american academy of osteopathy 2018 convocation program diagnostic...
TRANSCRIPT

AMERICAN ACADEMY OF OSTEOPATHY
2018 CONVOCATION PROGRAM
DIAGNOSTIC TOUCH AND THE CENTRAL FIELD
ANTHONY G. CHILA, DO, FAAO DIST, FCA, DP/ FELLOW, NAP (OST. MED.)
DALLAS, TX MARCH 22, 2018
ANTHONY G. CHILA 7948 ROLLING HILLS DRIVE
ATHENS, OH 45701-3525 USA
COPYRIGHT © 2017 ANTHONY G. CHILA
PROGRAM
As specified by the 2018 Convocation program chair (David R. Boesler, DO), this program will present an offering of two (2) Mentors who were influential in
facilitating the development of my osteopathic thought and practice.
To begin, let us review some fundamental definitions:
• Mentor: A close, trusted and experienced counselor or guide who, because (s)he is detached and disinterested, can hold up a mirror to us. (After Mentor, tutor of Telemachus in the Odyssey of Homer).
• Legacy: Something coming from the past (as from an age, event, or policy).
With the foundation provided by these definitions, let us consider the mentors I
have chosen. In doing so, let us also keep in mind that Mentor(s) offer guidance for further development of thought. A significant component of the mentoring
process is the obligation of the student to inquire, absorb, synthesize and offer ongoing development/expansion of thought. This is the dynamic which gives meaning to the role of the mentor(s) and contributes to the perpetuation of
legacy.

A TRIBUTE TO TWO BROTHERS
Alan R. Becker and Rollin E. Becker
Osteopathic Physicians whose fidelity to the osteopathic medical profession, its theory, methods and practice remains unchallenged and continues to nourish subsequent generations of aspirants. Through their father, Arthur D. Becker,
they were privileged to share and continue a lineage that extended from Andrew Taylor Still and William Garner Sutherland.
Alan R. Becker (1913-2000): Des Moines Still College, 1937
President, American Academy of Osteopathy; 1982-1983
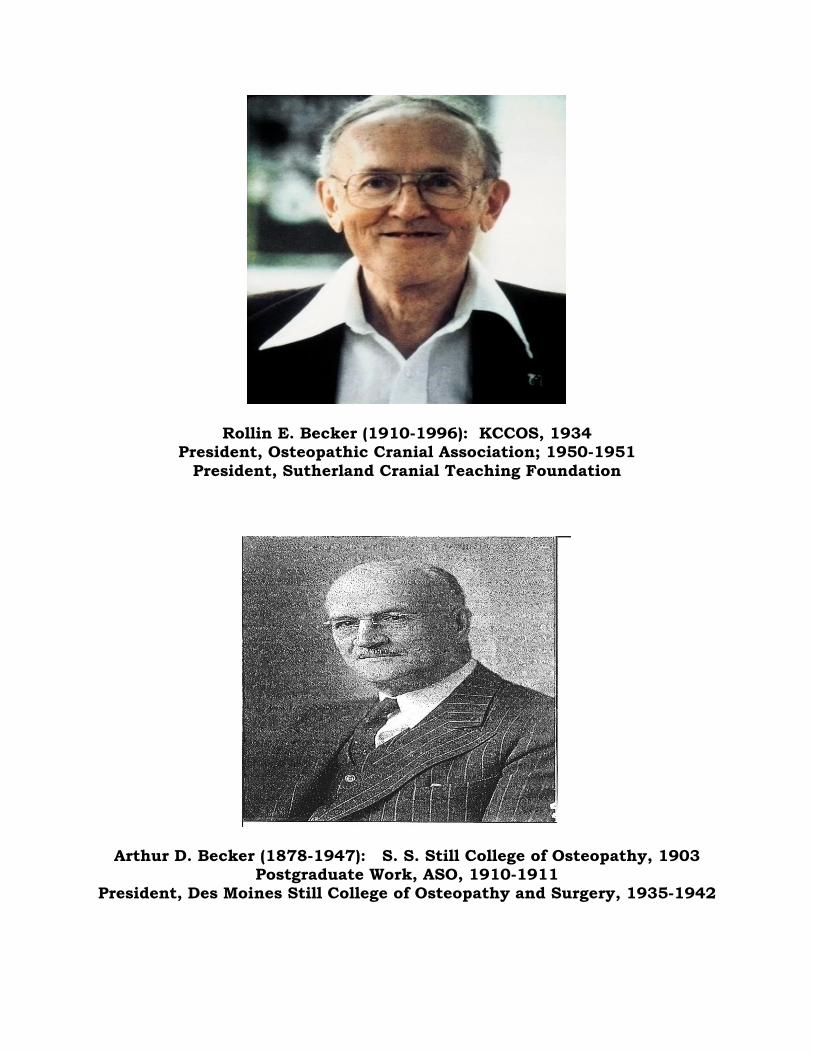
Rollin E. Becker (1910-1996): KCCOS, 1934 President, Osteopathic Cranial Association; 1950-1951
President, Sutherland Cranial Teaching Foundation
Arthur D. Becker (1878-1947): S. S. Still College of Osteopathy, 1903 Postgraduate Work, ASO, 1910-1911
President, Des Moines Still College of Osteopathy and Surgery, 1935-1942
FURTHER THOUGHTS ABOUT MENTORING
Many of us have the tendency to think in terms of “My Mentor”, often stated in the singular mode. There is also another mode about “Mentoring” which has a
much broader impact. To begin this thought, it is helpful to recognize that one’s life is an ongoing
encounter with various experiences. All experiences of any kind contribute to the formation of the whole, unique individual who is impacted more by certain experiences and, in turn, contributes to the formation of other unique
individuals.
“When the student is ready, the teacher appears”
So it was for me in my encounters with Doctors Alan and Rollin Becker. My
encounter with Dr. Alan Becker began in 1975, and with Dr. Rollin Becker in 1978. Over a number of years and under different circumstances, each had a
specific influence on my thought which shaped the modes of my practice and teaching. For that I am grateful.
“I felt that I must anchor my boat to living truths and follow them wheresoever they might drift” Andrew T. Still: Philosophy of Osteopathy (1899); p. 24
My first meeting with Dr. Alan Becker occurred in 1975, at the time of the AOA National Conference at San Francisco, CA. We were introduced by a mutual
friend, and Dr. Alan’s very firm handshake and intensive eye contact were the beginning of an ongoing friendship. Several years later, he contributed a key piece of knowledge to the shaping of my practice. My first meeting with Dr. Rollin
Becker occurred during the Cranial Academy Conference of 1978 at Michigan State University. I was a presenter on that program, and after completing my
discussion, he kindly said to me “You see it”. In essence, then, both brothers provided complementary perspectives which emphasized visualization as a major component of osteopathic theory, methods and practice. Subsequently, this led
to the development of my personal five-points paradigm for diagnosis and treatment.
Dr. Rollin Becker is most prominently remembered for his discussion of “Three Problems” and the use of diagnostic touch through a fulcrum. This, in turn,
leads to his observation that there are no techniques, in the ordinary sense of teaching and practice. Dr. Alan Becker cemented this thought for me with his comment that it was also necessary to enter the central field in order to fully
realize the potency of the wisdom of the patient’s body. It should also be noted that Dr. Alan was first to encounter the teaching of William G. Sutherland and
to then encourage Dr. Rollin to avail himself of that experience. The rest is osteopathic history.

DIAGNOSTIC TOUCH (ROLLIN E. BECKER)
“At all times, the patient and his problem presents a challenge to the physician.
In this work of using a diagnostic touch, the patient is the taskmaster. His problem is the schoolroom. His biodynamic intrinsic forces and their unerring potency are the teachers. The diagnostic touch of the physician, operating
through a fulcrum point for each hand contact, is the pupil. Diagnostic touch involves learning to feel and understand the biodynamic intrinsic forces and learning to be aware of the unerring potency within them.”
ACADEMY OF APPLIED OSTEOPATHY 1964 YEARBOOK, p. 161
THE CENTRAL FIELD (ALAN R. BECKER)
“Only when entering the central field is the physician able to appreciate the
potential of the patient in the process of healing.”
PERSONAL COMMENT BY DR. ALAN R. BECKER WHEN ADMINISTERING AN OSTEOPATHIC TREATMENT TO ME DURING AN AAO CONVOCATION PROGRAM, circa 1984
PARADIGM FOR PRACTICE AND TEACHING (ANTHONY G. CHILA)
The described comments and encounters with the Doctors Rollin E. and Alan R.
Becker helped guide, define and shape my approach to patient care through osteopathic theory, methods and practice. The five points which emerged became stated as (circa 1986):
• LOOK; SEE; PERCEIVE. (Observation and Assessment of the patient).
• LISTEN; HEAR; UNDERSTAND. (History acquired from the patient).
• REMOVE; YOUR; SELF. (Acknowledge the wisdom of the body).
• FACILITATE; OBSERVE; AWARE. (Recognize biodynamic intrinsic forces).
• SEE; NO; THING. (Allow and accept patient’s expression of self-healing). Further:
The history is not the history until it is the history. The use of manipulative interventions is best understood as the physician’s use of methods engaging resistance (to the tolerance of the patient) or compliance (to the tolerance of the patient). It is the patient who exercises the option to respond completely, partially, or not at all. The patient is the focal point for any/all manual interventions which are, in fact, true representations of osteopathic manipulation.

INITIATING THE ENCOUNTER
Every patient is a new patient, no matter whether the professional encounter is the first or one of several over a course of osteopathic management. For this reason, I have chosen to phrase questions as follows: INITIAL VISIT: What brings you to see me today? How can I be of assistance to you? As general discussion and answers to questions emerge, I prefer to devote a great deal of time to visual assessment of the cranium. A format suggested by Dr. Harold I. Magoun, Sr. is quite helpful:
SUGGESTIVE DIAGNOSTIC FINDINGS
A. Face 1. Frontal: Supranasal vertical folds augmented by scowling
2. Orbits: Alteration of superomedial-inferolateral diameter;
Prominence of eyeball 3. Zygomae: Eversion of orbital rim
4. Maxillae: Asymmetry of Nasolabial crease
5. Nose: Deviation of bridge and septum; Maxillae
6. Mouth: Upper jaw: Maxillae Lower jaw: Temporals
Once treatment is engaged and completed for the initial encounter, discussion, explanation and preparation for a second visit are completed. I utilize a single, basic question for initiation of any subsequent encounter: SECOND VISIT: How are you today?

WORKSHOP FORMAT
(Anthony G. Chila)
The format which we will use during this Workshop Session is based on, and derived from, methods of teaching and practice which I have utilized throughout my professional practice and academic careers. Conventional approaches and terminology are most useful in establishing relevance to current osteopathic medical thought and teaching in osteopathic methods and practice. For these reasons, we will make use of three patient body positions:
STANDING SEATED SUPINE
In beginning these exercises, we will vigorously emphasize:
MOTION TESTING, RANGE OF MOTION, JOINT PLAY, END RANGE ARE NOT UTILIZED IN THIS WORKSHOP! WE WILL FOCUS OUR SKILLS SO AS TO:
• BE WITH OR SLIGHTLY BEHIND THE DEMAND FOR MOTION
• MODIFY AND/OR SHIFT OUR FULCRUM TO ACCOMMODATE THE BODY’S EXPRESSIONS
• BE AWARE OF AND REALIZE THE ENTRY TO SILENCE WHICH SIGNALS THE NEXT STAGE(S) OF HEALING
We will also keep in mind that osteopathic manipulative methods, as taught, are not units of exclusivity. Rather, through these methods, we are given the privilege of being spectators at a panoramic exhibition of the body’s wisdom being unrolled a part at a time. All methods are anchored in the fascial system of the body.

STANDING: LOOK SEE PERCEIVE LISTEN HEAR UNDERSTAND REMOVE YOUR SELF
A. Position of feet on floor
B. Curve/Direction of lower extremity compartments
C. Pelvic translation
D. Spinal curve: Lumbar/Thoracic/Cervical
E. Costal cage/Sternal deviation
F. Scapular levels
G. Shoulder levels
H. Curve/Direction of upper extremity compartments
I. Head
EFFECT(S) OF CLOTHING ON BODY FORM, FUNCTION, MOTION
DEMAND
HAND POSITIONS FOR ASSESSMENT
Anterior Patella Scapula
Lateral Tibiofibula Cervicothoracic Juncti on
Iliac Crest; ASIS/PSIS Shoulder/Upper Extremity
Thoracolumbar Junction Cranium

SEATED: LOOK SEE PERCEIVE LISTEN HEAR UNDERSTAND REMOVE YOUR SELF
A. Curve/Direction of lower extremity compartments
B. Pelvic translation
C. Spinal curve: Lumbar/Thoracic/Cervical
D. Costal cage/Sternal deviation
E. Scapular levels
F. Shoulder levels
G. Curve/Direction of upper extremity compartments
H. Thoracic stabilization by alternate crossing of upper
Extremities
Head
EFFECT(S) OF CLOTHING ON BODY FORM, FUNCTION, MOTION
DEMAND
HAND POSITIONS FOR ASSESSMENT
Patellofemoral Compression Scapula
Tibiofibular Torque Cervicothoracic Junction
Iliac Crest; ASIS/PSIS Shoulder/Upper Extremity
Thoracolumbar Junction Cranium
SUPINE: LOOK SEE PERCEIVE LISTEN HEAR UNDERSTAND REMOVE YOUR SELF A. Observation of respiratory pattern (J. Gordon Zink)
Respiratory Effort/Effectiveness
Type Motion of the abdominal wall
Rate Duration of cycle
Sternal/diaphragm deviation
Arching/Flattening of Lumbar spine Angles of Upper and Lower extremities
Edematous change
Supraclavicular Posterior and Anterior axillary folds Midline of abdomen
Intercostal Breast
Inguinal node (Left)
EFFECT(S) OF CLOTHING ON BODY FORM, FUNCTION,
MOTION DEMAND
HAND POSITIONS FOR ASSESSMENT
General Vault Hold
Fronto-Occipital Hold
Study of transfer(s) of force throughout the entirety of the body

INITIATION AND CONDUCT OF TREATMENT
The greatest challenge to treatment rests with the expectation that the osteopathic physician is/can be/ will indeed seek to be always attentive to the
wisdom of the body’s participation in the treatment. Hence, “The Three Problems” presented in the clinical circumstance:
• The patient’s belief(s)
• The physician’s concept(s)
• The body’s wisdom In any encounter then, or through successive encounters, patient and physician must each reconcile their viewpoints to the body’s wisdom.
Only when the physician addresses and begins to master the discipline of such practice will the expansion of healing potential express itself through the body’s
wisdom. Such encounter is not at all “technique” in the ordinary sense of teaching and practice.
My general preference is to emphasize/utilize movements toward compliance in seeking resolution of dysfunction. This does not mean, however, that
movements toward resistance are completely ignored. Tissue analysis is multifactorial throughout a clinical encounter: This is what enhances the
physician’s awareness of the body’s expression of wisdom.
FACILITATE OBSERVE AWARE
With the gradual modification and resolution of dysfunctional manifestation, it becomes apparent to the physician that the body’s expression is entering a
period of silence. This is not the time for the physician to demonstrate incompetence by assuming a privilege of overriding the silence being
expressed in the central field. This is the time for sharing mutual love.
SEE NO THING
As the patient is able to absorb and realize the cleansing effect(s) of the clinical
encounter, the physician is enabled to prepare for and offer further guidance in the healing process.
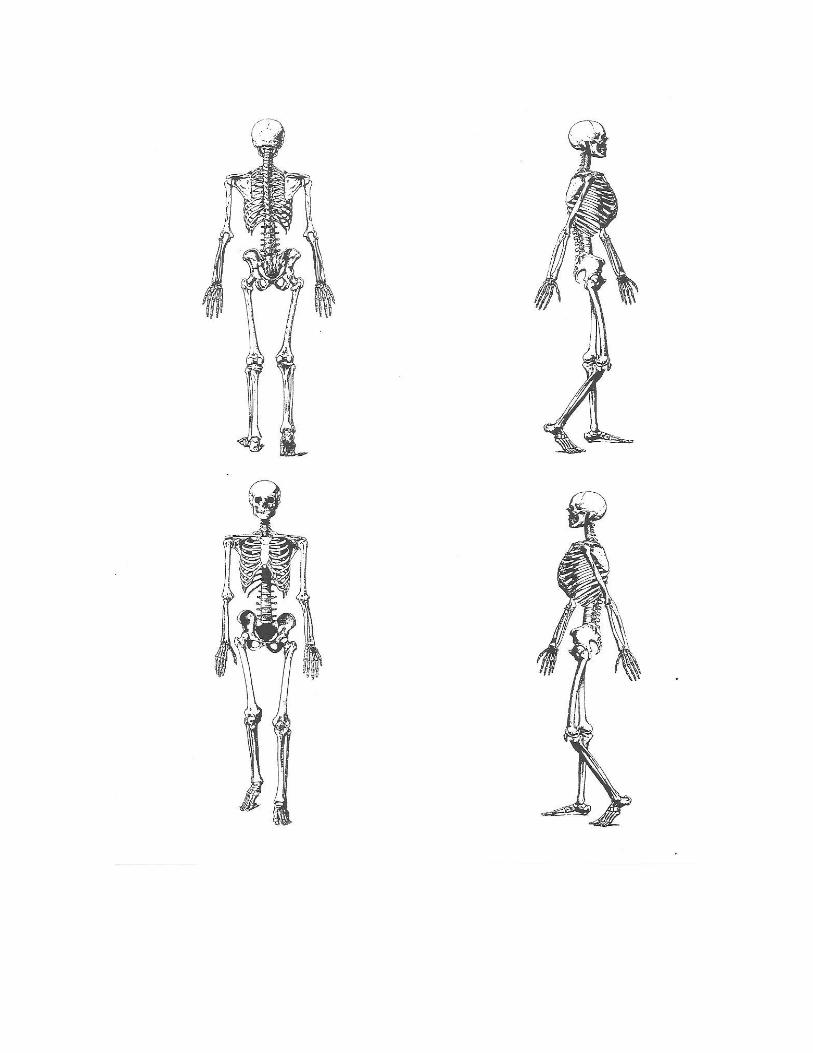
RECORDING AND DOCUMENTING FINDINGS
The next (final) page of this document may be reproduced and utilized in your office, should you wish to do so.
The graphic arrangement of skeleton figures was done for me, at my request, by members of the Graphics Department at then Ohio University College of
Osteopathic Medicine. Graphic arrangement and transposition of skeletal figures from an anatomy textbook (Lockhart, Hamilton, Fyfe: Anatomy of the Human Body ; J.B. Lippincott Company (USA), 1959. This resulted in scaling
and placement of figures so as to represent posterior, right lateral, left lateral and anterior skeletal views.
For many years, during my affiliation with OUCOM/HCOM, I utilized this page for marking (colored pens), comment, acknowledgment of existing, old, new
diagnoses, etc. I found that by developing my own system of coding and description, I could accomplish a significant amount of clinical work on this
sheet, and then transfer to subsequent computer iterations. I learned further that practicing in this manner made it possible to prepare a narrative patient encounter which was also amenable to inclusion of various coding terminologies.