altered skeletal muscle metabolic response to exercise...
TRANSCRIPT
1597
Altered Skeletal Muscle Metabolic Responseto Exercise in Chronic Heart Failure
Relation to Skeletal Muscle Aerobic Enzyme Activity
Martin J. Sullivan, MD; Howard J. Green, PhD; and Frederick R. Cobb, MD
Background. Exertional fatigue, which frequently limits exercise in patients with chronicheart failure, is associated with early anaerobic metabolism in skeletal muscle. The presentstudy was designed to examine the skeletal muscle metabolic response to exercise in thisdisorder and determine the relation of reduced muscle blood flow and skeletal musclebiochemistry and histology to the early onset of anaerobic metabolism in patients.Methods and Results. We evaluated leg blood flow, blood lactate, and skeletal muscle metabolic
responses (by vastus lateralis biopsies) during upright bicycle exercise in 11 patients withchronic heart failure (ejection fraction 21±8%) and nine normal subjects. In patientscompared to normal subjects, peak exercise oxygen consumption was decreased (13.0+3.3ml/kg/min versus 30.2 +8.6 ml/kg/min, p<0.01), whereas peak respiratory exchange ratio andfemoral venous oxygen content were not different (both p >0.25), indicating comparableexercise end points. At rest in patients versus normals, there was a reduction in the activity ofhexokinase (p=0.08), citrate sythetase (p<0.02), succinate dehydrogenase (p=0.0007), and3-hydroxyacyl CoA dehydrogenase (p=0.04). In patients, leg blood flow was decreased at rest,submaximal, and maximal exercise when compared to normal subjects (allp<0.05), and bloodlactate accumulation was accelerated. In patients, during submaximal exercise blood lactatelevels were not closely related to leg blood flow but were inversely related to rest citratesynthetase activity in skeletal muscle (r=-0.74, p<0.05). At peak exercise there were nointergroup differences in skeletal muscle glycolytic intermediates, adenosine nucleotides, or
glycogen, whereas in patients compared to normal subjects less lactate accumulation andphosphocreatine depletion were noted (both p<0.05), suggesting that factors other than themagnitude of phosphocreatine depletion or lactate accumulation may influence skeletal musclefatigue in this disorder.
Conclusions. The results of the present study suggest that in patients with chronic heartfailure reduced aerobic activity in skeletal muscle plays an important role in mediating theearly onset of anaerobic metabolism during exercise. Our findings are consistent with theconcept that reduced aerobic enzyme activity in skeletal muscle is, in part, responsible fordetermining exercise tolerance and possibly the response to chronic interventions in patientswith chronic heart failure. (Circulation 1991;84:1597-1607)
R ecent studies indicate that skeletal musclefatigue associated with early anaerobic me-
tabolism is the primary factor limiting exer-
cise tolerance in patients with chronic heart fail-ure.1-4Although skeletal muscle hypoperfusion likely
See p 1868
plays an important role in early lactate produc-tion,25-6 recent studies in our laboratory7 and oth-ers8,9 have identified reduced aerobic enzyme activityand an increased percentage of fast-twitch type lIbfibers in skeletal muscle in patients with chronicheart failure. These alterations have previously beenshown to be a potent stimulus for early anaerobic
From the Department of Medicine (M.J.S., F.R.C.), Division ofCardiology and the Center for Living, Duke University MedicalCenter and the Durham Veterans Administration Medical Center,Durham, N.C.; and the Department of Kinesiology (H.J.G.),University of Waterloo, Waterloo, Ontario, Canada.
Supported by grant HL-17670 from the National Heart, Lung,and Blood Institute, Bethesda, Md.; by General Medical ResearchFunds from the Veterans Administration Medical Center,Durham, N.C.; and by grant M01-RR-30, Division of ResearchResources, General Clinical Research Centers Program, NationalInstitutes of Health, Bethesda, Md. Dr. Sullivan is an EstablishedInvestigator of the American Heart Association and was sup-ported by a grant-in-Aid from the American Heart Associationand by a grant from the Bayer Cardiovascular Fund.Address for reprints: Martin J. Sullivan, MD, Duke University
Medical Center, Center for Living, PO Box 3022, Durham, NC 27710.Received October 2, 1990; revision accepted June 4, 1991.
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from
1598 Circulation Vol 84, No 4 October 1991
metabolism during exercise in animals'0"1 and innormal humans12'13 and may also play a role inmediating early lactate production in this disorder.This concept is supported by the findings of 31p_nuclear magnetic resonance (`P-NMR) studies byWeiner et al14 and Massie et al,1516 which havedemonstrated an abnormal metabolic response toarm exercise in this disorder that appears to beindependent of hemodynamic abnormalities. Al-though intrinsic skeletal muscle biochemical andhistological changes that may lead to early anaerobicmetabolism have been demonstrated in patients, therelation between these changes and the metabolicresponse to exercise in this disorder has not beenclearly defined.The present study was designed to examine the
skeletal muscle metabolic response to maximal up-right bicycle exercise in patients with chronic heartfailure and in normal subjects using direct biochem-ical analysis of rest and exercise biopsy samples of thevastus lateralis muscle. We have previously reportedthe rest skeletal muscle biochemical and histologicalcharacteristics, demographics, peak exercise oxygenconsumption (Vo2), and femoral venous blood lac-tate and oxygen saturation response to exercise in the11 patients and nine normal subjects who form thestudy groups in this report.7 This previous studydemonstrated that in patients compared to normalsubjects, skeletal muscle aerobic enzyme content andpercent composition of type I fibers were reduced,whereas glycolytic enzyme content was not changed.Although these skeletal muscle alterations in pa-tients may be largely due to chronic exercise decon-ditioning, it is possible that the heart failure stateitself may also contribute. The present study com-bines leg blood flow and blood lactate measurementsduring exercise and vastus lateralis biopsies at restand during exercise to examine the relation betweenhemodynamic and intrinsic skeletal muscle alter-ations in determining the metabolic response toexercise in this disorder. An important aim of thestudy was to evaluate muscle phosphagen, substratestores, and lactate content at peak exercise in pa-tients and normal subjects. This study also examinesthe relation of blood lactate levels to intramuscularlactate and phosphocreatine (PCr) in patients and innormal subjects.
MethodsEleven men with chronic heart failure due to left
ventricular systolic dysfunction (left ventricular ejec-tion fraction, 21±8%) participated in the study. Allsubjects were taking stable dosages of digoxin anddiuretics, and all were free of rales or peripheralbruits. Three subjects were chronically taking vasodi-lators (captopril, n=2; nitrates, n=1), and one wastaking an oral phosphodiesterase inhibitor (enoxi-mone). Patients were included only if limited primar-ily by general and/or leg fatigue during bicycle ergom-etry. The New York Heart Association functionalclassification of the patients was as follows: one was
class I, three were class II, six were class III, and onewas class IV. Nine healthy men volunteered to partic-ipate in the protocol. All had normal physical exami-nations and electrocardiographic responses to ascreening bicycle exercise study, and none was takingmedications. All studies were performed under aresearch protocol approved by the Institutional Re-view Boards at Duke University Medical Center andDurham Veterans Administration Medical Center.
Study ProtocolAll subjects underwent three maximal exercise
tests on a Fitron isokinetic bicycle in the uprightposition with the exercise work rate beginning at 150kilopond (kpm) per minute and increasing in3-minute stages of 150 kpm/min. During the first twoexercise studies, expired gases were measured con-tinuously in all subjects at rest and during exerciseusing a Sensormedics 4400 unit (Anaheim, Calif.).4"17Two to 14 days after a familiarization test, subjectsunderwent two identical exercise tests within a 10-day period. All vasodilators and phosphodiesteraseinhibitors were discontinued 48 hours prior to thesecond and third exercise tests. During the secondstudy, hemodynamic measurements and blood lac-tate levels were obtained, and during the third studyrest and exercise biopsies were obtained from thevastus lateralis muscle. During the second exercisesession, all normal subjects and 9 patients had abrachial artery cannula and a femoral venous cathe-ter (model 93a-105-5F, Edwards Laboratory, SantaAna, Calif.) inserted under local anesthesia 1 hourprior to exercise. Leg blood flow was measured atupright rest and two to four times during each workrate, using a bolus thermodilution technique as pre-viously described in our laboratory.5,17 At upright restand in the last minute of each work rate, arterial andfemoral venous blood samples were taken and imme-diately chilled in an ice bath. Oxygen content andsaturation were measured using a calibrated Instru-ments Laboratory 282 CO-Oximeter (Lexington,Mass.), and lactate concentration was analyzed usinga Calbiochem Behring rapid lactate kit (San Diego,Calif.). In all normal subjects and five patients,femoral venous blood was also analyzed for pH andPco2 (Instruments Laboratory, Lexington, Mass.).During the second exercise session, subjects per-
formed an identical exercise protocol and reached atleast the same peak work rate achieved during thehemodynamic exercise study. Before this exercise,biopsy sites on the anterior thigh were anesthetizedwith 2% xylocaine, and 0.5 -cm incisions were madethrough the skin and fascia lata. Biopsies of thevastus lateralis muscle were obtained using the mod-ified Bergstrom technique18 at rest, 3-8 seconds afteran interruption of exercise at a work rate represent-ing 55±13% of the peak work rate, and 3-8 secondsafter peak exercise. Biopsy samples were immedi-ately placed in liquid nitrogen and transferred to afreezer at -70°C. It was not technically possible toobtain both submaximal and maximal exercise biop-
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from

Sullivan et al Altered Skeletal Muscle Metabolic-Response to Exercise 1599
a-RestO-Submaximal Exercise0-Maximal Exercise
D
ECL
6-
41
- 40*
E 20-
0
0_-J 0~
i i20 40 60 80
Time Post
0gO~~~~
Ly---C> h~-
i p 'i
Q ==:-0
FIGURE 1. Skeletal muscle water content (%),ATP, creatinephosphate, and lactate (all mM/kgwet wt) from rest (open squares), submaximal(open circles), and maximal (open triangles)exercise with the time course before freezingshown on the horizontal axis.
20 40 60 80Biopsy (sec )
sies during this continuous exercise protocol in allsubjects. Submaximal exercise biopsies were not ob-tained in two normal subjects and in four patients,and maximal exercise biopsies were not obtained intwo patients. Biopsy samples were weighed, freeze-dried, and extracted according to the method ofHarris et al.19 Creatine, PCr, inorganic phosphate,glycogen, glucose, glucose-i-phosphate, glucose-6-phosphate, fructose-6-phosphate, and lactate wereanalyzed fluorometrically using methods as previ-ously described.7,20 Adenosine triphosphate (ATP)and adenosine diphosphate (ADP) were determinedusing high-pressure liquid chromatography.7'20
In a preliminary study, we examined the effects ofthe time duration between obtaining the skeletalmuscle biopsy and the freezing of samples on bio-chemical determinations of muscle metabolism. Weobtained biopsies of the vastus lateralis at rest, atsubmaximal, and at maximal bicycle exercise in twonormal subjects; the biopsies were then divided andplaced in liquid nitrogen after delaying freezing by0-70 seconds. Figure 1 illustrates the stability ofmeasurements of water content, ATP, PCr, andlactate with variations in time to freezing. Our resultsare consistent with previous studies by Soderlundand Hultman21 in demonstrating that determinationof skeletal muscle metabolism by biopsy and directbiochemical analysis is not significantly influenced byshort delays in freezing specimens. To examine theday-to-day reproducibility of rest and exercise skele-tal muscle biochemical analysis from biopsies in ourlaboratory, three normal subjects underwent identi-cal exercise studies on two separate days with biop-sies obtained at rest, at identical submaximal workrates, and at maximal exercise. Regression of pairedrest and exercise measurements of PCr, lactate, ATP,and glycogen demonstrated good day-to-day repro-ducibility (all r>0.75, p<0.01), with the slope of thederived regression equations not different from theline of identity (Figure 2).
Statistical AnalysisIntergroup and intragroup comparisons were per-
formed using unpaired and paired Student's t testswhere appropriate. To determine the relation ofvariables, linear regression analysis was performedusing the least squares method. Probability valuesless than 0.05 were considered statistically significant.All data are presented as mean+SD.
ResultsAlthough in patients (PT) versus normals (NL)
there were minor differences in age (PT, 59+13versus NL, 49+ 12 years;p=0.10), weight (PT, 69+ 12kg versus NL, 77+6 kg, p=0.10), and surface area(PT, 1.79+0.16 m2 versus NL, 1.90±+0.10 m2;p=0.08),these differences did not reach statistical signifi-
LACTATE0.8 r 0.94 5 Y=X
SE = .09 0
0.6o0
0.4
0
0.2
0.1 0.3 0.5 0.7
CREATINE PHOSPHATE
r = 0.78 y=x.11
0.6 0
0.4 o
o
0.20
0.1 0.3 0.6 0.7
,iM/±£M CREATINEDay 1
FIGURE 2. Day-to-day reproducibility of skeletal musclebiochemistry at rest and during exercise in three normalsubjects. r=correlation coefficient, SE=standard error.
801
011-
(-
U)0
:z70
0
cnL 3rx 20CL -,ho
_ E 10
2(U)
ATP
0.3 - r = 0.80 y=xSE =.04
0.2_ 0
0
0.1 yWz
< c 0.1 0.2 0.3
oc GLYCOGEN3- r=0.76 0
SE =.06
02
1 2
1 2-L
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from

1600 Circulation Vol 84, No 4 October 1991
TABLE 1. Rest and Exercise Hemodynamic and Metabolic Parameters in Patients and Normal Subjects
Upright rest 300 kpm/min Peak exercise
Variable Patients Subjects Patients Subjects Patients Subjects
HR (beats/min) 84+ 17 75+10 109+20 100±+14 121±25t 168+14RER 0.91+0.08 0.89+0.07 1.22±0.11t 0.90±0.07 137+0.14 1.31±0.09LBF (1/min) 0.3±0.1* 0.4+0.2 1.4±0.5t 2.4±0.3 1.8±1.1t 6.2±+1.4FVo2ST(%) 38+16* 55±12 24+9±t 37+4 22+9 27+6FVo2CT (ml/dl) 8.0±3.8* 11.8±2.4 4.7±2.6* 8.0±1.3 4.5±2.3 5.9±1.5FLAC (mM/1) 1.1±0.7 0.9±0.5 4.2±1.5t 1.7+0.7 7.6±3.2: 12.3+3.1ARTLAC (mM/1) 0.8+0.7 0.8±0.5 2.9+ 1.04: 1.4+0.7 5.3+1.64: 9.9±3.5LAVL (mM/1) 0.2+0.3 0.2+0.2 1.3+1.0* 0.3+0.2 2.7±2.0 2.4+2.5PLLA (mM/min) 0.1±0.1 0.1+0.1 1.9+1.5 0.8±0.4 5.8±6.3 13.0+12.7FVpH 7.36+0.01 7.35±0.03 7.25±0.05* 7.30±0.03 7.25+0.06* 7.15+0.07FVPco2 (mm/Hg) 45±4 43+3 52±4* 42±3 59±7 57±6
HR, heart rate; RER, respiratory exchange ratio; LBF, single leg blood flow; FVo2ST, femoral venous oxygensaturation; FVo2CT, femoral venous oxygen content; FLAC, femoral venous lactate concentration; ARTLAC, arteriallactate; LAVL, femoral venous arterial lactate difference; PLLA, leg production of lactate; FVpH, femoral venous pH;FVPco2, femoral venous Pco2.
*p<0.05, tp<0.001, 4:p<0.01 patients vs. normals.
cance. Table 1 summarizes the hemodynamic andmetabolic response to exercise in patients and nor-mals. There was no difference in blood hemoglobin atrest in patients when compared with normal subjects(PT, 14.6+ 2.4 versus NL, 15.3 +0.8 g/dL;p= 0.54). Atpeak exercise in patients compared with normals,Vo2 was decreased (PT, 13.0+3.3 versus NL,30.2±+8.6 ml/kg/min;p<0.001). There were no inter-group differences in peak respiratory exchange ratios(PT, 1.37+0.14 versus NL, 1.31±0.09, p=0.25) orfemoral venous oxygen saturation (PT, 21+±9% ver-sus NL, 27±6%;p=0.20). It is important to note thatboth patients and normals were coached to exerciseuntil general exhaustion or leg fatigue limited workoutput and that the peak respiratory exchange ratiosreported indicate a comparable maximal or near-maximal exercise effort in both groups. In patients,leg blood flow was reduced at rest and during exer-cise and was accompanied by reduced femoral ve-nous oxygen content and saturation at rest andduring submaximal exercise. Arterial lactate, femoralvenous lactate, and the femoral venoarterial lactatedifference were comparable in the groups at rest, butall were increased in patients versus normals at 300kpm/min. At peak exercise both femoral venous andarterial lactate levels were lower in patients versusnormals. Leg production of lactate was no differentat rest or at maximal exercise but tended to be higherin patients at 300 kpm/min (p<0.07). There were nointergroup differences in femoral venous pH andPco2 at rest; however, femoral venous pH was de-creased at 300 kpm/min in patients but was higherthan normals at peak exercise. It should be notedthat of the five patients who had femoral venousblood gas measurements, four completed only the300 kpm/min work rate. Femoral venous Pco2 washigher in patients at 300 kpm/min but was notdifferent from normals at peak exercise.
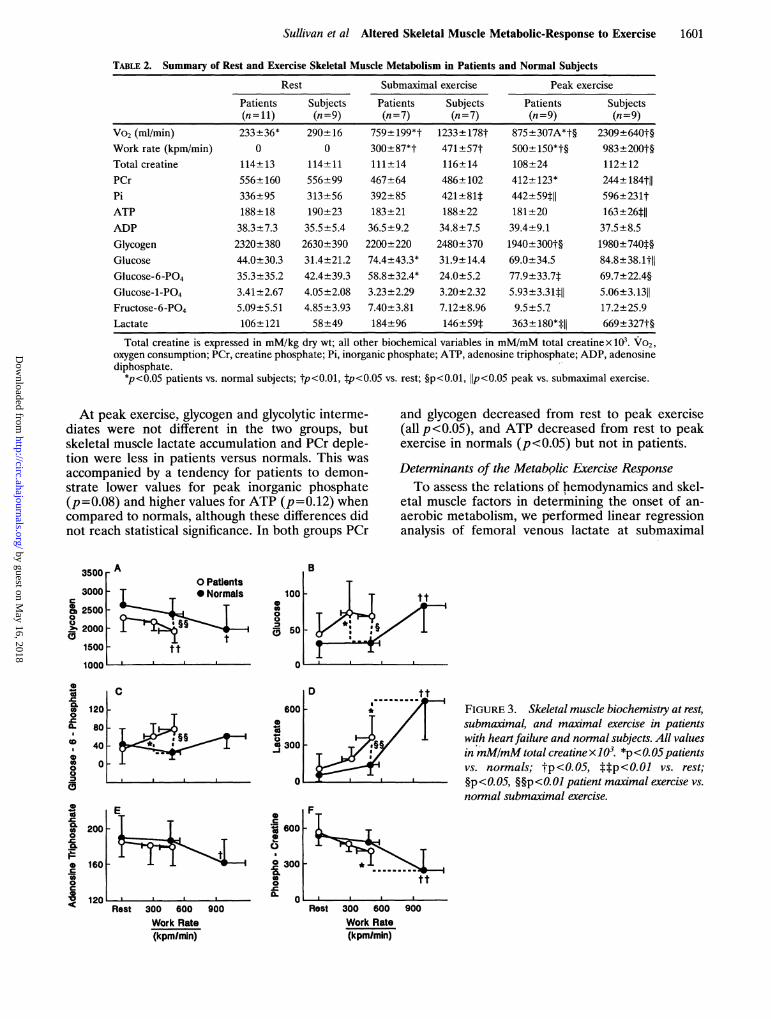
Skeletal Muscle Metabolic ResponseTable 2 and Figure 3 summarize muscle biochemical
analyses at rest and during exercise in patients andnormals. Submaximal biopsies were obtained at300±87 kpm/min in seven patients and at 471+57kpm/min in seven normal subjects (p<O.01). Althoughin patients versus normals this represented a similarpercent of the peak exercise work rate (PT, 57+14%versus NL, 53+14%,p=0.51), the percent of peak Vo2was different (PT, 76+9% versus NL, 60+12%;p<0.05). At rest, glycogen content tended to be slightlylower in patients (p=0.08). At submaximal exercise,PCr, inorganic phosphate, ATP, and ADP were notdifferent in the two groups. At submaximal exerciseglycogen tended to be slightly lower in patients, but thisdifference did not reach statistical significance(p=0.11), and glucose and glucose-6-phosphate wereincreased in patients compared to normals. Althoughthese submaximal measures were performed at differ-ent relative percentages of peak Vo2 in the two groups,the results indicate that accumulation of glucose andglucose-6-phosphate occurred in patients at levels ofexercise that would be encountered during routinedaily activities in normal subjects.To compare the rate of change of skeletal muscle
metabolism in relation to absolute work rate, maxi-mal data from patients were compared to the sub-maximal data from normals. The maximal work rateof patients (500±150 kpm/min) was similar to thesubmaximal work rate at which biopsies were ob-tained in normal subjects (471+57 kpm/min,p=0.61). Although phosphagens and adenosine nu-cleotides were not different in the two groups, inpatients versus normals, glycogen was decreasedwhereas glycolytic intermediates and lactate wereincreased (see Figure 3). Thus, glycolysis and glyco-genolysis were accelerated in relation to absolutework rate in patients.
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from
Sullivan et al Altered Skeletal Muscle Metabolic-Response to Exercise 1601
TABLE 2. Summary of Rest and Exercise Skeletal Muscle Metabolism in Patients and Normal Subjects
Vo2 (m/min)Work rate (kpm/min)Total creatinePCrPiATPADPGlycogenGlucoseGlucose-6-PO4Glucose-1-PO4Fructose-6-PO4Lactate
Rest
Patients Subjects(n=11) (n=9)233+36* 290+16
0 0114+13 114±11556+ 160 556±99336±95 313±56188±18 190±2338.3±7.3 35.5±5.42320±380 2630±39044.0±30.3 31.4±21.235.3±35.2 42.4±39.33.41±2.67 4.05±2.085.09±5.51 4.85±3.93106±121 58±49
Submaximal exercise
Patients Subjects(n=7)
759±+199*t300±87*t111±+14467±64392±85183+2136.5±9.22200±22074.4+43.3*58.8±32.4*3.23±2.297.40+3.81184±96
(n=7)
1233±178t471 ±57t116+ 14486±102421±81t188±2234.8±7.52480±37031.9±14.424.0±5.23.20±2.327.12±8.96146±59t
Peak exercise
Patients Subjects(n=9) (n=9)
875±+307A*t§ 2309+640t§500±+150*t§ 983±200t§108+24 112± 12412± 123* 244±184th442±59til 596±231t181±20 163±26t1139.4±9.1 37.5±8.51940±300t§ 1980±7401§69.0±34.5 84.8±38.1t77.9±33.7t 69.7+22.4§5.93±3.3111 5.06±3.13119.5±5.7 17.2±25.9363+180*111 669±327t§
Total creatine is expressed in mM/kg dry wt; all other biochemical variables in mM/mM total creatinex 10. VO2,oxygen consumption; PCr, creatine phosphate; Pi, inorganic phosphate; ATP, adenosine triphosphate; ADP, adenosinediphosphate.
*p<0.05 patients vs. normal subjects; tp<0.01, Ip<0.05 vs. rest; §p<0.01, 1Ip<O.OS peak vs. submaximal exercise.
At peak exercise, glycogen and glycolytic interme-diates were not different in the two groups, butskeletal muscle lactate accumulation and PCr deple-tion were less in patients versus normals. This wasaccompanied by a tendency for patients to demon-strate lower values for peak inorganic phosphate(p=0.08) and higher values for ATP (p =0.12) whencompared to normals, although these differences didnot reach statistical significance. In both groups PCr
A
CDCD002%
0
0
000.p
Jr.
CLCDI
and glycogen decreased from rest to peak exercise(all p<0.05), and ATP decreased from rest to peakexercise in normals (p<0.05) but not in patients.
Deterninants of the Metabolic Exercise ResponseTo assess the relations of hemodynamics and skel-
etal muscle factors in determining the onset of an-aerobic metabolism, we performed linear regressionanalysis of femoral venous lactate at submaximal
B
00
-
0
s0
a 1
00
00CL
Rest 300 600 900Work Rate(kpm/min)
FIGURE 3. Skeletal muscle biochemistry at rest,submaximal, and maximal exercise in patientswith heartfailure and normal subjects. All valuesinmM/mM totalcreatinex103. *p<OO5patientsvs. normals; tP<O.OS, t*p<0.01 vs. rest;§p< 0.05, §§p<O. 01 patient maximal exercise vs.normal submaximal exercise.
Rest 300 600 900Work Rate(kpmlmin)
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from
1602 Circulation Vol 84, No 4 October 1991
8 or = -0.34
6 - pa0.37
4-_40~~0
2
0 ,a .0.5 1.0 1.5 2.0 2.5
Leg Blood Flow (1/min)
0
Br a -0.45p = 0.22o
00 0
8 ° r=0.35
6 - p c 0.36
4
° o°2
10 20 30 40 50Femoral Venous 02 Saturation (%)
r = -0.74pa 0.02
FIGURE 4. Relations of leg blood flow, fem-oral venous oxygen saturation, skeletal musclecapillary density, and citrate synthetase tofemoral venous blood lactate at 300 kpm/minin patients with chronic heart failure.r=correlation coefficient.
-0
0.5 1.0 1.5 2.0 2.5Skeletal Muscle Ctrate Synthetase
(pMIg protein)
exercise with rest skeletal muscle biochemistry andhistology and hemodynamic data at the correspond-ing work rate. Exercise work rates of 300 kpm/minwere chosen in patients and 600 kpm/min in normalsubjects, although similar results were obtained at150 kpm/min and 450 kpm/min in the two groups,
10 ~~~~~tt10 A
8 **
tU 6 tt
0 Patients'2 -
O2 _* Normals
0Rest 300 600 900
respectively. In patients, femoral venous lactate lev-els at 300 kpm/min were significantly inversely corre-lated with citrate synthetase (r= -0.74, p<0.05) (Fig-ure 4) and succinate dehydrogenase activity(r= -0.67, p<0.05) but were not significantly corre-lated with leg blood flow or femoral venous oxygen
0
12 B tt
cu10
CO~ 8
t-
0 2
E0
ITLL.nest iuU 6UU 9UU
0
<xs 20
0 1
0
0
K 10
_v _
CD
c
0
10L.0
CO0
to_i
Rest 300 600 900 Rest 300 600 900Work Rate (kpm/min) Work Rate (kpm/min)
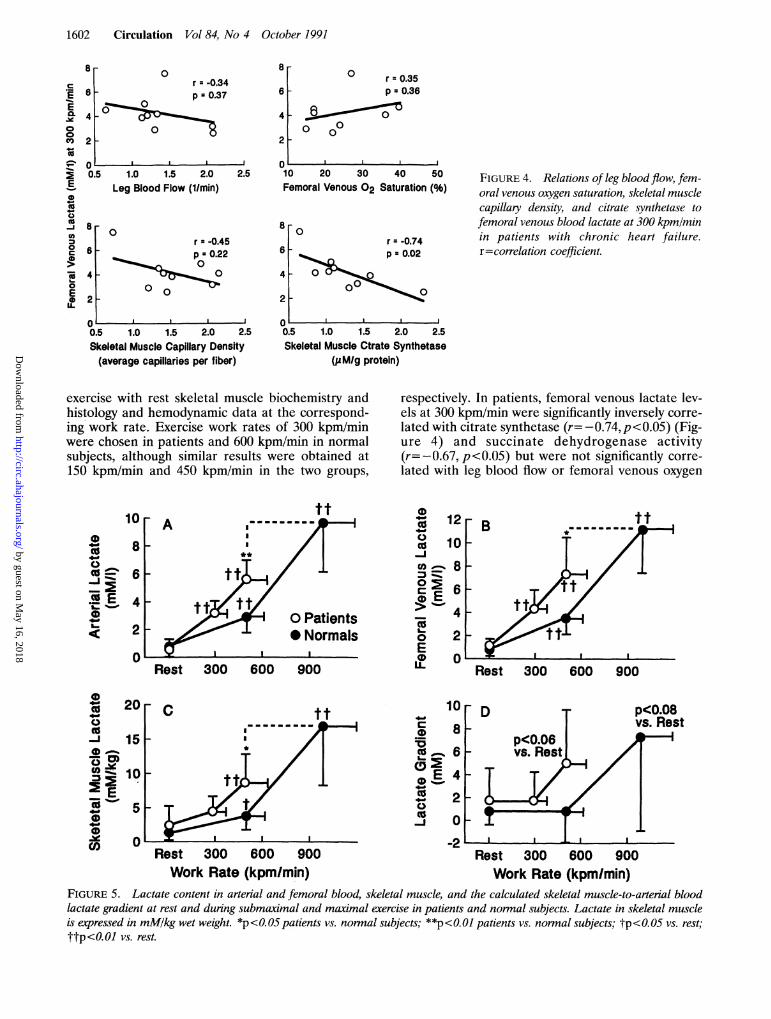
FIGURE 5. Lactate content in arterial and femoral blood, skeletal muscle, and the calculated skeletal muscle-to-arterial bloodlactate gradient at rest and during submaximal and maximal exercise in patients and normal subjects. Lactate in skeletal muscleis expressed in mM/kg wet weight. *p<O.O5 patients vs. normal subjects; **p<O.Ol patients vs. normal subjects; tp<0.05 vs. rest;
ttp<0.0l vs. rest.
c
EE
0o00
0
0
0-J
iv0te
C0
0
0.5 1.0 1.5 2.0 2.5Skeletal Muscle Capillary Density(average capillaries per fiber)
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from

Sullivan et al Altered Skeletal Muscle Metabolic-Response to Exercise
saturation, fiber typing, rest glycogen content, glyco-lytic enzyme activity, capillary density, or hexokinaseactivity. In normal subjects, femoral venous lactatelevels at 600 kpm/min were significantly inverselycorrelated with the corresponding leg blood flow(r=-0.76, p<0.05), succinate dehydrogenase(r=-0.76, p<0.05) and citrate synthetase activity(r=-0.61, p=0.08), and rest glycogen content(r= -0.64, p=0.06) but were not significantly corre-lated with femoral venous oxygen saturation, glyco-lytic enzyme activity, or capillary density. In patients,peak Vo2 was significantly correlated with succinatedehydrogenase activity (r=0.68,p<0.05), citrate syn-thetase activity (r=0.54, p=0.08), and average fibersize (r=0.77, p<0.01) but was unrelated to relativefiber typing, glycogen content, glycolytic enzyme ac-tivity, or capillary density. Peak leg blood flow was
significantly correlated with citrate synthetase activityin both groups (both r>0.77, p<0.05). In normalsubjects, peak Vo2 was related to citrate synthetaseactivity (r=0.81, p<0.01) but was unrelated to glyco-lytic enzyme activity, glycogen content, fiber size,relative fiber composition, or capillary density.
Relation ,)fBlood to Muscle Lactate in Patients andNormal Subjects
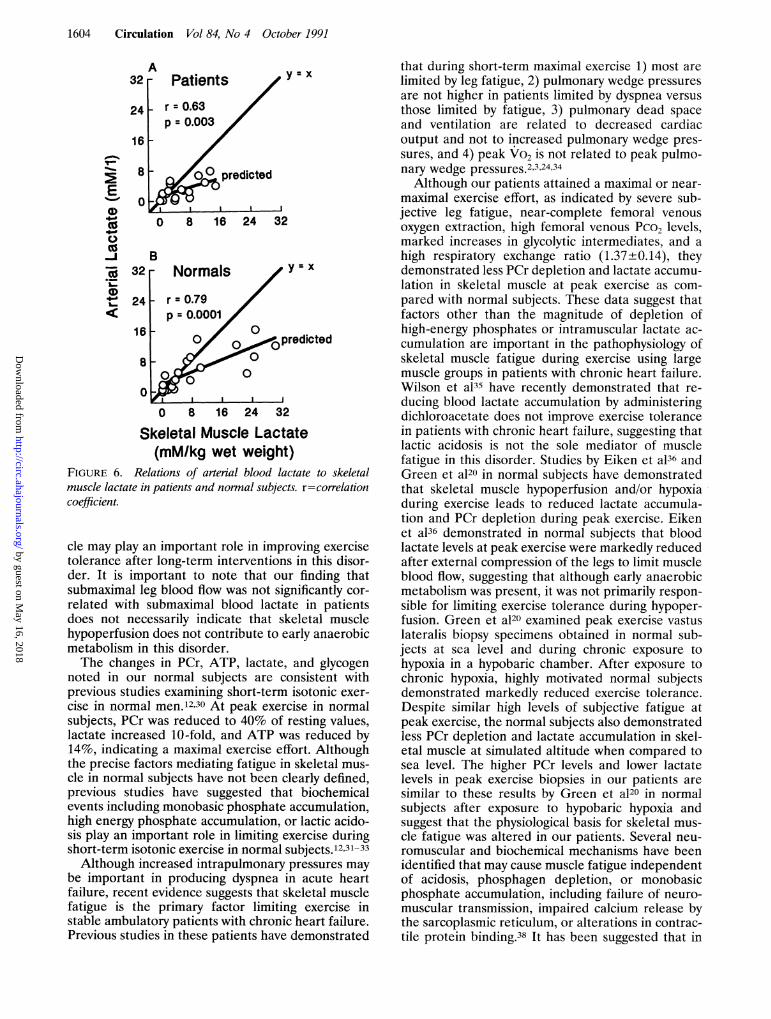
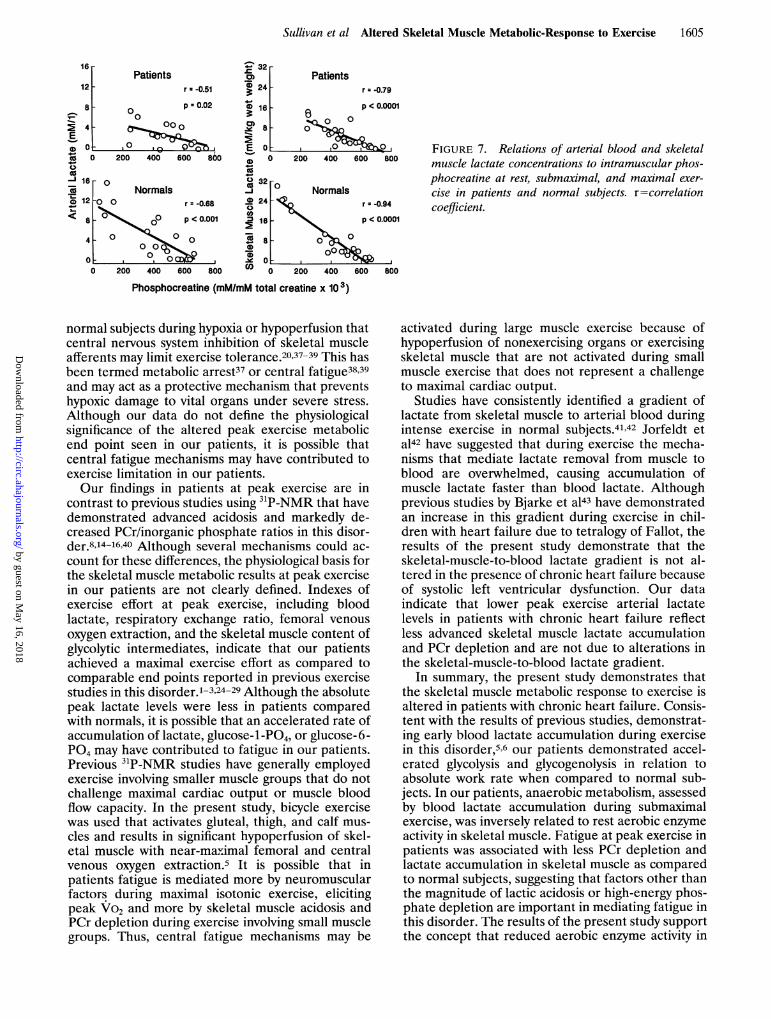
Figure 5 illustrates blood and muscle lactate dataat rest and during exercise in the two groups. Lactatetended to be higher in skeletal muscle when com-pared to femoral venous or arterial blood in bothgroups at maximal exercise (both p<0.08), althoughthese differences did not reach statistical signifi-cance. There were no differences in the calculatedgradients of skeletal muscle to femoral venous orarterial blood lactate in the two groups at rest,submaximal, or maximal exercise. Figure 6 demon-strates the relation of arterial lactate to skeletalmuscle lactate at rest and during exercise in patientsand normal subjects. In both groups, the predictedslope is less than unity, indicating that as arteriallactate levels increase so does the muscle-to-arterialblood lactate gradient. Figure 7 illustrates the rela-tion of arterial lactate to skeletal muscle lactate andPCr in patients and normals. Arterial lactate andskeletal muscle lactate were inversely significantlycorrelated with skeletal muscle PCr in both groups.Although the derived intercept was higher and theslope steeper in normals, similar relations of thesetwo variables with PCr were noted in the range ofPCr and lactate seen in patients, suggesting similarmuscle buffer capacity for lactate in skeletal musclein the two groups.
DiscussionThe present study demonstrates important differ-
ences in the skeletal muscle metabolic response tosubmaximal and maximal upright exercise in patientswith chronic heart failure when compared to normalsubjects. Our finding that glycolysis and glycogen-olysis were accelerated in relation to absolute workrate in patients is consistent with previous studies
evaluating the blood lactatel25 and the 31P-NMRresponse8J5'6 to exercise in this disorder. Our resultsextend these observations by demonstrating that ox-idative enzyme activity in skeletal muscle was in-versely related to blood lactate accumulation duringsubmaximal exercise in patients and support theconcept that reduced skeletal muscle aerobic enzymeactivity plays a role in determining the metabolicresponse to exercise in patients with chronic heartfailure. In addition to examining the determinants ofthe skeletal muscle metabolic response to exercise,the present study demonstrates that during peakbicycle exercise, skeletal muscle PCr depletion andlactate accumulation were less in patients versusnormals despite attaining comparable respiratory ex-change ratios and near complete oxygen extraction inworking skeletal muscle. Although these data do notdelineate the mechanisms responsible for fatigue inpatients, our results suggest that the magnitude ofPCr depletion or lactic acidosis in skeletal musclemay not be the primary factors underlying earlymuscle fatigue in patients with chronic heart failure.Our finding that blood lactate accumulation at a
given work rate was inversely related to aerobicenzyme activity is consistent with previous studiesthat have suggested that aerobic enzyme content isan important determinant of lactate production dur-ing exercise in humans'1'222 and animals.101 Al-though Mancini et a18 did not demonstrate a relationbetween skeletal muscle biochemical alterations andexercise metabolism in this disorder, our data areconsistent with previous studies by Drexler et a123that have demonstrated a relation between ultra-structural alterations in skeletal muscle and peak Vo2in patients with chronic heart failure. Several lines ofevidence are consistent with this concept that intrin-sic skeletal muscle alterations play a role in deter-mining exercise tolerance in this disorder. A numberof studies24-26 have consistently demonstrated norelation between peak Vo2 and resting left ventricu-lar ejection fraction in patients. Acute administrationof vasodilators or inotropic agents do not increasepeak Vo2 despite immediate improvements in centralhemodynamics24 and leg blood flow.28'29 However,chronic vasodilator therapy with nitrates or angioten-sin converting enzyme inhibitors may improve peakVo2 after a period of weeks or months, suggestingthat peripheral training-like effects may play a role inthis response.24 A recent study by Drexler et a129 hasdemonstrated that chronic therapy with an angioten-sin converting enzyme inhibitor improves peak Vo2and is accompanied by increased femoral venousoxygen extraction during peak exercise. Previousstudies in our laboratory17 have demonstrated thatexercise training in this disorder decreases bloodlactate levels during submaximal exercise and im-proves endurance exercise without altering submaxi-mal exercise cardiac output or leg blood flow. Ourfindings after exercise training17 and those of Drexleret a129 after chronic vasodilator therapy suggest thatincreases in aerobic enzyme activity in skeletal mus-
1603
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from
1604 Circulation Vol 84, No 4 October 1991
32A
241h
161
00,1
-
-
cu
L._CO
8
0
- Patients y
-r = 0.63p = 0.003
pr 00cpredicted
0 8 16 24 32
B32 r
24
16
8
0
= X
- Normals y=x
- r=0.79p = 0.0001
00 0predicted0
00 0
1 1 10 8 16 24 32
Skeletal Muscle Lactate(mM/kg wet weight)
FIGURE 6. Relations of arterial blood lactate to skeletalmuscle lactate in patients and normal subjects r=correlationcoefficient.
cle may play an important role in improving exercisetolerance after long-term interventions in this disor-der. It is important to note that our finding thatsubmaximal leg blood flow was not significantly cor-related with submaximal blood lactate in patientsdoes not necessarily indicate that skeletal musclehypoperfusion does not contribute to early anaerobicmetabolism in this disorder.The changes in PCr, ATP, lactate, and glycogen
noted in our normal subjects are consistent withprevious studies examining short-term isotonic exer-cise in normal men.12,30 At peak exercise in normalsubjects, PCr was reduced to 40% of resting values,lactate increased 10-fold, and ATP was reduced by14%, indicating a maximal exercise effort. Althoughthe precise factors mediating fatigue in skeletal mus-cle in normal subjects have not been clearly defined,previous studies have suggested that biochemicalevents including monobasic phosphate accumulation,high energy phosphate accumulation, or lactic acido-sis play an important role in limiting exercise duringshort-term isotonic exercise in normal subjects.12'3'-33Although increased intrapulmonary pressures may
be important in producing dyspnea in acute heartfailure, recent evidence suggests that skeletal musclefatigue is the primary factor limiting exercise instable ambulatory patients with chronic heart failure.Previous studies in these patients have demonstrated
that during short-term maximal exercise 1) most arelimited by leg fatigue, 2) pulmonary wedge pressuresare not higher in patients limited by dyspnea versusthose limited by fatigue, 3) pulmonary dead spaceand ventilation are related to decreased cardiacoutput and not to increased pulmonary wedge pres-sures, and 4) peak Vo2 is not related to peak pulmo-nary wedge pressures.2,3,24,34Although our patients attained a maximal or near-
maximal exercise effort, as indicated by severe sub-jective leg fatigue, near-complete femoral venousoxygen extraction, high femoral venous Pco2 levels,marked increases in glycolytic intermediates, and ahigh respiratory exchange ratio (1.37±0.14), theydemonstrated less PCr depletion and lactate accumu-lation in skeletal muscle at peak exercise as com-pared with normal subjects. These data suggest thatfactors other than the magnitude of depletion ofhigh-energy phosphates or intramuscular lactate ac-cumulation are important in the pathophysiology ofskeletal muscle fatigue during exercise using largemuscle groups in patients with chronic heart failure.Wilson et a135 have recently demonstrated that re-ducing blood lactate accumulation by administeringdichloroacetate does not improve exercise tolerancein patients with chronic heart failure, suggesting thatlactic acidosis is not the sole mediator of musclefatigue in this disorder. Studies by Eiken et a136 andGreen et a120 in normal subjects have demonstratedthat skeletal muscle hypoperfusion and/or hypoxiaduring exercise leads to reduced lactate accumula-tion and PCr depletion during peak exercise. Eikenet a136 demonstrated in normal subjects that bloodlactate levels at peak exercise were markedly reducedafter external compression of the legs to limit muscleblood flow, suggesting that although early anaerobicmetabolism was present, it was not primarily respon-sible for limiting exercise tolerance during hypoper-fusion. Green et a120 examined peak exercise vastuslateralis biopsy specimens obtained in normal sub-jects at sea level and during chronic exposure tohypoxia in a hypobaric chamber. After exposure tochronic hypoxia, highly motivated normal subjectsdemonstrated markedly reduced exercise tolerance.Despite similar high levels of subjective fatigue atpeak exercise, the normal subjects also demonstratedless PCr depletion and lactate accumulation in skel-etal muscle at simulated altitude when compared tosea level. The higher PCr levels and lower lactatelevels in peak exercise biopsies in our patients aresimilar to these results by Green et a120 in normalsubjects after exposure to hypobaric hypoxia andsuggest that the physiological basis for skeletal mus-cle fatigue was altered in our patients. Several neu-romuscular and biochemical mechanisms have beenidentified that may cause muscle fatigue independentof acidosis, phosphagen depletion, or monobasicphosphate accumulation, including failure of neuro-muscular transmission, impaired calcium release bythe sarcoplasmic reticulum, or alterations in contrac-tile protein binding.38 It has been suggested that in
r
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from
Sullivan et al Altered Skeletal Muscle Metabolic-Response to Exercise 1605
16Patients
12 - r--0.51
8 0 p =0.02
s4 c o000
aD)0 000 200 400 600 860
0
_< Normals0 12 -00 r -0.68
< 8 00p° < 0.001
4 - 00 O000
0 00 00 200 400 600 800
- 32CD PatientsD 24 r = -0.79
(D 16 p < 0.0001
as
CD 0 0
E2 - 0
0 200 400 600 800
32-
Normals
024 -r =-0.94
U)16 p <0.0001
0s 8 - 60
CD 0 200 400 600
FIGURE 7. Relations of arterial blood and skeletalmuscle lactate concentrations to intramuscular phos-phocreatine at rest, submaximal, and maximal exer-cise in patients and normal subjects. r=correlationcoefficient.
800
Phosphocreatine (mMImM total creatine x 103)
normal subjects during hypoxia or hypoperfusion thatcentral nervous system inhibition of skeletal muscleafferents may limit exercise tolerance.20,37-39 This hasbeen termed metabolic arrest37 or central fatigue38'39and may act as a protective mechanism that preventshypoxic damage to vital organs under severe stress.Although our data do not define the physiologicalsignificance of the altered peak exercise metabolicend point seen in our patients, it is possible thatcentral fatigue mechanisms may have contributed toexercise limitation in our patients.Our findings in patients at peak exercise are in
contrast to previous studies using 31P-NMR that havedemonstrated advanced acidosis and markedly de-creased PCr/inorganic phosphate ratios in this disor-der.814-16,40 Although several mechanisms could ac-count for these differences, the physiological basis forthe skeletal muscle metabolic results at peak exercisein our patients are not clearly defined. Indexes ofexercise effort at peak exercise, including bloodlactate, respiratory exchange ratio, femoral venousoxygen extraction, and the skeletal muscle content ofglycolytic intermediates, indicate that our patientsachieved a maximal exercise effort as compared tocomparable end points reported in previous exercisestudies in this disorder.'-3,24-29Although the absolutepeak lactate levels were less in patients comparedwith normals, it is possible that an accelerated rate ofaccumulation of lactate, glucose-1-PO4, or glucose-6-PG4 may have contributed to fatigue in our patients.Previous 31P-NMR studies have generally employedexercise involving smaller muscle groups that do notchallenge maximal cardiac output or muscle bloodflow capacity. In the present study, bicycle exercisewas used that activates gluteal, thigh, and calf mus-cles and results in significant hypoperfusion of skel-etal muscle with near-maximal femoral and centralvenous oxygen extraction.5 It is possible that inpatients fatigue is mediated more by neuromuscularfactors during maximal isotonic exercise, elicitingpeak Vo2 and more by skeletal muscle acidosis andPCr depletion during exercise involving small musclegroups. Thus, central fatigue mechanisms may be
activated during large muscle exercise because ofhypoperfusion of nonexercising organs or exercisingskeletal muscle that are not activated during smallmuscle exercise that does not represent a challengeto maximal cardiac output.
Studies have consistently identified a gradient oflactate from skeletal muscle to arterial blood duringintense exercise in normal subjects.41'42 Jorfeldt eta142 have suggested that during exercise the mecha-nisms that mediate lactate removal from muscle toblood are overwhelmed, causing accumulation ofmuscle lactate faster than blood lactate. Althoughprevious studies by Bjarke et a143 have demonstratedan increase in this gradient during exercise in chil-dren with heart failure due to tetralogy of Fallot, theresults of the present study demonstrate that theskeletal-muscle-to-blood lactate gradient is not al-tered in the presence of chronic heart failure becauseof systolic left ventricular dysfunction. Our dataindicate that lower peak exercise arterial lactatelevels in patients with chronic heart failure reflectless advanced skeletal muscle lactate accumulationand PCr depletion and are not due to alterations inthe skeletal-muscle-to-blood lactate gradient.
In summary, the present study demonstrates thatthe skeletal muscle metabolic response to exercise isaltered in patients with chronic heart failure. Consis-tent with the results of previous studies, demonstrat-ing early blood lactate accumulation during exercisein this disorder,5'6 our patients demonstrated accel-erated glycolysis and glycogenolysis in relation toabsolute work rate when compared to normal sub-jects. In our patients, anaerobic metabolism, assessedby blood lactate accumulation during submaximalexercise, was inversely related to rest aerobic enzymeactivity in skeletal muscle. Fatigue at peak exercise inpatients was associated with less PCr depletion andlactate accumulation in skeletal muscle as comparedto normal subjects, suggesting that factors other thanthe magnitude of lactic acidosis or high-energy phos-phate depletion are important in mediating fatigue inthis disorder. The results of the present study supportthe concept that reduced aerobic enzyme activity in
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from
1606 Circulation Vol 84, No 4 October 1991
skeletal muscle plays an important role in determin-ing the metabolic response to exercise in patientswith chronic heart failure and suggest that long-terminterventions that improve exercise tolerance mayact, in part, through effects on skeletal muscle.
AcknowledgmentsWe wish to acknowledge the assistance of Donna
Bowen, RN, Pat Shaw, NMT, James Stanfield, NMT,Debbie Repass, NMT, Jean Wilson, RN, and JohnnyEtheridge, RN for their assistance in performing thestudies; David Knight, PhD, for data analysis; LibFranklin and Chris Kendall for preparation of themanuscript; and Dr. Bengt Saltin for discussing themanuscript and for performing the biochemical anal-yses for the freezing validation study; and Marg Ball-Burnett and Ian Fraser for their expertise in perform-ing skeletal muscle analyses.
References1. Weber KT, Janicki JS: Lactate production during maximal and
submaximal exercise in patients with chronic heart failure. JAm Coll Cardiol 1985;6:717-724
2. Wilson JR, Martin JL, Schwartz D, Ferraro N: Exerciseintolerance in patients with chronic heart failure: Role ofimpaired nutritive flow to skeletal muscle. Circulation 1984;69:1079-1087
3. Poole-Wilson PA, Buller NP: Causes of symptoms in chroniccongestive heart failure and implications for treatment. Am JCardiol 1988;62:31A-34A
4. Sullivan MJ, Higginbotham MB, Cobb FR: Exercise trainingin patients with chronic heart failure delays ventilatory anaer-obic threshold and improves submaximal exercise perfor-mance. Circulation 1989;79:324-329
5. Sullivan MJ, Knight JD, Higginbotham MB, Cobb FR: Rela-tion between central and peripheral hemodynamics duringexercise in patients with chronic heart failure. Circulation1989;80:769-781
6. Zelis R, Longhurst J, Capone RJ, Mason DT: A comparison ofregional blood flow and oxygen utilization during dynamicforearm exercise in normal subjects and patients with conges-tive heart failure. Circulation 1974;50:137-143
7. Sullivan MJ, Green HJ, Cobb FR: Skeletal muscle biochem-istry and histology in ambulatory patients with long-term heartfailure. Circulation 1990;81:518-527
8. Mancini DM, Coyle E, Coggan A, Beltz J, Ferraro N, MontainS, Wilson JR: Contribution of intrinsic skeletal musclechanges to 31P NMR skeletal muscle metabolic abnormalitiesin patients with chronic heart failure. Circulation 1989;80:1338-1346
9. Yancy CW, Parsons D, Lane L, Carry M, Firth BG, BlomqvistCG: Capillary density, fiber type and enzyme composition ofskeletal muscle in congestive heart failure (abstract). J AmColl Cardiol 1989;13(suppl A):38A
10. Walker PM, Idstrom JP, Schersten T, Bylund-Fellenius AC:Metabolic response in different muscle types to reduced bloodflow during exercise in perfused rat hindlimb. Clin Sci 1982;63:293-299
11. Dudley GA, Tullson PC, Terjung RL: Influence of mitochon-drial content on the sensitivity of respiratory control. J BiolChem 1987;262:9109-9114
12. Saltin B, Gollnick PD: Skeletal muscle adaptability: Signifi-cance for metabolism and performance, in Peachey LD (ed):The Handbook of Physiology: The Skeletal Muscle System.Bethesda, Md, American Physiological Society, 1982, pp555-631
13. Karlsson J, Sjodin B, Jacobs I, Kaiser P: Relevance of musclefibre type to fatigue in short intense and prolonged exercise inman. Ciba Found Symp 1981;82:59-74
14. Weiner DH, Fink LI, Maris J, Jones RA, Chance B, WilsonJR: Abnormal skeletal muscle bioenergetics during exercise inpatients with heart failure: Role of reduced muscle blood flow.Circulation 1986;73:1127-1136
15. Massie BM, Conway M, Yonge R, Frostick S, Ledingham J,Sleight P, Radda G, Rajagopalan B: Skeletal muscle metabo-lism in patients with congestive heart failure: Relation toclinical severity and blood flow. Circulation 1987;76:1009-1019
16. Massie BM, Conway M, Rajagopalan B, Yonge R, Frostick S,Ledingham J, Sleight P, Radda G: Skeletal muscle metabolismduring exercise under ischemic conditions in congestive heartfailure. Circulation 1988;78:320-326
17. Sullivan MJ, Higginbotham MB, Cobb FR: Exercise trainingin patients with severe left ventricular dysfunction: Hemody-namic and metabolic effects. Circulation 1988;78:506-515
18. Bergstrom J: Muscle electrolytes in man. Scand J Clin LabInvest 1962;68(suppl):7-100
19. Harris RC, Hultman E, Nordesjo LO: Glycogen, glycolyticintermediates and high-energy phosphates determined inbiopsy samples of musculus quadriceps femoris of man at rest:Methods and variance of values. Scan J Clin Lab Invest1974;33:109-120
20. Green HJ, Sutton J, Cymerman A, Young PM, Houston CS:Operation Everest II: Muscle energetics during maximalexhaustive exercise. JAppl Physiol 1989;66:142-150
21. Soderlund K, Hultman E: Effects of delayed freezing oncontent of phosphagens in human skeletal muscle biopsysamples. JAppl Physiol 1986;61:832-835
22. Ivy JL, Withers RT, Van Handel PJ, Elger DH, Costill DL:Muscle respiratory capacity and fiber type as determinants ofthe lactate threshold. J Appl Physiol 1980;48:523-527
23. Drexler H, Riede U, Hiroi M, Munzel T, Holubarsch C,Meinertz T: Ultrastructural analysis of skeletal muscle inchronic heart failure: Relation to exercise capacity and indicesof LV dysfunction. Circulation 1988;78(suppl II):II-107
24. Massie BM: Exercise tolerance in congestive heart failure:Role of cardiac function, peripheral blood flow, and musclemetabolism and effect of treatment. Am J Med 1988;84(suppl3A):75-82
25. Higginbotham MB, Morris KG, Conn EH, Coleman RE, CobbFR: Determinants of variable exercise performance amongpatients with severe left ventricular dysfunction. Am J Cardiol1983;51:52-60
26. Benge W, Litchfield RL, Marcus ML: Exercise capacity inpatients with severe left ventricular dysfunction. Circulation1980;61:955-959
27. Wilson JR, Ferraro N: Effect of the renin-angiotensin systemon limb circulation and metabolism during exercise in patientswith heart failure. JAm Coll Cardiol 1985;6:556-563
28. Wilson JR, Martin JL, Ferraro N, Weber KT: Effect ofhydralazine on perfusion and metabolism in one leg duringupright bicycle exercise in patients with heart failure. Circula-tion 1983;68:425-432
29. Drexler H, Banhardt U, Meinertz T, Wollschlager H, Leh-mann M, Just H: Contrasting peripheral short-term andlong-term effects of converting enzyme inhibition in patientswith congestive heart failure. Circulation 1989;79:491-502
30. Harris RC, Sahlin K, Hultman E: Phosphagen and lactatecontents of m quadriceps femoris of man after exercise. JApplPhysiol 1977;43:852-857
31. Mainwood GW, Renaud JM: The effect of acid-base balanceon fatigue of skeletal muscle. Can J Physiol Pharmacol 1985;63:403-416
32. Edwards RHT: Interaction of chemical with electromechani-cal factors in human skeletal muscle fatigue. Acta PhysiolScand 1986;128(suppl 556):149-155
33. Miller RG, Boska MD, Moussavi RS, Carson PJ, Weiner MW:31P nuclear magnetic resonance studies of high energy phos-phates and pH in human muscle fatigue. J Clin Invest 1988;81:1190-1196
34. Sullivan MJ, Higginbotham MB, Cobb FR: Increased exerciseventilation in chronic heart failure: Intact ventilatory controldespite hemodynamic and pulmonary abnormalities. Circula-tion 1988;77:552-559
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from

Sullivan et al Altered Skeletal Muscle Metabolic-Response to Exercise 1607
35. Wilson JR, Mancini DM, Ferraro N, Egler J: Effect ofdichloroacetate on the exercise performance of patients withheart failure. JAm Coll Cardiol 1988;12:1464-1469
36. Eiken 0, Bjurstedt H: Dynamic exercise in man as influencedby experimental restriction of blood flow in the workingmuscles. Acta Physiol Scand 1987;131:339-345
37. Hochachka PW, Dunn JF: Metabolic arrest: The most effec-
tive means of protecting tissues against hypoxia, in Sutton JR,Houston CS, Jones NL (eds): Hypoxia, Exercise, and Attitude.New York, Alan R Liss, 1983, pp 297-309
38. Green HJ: Manifestations and sites of neuromuscular fatigue.Biochem Exer 1990;21:13-35
39. Garner SH, Sutton JR, Burse RL, McComas AJ, CymermanA, Houston CS: Operation Everest II: Neuromuscular perfor-mance under conditions of extreme simulated altitude. JApplPhysiol 1990;1167-1172
40. Mancini DM, Ferraro N, Tuchler M, Chance B, Wilson JR:Detection of abnormal calf muscle metabolism in patients withheart failure using phosphorus-31 nuclear magnetic reso-nance. Am J Cardiol 1988;62:1234-1240
41. Green HJ, Hughson RL, Orr GW, Ranney DA: Anaerobicthreshold, blood lactate, and muscle metabolites in progres-sive exercise. JAppl Physiol 1983;54:1032-1038
42. Jorfeldt L, Juhlin-Dannfelt A, Karlsson J: Lactate release inrelation to tissue lactate in human skeletal muscle duringexercise. J Appl Physiol 1978;44:350-352
43. Bjarke B, Erickson BO, Saltin B: ATP, CP and lactateconcentrations in muscle tissue during exercise in malepatients with tetralogy of Fallot. Scan J Clin Lab Invest1974;33:225-231
KEYWORDS * heart failure * exercise * oxygen consumption
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from

M J Sullivan, H J Green and F R Cobbto skeletal muscle aerobic enzyme activity.
Altered skeletal muscle metabolic response to exercise in chronic heart failure. Relation
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1991 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.84.4.1597
1991;84:1597-1607Circulation.
http://circ.ahajournals.org/content/84/4/1597the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 16, 2018
http://circ.ahajournals.org/D
ownloaded from