ambulance service conveyance policy - … service conveyance... · ambulance service conveyance...
TRANSCRIPT

Ambulance Service Conveyance Policy Page 1 of 48 Version 8
AMBULANCE SERVICE CONVEYANCE POLICY
Document Author Authorised Signature
Written By: Dana Whawell
Signed:
Date: 4 December 2013
Authorised By: Karen Baker
Signed: Date: 18 February 2014
Job Title: Patient Transport Services / Hospital Liaison Manager
Job Title: Chief Executive
Lead Director: Executive Medical Director
Effective Date: 18 February 2014
Review Date: 17 February 2017 Extension: 17 April 2017 Extension: 17 July 2017 Extension: 17 September 2017 Extension: 17 December 2017 Extension: 17 January 2018 Extension: 17 February 2018 Extension: 17 April 2018 Extension: 17 May 2018 Extension: 17 June 2018
Approval at: Policy Management Group Extensions to review date approved at: Corporate Governance & Risk Sub-Committee Extensions to review date approved at: Policy Management Sub-Committee
Date Approved: 18 February 2014 Extension Approved:14th February 2017 Extension Approved: 14th March 2017 Extension Approved: 11th July 2017 Extension Approved: 12th Sep 2017 Extension Approved: 12th Dec 2017 Extension Approved: 9th January 2018 Extension Approved: 13th February 2018 Extension Approved: 10th April 2018 Extension Approved: 8th May 2018

Ambulance Service Conveyance Policy Page 2 of 48 Version 8
NB This policy relates to the Isle of Wight NHS Trust hereafter referred to as the Trust
DOCUMENT HISTORY (Procedural document version numbering convention will follow the following format. Whole numbers for approved versions, e.g. 1.0, 2.0, 3.0 etc. With decimals being used to represent the current working draft version, e.g. 1.1, 1.2, 1.3, 1.4 etc. For example, when writing a procedural document for the first time – the initial draft will be version 0.1)
Date of Issue
Version No.
Date Approved
Director Responsible for Change
Nature of Change
Feb 03 1 D. Arnold Mainland Transfer Policy
Apr 08 1.1 S.Carter R.Andrews N.Puckett
Superseded ‘Mainland Transfer Policy’
Feb 09 2 S.Carter R.Andrews N.Puckett
Reviewed at Integrated Governance Committee
Mar 09 2 S.Carter R.Andrews N.Puckett
Approved at Integrated Governance Committee Chairman’s Action after amendments made following February’s meeting
Jun 11 3 D.Whawell
24 Aug 11 4 24 Aug 11 D.Whawell
18 Oct 11 5.1 D.Whawell
28 Nov 12 5.1 28 Nov 12 Amended to reflect NHSLA standards
5.1 Ratified at Ambulance Senior Management Group
14 Dec 12 5.1 Ratified at Policy Management Group
17 Dec 12 6.0 17 Dec 12 Approved at Executive Board
Dec 13 7.0 Executive Medical Director Policy Reviewed
07 Feb 14 7.0 Executive Medical Director Ratified at Clinical Standards Group
18 Feb 14 8 Executive Medical Director Approved at Policy Management Group
14 Feb 17 8 Executive Medical Director Extension for 1 month approved at Corporate Governance & Risk Sub-Committee
14 Mar 17 8 Executive Medical Director Extension for 3 months approved at Corporate Governance & Risk Sub-Committee
11 July 17 8 Executive Medical Director Extension to review date for a further 2 months approved at Corporate Governance & Risk Sub-Committee
12 Sep 17 8 Executive Medical Director Extension to review date for a further 3 months approved at Corporate Governance & Risk Sub-Committee
12 Dec 18 8 Executive Medical Director Extension to review date for a further 1 month approved at Corporate Governance & Risk Sub-Committee
09 Jan 18 8 Executive Medical Director Extension to review date for a further 1 month approved at Policy Management Group
13 Feb 18 8 Executive Medical Director Extension to review date for a further 2 months approved at Policy Management Sub-Committee
10 April 18 8 Executive Medical Director Extension to review date for a further month approved at Policy Management Sub-Committee
9 May 18 8 Executive Medical Director Extension to review date for a further month approved at Policy Management Sub-Committee

Ambulance Service Conveyance Policy Page 3 of 48 Version 8
Contents Page 1. Executive Summary 5 2. Introduction 6-7 3. Scope 7 4. Purpose 7 5. Roles and Responsibilities 7-9 6. Policy detail / course of action 9-20 7. Consultation 20 8. Training 21 9. Dissemination Process 21
10. Equality Analysis 21
11. Review and Revision arrangements 22 12. Monitoring Compliance and Effectiveness 22
13. Links to Other Organisation Policies/Documents 22 14. References 22
15. Disclaimer 22 16. Acronyms 23
Appendices:
A. Key definitions for documentation 24
B. Checklist for the development and approval of controlled 25-26 Documentation C Impact assessment forms on policy implementation 27-29 (including checklist) D Mainland Transfer Flow chart 30 E Island Operational Minimum Cover 31 F Integrated Care Hub Contact details 32 G Tariff of Charges 33 H Ambulance Transport booking process and forms 34

Ambulance Service Conveyance Policy Page 4 of 48 Version 8
I Ambulance Transport Request Form 35 J Hospital Car Service Transport Request Form 36 K Ambulance Service Transport Flow Chart 37 L Mainland Transfer Triage Tool 38 M Guidance for the Transfer of Children to other Hospitals 39-41 N Transportation of Short Notice Urgent Transfer Patients 42-44 By the Hampshire and Isle of Wight Air Ambulance O Equality analysis and action plan 45-48
Ambulance Service Conveyance Policy Page 5 of 48 Version 8
1. EXECUTIVE SUMMARY The overall aim of this document is to reduce clinical risk and increase patient safety by conveying patients when required to the most appropriate healthcare facility by the most appropriate means, with the most appropriate skill mix, and within the most appropriate timeframe. The document Taking healthcare to the patient: Transforming NHS ambulance services (DH 2005) sets out the increasing expectations facing the ambulance service. These ongoing changes highlight the need for ambulance services to utilise their skills and resources to the best effect. This policy sets out expectations for service delivery in the conveyance of patients by the Ambulance Service and the expectations of the organisation on how departments/clinicians utilize this service, in particular the management of resources and costs of mainland transfers. This policy is intended to be an overarching policy which directs all members of staff to more detailed policies/procedures. It should therefore be read in conjunction with all of the appropriate policies/procedures listed

Ambulance Service Conveyance Policy Page 6 of 48 Version 8
2. INTRODUCTION The Isle of Wight is a large Island (147 Sq Miles) off the South Coast of England bordered by the English Channel to the South and the Solent to the north. The permanent population is around 140000 people and increasing, the mean age of Island residents is significantly higher than that of mainland counties. The population during certain events significantly increases in the summer. It is a non metropolitan, ceremonial county in its own right and has no fixed link to the mainland. Instead ferries dock in 3 ports around the north of the Island and link with Lymington, Southampton or Portsmouth. The ferry journey varies in time by route and can be in excess of one hour in duration, not including the journey times to and from the port. The Isle of Wight NHS is a unique organisation which combines a full and diverse healthcare system under one auspice. The organisation is responsible for this population’s healthcare. It provides a number of services that are dependant upon an integrated approach amongst its directorates. The NHS IOW base is at St Mary’s Hospital, which is the only District General Hospital on the Island. It comprises an Accident and Emergency (A&E) department and other specialist centres such as Coronary Care, Intensive Care, Maternity, Mental Health and Children’s wards amongst its departments. As such it is the hub of conveyance. Patients are often transported to and from this hub. Although the largest healthcare facility on the Isle of Wight it is not the only one patients are required to be conveyed to or from. Patients should receive their treatment in an appropriate location and not be unnecessarily moved between NHS organisations. Staff will therefore use procedures to identify the best location for a patient’s specific need and convey them to that location at any time of the day or night. The organisation is limited by need, risk and cost to some services and treatments. These Services and treatments are often specialist in nature which results in some patients being transferred off the Island and to alternative healthcare providers on the Mainland. These patients’ conditions can vary too, from routine outpatients, to emergency transfers to specialist units. Often Ambulance transport will be the primary option in the transferring of these patients – other options include patients own transport, hospital car service, Hampshire and Isle of Wight Air Ambulance (HIOWAA) or HM Coastguard Helicopter. The Isle of Wight Ambulance Service provides 24 hour emergency care to the 140000 permanent residents. Its current normal complement during the day is of 5 frontline emergency ambulances and 2 Response Car Paramedics. The aim is for each of these vehicles to have a State Registered Paramedic as part of the crew. At night the service uses only the 4 frontline ambulances and a Response Car Paramedic. Both Bronze and Silver commanders are available to respond appropriately to incidents throughout the day, and night via an on-call system. The Service is commissioned to operate a separate Patient Transport Service, this provision is for the transportation on non-urgent/acute customers being transported to hospital appointments on Island or to mainland centres (Southampton/Portsmouth) and who meet strict eligibility criteria as laid down by the Department of Health. The Isle of Wight Ambulance Service strives to be a national leader in patient care including clinical outcomes, whereby the most appropriate resource is identified with the patient at the time of call triage. From that point the clinicians/staff who answer the incoming calls or work on our vehicles can determine the most appropriate method of treatment which may include conveyance to the most appropriate destination. Often after the result of good clinical assessment treatment can be given in situ or signposting to alternative healthcare facilities meaning that some patients need not be conveyed at all.

Ambulance Service Conveyance Policy Page 7 of 48 Version 8
Procedures, guidelines and support are in place to ensure staff are able to identify the most appropriate course of action for any given patient. Poorly planned or inappropriate use of this limited resource significantly affects the standards that the NHS IOW endeavours to maintain and significantly reduces the service that the population of the Isle of Wight expects. One emergency ambulance on the mainland will reduce ambulance cover by up to 25%. Additionally, some relocations require expediency for medical reasons. In these instances the most expedient route should be considered.
3. SCOPE
This policy applies to any area that may engage in the ambulance transfer of a patient be it the planning, facilitating or relocation of that patient.
4. PURPOSE To provide information on the conveyance of patients and service types available.
5. ROLES AND RESPONSIBILITIES With regard to the conveyance of patients the Chief Executive has overall accountability to ensure that an effective risk management system operates within this Trust and for ensuring that an effective system of internal control functions within the Trust. The day to day responsibility for risk management is delegated to nominated Directors. The Executive Medical Director has delegated responsibility for managing risks associated with the conveyance of patients. The Head of Corporate Governance & Risk Management has delegated responsibility for managing the strategic development and implementation of organisational risk management strategy. The Executive Director of Nursing & Workforce has delegated responsibility for managing the strategic development and implementation of clinical governance. The Head of Ambulance has delegated responsibility for:
rategy within the Medical Services directorate.
complex or multi-casualty incidents.
equests on the Island.
and in place so that vehicles are regularly purchased to be able convey patients in a safe and a clinically risk adverse manner.
to its core duty by maintaining a minimal level (see appendix E) of operational ambulance vehicles on duty on the Island.
control and clinical governance.
ks associated with the conveyance of patients.
Ambulance Service Conveyance Policy Page 8 of 48 Version 8
The Performance Support Officers (Operations) have responsibility for the day to day delivery of the conveyance process and any associated risks. The Service Delivery Manager and Performance Support Officers (Integrated Care Hub) will ensure:
Integrated Care Hub staff are familiar with and trained to capture, collate and action any request for transport and that these skills are maintained / audited.
Ensure that procedures and equipment are in place to facilitate this capture, collation and recording of requests for transport.
Be responsible for dissemination of this policy amongst the Integrated Care Hub staff and their adherence to it.
Operational Staff are responsible for the day to day delivery of the conveyance process. This includes (but is not limited to) Senior Management Team, Clinical Support Officers, Emergency Care Practitioners Clinical Support Desk, Paramedics, Emergency Vehicle Operatives, Patient Transport Service, Emergency Medical Call Assessors and Dispatchers. It is the responsibility of all staff to: Identify risks and to highlight these to the appropriate manager, usually via the general report form or the Trust’s Incident Reporting Procedures. Employees also have a responsibility to cooperate with managers and to contribute to the process of identifying and reducing risks. Identify issues with this policy with the Ambulance Liaison Lead Comply with section 9 of the Transport Engineering Policy. Any driver of any vehicle that is being used to convey a patient is responsible for the safe carriage of that patient bearing due consideration to driving laws, their allowed exemptions, road conditions, environmental factors and other road users. The Fleet Engineering Manager is responsible for ensuring the maintenance of the fleet of patient carrying vehicles by ensuring that all defects are dealt with in a timely fashion and that in conjunction with the Ambulance Management processes are being adhered to with relation to the reporting of defects.
The Senior Clinician in attendance will be responsible for:
The decision to convey their patient, the triage assessment as to the urgency or level of care and the ambulance category for transport. The decision to transfer should be made as a balance of risk and benefit.
Ensuring that a bed is available at the receiving facility PRIOR to the conveyance being booked.
Informing the Ambulance service of any care requirements or advanced instructions regarding treatment. Liaison with the Integrated Care Hub and the Ambulance Duty Performance Support Officer’s is essential.
Communication with the receiving unit and with the clinician in charge with the patient during transfer.
In liaison with the Integrated Care Hub, are responsible for the timing of the conveyance and ensuring the patient is ready at the agreed pick up time.
The stabilisation of the patient prior to conveyance and determining who needs to accompany the patient within the limitation of resources that are available.
Ambulance Service Conveyance Policy Page 9 of 48 Version 8
Patient being ready in the correct location for pick up at the time the Ambulance Staff arrive. This is particularly with reference to TTO’s, Discharge summaries and use of Discharge lounge.
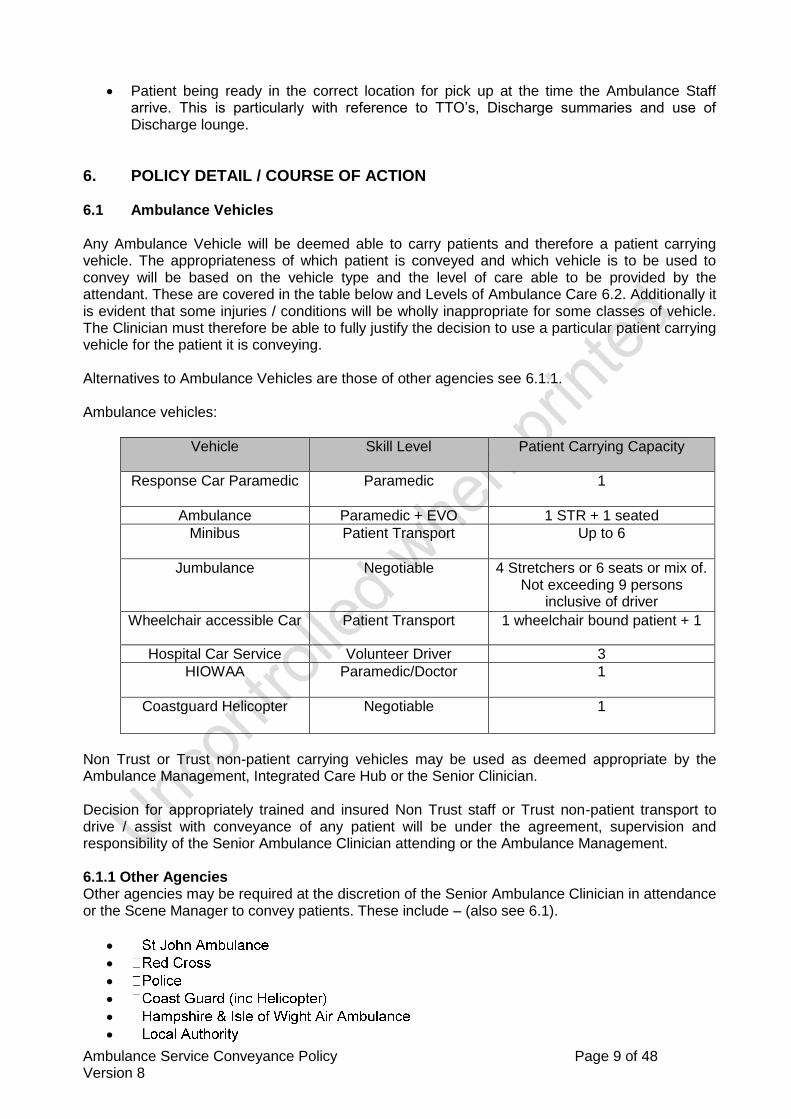
6. POLICY DETAIL / COURSE OF ACTION 6.1 Ambulance Vehicles Any Ambulance Vehicle will be deemed able to carry patients and therefore a patient carrying vehicle. The appropriateness of which patient is conveyed and which vehicle is to be used to convey will be based on the vehicle type and the level of care able to be provided by the attendant. These are covered in the table below and Levels of Ambulance Care 6.2. Additionally it is evident that some injuries / conditions will be wholly inappropriate for some classes of vehicle. The Clinician must therefore be able to fully justify the decision to use a particular patient carrying vehicle for the patient it is conveying. Alternatives to Ambulance Vehicles are those of other agencies see 6.1.1. Ambulance vehicles:
Vehicle
Skill Level Patient Carrying Capacity
Response Car Paramedic Paramedic 1
Ambulance Paramedic + EVO 1 STR + 1 seated
Minibus Patient Transport Up to 6
Jumbulance Negotiable 4 Stretchers or 6 seats or mix of. Not exceeding 9 persons
inclusive of driver
Wheelchair accessible Car Patient Transport 1 wheelchair bound patient + 1
Hospital Car Service Volunteer Driver 3
HIOWAA
Paramedic/Doctor 1
Coastguard Helicopter Negotiable 1
Non Trust or Trust non-patient carrying vehicles may be used as deemed appropriate by the Ambulance Management, Integrated Care Hub or the Senior Clinician. Decision for appropriately trained and insured Non Trust staff or Trust non-patient transport to drive / assist with conveyance of any patient will be under the agreement, supervision and responsibility of the Senior Ambulance Clinician attending or the Ambulance Management. 6.1.1 Other Agencies Other agencies may be required at the discretion of the Senior Ambulance Clinician in attendance or the Scene Manager to convey patients. These include – (also see 6.1).
Ambulance Service Conveyance Policy Page 10 of 48 Version 8
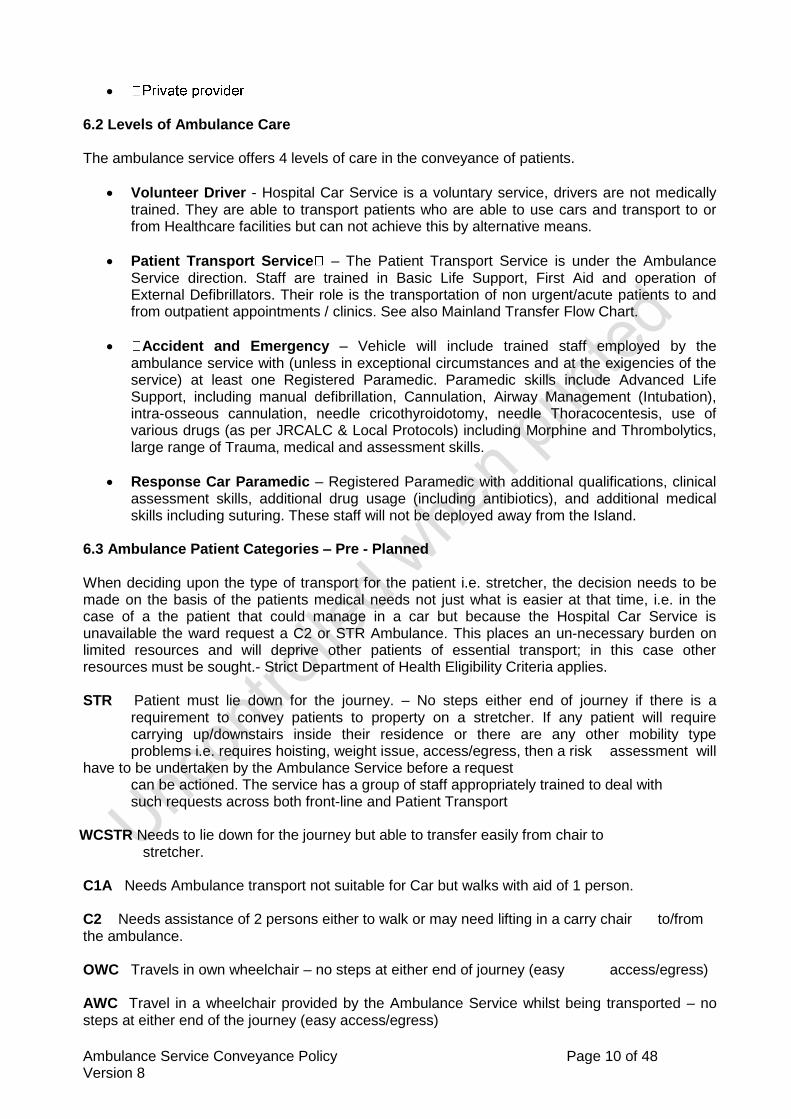
6.2 Levels of Ambulance Care The ambulance service offers 4 levels of care in the conveyance of patients.
Volunteer Driver - Hospital Car Service is a voluntary service, drivers are not medically trained. They are able to transport patients who are able to use cars and transport to or from Healthcare facilities but can not achieve this by alternative means.
Patient Transport Service – The Patient Transport Service is under the Ambulance Service direction. Staff are trained in Basic Life Support, First Aid and operation of External Defibrillators. Their role is the transportation of non urgent/acute patients to and from outpatient appointments / clinics. See also Mainland Transfer Flow Chart.
Accident and Emergency – Vehicle will include trained staff employed by the ambulance service with (unless in exceptional circumstances and at the exigencies of the service) at least one Registered Paramedic. Paramedic skills include Advanced Life Support, including manual defibrillation, Cannulation, Airway Management (Intubation), intra-osseous cannulation, needle cricothyroidotomy, needle Thoracocentesis, use of various drugs (as per JRCALC & Local Protocols) including Morphine and Thrombolytics, large range of Trauma, medical and assessment skills.
Response Car Paramedic – Registered Paramedic with additional qualifications, clinical assessment skills, additional drug usage (including antibiotics), and additional medical skills including suturing. These staff will not be deployed away from the Island.
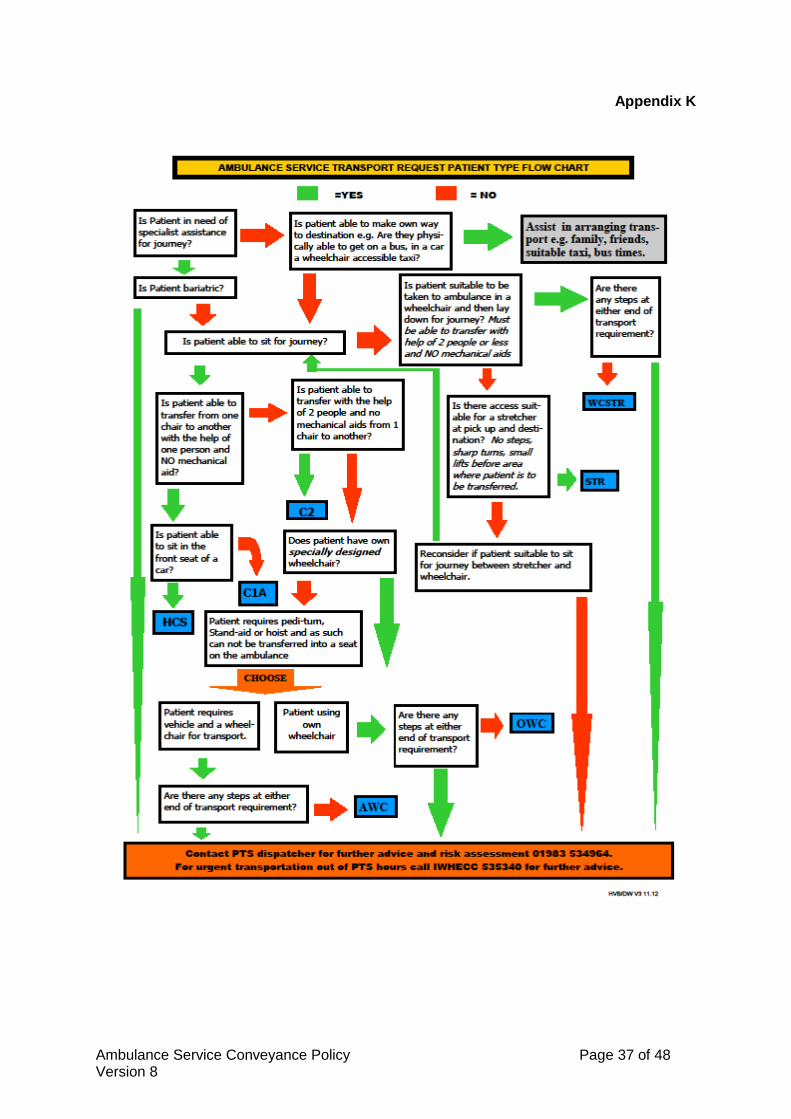
6.3 Ambulance Patient Categories – Pre - Planned When deciding upon the type of transport for the patient i.e. stretcher, the decision needs to be made on the basis of the patients medical needs not just what is easier at that time, i.e. in the case of a the patient that could manage in a car but because the Hospital Car Service is unavailable the ward request a C2 or STR Ambulance. This places an un-necessary burden on limited resources and will deprive other patients of essential transport; in this case other resources must be sought.- Strict Department of Health Eligibility Criteria applies. STR Patient must lie down for the journey. – No steps either end of journey if there is a requirement to convey patients to property on a stretcher. If any patient will require carrying up/downstairs inside their residence or there are any other mobility type problems i.e. requires hoisting, weight issue, access/egress, then a risk assessment will have to be undertaken by the Ambulance Service before a request can be actioned. The service has a group of staff appropriately trained to deal with such requests across both front-line and Patient Transport
WCSTR Needs to lie down for the journey but able to transfer easily from chair to stretcher. C1A Needs Ambulance transport not suitable for Car but walks with aid of 1 person. C2 Needs assistance of 2 persons either to walk or may need lifting in a carry chair to/from the ambulance. OWC Travels in own wheelchair – no steps at either end of journey (easy access/egress) AWC Travel in a wheelchair provided by the Ambulance Service whilst being transported – no steps at either end of the journey (easy access/egress)

Ambulance Service Conveyance Policy Page 11 of 48 Version 8
HCS Hospital Car Service - must be independent and able to get in/out of the vehicle with none or minimal assistance. Voluntary drivers do not have wheelchairs and are unable to transport walking frames A flow chart for categorising ambulance patients can be found at Appendix K Patients that are categorised incorrectly may prevent the patient from being conveyed by the Patient Transport vehicle tasked therefore delaying transportation.
NOTE Any incorrectly categorised patient can not be guaranteed to meet an agreed timeframe for conveyance. The Ambulance Service reserves the right to cross charge the requesting department for any costs incurred in re-tasking and conveying any incorrectly categorised patients. A tariff of charges can be found in Appendix G.
6.4 Ambulance Conveyance on the Island The Trust receives a variety of calls via different media (telephone, fax and or post) within the Integrated Care Hub these calls are received from a number of sources for example members of the public, GPs, GP Surgeries, hospital departments, dentists, midwives, emergency services and other healthcare providers. The types of call received are categorised as:-
• Emergency 999 calls • GP Urgent calls • Inter – Hospital / health facility transfers • Patient Transport bookings • Other related calls
The calls requiring conveyance of patients are prioritised within the Integrated Care Hub and all lead to the provision of an appropriate response such as:
• Emergency response • GP Urgent response • Hospital transfers or admission • Patient Transport response
Conveyance requirements for emergency patients will be determined by the clinicians’ /operational member of staff assessment of the patient in line with Joint Royal Colleges Ambulance Liaison Committee (JRCALC) Guidance, (2013). The organisation has accepted the JRCALC guidelines as best practice and all Ambulance clinical staff are issued with a JRCALC Manual and Pocket Book. The guidance provided within the JRCALC documentation allows clinicians to determine the best conveyance/referral options for patients based on their determined clinical condition. Ambulance clinicians will also use the Ambulance Service Clinical Support Desk, Ambulance Service Emergency Care Practitioners Procedures and the Ambulance Care Pathways Procedures to determine the appropriate conveyance of the patient. All conveyance information related to the movement of patients is recorded onto the relevant computer system and records the patients’ details, clinical condition, reason for transport or response, if appropriate conveyance destination, notes on specific condition or requirements, escort and whether medical notes and medications will be transported with the patient will be given to the conveying crews. This information is passed to the designated response via data transfer, paper format or voice – as appropriate. All telephone and radio communications are recorded and stored according to organisational policy.
Ambulance Service Conveyance Policy Page 12 of 48 Version 8
6.4.1 Emergency The Integrated Care Hub will be responsible for establishing the need for Ambulance Conveyance. This will be through a variety of mediums and utilising the Integrated Care Hub Protocols such as Computer Aided Dispatch NHS Pathways. The Duty Dispatcher and or Senior Clinician located within the Integrated Care Hub will oversee the calls and dispatch the most appropriate resource as per Ambulance procedures. Emergencies will predominantly arrive at the Integrated Care Hub by 999 calls. These will assessed and triaged, when identified most appropriate resource will be dispatched to respond. Resources will be despatched by the duty dispatcher. The location of where to convey the patient will be at the discretion of the senior clinician in attendance. Ambulance staff may admit patients direct through A&E, Coronary Care Unit, Children’s Ward or Maternity. Where able this decision will be discussed and communicated to the patient involved, or their legal guardian, or the next of kin, or responsible other person. The senior clinician in attendance following the assessment may wish to refer or access other health care facilities; this will be done via established procedures. 6.4.2 Urgent Urgent transport requests will be initiated in a variety of means. GP’s, call triage and other medical professionals. These sources will triage / assess the patient and will categorise the patient accordingly. All Urgent calls will have a response within 4 hours as standard, unless the GP requests a more urgent response. Integrated Care Hub contact numbers can be found in Appendix F. If during triage the GP requests a more urgent response, the options are:
If the condition of the patient or the risk of potentially life-threatening deterioration warrants defer will be to an 8 minute response with ‘blue lights and sirens’ Often the triaging / assessing clinician will have arranged admission to a specific place. As there is a time difference between their triage / assessment and the arrival of the ambulance, ambulance staff may on their assessment alter the location of the patient’s destination within St Mary’s. 6.4.3 Admissions, Discharges, Out Patient and Clinic Appointments
To enable the planning and appropriate resource management a minimum of 24 hours notice is required for all admissions, discharges, out patient and clinic appointments (please see exception to this rule for ED and MAAU below). Transportation using the Patient Transport Service resources is not a right but is based upon medical requirements. (Refer to the DOH eligibility criteria for patient transport 2008) The transfer by patient transport vehicles of patients who do not require this type of transport is inappropriate. Any requester department booking an inappropriate classification maybe cross charged.

Ambulance Service Conveyance Policy Page 13 of 48 Version 8
NOTE: Request for transport without 24 hour notice can not be guaranteed to be met. The Ambulance Service reserves the right to cross charge the requesting department for any costs incurred in meeting a late notice request. A tariff of charges can be found in Appendix G.
Admissions All admissions must be authorised by a Doctor or other allied health professional with prior agreement from the Ambulance service. The authorising person must have assessed the appropriateness of using ambulance transport and identified the correct category of transport required (see above).
Discharge Discharges are to be managed as per the Discharge Planning Policy. The Discharge area must be utilised at all times as per Discharge Planning Policy. Discharging patients via patient transport need to be ready for either 09:00hrs or 13:00hrs pickup. To access these discharge slots the patient’s transport must have been booked before 14:00hrs previous day. Patients requiring transfers out of hours will be conveyed on an “as and when” basis. Any out of hours discharges will likely reduce the Islands Emergency cover so no guarantees can be given. Availability of emergency ambulance vehicles for discharge commitments will be at the discretion of the Duty Dispatcher when making the request. To help facilitate the 4 hour target discharges will be accepted from the Emergency Department without 24 hours notice. These must be booked at the earliest indication of medical need for transport being required. A ‘Breach’ time must be added to the request to identify the target time for discharge. Discharges without 24 hour notice will also be accepted from MAAU for patients whose treatment required less than 24 hours admittance. Notice of a pending discharge should be given as early as possible, ideally after initial triage. A sample audit of 25 requests will be undertaken for appropriateness of use. All patients must be referred to the Discharge Area for collection.
Out Patient and Clinic Appointments
Island out patient and clinic appointments will be booked and confirmed by the requesting GP surgery / clinic / area. Out patient and clinic appointment times for patients conveyed by patient transport and hospital car service will be either 10:00hrs for morning clinics or 14:00hrs for afternoon clinics. It is the responsibility of the person/department making the booking to ensure the patient and out patient clinic is informed of the appointment time. Patients are expected to be ready at the designated time and any cancellations must be directed to the Patient Transport Service Dispatch Team at the Integrated Care Hub prior to the event. All patients are contacted 24hrs prior to their expected journey and given a time when they are expected to be ready from.
Arranging Transport
Wards and department wishing to arrange transport for a patient should complete in full the current ambulance transport request forms, current copies of this can be found on the Trust intranet site under ambulance. (Appendix I & J). An E-booking programme is currently being

Ambulance Service Conveyance Policy Page 14 of 48 Version 8
reviewed for implementation in the future. (On implementation full training in all areas will be offered) Bookings will not be taken any more than 6 weeks in advance. All transport requests must have all fields completed including the patient’s NHS number/DOB/Last recorded weight/all details of the requester and their contact numbers. Please note – any patient being transferred/discharged to an address which is not their permanent address must have details of their permanent address put onto the transport request form 6.5 Special considerations 6.5.1 Escorts and Luggage Non medical escorts i.e. relatives / friends of patients being transported to hospital will usually be limited to one person per patient. This is due to the available space and legality with regard to seat orientation and passenger securing. In some circumstances escorts will not be able to travel with the patient, this will be at the discretion of the senior clinician in attendance. In the instance of a patient who requires to be restrained for what ever reason (prisoner, mental health patient detained under the Mental Health Act) enough escorts to safely secure the patient and the occupants within it will be allowed. Escorts travelling with the Hospital Car Service will be charged at the current patient rate. Current Tariff available on the Trust Web site under Ambulance (Hospital Car Service) Escorts will only be allowed to travel in the Response Car Paramedic car at the discretion of the ambulance clinician. Medical Escorts will be accommodated at the discretion and in discussion with the senior clinician in charge. It is good practice for residential and nursing homes to provide escorts to facilitate care while attending clinics. Non medical escorts i.e. relatives / friends from wards will not be permitted to travel and will be required to make there own way to the destination. Luggage for patients will be restricted to one bag per patient not exceeding a size assessed by the staff to be safe. Walking frames will be conveyed by Patient Transport Service staff for patients who’s needs are such that to leave behind would put the patient at risk or raise safeguarding issues at their destination. Any bag conveyed MUST have the patient’s name written clearly attached to it to ensure it is delivered to the correct address and with the correct patient. Emergency Vehicles will not carry items that can not be secured safely; this will include items such as wheel chairs, walking frames, or animals. The Hospital Transport Department (non-patient) will transport items too bulky for Patient Transport Service to convey as long as they have at least 24hrs notice and this can be accommodated with their routine journey planning between the hours of 08:30-16:30 Monday to Friday. The department reserve the right to cross charge for this. 6.5.2 Medicines When conveying a patient to/from a healthcare facility the patients’ medication must always be conveyed with the patient in a ‘green patient medications bag’ as supplied by pharmacy, with the patients name clearly written on the outside. These in turn must be handed to an appropriate member of staff on arrival at receiving facility. This should also be recorded on the Electronic Patient Clinical Record (EPCR) where appropriate.
Ambulance Service Conveyance Policy Page 15 of 48 Version 8
6.5.3 Wheelchairs
The conveyance of patients in their own wheelchairs will be kept to a minimum, unless there is a medical need for transporting a patient within their wheelchair requiring medical attention to the designated department/hospital then other modes of transportation must be booked i.e. wheelchair assisted taxi. Electrically operated wheelchairs will only be transported if the chair can be placed into manual mode and operated at the rear by a member of staff. See ‘Wheelchair policy’ appendix I – Moving and Handling of Loads Policy – Safe Practise and Avoidance of musculoskeletal injuries 17/12/2012 6.5.4 Infectious Patients Any patient that is suspected or confirmed to have an infectious disease must be identified to the Patient Transport Dispatch Team at the time of booking a transport request. Any ambulance crew attending a patient that is suspected or confirmed to have an infectious disease must notify the Integrated Care Hub before committing to transporting the patient. In all cases of conveyance of a patient that is suspected or confirmed to have an infectious disease the guidance and procedures identified in the following documents must be followed: Infection Prevention & Control Diarrhoeal Infections Policy (including Norovirus), Infection Prevention & Control MRSA Policy, Infection Prevention & Control Clostridium Difficile Policy (Section 13 Infection Control Policy), Infection Prevention & Control Environmental Cleaning & Disinfection Policy, Infection Prevention & Control Isolation Policy. 6.5.5 Disruption to Normal Service There may be occasions where normal operating practice and procedure will need to be adaptive due to an incident, service demand or resource issue that affects service delivery of the organisation or any individual service that requires an ambulance conveyance. In these occasions the appropriate plan (Escalation, Major Incident and Business Continuity) will be followed. Any area experiencing operational problems on the day complying with the normal ambulance conveyance procedures should contact the Duty Dispatcher / Duty PTS Dispatcher (whichever relevant) within the Integrated Care Hub to discuss requirements and the Ambulance Service capacity to assist. 6.5.6 Ambulance Handover Delays at Hospital Overall safety issues of handover delays both for the individual patient who has not yet been ‘accepted’ by the emergency department and, potentially the unseen ‘life threatening’ call that maybe awaiting the availability of ambulance service resource tied up in the emergency department requires commitment for handover times to kept below 15 minutes with a turnaround time of 30 minutes to reduce risk. The handover period is precisely for handover, not the time before handover occurs. It is not acceptable that incident’s that happen to a patient in the department, but before formal handover has taken place is an ambulance issue. Where severe handover delays are experienced the Duty Bronze Commander will be dispatched to A/E and Site Co-ordinator contacted who in-turn will inform the Modern Matrons who will report to Accident & Emergency to determine why delays are occurring and what actions are required. Where ‘life threatening’ calls remain outstanding and with no allocated resources permission may be given to release the crew prior to formal handover if the expected 30 minutes have passed. The rational being that the risk of leaving patients before formal handover is less than a risk of
Ambulance Service Conveyance Policy Page 16 of 48 Version 8
delaying resource allocation to ‘life threatening’ calls. ‘Interim Escalation Measures continually being reviewed’ 6.6 Mainland Transfers Inherently there will be occasions whereby patients are required to be transferred to medical facilities that are not on the Isle of Wight. A transfer for clinical reasons necessary to provide specialist care not available on site e.g. cardio thoracic surgery, neurosurgery, paediatric critical care, hyperbaric medicine, diagnostic testing, etc. From April 2009 the cost of transfers of lodged patients to the mainland will be crossed charged to the department requesting the transfer. A tariff of charges for mainland transfers can be found at Appendix G. There is a significant risk both to the patient and to the rest of the population if mainland transfers are inappropriately booked. The Ambulance Service reserves the right to refuse any transfer via a land ambulance if to do so would compromise the Island operational minimum for emergency cover (Appendix E). Mainland transfers that result in a reduction in the pre-planned level of cover are to be reported via the incident reporting process. A reduction of one resource would normally indicate an amber incident and a reduction of two resources, breaching the Island operational minimum for emergency cover, a red. Transfers will fall into 3 categories: Elective, Urgent and Emergency, The authorising doctor is required to use the transfer triaging process in Appendix I to determine the transfer category. A Mews Score MUST be given for all urgent/emergency mainland transfer requests. Urgent and emergency transfers will not be transferred directly to the mainland from a home address without prior assessment / stabilisation at St Mary’s hospital. In exceptional circumstances where transfer from the community via ED increases the risk to the patient, transfer direct to the mainland may be sanctioned after discussion between the clinician, ED and Ambulance Operational Management.
NOTE: A request for emergency land transfer to any Mainland Hospital which reduces the Ambulance Service Island Operational cover by 25% or more, Then the Ambulance Service reserve the right to cross charge to the requesting department any additional costs incurred to increase cover back to the minimum levels A tariff of charges can be found in Appendix G.
Note Transport to facilities outside of Southampton and Portsmouth Other than the patients from St Mary’s Hospital to another place of care, receiving units outside of Southampton and Portsmouth will be cross charged for the travel as the care provider is responsible for transport. Therefore the patients transport requirements must be made known to the provider and authorisation gained for transport to be provided by IOW Ambulance Service at the time of booking. When completing the transport request form the patient’s home address their own GP must be identified

Ambulance Service Conveyance Policy Page 17 of 48 Version 8
6.6.1 Elective Patients requiring out patient appointments or able to wait greater than 24 hours for relocation fall into this category. A minimum of 48 hours notice is required and the patient will arrive at the destination in the time frame stated in the request. This category of patient will normally be conveyed by Patient Transport Service or Volunteer Hospital Car Service as deemed appropriate against the patient’s medical needs. Charges apply for using the Hospital Car Service. Current tariff is available on the Trust intranet under ambulance.
Note Patient’s appointment times should not be arranged for earlier than 10:00 hrs. Patients need to be prepared for an early start and may experience a long day, as morning and afternoon appointments will travel in the same vehicle incurring only one mainland crossing a day.
6.6.2 Urgent This patient is stable but in need of care that can not be given by this hospital. Their care can best be provided by another healthcare provider. There is no immediate threat to this patient provided care is provided in less than 24 hours. The Ambulance Service will arrange for the patient to be picked up in under 12 hours and endeavour to arrive at the destination in the time frame stated in the transport request. Transport request may be initiated by phone with the Integrated Care Hub with a commitment for the transport request form to be delivered before the actual transfer is started. There is no minimum notice required for these transfers although an early discussion of potential transfer requirements with the Integrated Care Hub would be appreciated. Once the authorising Doctor has secured a destination the patient should be triaged for transfer and the request made with the Integrated Care Hub. At this point in the booking bed availability MUST BE confirmed otherwise the booking will not be accepted. The Ambulance Service Duty Performance Support Officer and the Bed Manager will negotiate with the receiving destination to affect the most appropriate route, mode and timings for the transfer, according to the urgency of the case. The requesting Doctor/department will then be notified of the pick-up time for when the patient would be expected to be ready. 6.6.3 Emergency This is a patient in a life or limb threatening condition or who is in such a condition whereby medical intervention that is unable to be provided at St Mary’s is required IMMEDIATELY. This decision will be based upon the Consultant responsible for that patient to decide using the Mainland Transfer Triage Tool in Appendix D. This decision is based upon medical need; such a priority will require the most expedient transfer route. All mainland ITU transfers will be categorised as Emergency transfers, the ambulance Service will provide a ‘blue light trained’ ‘driver only’ and vehicle. Reference to the Wessex Critical Care Networks Policy and Procedures for the Transfer of Critically Ill Patients must be followed. Any Ambulance emergency transfer WILL be with blue lights and sirens. Medical need must therefore be present for ambulance to claim this exemption from driving regulations.

Ambulance Service Conveyance Policy Page 18 of 48 Version 8
If the transfer is time critical the Doctor authorising should state this at the time of the transfer request, identifying the time critical nature and reason. Transport request may be initiated by phone with the Integrated Care Hub with a commitment for the transport request form to be received before the actual transfer is started. The Ambulance Service will aim for the patient to arrive at their destination usually in under 4 hours. Please Note
These times are dependant on many factors outside of our control or influence and should not be the norm expected. As with urgent transfers, once the request has been made to the Integrated Care Hub the Ambulance Service Duty Performance Support Officer and the Bed Manager will negotiate with the receiving destination to affect the most appropriate route, mode and timings for the transfer. Given the emergency nature of the case the most expedient route is via air transfer, secondary retrieval via Hampshire & Isle of Wight Air Ambulance (HIOWAA) or HM Coastguard. Please refer to Helicopter Transfers below. The requesting Doctor/department will be notified of the pick-up time but the patient would be expected to be ready for immediate pick up from time of request. This category of patient can be conveyed by paramedic if there is a specific care requirement for one. Please recognise utilising one frontline emergency ambulance out of hours reduces Island resources by 25%. 6.6.4 Helicopter Transfers The HIOWAA and the HM Coastguard helicopters are available to the Ambulance Service for mainland transfers. The procedure and criteria for helicopter transfers can be found in Appendix N. If a department requests a helicopter transfer or requests an Emergency Transfer which must arrive at the destination ASAP or within 3 hours the Ambulance Service will initiate a helicopter transfer if it meets the criteria for such a transfer. The cost of this transfer will be borne by the requesting department. The Ambulance Service may use a helicopter for the transfer of a patient if there is a lack of Ambulance Service capacity and the transfer meets the helicopter criteria. In these instances the requesting department will only be charged the standard ambulance tariff for the transfer and not the cost for the helicopter. The completed documentation for Helicopter Transfer MUST be authorised/received before activation/dispatch of the helicopter. Where the transfer is from within the hospital environment the ‘vacuum’ mattress from ITU must be used to transport the patient. This will be returned by the Nurse/Dr escort. Where spinal injuries are suspected and to transfer a patient already secured on an Ambulance Spinal Immobilisation Board would be detrimental, in this instance this will be used to transfer the patient, but the responsibility of returning this equipment will remain with the escort travelling with the patient. Failure to return equipment may result in charges being made for replacement to the requesting department.
Ambulance Service Conveyance Policy Page 19 of 48 Version 8
Note Exceptions to these Transfers will be assessed on an Individual basis in consultation with the Ambulance Service, their Medical representative (A&E Consultant) and the Consultant responsible for the patient. Any deviation or transfer occurring outside of this framework should be reported as an adverse incident through the organisations’ incident reporting process by any involved party. Mainland Transfer Flowchart – please see Appendix D. 6.6.5 Transfer routes
Conveyance methods:
- Patients own transport. – Can the patient be conveyed by non NHS means? - Hospital Car Service – Patient fully mobile no assistance required – charges apply. - Patient Transport Service./ Patient Transport Team - Emergency Vehicle Operative – Blue light driver - Hampshire and Isle of Wight Air Ambulance - HM Coast Guard - Ambulance car - Emergency Ambulance
Routes:
- East Cowes – Southampton. Via Red Funnel Car Ferry. - Fishbourne – Portsmouth. Via Wightlink Car Ferry. - Yarmouth – Lymington. Via Wightlink Car Ferry - MedEvac – St Mary’s Helipad to Southampton / Portsmouth hospitals.
6.7 Special Patient Categories Conveying certain people will require special consideration and be at the discretion of the senior clinician in attendance. These patients include, children, vulnerable persons, Prisoners and CBRN / Majax patients. These patients will be conveyed using established protocols and joint working with other agencies, utilising the other agencies’ protocols. Conveyance of these patients will be done in a safe and risk adverse manner. The special considerations will include, safely securing the passenger, escorts, additional documentation, health and safety issues, privacy issues and vulnerability of staff issues. Mental Health patients will be conveyed in line with the multi-agency transportation protocol for Clients from the Hampshire and Isle of Wight Mental Health Services. The Ambulance Service will not convey any patient whose behaviour represents a real and present threat to the safety of staff. Staff required to convey bariatric patients or patients with special manual handling needs, should refer to the Safe Moving of Loads & Avoidance of Musculoskeletal Injuries Policy. Emergency and urgent maternity transfers into hospital from the community are able to be requested by the attending midwife. Please refer to the Labour ward guideline: Maternal Transfer in from the Community. Emergency and Urgent maternity and neonatal mainland transfers should refer to Labour Ward guidelines: Maternal Mainland Transfer and Neonatal Transfer to the Mainland. For the transfer of children to other hospitals please refer to guidance in Appendix M.

Ambulance Service Conveyance Policy Page 20 of 48 Version 8
Patients that die while being transported by ambulance, including those that have undergone unsuccessful resuscitation, will be taken to the mortuary and the established procedure for Recognition Of Life Extinct (ROLE) will be followed.
All children (less than 18 years) whether deceased or undergoing resuscitation will be conveyed to the Emergency Department, regardless of the viability of the ongoing resuscitation, attempt as per Kennedy Report (Sudden unexpected death in infancy: a multi-agency protocol for care and investigation. The report of a working group convened by The Royal College of Pathologists and The Royal College of Paediatrics and Child Health Guideline).
6.8 Documentation All conveyance information related to the movement of patients is recorded onto the relevant computer system and records the patients’ details, clinical condition, reason for transport or response, available Risk Assessments, alerts, if appropriate conveyance destination, notes on specific condition or requirements, escort and whether medical notes and medications will be transported with the patient will be given to the conveying crews. This information is passed to the designated response via data transfer, paper format or voice – as appropriate. All telephone and radio communications are recorded and stored according to Trust policy. 6.8.1 Patient Clinical Record (PCR) The Electronic Patient Clinical Record (EPCR) is completed by ambulance staff for each patient attended including emergencies, GP urgent admissions and transfers. For more details staff should refer to the current Guidelines for the Completion of Ambulance Patient Clinical Records. In the event of an electronic system failure a paper Patient Clinical Record will be completed. This Patient Clinical Record comprises a sheet with a carbon copy. The top copy of the completed form is retained by the attending member and sent to ambulance HQ for entry onto the Clinical Audit Review System (CARS). The bottom copy is presented to medical staff at the receiving hospital, or left with the patient. (A signature of the receiving member of staff must be obtained at handover on the form) Conveyance to hospital is not always the most appropriate outcome for the patient. The attending clinician may decide that the patient’s condition does not warrant transportation to hospital or that referral to an alternative care pathway is preferable. Alternatively, the patient may decide that he or she does not wish to be conveyed. The refusal section of the Electronic Patient Clinical Record (EPCR) must be fully completed if using paper version the carbon copy left with the patient. For more details staff should refer to the Guidelines for the completion of Ambulance Patient Clinical Records, Emergency Care Practitioners Procedures and the Ambulance Care Pathway Guidelines. If the conveying crew is presented with a GP letter or patients notes these must always be conveyed with the patient and recorded on the Electronic Patient’s Clinical Record form. If the conveying crew are transferring a GP Urgent and the GP has left a letter with the patient this should be conveyed to the receiving unit. Conveying crews have access to the letters and notes if they have concerns about the patient’s condition.
7. CONSULTATION This revision of the existing policy has been considered by the Ambulance Senior Management Group.

Ambulance Service Conveyance Policy Page 21 of 48 Version 8
8. TRAINING The Ambulance Conveyance Policy does not have a mandatory training requirement but the following non mandatory training is recommended. The Ambulance Liaison Lead is to work with stakeholders on understanding processes within this policy, support, advice and will be the first point of contact should wards wish to review procedure. The information within this policy will be disseminated to ambulance staff through various service training modules as appropriate. Further awareness sessions will be made available to any area by the Ambulance Liaison Lead as identified by any lead clinician or department head.
9. DISSEMINATION 9.1 When approved this document will be available on the Intranet and will be subject to
document control procedures. Approved documents will be placed on the Intranet within 5 working days of date of approval once received by the Risk Management Team.
9.2 When submitted to the Risk Management Team for inclusion on the Intranet this
document will have fully completed document details including version control with the actual hard copy signed by the relevant Lead Director. Keywords and description for the Intranet search engine will be supplied by the author at the time of submission.
9.3 Notification of new and revised documentation will be issued on the Front page of the
Intranet, through e-bulletin, and on staff notice boards where appropriate. Any controlled documents noted at the Trust Executive Committee will be notified through the e-bulletin.
9.4 Staff using the Trust’s intranet can access all procedural documents. It is the
responsibility of managers to ensure that all staff are aware of where, and how, documents can be accessed within their areas of work.
9.5 It is the responsibility of each individual who prints a hard copy of any document to ensure
that the printed hardcopy is the current version. Current versions are maintained on the Intranet.
10 EQUALITY ANALYSIS The IOWAS acknowledges the following basic rights for all people it may see.
– for all patients. These rights carry with them responsibilities and the Service requires all members of staff to recognise these rights and to act in accordance with them in all dealings with patients. In addition, the Service will comply with all relevant legislation and good practice, in line with the Equality and Diversity Policy 01/10/2012 No individual will be unjustifiably discriminated against. This includes, but not exclusively, on the basis of gender, race, nationality, ethnic origin, religious or political beliefs, disability, marital status, social background, family circumstance, sexual orientation, gender reassignment, psychiatric disorder, criminal convictions, age or for any other reason.
This procedure has undergone an equality analysis please refer to Appendix O
Ambulance Service Conveyance Policy Page 22 of 48 Version 8
11. REVIEW AND REVISION ARRANGEMENTS This policy will be reviewed 3 yearly by the Ambulance Service hospital Liaison Lead
12. MONITORING COMPLIANCE AND EFFECTIVENESS A periodic review will be undertaken along with a ‘snap shot’ audit to correlate CAD dispatches against EPCR completion. This will be carried out by the Deputy Head of Ambulance (Clinical) Any mainland transport requests that result in the Islands Emergency Ambulance cover falling below the minimum level will be reported via the organisations incident reporting system. These will be reported by the Performance Support Officers (Operational/Hub) Helicopter usage will be audited for appropriateness and will be reported at the Ambulance Senior Management meeting as required. Review of the on-going audit of Primary Percutaneous Coronary Intervention (PPCI) within the EPCR system will be reported monthly to the Ambulance Clinical Effectiveness Group and Senior Management Group via Ambulance Co-Sitrep AQI The Ambulance Liaison Lead will report any issues with the operation of this policy to the Ambulance Senior Management Group as required.
13. LINKS TO OTHER ORGANISATION POLICIES/DOCUMENTS Equality and Diversity Policy JRCALC Clinical Guidelines Ambulance Care Pathway Guidelines Guidelines for the completion of Ambulance Patient Clinical Records Ambulance Emergency Care Practitioner Procedures Maternity Guidelines: Guidelines for Ambulance Transfers. Discharge Planning Policy Safe Moving of Loads & Avoidance of Musculoskeletal Injuries Policy Mental Capacity Act Ambulance Service Operational Instructions Transport Policy Health & Safety Policy Hampshire & Isle of Wight Air Ambulance Standard Operating Procedures Helicopter Transfer Policy
14. REFERENCES
Risk Management Strategy
Incident and Reporting and Management Policy
Health Records Policy and Procedures
Trust Job Descriptions
15. DISCLAIMER
It is the responsibility of all staff to check the Trust intranet to ensure that the most recent version/issue of this document is being referenced
Ambulance Service Conveyance Policy Page 23 of 48 Version 8
16. ACRONYMS
A&E Accident & Emergency
CAD Computer Aided Dispatch
CARS Clinical Audit Review
CBRN Chemical, Biological, Radiological, Nuclear
DOH Department of Health
ED Emergency Department
EPCR Electronic Patient Clinical Record
EVO Emergency Vehicle Operative
HIOWAA Hampshire & Isle of Wight Air Ambulance
JRCALC Joint Royal College Liaison Committee
MAAU Medical Assessment and Admissions Unit
PPCI Primary Percutaneous Coronary Intervention
PTS Patient Transport Service TTO's To Take Out (Take home medication)

Ambulance Service Conveyance Policy Page 24 of 48 Version 8
Appendix A
KEY DEFINITIONS FOR DOCUMENTATION
Conveyance for the purpose of this policy is: The conveyance of patients, medical and clinical personnel, equipment and associated records, as appropriate including from one healthcare facility to another as well as the initial journey from the scene. Patient carrying Ambulance Vehicles are defined as any vehicle, which at the discretion of the clinician on board responsible for that patient, is capable of appropriately and safely convey that patient according to established clinical protocols and guidelines. Lodged Patient is a patient who has been admitted onto a ward within the hospital; this includes patients in the Medical Assessment Unit but excludes patients within the Accident & Emergency Department.

Ambulance Service Conveyance Policy Page 25 of 48 Version 8
Appendix B
CHECKLIST FOR THE DEVELOPMENT AND APPROVAL OF CONTROLLED DOCUMENTATION
To be completed and attached to any document when submitted to the appropriate committee for consideration and approval. Title of document being reviewed:
Y/N/ Unsure
Comments
1. Title/Cover
Is the title clear and unambiguous? Y
Does the title make it clear whether the controlled document is a guideline, policy, protocol or standard?
Y
2. Document Details and History
Have all sections of the document detail/history been completed? Y
3. Development Process
Is the development method described in brief? Y
Are people involved in the development identified? Y
Do you feel a reasonable attempt has been made to ensure relevant expertise has been used?
Y
4. Review and Revision Arrangements Including Version Control
Is the review date identified? Y
Is the frequency of review identified? If so, is it acceptable? Y
Are details of how the review will take place identified? Y
Does the document identify where it will be held and how version control will be addressed?
Y
5. Approval
Does the document identify which committee/group will approve it?
Y
If appropriate have the joint Human Resources/staff side committee (or equivalent) approved the document?
N/A
6. Consultation
Do you have evidence of who has been consulted? N
7. Table of Contents
Has the table of contents been completed and checked? Y
8. Summary Points
Have the summary points of the document been included? N
9. Definition
Is it clear whether the controlled document is a guideline, policy, protocol or standard?
Y
10. Relevance
Has the audience been identified and clearly stated? Y
11. Purpose
Are the reasons for the development of the document stated? Y
12. Roles and Responsibilities
Are the roles and responsibilities clearly identified? Y
Ambulance Service Conveyance Policy Page 26 of 48 Version 8
Title of document being reviewed:
Y/N/ Unsure
Comments
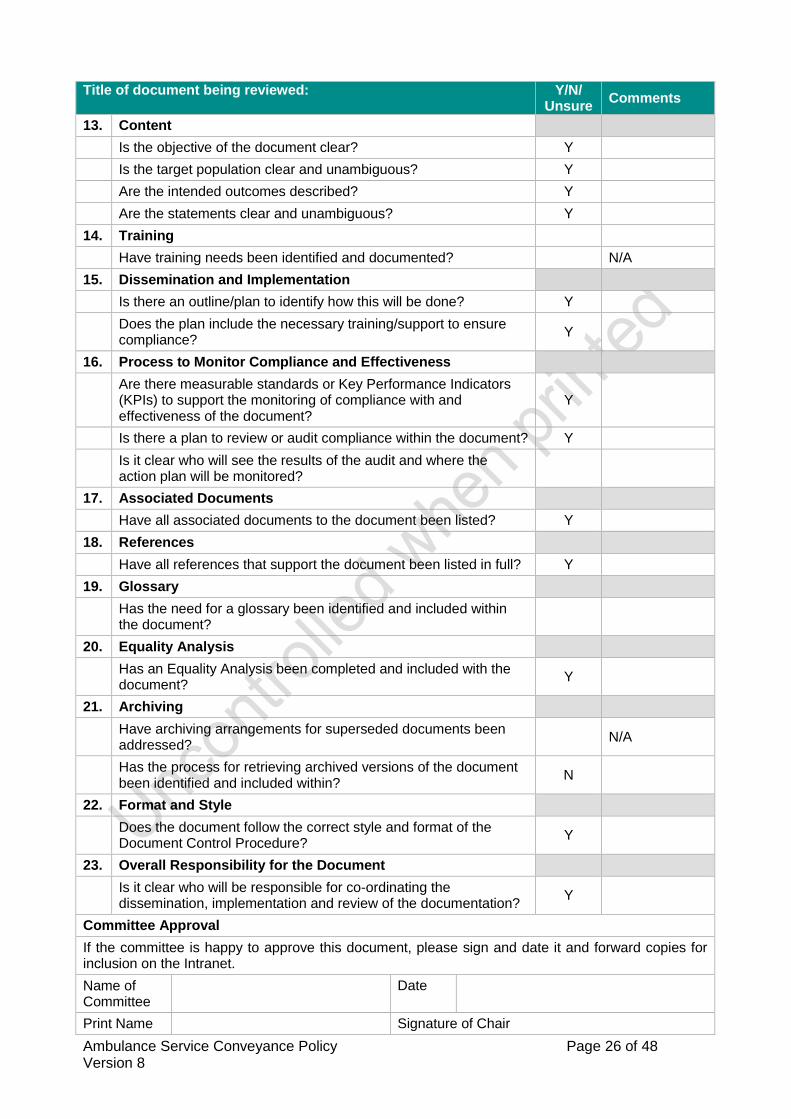
13. Content
Is the objective of the document clear? Y
Is the target population clear and unambiguous? Y
Are the intended outcomes described? Y
Are the statements clear and unambiguous? Y
14. Training
Have training needs been identified and documented? N/A
15. Dissemination and Implementation
Is there an outline/plan to identify how this will be done? Y
Does the plan include the necessary training/support to ensure compliance?
Y
16. Process to Monitor Compliance and Effectiveness
Are there measurable standards or Key Performance Indicators (KPIs) to support the monitoring of compliance with and effectiveness of the document?
Y
Is there a plan to review or audit compliance within the document? Y
Is it clear who will see the results of the audit and where the action plan will be monitored?
17. Associated Documents
Have all associated documents to the document been listed? Y
18. References
Have all references that support the document been listed in full? Y
19. Glossary
Has the need for a glossary been identified and included within the document?
20. Equality Analysis
Has an Equality Analysis been completed and included with the document?
Y
21. Archiving
Have archiving arrangements for superseded documents been addressed?
N/A
Has the process for retrieving archived versions of the document been identified and included within?
N
22. Format and Style
Does the document follow the correct style and format of the Document Control Procedure?
Y
23. Overall Responsibility for the Document
Is it clear who will be responsible for co-ordinating the dissemination, implementation and review of the documentation?
Y
Committee Approval
If the committee is happy to approve this document, please sign and date it and forward copies for inclusion on the Intranet.
Name of Committee
Date
Print Name Signature of Chair
Ambulance Service Conveyance Policy Page 27 of 48 Version 8
Appendix C (or subsequent letter appendix after other appendices) IMPACT ASSESSMENT ON DOCUMENT IMPLEMENTATION Summary of Impact Assessment (see next page for details)
Document title
Totals WTE Recurring £
Non Recurring £
Manpower Costs
Training Staff
Equipment & Provision of resources
Summary of Impact: Risk Management Issues:
Benefits / Savings to the organisation: Equality Impact Assessment Has this been appropriately carried out? YES / NO Are there any reported equality issues? YES / NO If “YES” please specify:
Use additional sheets if necessary.

Ambulance Service Conveyance Policy Page 28 of 48 Version 8
IMPACT ASSESSMENT ON POLICY IMPLEMENTATION Please include all associated costs where an impact on implementing this policy has been considered. A checklist is included for guidance but is not comprehensive so please ensure you have thought through the impact on staffing, training and equipment carefully and that ALL aspects are covered.
Manpower WTE Recurring £
Non-Recurring £
Operational running costs
Additional staffing required - by affected areas / departments:
Totals: NIL NIL
Staff Training Impact Recurring £
Non-Recurring £
Affected areas / departments e.g. 10 staff for 2 days
Totals: NIL NIL
Equipment and Provision of Resources Recurring £ *
Non-Recurring £ *
Accommodation / facilities needed
Building alterations (extensions/new) IT Hardware / software / licences Medical equipment Stationery / publicity Travel costs Utilities e.g. telephones Process change Rolling replacement of equipment Equipment maintenance Marketing – booklets/posters/handouts, etc
Totals: NIL NIL
Capital implications £5,000 with life expectancy of more than one year.
Funding /costs checked & agreed by finance: Signature & date of financial accountant: Funding / costs have been agreed and are in place: Signature of appropriate Executive or Associate Director:
Ambulance Service Conveyance Policy Page 29 of 48 Version 8
IMPACT ASSESSMENT ON DOCUMENT IMPLEMENTATION - CHECKLIST
Points to consider
Have you considered the following areas / departments?
Have you spoken to finance / accountant for costing?
Where will the funding come from to implement the policy?
Are all service areas included? o Ambulance o Acute o Mental Health o Community Services, e.g. allied health professionals o Public Health, Commissioning, Primary Care (general practice, dentistry,
optometry), other partner services, e.g. Council, PBC Forum, etc. Departments / Facilities / Staffing
Transport
Estates o Building costs, Water, Telephones, Gas, Electricity, Lighting, Heating, Drainage,
Building alterations e.g. disabled access, toilets etc
Portering
Health Records (clinical records)
Caretakers
Ward areas
Pathology
Pharmacy
Infection Control
Domestic Services
Radiology
A&E
Risk Management Team are responsible to ensure the policy meets the organisation approved format
Human Resources
IT Support
Finance
Rolling programme of equipment
Health & safety/fire
Training materials costs
Impact upon capacity/activity/performance
Ambulance Service Conveyance Policy Page 30 of 48 Version 8
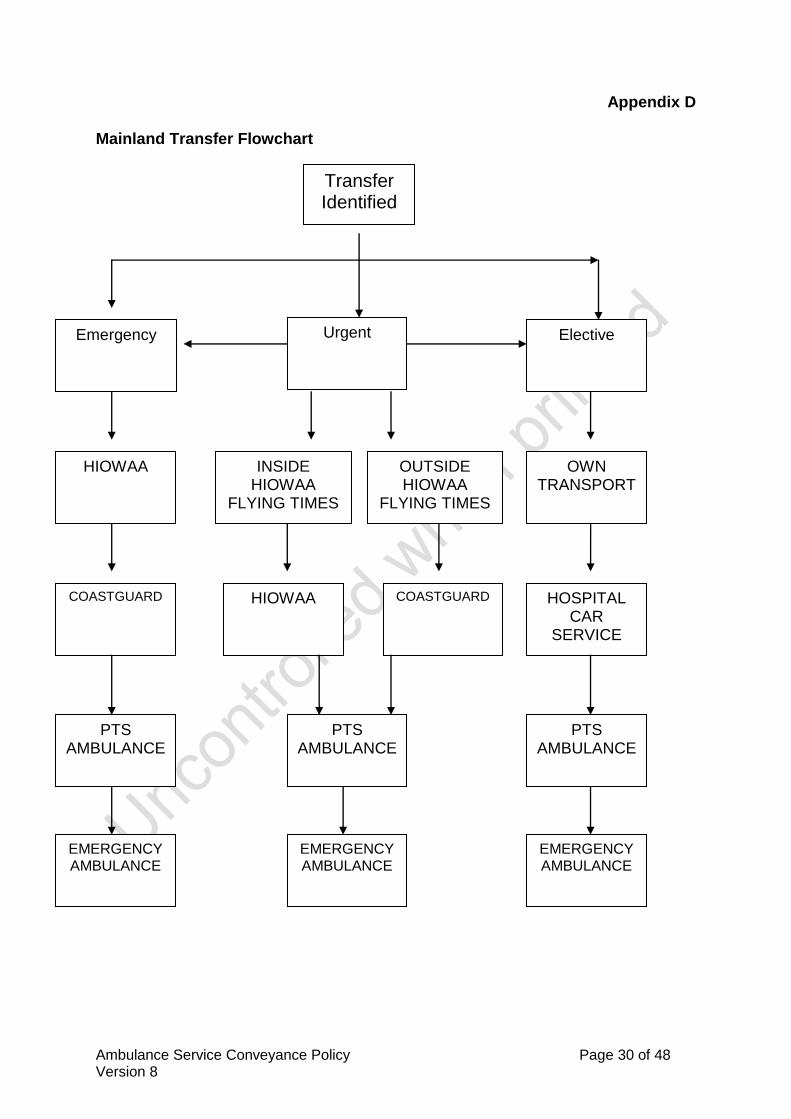
Appendix D Mainland Transfer Flowchart
Transfer Identified
Urgent Elective Emergency
HIOWAA INSIDE HIOWAA
FLYING TIMES
OUTSIDE HIOWAA
FLYING TIMES
OWN TRANSPORT
COASTGUARD HIOWAA COASTGUARD HOSPITAL CAR
SERVICE
PTS AMBULANCE
PTS AMBULANCE
PTS AMBULANCE
EMERGENCY AMBULANCE
EMERGENCY AMBULANCE
EMERGENCY AMBULANCE

Ambulance Service Conveyance Policy Page 31 of 48 Version 8
Appendix E
AMBULANCE SERVICE MINIMUM LEVEL OF OPERATIONAL ISLAND COVER
The level of cover below represents the pre-planned service level required for normal service activity. The Island operational minimum cover is the pre-planned levels minus ONE resource. This has been identified to enable the ambulance service to maintain core service delivery of responding to 999 calls on the Island. The reduction of this resource will still have an impact on other ambulance activity in order to maintain its 999 response. Mainland transfers that result in a reduction in the pre-planned level of cover are to be reported via the Trust incident reporting process. A reduction of one resource would normally indicate an amber incident and a reduction of two resources, breaching the Island operational minimum, a red. The minimum Operational cover for the Island should be maintained at the following levels: Weekday Days 4 Ambulances.
1 RCP. 4 PTS
Weekday Evening / Night 4 Ambulances
1 RCP
Weekend 4 Ambulances 1 RCP
The minimum Integrated Care Hub cover for the Island should be maintained at the following levels: Weekdays 07:00 - 00:00 1 Emergency Dispatcher 1 PTS Dispatcher (07:30-20:00)
3 Emergency Medical Call Assessors. 2 Clinical Support Desks 1 Performance Support Officer
00:00 – 07:00 1 Emergency Dispatcher
3 Emergency Medical Call Assessors 1 Clinical Support Desk
Saturday 07:00 – 00:00 1 Emergency Dispatcher
1 PTS Dispatcher (07:30-20:00) 5 Emergency Medical Call Assessors 3 Clinical Support Desks 1 Performance Support Officer
00:00 – 07:00 1 Emergency Dispatcher 3 Emergency Medical Call Assessors 1 Clinical Support Desk Sunday 07:00 – 00:00 1 Emergency Dispatcher
4 Emergency Medical Call Assessors 3 Clinical Support Desks 1 Performance Support Officer
00:00 – 07:00 1 Emergency Dispatcher 3 Emergency Medical Call Assessors 1 Clinical Support Desk

Ambulance Service Conveyance Policy Page 32 of 48 Version 8
Appendix F INTEGRATED CARE HUB CONTACT NUMBERS
Crews Dedicated 01983 232555 Priority answer for assistance GP’s Dedicated 01983 232444 GP’s urgent admissions etc Internal extension lines 01983 822099 ext 3503 Dispatcher
01983 822099 ext 3502 Routine 01983 822099 ext 3504 Patient Transport Dispatcher 01983 822099 ext 3505 Hospital Car Service
01983 534104 Fax: Integrated Care Hub including PTS/HCS
Public Number 111 Island Health line
Note All telephone lines into the Integrated Care Hub are
automatically recorded.
Ambulance Service Conveyance Policy Page 33 of 48 Version 8
Appendix G TARIFF OF CHARGES Ambulance Single Journey Tariff as at November 2013 Charges are calculated per trip, skill level, escorts, overnight accommodation against long distance journey, subsistence. For an up to date breakdown of cost against journey please contact the Administration Team at Ambulance HQ.
Ambulance Service Conveyance Policy Page 34 of 48 Version 8
Appendix H AMBULANCE TRANSPORT BOOKING PROCESS & FORM Wards and departments wishing to arrange transport for a patient should complete all the relevant ambulance transport request forms identified below, these forms should be authorised by a Doctor, Prescribing Nurse Practitioner or other Health Professional with prior agreement. If there is less than 24hours notice the Integrated Care Hub should be contacted via the telephone, during daytime hours 08:00-20:00 822099 ext 3504. All other times please phone 822099 ext 3502 to check availability of resources, the request should then be faxed to the Integrated Care Hub on 01983 534104 The Ambulance Service Transport Request form (Patient Transport/Hospital Car) should be completed in full including telephone numbers, patient weight, home address if being transferred to the mainland or to another care destination which is not their home address, and any additional information; this will enable the Patient Transport Team to assign the correct vehicle to the commitment. (If the form has not been completed correctly or in full the form will be returned which will cause delays) It is very important that the additional information section is completed, this information identifies any special needs, i.e. the patient is infectious, oxygen required, Bariatric or risk assessment required etc, Patient Transport Team/Integrated Care Hub can then resource the correct vehicle and appropriate crew. Patients being discharged from St Mary’s requiring ambulance transport will only be picked up from the Discharge Lounge; exceptional circumstances where a patient will be picked up from the ward will be when the patient requires emergency transfer to the mainland. The ambulance crew will then convey the patient from there. All discharges should be booked for am. All relevant paperwork (discharge summery & TTO’s) must be obtained prior to informing the Patient Transport Team/Integrated Care Hub that the patient is ready. The service is currently devising an on line e-booking process which will continue to be clinician lead and have the ability of sending requesting areas confirmation of receipt. It will also allow requesting areas to make amendments to bookings. All bookings will require a call handler to verify and confirm the booking.
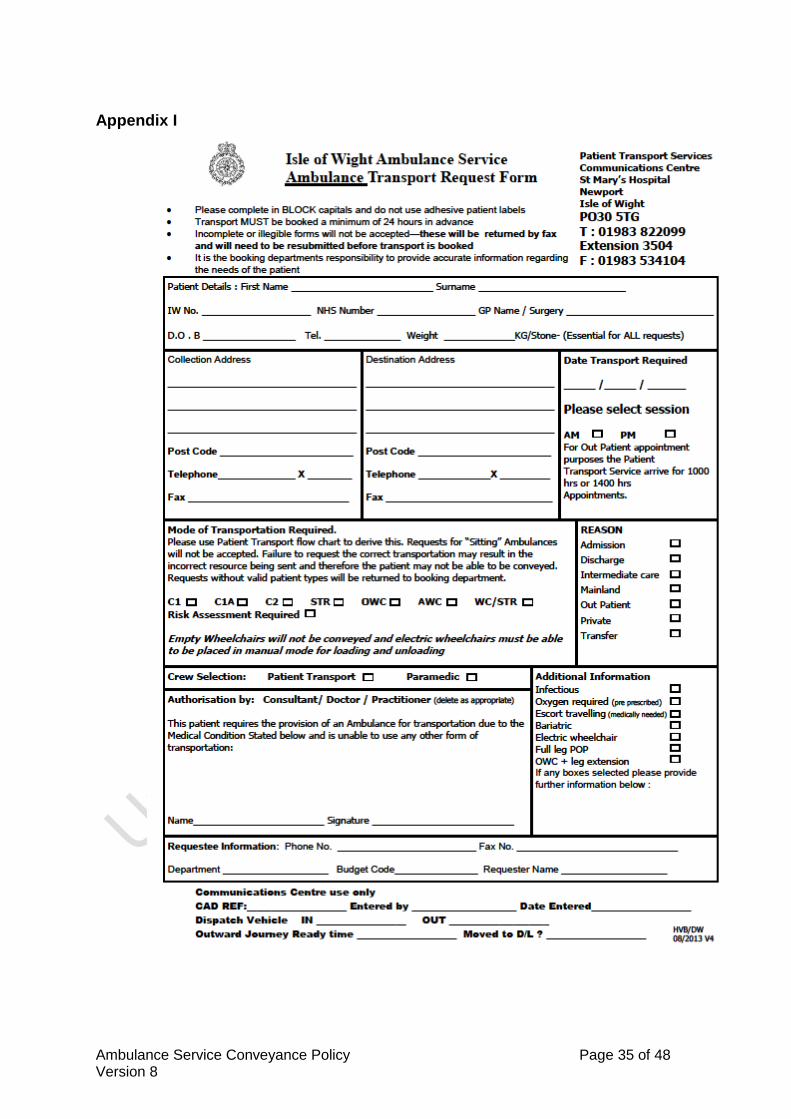
Ambulance Service Conveyance Policy Page 35 of 48 Version 8
Appendix I

Ambulance Service Conveyance Policy Page 36 of 48 Version 8
Appendix J
Ambulance Service Conveyance Policy Page 37 of 48 Version 8
Appendix K

Ambulance Service Conveyance Policy Page 38 of 48 Version 8
Appendix L Mainland Transfer Triage
To or From
ITU
Transfer Triage Tool
Current MEWS
Score > 2
Patient
Requiring
Ongoing
Intensive Care
Immediate Risk
To Life Or Limb
Critical
Illness
Time Critical
Transfer
MEWS > 4
in last six
hours
Consider
Urgent Transfer
NY
NY
Patient Meets Criteria For Emergency Transfer
No Notice Is Required For This Category Of Transport
If time Critical Please Stipulate The Latest Time The Patient Could Arrive At the Destination Hospital
Please Stipulate With Reasons The Minimum Skill Level Of The Transfer Team
The Ambulance Service Will Endeavour To Transport The Patient As Directed Or As soon As Possible
Guidance Notes:
If the patient were a new
presentation intervention
would be mandated within
six hours. Examples:-
Primary Angioplasty
Rescue Angioplasty
Unstable Angina (going to
directly to cath lab)
Aortic Dissection/aneurysm
Ischaemic Limb
Intracranial Pathology for
urgent neurosurgical
intervention
Guidance Notes:
Patient is travelling to or
from an intensive care
environment e.g. St Marys
ITU or Theater Recovery
ITU Environments are those
capable of delivering
advanced physiological
support and have a minimum
nurse to patient ratio of 2:1.
This would include Burns
Unit and Specialised
Maternity Services.
N Y Y

Ambulance Service Conveyance Policy Page 39 of 48 Version 8
Appendix M GUIDANCE FOR THE TRANSFER OF CHILDREN TO OTHER HOSPITALS It is recognised that the transferring of acutely sick children is inherently risky and there is very little research on this topic (Neil and Hughes, 2004, Heward, 2003). It is essential that children and young people are transferred safely and appropriately whilst also bearing in mind the unique geography of the Isle of Wight and the finite resources that are available for transport. Benchmarking that has been carried out relating to this topic indicates that they are several key factors that need to be addressed when considering the transfer of a sick child and these include:
Nursing Staff
Medical staff
Ambulance support
Planned transfer
Documentation
Parental Involvement
Equipment, including drugs
Protocols
It is recognised that the majority of transfers that take place are relatively short in distance, but may take time due to crossing the Solent, however it is still important to ensure that all aspects of patients safety and well-being are maintained at all times. Children and Young people under the care of Children’s Acute Services on the Isle of Wight will require transfer to another hospital for admission and investigation or for definitive treatment. Normally this is to the local tertiary Centre at Southampton General but may at times be further afield for specialist treatment or because of local pressure on available beds. “Arrangements should be in place for situations where retrieval is clinically inappropriate or time-critical, for example, severe head injury or intracranial bleeding, where waiting for the retrieval team may introduce unsafe delay. Under these circumstances, the retrieval will be undertaken by the referring hospital (primary transport). Arrangements should include:
advice from the lead centre;
a list of conditions that are time-critical for the hospital concerned;
contact details of relevant specialists where additional advice may
required, for example, neurosurgeons;
escort team of one doctor and one nurse;
Equipment.
(The acutely or critically sick or injured child in the District General Hospital, Department of Health, 2006) It is the responsibility of the referring lead clinician to assess and initiate the need for transfer of the child / young person. Routine transfers should be planned at least 24 hours in advance and communicated in a timely fashion to the Integrated Care Hub in order for them to plan and staff an appropriate transfer method.

Ambulance Service Conveyance Policy Page 40 of 48 Version 8
Urgent and emergency transfers need to be assessed on an individual basis and the most appropriate method of transfer (subject to time constraints and resources) used. It is the responsibility of the lead nurse to oversee the transfer and initiate telephone contact with Integrated Care Hub and warn them of the impending requirements for the transfer. Once transport for transfer is officially requested however, the patient must be ready to leave and all documentation, equipment and staffing organised. There is an implicit unwritten agreement between the Integrated Care Hub and Children’s ward that there is a degree of flexibility on both sides balancing the safe requirements of the transfer of the patient and organisation of the most appropriate method of transfer. The transfer may involve an ambulance, the Jumbulance, the HIOWAA or the Coast Guard Helicopter. The patient’s medical need and condition need to be weighed against the method of transfer and availability of staff and transfer vehicles. Traditionally, paediatric transfers are accompanied by a paediatric nurse with the appropriate skill level required for the transfer. It is Children’s Services aim to still accompany all mainland ambulance transfers due to the specialised nature of the patient. However, due to increasing dependence on the HIOWAA it may be physically impossible for paediatric staff to accompany patients requiring this transport. It is thus suggested that the staff requesting transfer discuss the patient’s requirement with the Integrated Care Hub in order that the most appropriate method of transfer can be agreed upon. The child will normally be escorted by a doctor and a nurse with experience and/or training in a) care of the critically sick child and/or b) emergency transfer and/or c) airway management. Appropriate drugs and equipment must be available for an emergency transfer. Drugs and equipment should be checked in accordance with local policy. (The acutely or critically sick or injured child in the District General Hospital, Department of Health, 2006). It is the responsibility of the transfer nurse to ensure all documentation pertaining to the child is collated and copied for the receiving hospital. Telephone communication is recommended between the transferring hospital and the receiving hospital to confirm arrival times, bed state etc. All transferring nurses will have access to the designated transfer ‘bag’ containing a portable full resuscitation kit specifically for paediatric patients. It is the responsibility of the transfer nurse to check this and all other medical supplies including equipment that they may need on the transfer. In preparation for the transfer, it is essential that resuscitation and stabilisation of the patient has occurred prior to transport. If there is any concern regarding the patients airway/breathing status then more senior advice should be sought and early airway intervention including intubation should be considered. The patient’s needs must be evaluated and attended to on a systems basis:
Airway management

Ambulance Service Conveyance Policy Page 41 of 48 Version 8
Spinal immobilisation
Respiratory system
Cardiovascular status /Haemodynamic status
Central Nervous system
Diagnostic studies as required
Appropriate wound care and fracture immobilisation
Nasogastric tube and urinary catheters as appropriate
It is important to ensure that transport orders are written and prescribed, patients x-rays and laboratory results are recorded. Whilst we recognise that it is important for any sick child to have family members present whilst in hospital and on transfer, if the HIOWAA or coastguard helicopter is being utilised, it will be impossible for a parent, relative or carer to accompany their child due to space constraints. The patients’ family will need to be informed of the transfer destination and be given instructions on how to reach the receiving hospital. If an ambulance is being used we should be able to accommodate one family member on the transfer. References: Department of Health, 2006. The acutely or critically sick or injured child in the District General Hospital, London. Heward, Y. 2003 Transfer from Ward to PICU: A Standard. Paediatric Nursing. Vol 15, no 1, February 2003. pp11-13. Neill, C and Hughes, U.2004 Improving inter-hospital transfer. Paediatric Nursing. Vol 16, no 7, September 2004. pp24-27.

Ambulance Service Conveyance Policy Page 42 of 48 Version 8
Appendix N
Procedure for the Consideration of and Transportation of Short Notice Urgent Transfer Patients By the Hampshire and Isle of Wight Air Ambulance
Any patient whose transportation to a mainland medical facility is requested by the treating consultant as a short notice transfer (transportation within 2 hours) should be considered for transportation by the Hampshire and Isle of Wight Air Ambulance A primary assessment of suitability should be carried out by the duty Performance Support Officer using the patient details given to the Integrated Care Hub by the requesting department. A secondary assessment should the be carried out by both the duty Operational Support Officer and the on-call Accident & Emergency Consultant by visiting the ward and directly assessing the patient and their medical notes. Any further concerns about suitability for transportation by the Air Ambulance should be discussed directly with the HEMS Desk. At weekends and out of hours the on duty A & E Consultant may only be contactable via telephone. Assessment of the patient will then be done by the duty Performance Support Officer in consultation with the on-call Emergency Department Consultant.
Time Line Events:
Integrated Care Hub
Duty Performance Support Officer or delegated person
A & E Consultant Ambulance Crew
Request for short notice transfer received from unit
Dispatcher advises PSO (OPS)
PSO Advised of request
Dispatcher checks availability of Helimed 56
Patient details faxed to PSO
Primary criteria met, contact with on-call A&E consultant
Advised of request by PSO
OSO visits ward to assess patient
Helimed advised of request by Dispatcher
Secondary criteria met – dispatcher informed.
The Integrated Care Hub dispatcher or appointed person to deploy helipad
PSO or delegated person co-ordinates packing and loading into helicopter
Dispatched to unit for loading and onto designated landing site
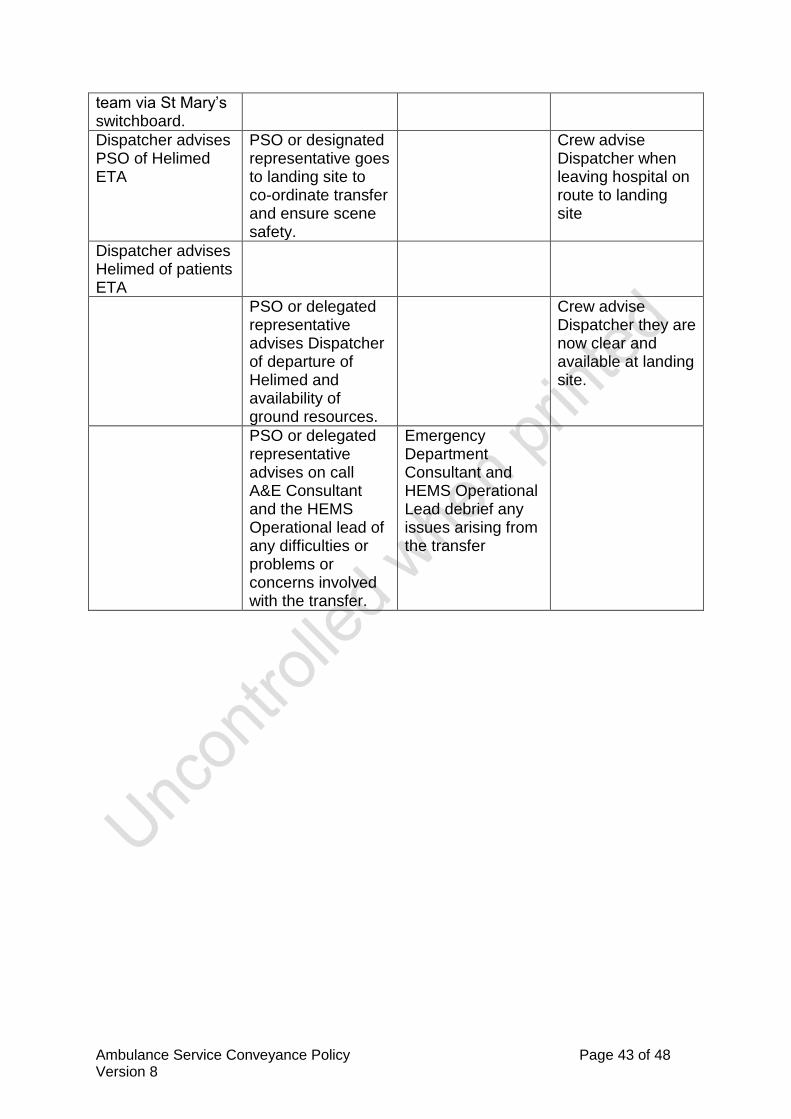
Ambulance Service Conveyance Policy Page 43 of 48 Version 8
team via St Mary’s switchboard.
Dispatcher advises PSO of Helimed ETA
PSO or designated representative goes to landing site to co-ordinate transfer and ensure scene safety.
Crew advise Dispatcher when leaving hospital on route to landing site
Dispatcher advises Helimed of patients ETA
PSO or delegated representative advises Dispatcher of departure of Helimed and availability of ground resources.
Crew advise Dispatcher they are now clear and available at landing site.
PSO or delegated representative advises on call A&E Consultant and the HEMS Operational lead of any difficulties or problems or concerns involved with the transfer.
Emergency Department Consultant and HEMS Operational Lead debrief any issues arising from the transfer
Ambulance Service Conveyance Policy Page 44 of 48 Version 8
Please refer to the Hampshire & Isle of Wight Air Ambulance Standard Operating Procedures for Pre-Hospital Care – Packaging of Patients.
The guidance below is part of the Standard Operating Procedures as issued by the Hampshire and Isle of Wight Air Ambulance Operations Group
In all aspects of helicopter flight the pilots’ decision is final
Primary Criteria for consideration of a patient for short notice urgent transfer by Air Ambulance 1) The patient should be transportable on the Helicopter transfer trolley. 2) The patient should be able to travel without medical escort (from the requesting ward). 3) The patient should have a patent, secure and properly managed airway. 4) The patient should not have been fitting immediately prior to request for transfer. 5) The patient should not have any uncontrolled haemorrhage. 6) The patient should be haemodynamically stable prior to request for transfer. 7) Under normal circumstances the patient should not have attempted suicide or be aggressive and uncooperative. 8) CCU patients should be assessed as stable for air transfer by the CCU consultant. 9) The patient should be ready for immediate transfer with all destination ward arrangements in place. Secondary Criteria for consideration of a patient for short notice urgent transfer by Air Ambulance 1) The patient should not be more suitable for transportation by other means. 2) The patient should not be dependant on any electronic medical equipment. Syringe drivers for Air Ambulance transfers will be available. 3) The patient must have all catheters, IV, central lines and monitoring leads securely protected prior to packaging on the ward. 4) The patient’s notes must travel with the patient and should be complete and up to date. 5) Ventilated trauma patients should be considered for bilateral thoracostomies prior to the request for transfer. 6) The transfer by Air Ambulance should be explained to the patient and consent obtained where possible. 7) The risk of cancellation of the Air Ambulance transfer due to another primary emergency mission should be explained to both the patient and the medical staff. 8) The patient should be properly prepared for the Air Ambulance transfer (psychologically and physically). 9) The patient should be secured using the Air Ambulance transfer equipment. (AeroHawk blanket, Vacuum mattress, Scoop and Straps)
10) All clinical risks and flight safety factors must be considered and any concerns or variances on the above guidance must be discussed with all parties; Duty Operational Support Officer, ED Consultant, patients Consultant and the pilot & Crew of Helimed 56.
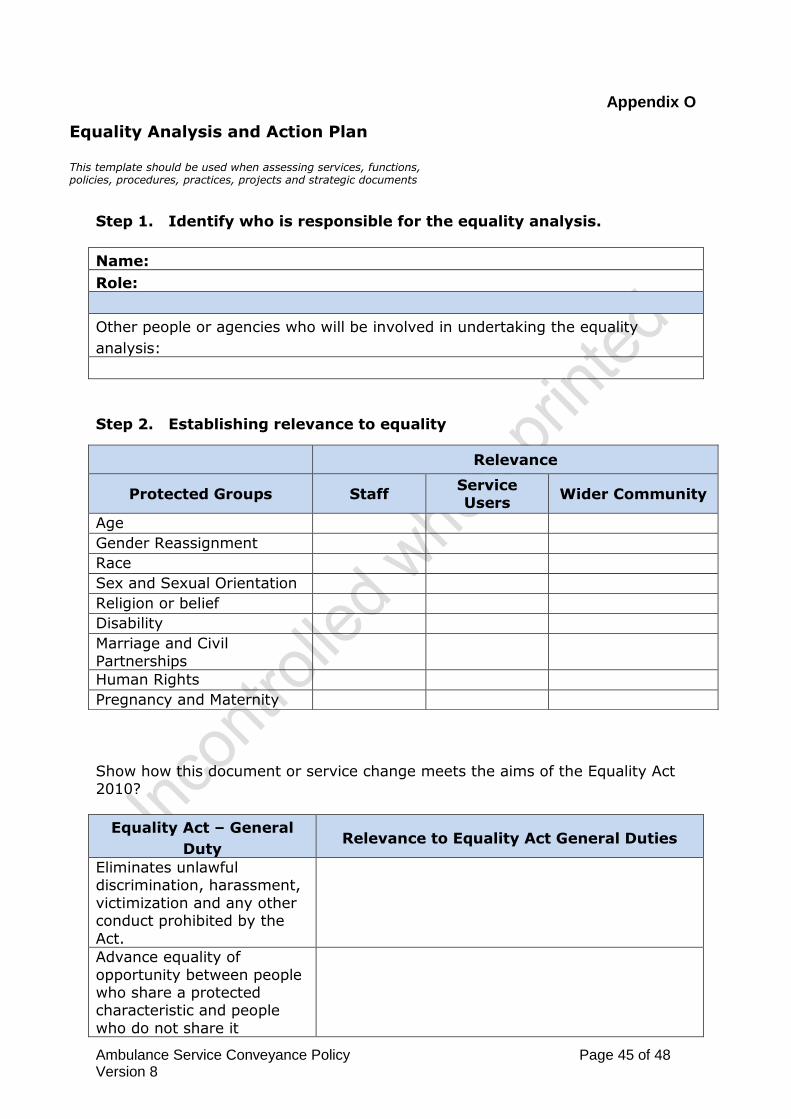
Ambulance Service Conveyance Policy Page 45 of 48 Version 8
Appendix O
Step 1. Identify who is responsible for the equality analysis.
Name:
Role:
Other people or agencies who will be involved in undertaking the equality
analysis:
Step 2. Establishing relevance to equality
Show how this document or service change meets the aims of the Equality Act 2010?
Equality Act – General
Duty Relevance to Equality Act General Duties
Eliminates unlawful discrimination, harassment,
victimization and any other conduct prohibited by the
Act.
Advance equality of
opportunity between people who share a protected characteristic and people
who do not share it
Relevance
Protected Groups Staff Service Users
Wider Community
Age Gender Reassignment Race Sex and Sexual Orientation Religion or belief Disability Marriage and Civil
Partnerships
Human Rights Pregnancy and Maternity
Equality Analysis and Action Plan This template should be used when assessing services, functions, policies, procedures, practices, projects and strategic documents

Ambulance Service Conveyance Policy Page 46 of 48 Version 8
Foster good relations between people who share a
protected characteristic and people who do not share it.
Step 3. Scope your equality analysis
Scope What is the purpose of this document or service
change?
Who will benefits? What are the expected outcomes?
Why do we need this
document or do we need to
change the service?
It is important that appropriate and relevant information is used about the different protected groups that will be affected by this document or service
change. Information from your service users is in the majority of cases, the most valuable.
Information sources are likely to vary depending on the nature of the document or service change. Listed below are some suggested sources of information
that could be helpful:
Results from the most recent service user or staff surveys. Regional or national surveys Analysis of complaints or enquiries
Recommendations from an audit or inspection Local census data
Information from protected groups or agencies. Information from engagement events.
Step 4. Analyse your information.
As yourself two simple questions:
What will happen, or not happen, if we do things this way?
What would happen in relation to equality and good relations?
In identifying whether a proposed document or service changes discriminates unlawfully, consider the scope of discrimination set out in the Equality Act 2010, as well as direct and indirect discrimination, harassment, victimization and
failure to make a reasonable adjustment.

Ambulance Service Conveyance Policy Page 47 of 48 Version 8
Findings of your analysis
Description Justification of your analysis No major change Your analysis
demonstrates that the proposal is robust and
the evidence shows no potential for discrimination.
Adjust your document or service change
proposals
This involves taking steps to remove
barriers or to better advance equality
outcomes. This might include introducing measures to mitigate
the potential effect.
Continue to implement
the document or service change
Despite any adverse
effect or missed opportunity to
advance equality, provided you can satisfy yourself it
does not unlawfully discriminate.
Stop and review Adverse effects that cannot be justified or
mitigated against, you should consider stopping the
proposal. You must stop and review if
unlawful discrimination is identified
5. Next steps.
5.1 Monitoring and Review.
Equality analysis is an ongoing process that does not end once the document has been published or the service change has been implemented.
This does not mean repeating the equality analysis, but using the
experience gained through implementation to check the findings and to make any necessary adjustments.
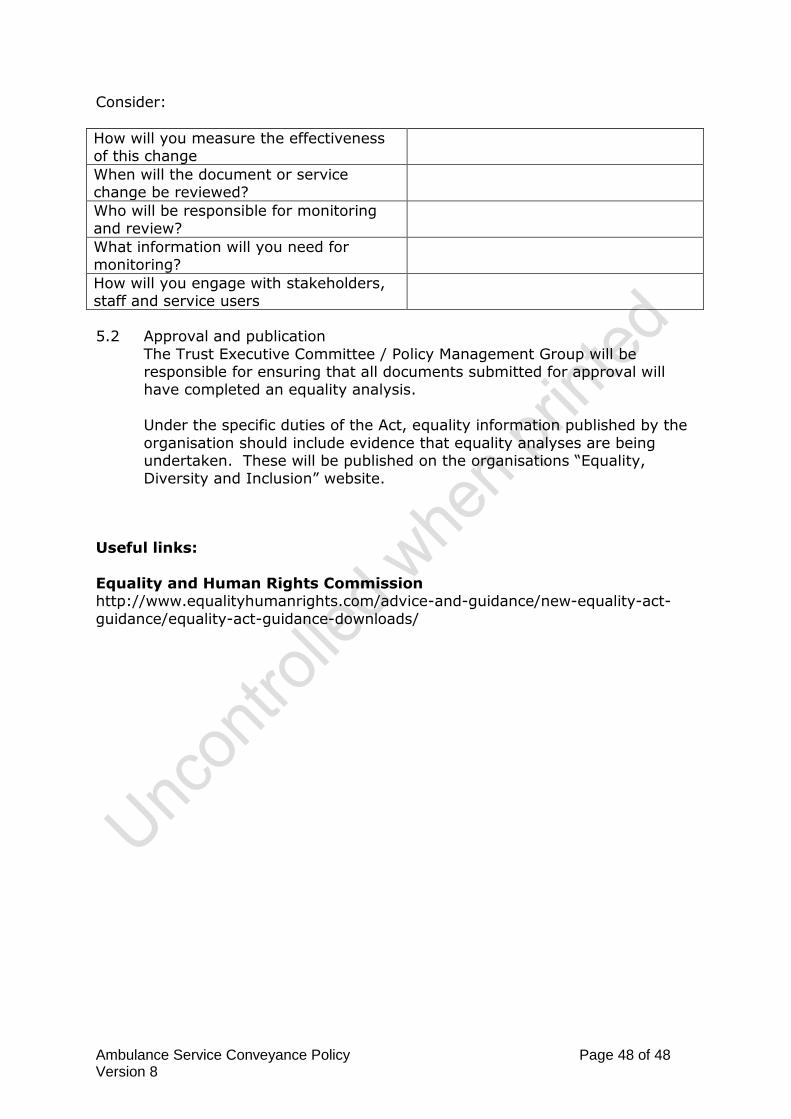
Ambulance Service Conveyance Policy Page 48 of 48 Version 8
Consider:
How will you measure the effectiveness of this change
When will the document or service change be reviewed?
Who will be responsible for monitoring and review?
What information will you need for monitoring?
How will you engage with stakeholders, staff and service users
5.2 Approval and publication
The Trust Executive Committee / Policy Management Group will be responsible for ensuring that all documents submitted for approval will have completed an equality analysis.
Under the specific duties of the Act, equality information published by the
organisation should include evidence that equality analyses are being undertaken. These will be published on the organisations “Equality, Diversity and Inclusion” website.
Useful links:
Equality and Human Rights Commission http://www.equalityhumanrights.com/advice-and-guidance/new-equality-act-
guidance/equality-act-guidance-downloads/