surrounding when you were listening to music?
(1= very quiet, 5 = very noisy)
1 2 3 4 5
5. Do you think hospital environment is a good place for music intervention?
(1 = totally disagree, 5 = totally agree)
1 2 3 4 5
6. Do you think the 15-minutes nursing education is enough for preparation and
explanation on the therapy? (1 = totally disagree, 5 = totally agree)
1 2 3 4 5
7. Do you think the Naxos Music Library has provided a good database for
selection of music? (1 = totally disagree, 5 = totally agree)
1 2 3 4 5
8. Do you think it is easy and convenient to access to the Naxos Music Library?
(1 = totally disagree, 5 = totally agree)
1 2 3 4 5
Part 2: Survey

102
9. Do you think there is enough assistance when you are in need?
(1 = totally disagree, 5 = totally agree)
1 2 3 4 5
10. Will you introduce music Intervention to others when you are discharged from
the hospital? (1 = very unlikely, 5 = very likely)
1 2 3 4 5
11. Overall, are you satisfied with the arrangement?
(1 = very dissatisfied, 5= very satisfied)
1 2 3 4 5
12. Other Suggestions and Comments
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________

103
Appendix XIV: Staff Self-evaluation Survey on Music Intervention
Please √ as appropriate: (1 = totally disagree, 5 = totally agree)
1. The innovation is well planned.
1 2 3 4 5
2. Staff training is enough and appropriate.
1 2 3 4 5
3. There is enough assistance and guidance.
1 2 3 4 5
4. The guideline is clear and easy to understand.
1 2 3 4 5
5. The Music Intervention Evaluation Form (part 1) does not take time to
complete.
1 2 3 4 5
6. The Music Intervention has decreased the workload in general.
1 2 3 4 5
7. There is less call bell regarding to pain medication request.
1 2 3 4 5
8. Music intervention is effective in reducing pain for cancer patients.
1 2 3 4 5
9. The client is compliant to the music intervention.
1 2 3 4 5
10. I am willing to give music therapy if the patient is eligible for the intervention.
1 2 3 4 5
11. I am knowledgeable enough about Music Therapy.
1 2 3 4 5
12. I am confident enough to provide Music Therapy for my clients.
1 2 3 4 5

104
13. The innovation should be promoted to other general wards.
1 2 3 4 5
14. The innovation has increased the autonomy for nurses.
1 2 3 4 5
15. The innovation has improved the quality of nursing care.
1 2 3 4 5
16. The innovation can bring reputation to the hospital.
1 2 3 4 5
17. What problems have you encountered during the provision of Music Therapy?
How do you think these problems can be solved?
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
18. Other Comments and Suggestions
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
______________________________________________________________

105
Appendix XV: Quiz on Music Intervention
1. How frequently should music therapy be introduced to patient each day?
A. One time each day
B. Two times each day
C. Three times each day
D. Four times or above
2. How long should each music session take?
A. 5 – 10 minutes
B. 10 – 20 minutes
C. 20 – 30 minutes
D. 30 – 40 minutes
3. Which of the following music tempo is best in providing sedative effect to
patient?
A. 60 – 80 beats per minute
B. 80 – 100 beats per minute
C. 100 – 120 beats per minute
D. 120 – 140 beats per minute
4. What is the name of the music database for selection of Music?
A. Pop Music Library
B. Classical Music Library
C. Naxos Music Library
D. Jazz Music Library

106
Appendix XVI: Doctors’ Perspective Survey on Music Intervention
1. Do you think music intervention is effective for pain control in cancer
patients?
Yes No
2. After reading the booklet, will you introduce music intervention to your
patients?
Yes No
3. Will you reduce the amount of analgesic prescribed in complementary to the
use of music intervention?
Yes No
4. Would you like to receive further information concerning the pilot test result
of the innovation?
Yes No
5. Do you think music intervention can bring benefits to doctors? Why?
Yes No
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
6. Other Suggestions and Comments.
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________

107
Appendix XVII: Eligibility Checklist for Music Intervention
Please √ as appropriate
1. Cancer Patient?
Yes No
2. Aged 18 or above?
Yes No
3. Suffer from acute or chronic pain?
Yes No
4. Any hearing deficit?
Yes No
5. Any cognitive impairment?
Yes No
6. Able to consent?
Yes No
7. Did you give music intervention to the above patient?
Yes No
Responsible Nurse and Post _____________________
Signature: _______________ Date: _______________
GUM LABEL
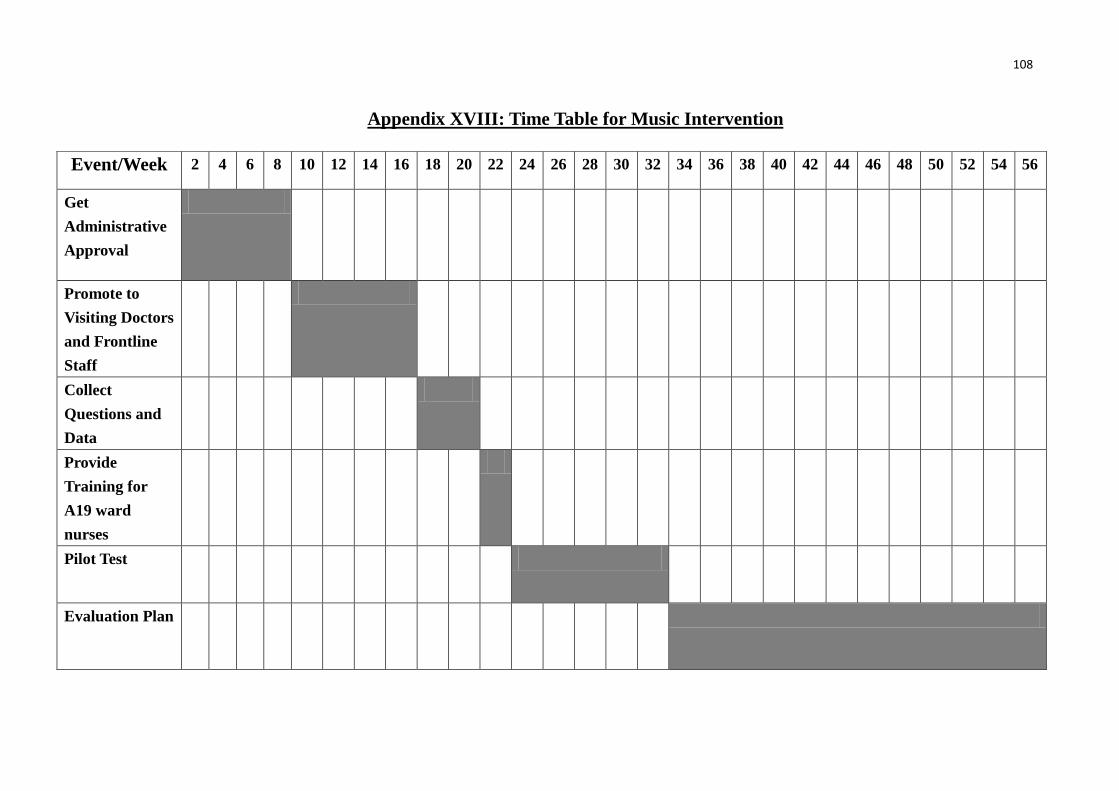
108
Event/Week 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56
Get
Administrative
Approval
Promote to
Visiting Doctors
and Frontline
Staff
Collect
Questions and
Data
Provide
Training for
A19 ward
nurses
Pilot Test
Evaluation Plan
Appendix XVIII: Time Table for Music Intervention

109
References
Allred, K.D., Byer. J.F. & Sole, M. L. (2010). The effect of music on postoperative
pain and anxiety. Pain Management Nursing, 11 (1), 15-25.
Bardia, A., Barton, D.L., Prokop. L.J., Bauer, B.A. & Moynihan, T.J. (2006). Efficacy
of complementary and alternative medicine therapies in relieving cancer pain: A
Systematic Review. Journal of Clinical Oncology, 24 (34), 5457-5464.
Burns, N., & Grove, S. K. (2005). The practice of nursing research: Conduct, critique,
and utilization. St. Louis, Mo: Elsevier/Saunders.
Catane, R., Cherny, N. I., Kloke, M., Tanneberger, S., Schrijvers, D., & European
Society for Medical Oncology. (2006). Handbook of advanced cancer care.
London: Taylor & Francis.
Clark, M., Isaacks-Downton, G., Wells, N., Redlin.-Frazier, S., Eck, C., Hepworth, J.
T., & Chakravarthy, B. (2006). Use of preferred music to reduce emotional
distress and symptom activity during radiation therapy. Journal of Music
Therapy, XLIII (3), 247-265.
Good, M., & Abn, S. (2008). Korean and American music reduces pain in Korean
women after gynecologic surgery. Pain Management Nursing, 9(3), 96-103.
Hong Kong Cancer Registry. Leading Cancer sites in Hong Kong in 2008. Retrieved
August 19, 2011, from http://www3.ha.org.hk/cancereg/e_stat.asp

110
Huang, S.T., Good, M. & Zauszniewski, J.A. (2010). The effectiveness of music in
relieving pain in cancer patients: a randomized controlled trial. International
Journal of Nursing Studies, 47, 1354-1362.
Kwekkeboom, K.L. (2008). Oncology nurses’ use of nondrug pain interventions in
practice. Journal of Pain and Symptom Management, 35(1), 83-94.
Kwekkeboom, K.L. (2003). Music versus distraction for procedural pain and anxiety
in patients with cancer. Online Nursing Forum, 30 (3), 433-440.
Li, X.M., Yan, H., Zhou, K.N., Dang, S.N., Wang, D.L. & Zhang, Y.P. (2011) Effects
of music therapy on pain among female breast cancer patients after radical
mastectomy: results from a randomized controlled trial. Breast Cancer Res
Treat, 128, 411-419
Magill, L. (2009). The spiritual meaning of pre-loss music therapy to bereaved
caregivers of advanced cancer patients. Palliative and Supportive Care, 7,
97-118.
Magill, L. (2008). The conjoint use of music therapy and reflexology with
hospitalized advanced stage cancer patients and their families. Palliative and
Supportive Care, 6, 289-296.

111
Margoles, M. S. & Weiner, R. (2010). Chronic pain. assessment, diagnosis and
management. CRC Press. Florida.
Nguyen, T.N., Nilsson, S., Hellstrom, A. & Bengtson, A. (2010). Music therapy to
reduce pain and anxiety in children with cancer undergoing lumbar
puncture: A randomized clinical trial. Journal of Pediatric Oncology Nursing,
27(3), 146-155.
Nilsson, U., Rawal, N. & Unosson, M. A comparison of intra-operative or
postoperative exposure to music – a controlled trial of the effects on
postoperative pain. Anaesthesia, 58, 699-703.
Pawuk, L.G. & Schumacher, J.E. (2010). Introducing music therapy in hospice and
palliative care: An overview of one hospice’s experience. Home Health Care
Nurse, 28(1), 37-44.
SIGN. 2009. Evidence table for intervention studies. Retrieved Apr 30, 2009 from
http://www.sign.ac.uk/guidelines/fulltext/50/compevidence.html
Shabanloei, R., Golchin, M., Efanhani, A., Dolatkhan, R., & Rasoulian, M. (2010).
Effects of music therapy on pain and anxiety in patients undergoing bone
marrow biopsy and aspiration. Association of Operating Room Nurse Journal,
91 (6), 746-751.

112
Skyes, N., Fallon, M.T. & Patt, R.B. (2003). Clinical pain management. Oxford
University Press. United state of America.