alzheimer disease developed by dr. june carroll, ms. shawna morrison and dr. judith allanson last...
TRANSCRIPT

Alzheimer disease
Developed by Dr. June Carroll, Ms. Shawna Morrison and Dr. Judith Allanson
Last updated April 2015

Disclaimer
• This presentation is for educational purposes only and should not be used as a substitute for clinical judgement. GEC-KO aims to aid the practicing clinician by providing informed opinions regarding genetic services that have been developed in a rigorous and evidence-based manner. Physicians must use their own clinical judgement in addition to published articles and the information presented herein. GEC-KO assumes no responsibility or liability resulting from the use of information contained herein.

Objectives• Following this session the learner will be able to:– Refer to their local genetics centre and/or order genetic
testing appropriately for Alzheimer disease (AD)– Discuss and address patient concerns regarding AD– Find high quality genomics educational resources
appropriate for primary care

Case 1
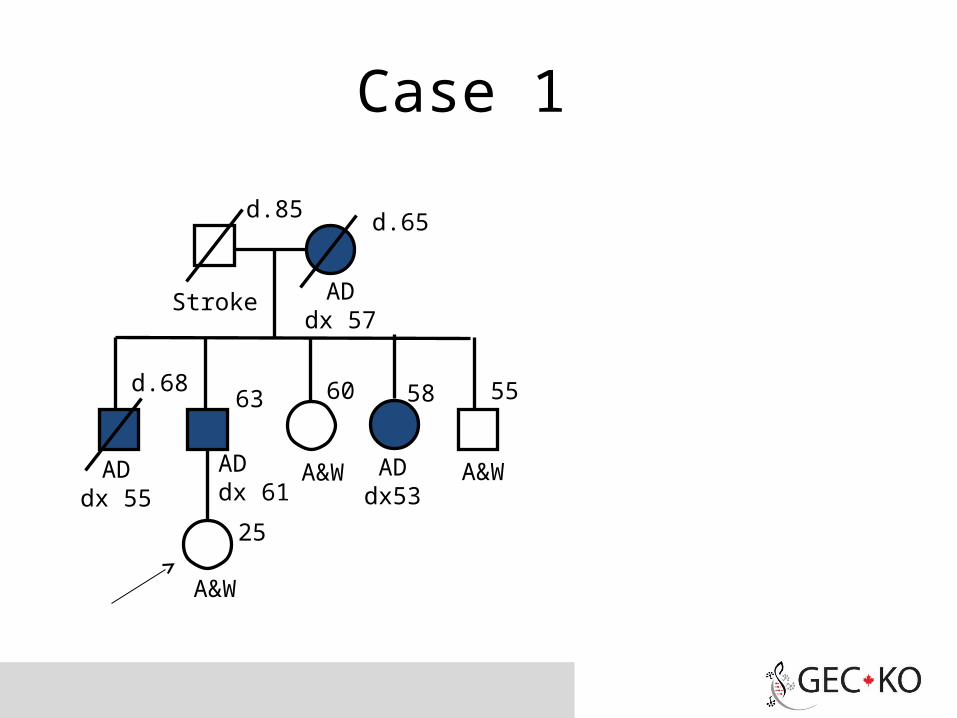
• Mary, 25yo female in good health
• Concerned about her risk of Alzheimer disease (AD) as her father’s condition is worsening quickly
ADdx 55
d.85
ADdx53
AD dx 61
25
d.65
ADdx 57
63 58 5560d.68
A&W A&W
A&W
Stroke

Case 2
• Mandy, 55yo female in good health
• Concerned about her risk of Alzheimer disease due to her father’s recent diagnosis
MI
ADdx 80
88 8690 75
55
80
d.87d.85
arthritis IDDM
A&W

Case 3
• Morgan, 55yo female in good health
• Concerned about her risk of Alzheimer disease due to her father’s recent diagnosis and family history
ADdx78
ADdx 80
d.88 8690 75
55
80
d.87d.85
AD dx83
IDDM
A&W

What is Alzheimer disease?• Alzheimer disease (AD) is an adult-onset progressive
dementia that gradually reduces a person’s memory and ability to learn, reason, make judgments, communicate and carry out daily activities. Individuals may also experience changes in personality and behaviour
• General population lifetime risk of developing dementia is 10-12%
Sporadic, late onset, unknown cause
Late-onset familial AD (LOAD)has a mean age of onset of >60-65years (15-25%)
Early-onset familial AD (EOAD) hasa mean age of onset < 60-65 years(<2%)
• Early-onset AD (EOAD) has an autosomal dominant inheritance pattern
• Three genes have been associated with EOAD:– amyloid precursor protein (APP)– presenilin 1 (PSEN1)– presenilin 2 (PSEN2)
• Each of these genes is involved in production of the amyloid ß (Aß) peptide, a major component of amyloid plaques
What do I need to know about the genetics of Alzheimer disease?
What do I need to know about the genetics of Alzheimer disease?
• Late-onset familial AD (LOAD) has been associated with apolipoprotein E (APOE)
• APOE is considered a risk modifier, especially APOE 4
• Approximately 1% of the general population are APOE 4 homozygotes (carry two copies of 4)
• Approximately 42% of persons with AD do NOT have an APOE 4 allele
• APOE 4 is neither necessary nor sufficient to cause LOAD
What do I need to know about the genetics of Alzheimer disease?
• Alzheimer disease (AD) develops due to a complex interaction between genetic and environmental factors
• With one affected first-degree relative, the risk of Alzheimer disease is approximately 20-25% (approximately double the population risk)
Who should be offered referral for genetic consultation?
Consider a genetics consult for:Patients with Alzheimer disease (AD) with onset <60-
65 yearsPatients with late-onset AD and multiple affected
close relativesClose relatives of the above two types of patientsA member of a family in which there is an identified
mutation in the APP, PSEN1 or PSEN2 genes
Who will be offered genetic testing and what do the test results mean?
• Genetic testing for Alzheimer disease (AD) is only available for a small number of families with early-onset AD (EOAD)– Testing likely to be initiated in a living affected
relative• If a gene mutation is found, other family members
are eligible for testing focused on the identified family mutation– Inheriting a mutation in APP, PSEN1 or PSEN2
gene causes early-onset Alzheimer disease (EOAD)

• Clinical testing is currently not available for late-onset AD (LOAD) or sporadic cases
• When there are multiple related affected individuals, research testing may be available
• APOE 4 testing is not recommended for risk assessment because of low sensitivity and specificity
• APOE 4 is neither necessary nor sufficient for the disease
Who will be offered genetic testing and what do the test results mean?

How will genetic testing help you and your patient?
• In the case of genetic testing for early-onset Alzheimer disease (EOAD), – A positive test result for a known family gene mutation
can result in:• Relief from uncertainty• An increased feeling of control• Opportunity to plan life decisions
– A negative test result for a known family gene mutation can result in:• Relief from fear of developing EOAD• Knowledge that children are not at risk for EOAD
Are there harms or limitations of genetic testing?
• Currently no cure or effective preventive therapy is available if a gene mutation is found
• In the case of genetic testing for early-onset Alzheimer disease (EOAD), – A positive test result for a known family gene mutation
can result in:• Adverse psychological reaction, family issues/distress• Insurance/job discrimination, confidentiality issues
– A negative test result for a known family gene mutation can result in survivor guilt
Case 1
ADdx 55
d.85
ADdx53
AD dx 61
25
d.65
ADdx 57
63 58 5560d.68
A&W A&W
A&W
Stroke

Case 1
• Family history is suggestive of early-onset AD (EOAD – dx<60-65y) and dominant inheritance pattern
• Offer referral for genetics consultation with option of genetic testing
ADdx 55
d.85
ADdx53
AD dx 61
25
d.65
ADdx 57
63 58 5560d.68
A&W A&W
A&W
Stroke

Case 2
MI
ADdx 80
88 8690 75
55
80
d.87d.85
arthritis IDDM
A&W

Case 2
• Family history is suggestive of sporadic AD
• Mandy’s AD risk is about 20-25% because of an affected FDR
• No referral to genetics indicated
MI
ADdx 80
88 8690 75
55
80
d.87d.85
arthritis IDDM
A&W

Case 3
ADdx78
ADdx 80
d.88 8690 75
55
80
d.87d.85
AD dx83
IDDM
A&W
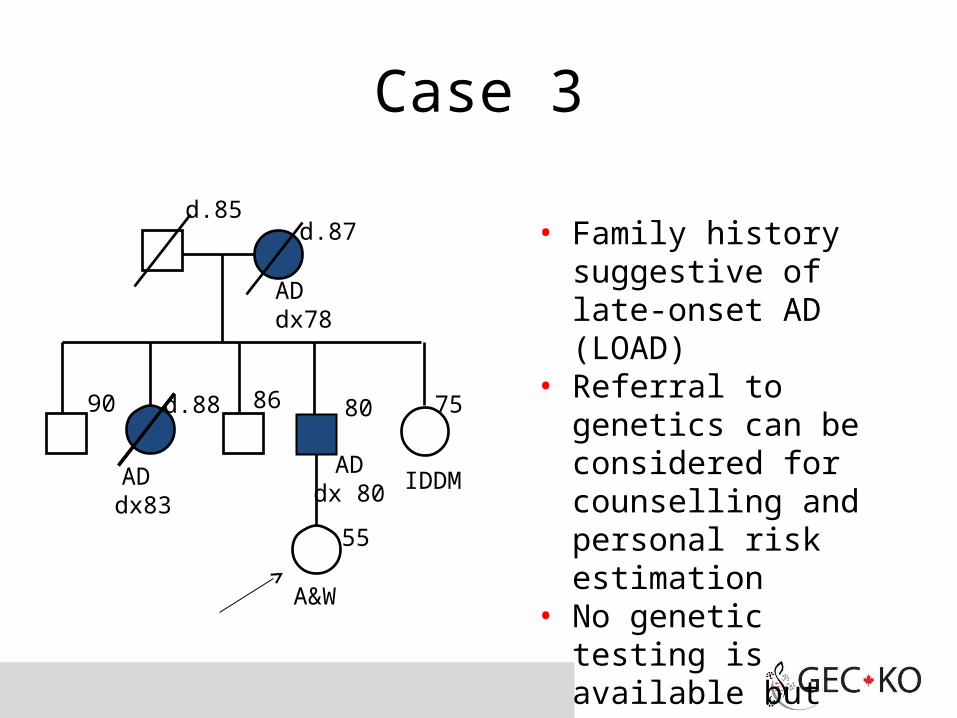
Case 3
• Family history suggestive of late-onset AD (LOAD)
• Referral to genetics can be considered for counselling and personal risk estimation
• No genetic testing is available but participation in research may be possible
ADdx78
ADdx 80
d.88 8690 75
55
80
d.87d.85
AD dx83
IDDM
A&W
Pearls
•Informative genetic testing is currently available to only a small number of families with early-onset (<60-65 years of age) Alzheimer disease (EOAD)
•Genetic testing is not possible for most cases of AD
•Apolipoprotein E gene variations alone cannot be used to predict risk of developing AD

References• Alonso Vilatela ME et al., Genetics of Alzheimer’s disease. Arch Med Res.
2012; 43(8): 622-31 and Goldman JS et al., Genetic counseling and testing for Alzheimer disease: Joint practice guidelines of the American College of Medical Genetics and the National Society of Genetic Counselors. Genet Med 2011; 13(6): 597-605
• American College of Medical Genetics/American Society of Human Genetics Working Group on APOE and Alzheimer's disease (1995) Statement on use of apolipoprotein E testing for Alzheimer's disease. JAMA 1995; 274(20): 1627-1629
• Bird TD. Alzheimer Disease Overview. 1998 Oct 23 [Updated 2014 Jan 30]. In: Pagon RA, Adam MP, Bird TD, et al., editors. GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2014. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1161/
• Genetics Education Project