altered responses in serum calcium phosphorus and parathyroid hormone to oral calcium load in...
TRANSCRIPT

ALTERED RESPONSES IN SERUM CALCIUM PHOSPHORUS
AND PARATHYROID HORMONE TO ORAL CALCIUM
LOAD IN SYMPTOMATIC ANQ ASYMPTOMATIC MEMBERS
OF FAMILY WITH IDIOPATHIC HYPERCALCEMIA
DAVID JUAN, M.D.
From the Veterans Administration Medical Center, and Departments of Medicine and Pharmacology, University of Arkansas for Medical Sciences, Little Rock, Arkansas
ABSTRACT-A family of idiopathic hypercalciuria (IH), 3 symptomatic and 2 asymptomatic, plus 3 normal subjects were given the 1 Gm oral calcium challenge. Biochemical parameters measured included: serum and urinary calcium and phosphate, urinary cyclic AMP, and serum intact and carboxyl-terminal parathyroid hormone. Major differences between the normal control and the family with IH include: (1) higher calcemic response in the family with IH (0.9 vs 0.4 mg/dl); (2) a fall in carboxyl-terminal PTH and urinary cyclic AMP in the IH family in contrast to control subjects in whom there were no changes; (3) a rise in serum phosphorus in the IH family (0.8 vs 0.2 mg/dl, p < 0.05). Urinary excretion of calcium, phosphorus, and sodium after the calcium chal- lenge was minimal. The oral calcium challenge is a simple and useful test in demonstrating in- creased calcium absorption even in asymptomatic relatives of patients with idiopathic hypercal- ciuria.
Albright and colleagues’ first coined the term “idiopathic hypercalciuria” to describe a syn- drome characterized by normocalcemic hyper- calciuria associated with a tendency to hypo- phosphatemia. There are three proposed mech- anisms to account for the hypercalciuria in this condition. The first hypothesis championed by Coe and coworkers2 states that the hypercal- ciuria represents a subtle form of primary hyperparathyroidism. The second hypothesis focuses on the primary defect in the renal tubu- lar reabsorption of calcium (renal hypercal- ciuria).3 The third hypothesis emphasizes the enhanced intestinal absorption of calcium (ab- sorptive hypercalciuria) as a consequence of ele- vated circulating 1,25-dihydroxy vitamin D3 and/or hypophosphatemia.4
Using increasing amounts of calcium in the diet, Pak and coworkers5 found that a subset of patients with idiopathic hypercalciuria, the ab- sorptive hypercalciuria, showed a positive cor-
relation between dietary calcium intake and urinary calcium excretion in the absence of sig- nificant changes in serum calcium. More re- cently, Broadus, Dominguez, and Barttere used the oral calcium tolerance test to characterize distinctive subgroups of hypercalciuria.
The genetic influence in the pathogenesis of calcium nephrolithiasis is not well understood. Resnick, Pridgen, and Goodman’ provided data to support the existence of a polygenic sys- tem among kidney stone formers with a lesser risk for females. Thomas, Berge, and Brunssch- wigS showed that the risk of calcium oxalate stone developing among the first-degree relative is four times higher than those with calcium phosphate stone.
There is a paucity of data concerning the metabolic status of asymptomatic relatives of patients with idiopathic hypercalciuria. The author was fortunate to encounter a family in which two members were totally asymptomatic
162 UROLOGY / AUGUST 1984 / VOLUME XXIV, NUMBER 2

TABLE I. Baseline 24hr urinary excretion of Ca, P, Na, and uric acid in the family with
idiopathic hypercalciuria
Patient
Symptomatic
- Urinary Excretion* - Ca P Na Uric Acid
DT CS DS
Asymptomatic
173 474 114 537 161 378 89 247 195 1053 103 200
PD 325 602 99 288 MS 208 723 84 203
*Values for Ca, P, uric acid in mg/Gm Cr; Na in mmol/Gm Cr.
at the time of the study. This report constitutes the response of serum and urinary calcium, phosphorus, serum intact and carboxyl- terminal parathyroid hormone in 3 normal sub- jects as well as this family with idiopathic hy- percalciuria to an oral calcium load. Abnormal calcemic, phosphatemic, as well as changes in intact and carboxyl-terminal parathyroid hor- mone levels were observed among both sympto- matic and asymptomatic members of this fam- ily.
Material and Methods
Patient populations
Normal. Two males and 1 female (aged 21 to 26 years, mean 23) participated in this study. They were all healthy, on regular diets with nor- mal intake of calcium and phosphorus (Ca 500- 1,000 mg/day: P 800-1,200 mglday). They were not taking medication or vitamins.
Family with IH: The family tree shows the members in the present study (Fig. 1). The eldest son, LS, lived in another state and was reported to have calcium oxalate stones cur- rently being treated with a thiazide diuretic. The mother, DT, and her two sons (DS, CS) all had documented calcium oxalate stones in the past. CS and DS had three kidney stones each in the last five years but were not being treated with any medication at the time of the study. Her two daughters, PD and RS, have never had calcium stones. Because RS had inflammatory bowel disease, she was excluded from this study. The mother, DT, was treated with hydro- chlorothiazide (25 mg a day). The only child of CS, MS, had unexplained recurrent lower ab- dominal pains. None of the subjects tested had ingested vitamin D or were known to have dis- orders of calcium metabolism such as sarcoido- sis, hypercalcemia, or osteoporosis. Findings on
DT (5BY/O)
+-r 0
d
MS (BY/O)
FIGURE 1. Family tree of symptomatic and asymptomatic patients with idiopathic hypercal- ciuria, symptomatic (W, l ), asymptomatic (0, 0).
their physical examinations were completely normal. By detailed history-taking, daily intake of calcium was estimated to be between 600 to 1,000 mg a day and phosphorus intake 800 to 1,200 mg a day. Hydrochlorothiazide in DT was discontinued twenty-four hours prior to the calcium challenge. Repeated twenty-four-hour urine values for calcium, phosphorus, sodium, and uric acid on ad lib diet were done (Table I). A consent form was obtained from each subject before the study.
Study protocol
All subjects were told to take nothing by mouth except water after 7 PM the previous eve- ning. After arriving in the laboratory, they were told to void and then to start drinking three cups of tap water every hour until the comple- tion of the study. Urine was collected at 11:OO and 13:00 hours (0 and 120 minutes) after the oral calcium load. Blood was drawn at ll:OO, 12:00, and 13:00 hours (0, 60, and 120 min) af- ter they had received the 1,000 mg calcium load, consisting of 35 ml Neo-calglucon and 8 ounces of whole milk, similar to the one used by Broadus, Dominguez, and Bartter.e All subjects had to lie flat for thirty minutes prior to each venipuncture. In between blood samples, their activities were limited to bed, chair, and bathroom.
Biochemical analysis
Total calcium (TCa) was measured by atomic absorption spectrophotometry,Q ionized calcium (Ca+ ‘) by the calcium specific electrode (Ap- plied Medical Technology, Palo Alto, CA), and serum phosphorus (Pi) by the Fiske and Subbar- row method.‘O Both intact and carboxyl- terminal parathyroid hormones (PTH,, PTH,) were measured by Dr. Charles Hawker and Dr. Frank DiBella at the Upjohn Company (Kala- mazoo, MI) by established methods.” They re- ported interassay coefficients of variation for
UROLOGY / AUGUST 1984 / VOLUME XXIV, NUMBER 2 163

TABLE II. Effect of calcium load on TCa, Ca’ +, P, PTH, and PTH, in 3 normal subjects and a family with idiopathic hypercalciuria *
TCa Ca++ Subjects Time (8.8-10.0) (3.7-4.7) (2.sp-s.s)
PTH, PTH, (163-347) (150-375)
NORMAL VP
cs
JH
IH FAMILY Symptomatic
cs
DT
DS
Asymptomatic MS
PD
0 10.1 4.69 60 10.4 4.70
120 10.7 4.82 0 9.9 5.29
60 10.3 4.74 120 10.0 4.72
0 9.7 4.42 60 10.2 4.61
120 10.2 4.78
0 9.9 60 10.7
120 10.1 0 9.5
60 10.1 120 10.1
0 9.8 60 10.9
120 L 10.5
0 60
120 0
60 120
9.5
9:7
4:+5 4.72 4.36 4.54 3.64 4.61 5.02 5.02
4.46 4.8 221 150
4:5’7 4.78 4.83 4.90
ii 4.0
ii
j5b i65 268 208 292 190 267 185
3.9 . .
i::
3.8 3.5
ii3
220 210 221 200 229 211 274 234 279 233 208 200 282 238 305 256 283 240
3.1
4.i 2.7
262 222 236 182 255 208 349 224 309 191 265 236 220 262 232 150 230 236
Values for TCa, Ca’ +, P in mgidl; PTH,, PTH, in pgEqlm1.
both assays between 7 to 12 per cent. Urinary cyclic AMP was measured by the Amersham Kit TRK 432 (Amersham, Chicago, IL). Normal values for males and females were 1.2 to 5.3 pmol/Gm creatinine.
Statistical analyses In the tables and figures, results are given as
mean + standard error of the mean (SEM). Student’s t test for paired observations was used to analyze for statistical significance.
Results
Basal twenty-four-hour urine in family with idiopathic hypercalciuria
Table I shows the twenty-four-hour urine values for calcium, phosphorus, sodium, and uric acid in symptomatic (DT, CS, DS) and asymptomatic (PD, MS) members in this fam- ily. Except for hypercalciuria, their other bio- chemical parameters were within the normal range.
Effects of calcium load on serum and urinary calcium
As shown in Table II basal TCa and Ca’ + values in the family with IH were slightly lower than the control. Nonetheless, the urinary cal- cium values were much higher in the family with IH (0.298 vs 0.075 mg/mg Cr) (Table III). After the oral calcium load, a higher calcemic response was noted in the family with IH than in the control (0.9 vs 0.4 mgldl) at the end of one hour, and the difference was less noticeable at two hours. The urinary calcium in the con- trol remained unchanged whereas it fell in the family with IH.
Effects of calcium load on intact and carboxyl-terminal parathyroid hormone levels and urinary cyclic AMP
Except for DT whose intact PTH level was slightly over the normal range, the family with IH had comparable basal levels compared with control subjects (Table II). The eight-year-old
164 UROLOGY / AUGUST 1984 / VOLUME XXIV, NUMBER 2
II .o
10.0 b 2 9. 0 I
--_ --b
4.6 4.7
*
G 4.5
4.3 1
4.7 4.5 4.3 4.1 3.9 3.7
9 3.3 3.3 I
I ** __-- e --
k -- -_-- _--- i _--
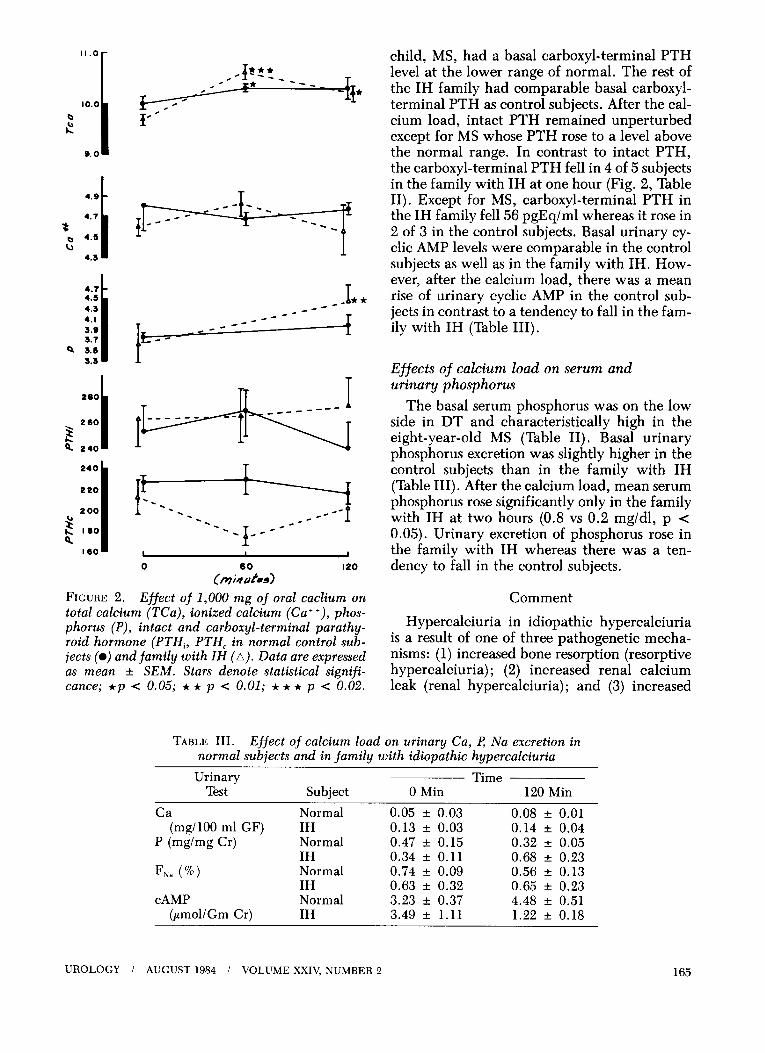
child, MS, had a basal carboxyl-terminal PTH level at the lower range of normal. The rest of the IH family had comparable basal carboxyl- terminal PTH as control subjects. After the cal- cium load, intact PTH remained unperturbed except for MS whose PTH rose to a level above the normal range. In contrast to intact PTH, the carboxyl-terminal PTH fell in 4 of 5 subjects in the family with IH at one hour (Fig. 2, Table II). Except for MS, carboxyl-terminal PTH in the IH family fell 56 pgEq/ml whereas it rose in 2 of 3 in the control subjects. Basal urinary cy- clic AMP levels were comparable in the control subjects as well as in the family with IH. How- ever, after the calcium load, there was a mean rise of urinary cyclic AMP in the control sub- jects in contrast to a tendency to fall in the fam- ily with IH (Table III).
220
260
2 q 240 1
240
Effects of calcium load on serum and urinary phosphorus
220
200 u
$ I00
I60 I
The basal serum phosphorus was on the low side in DT and characteristically high in the eight-year-old MS (Table 11). Basal urinary phosphorus excretion was slightly higher in the control subjects than in the family with IH (Table III). After the calcium load, mean serum phosphorus rose significantly only in the family with IH at two hours (0.8 vs 0.2 mg/dl, p < 0.05). Urinary excretion of phosphorus rose in the family with IH whereas there was a ten- dency to fall in the control subjects.
FIGURE 2. Effect of 1,000 mg of oral caclium on Comment total calcium (TCa), ionized calcium (Ca+ +), phos- phorus (P), intact and carboxyl-terminal parathy- roid hormone (PTH,, PTH, in normal control sub- jects (@) and family with ZH (A). Data are expressed as mean + SEM. Stars denote statistical signifi- cance; *p < 0.05; ** p < 0.01; *** p < 0.02.
Hypercalciuria in idiopathic hypercalciuria is a result of one of three pathogenetic mecha- nisms: (1) increased bone resorption (resorptive hypercalciuria); (2) increased renal calcium leak (renal hypercalciuria); and (3) increased
TABLE III. Effect of calcium load on urinary Ca, P Na excretion in normal subjects and in family with idiopathic hypercalciuria
Urinary Time Test Subject 0 Min 120 Min
Ca Normal 0.05 f 0.03 0.08 AZ 0.01 (mg/lOO ml GF) IH 0.13 + 0.03 0.14 + 0.04
P (mg/mg Cr) Normal 0.47 + 0.15 0.32 + 0.05 IH 0.34 f 0.11 0.68 f 0.23
Fiva (%) Normal 0.74 + 0.09 0.56 f 0.13 IH 0.63 + 0.32 0.65 f 0.23
CAMP Normal 3.23 AZ 0.37 4.48 f 0.51 (pmol/Gm Cr) IH 3.49 + 1.11 1.22 + 0.18
UROLOGY i AUGUST1984 / VOLUMEXXIV,NUMBER2 165

intestinal absorption of calcium (absorptive hy- percalciuria) . 2-4 Pak’s classification of hypercal- ciuria depends on measuring serum and urinary calcium, urinary cyclic AMP, parathyroid hor- mone, and responses of these biochemical pa- rameters to a calcium load.5 Characteristically, patients with absorptive hypercalciuria have normal fasting urinary and serum calcium. Af- ter an oral 1 Gm calcium load, there is a dra- matic increase in both serum and urinary cal- cium in association with a greater suppression of nephrogenous cyclic AMP5s6 It was noted by Peacock, Knowles, and Nordin12 that an over- night fast may not be sufficient to normalize urinary calcium in some patients. Prolonged fasting (6-8 hr) is necessary to accomplish this aim. Patients with renal hypercalciuria, on the other hand, have normal serum calcium, higher fasting urinary calcium, higher fasting urinary cyclic AMP which normalize after an oral cal- cium load.e These subjects do not show the dra- matic calcemic or calciuric responses as do pa- tients with absorptive hypercalciuria.
Interestingly, the twenty-four-hour urinary calcium in the asymptomatic subjects (PD and MS) were even higher than their symptomatic relatives. Since DT had been taking hydro- chlorothiazide for her kidney stone, her twenty- four-hour urinary calcium was unexpectedly high. There was no evidence of excess sodium or urate excretion in this family (Table I).
Baseline TCa and Ca+ + values were lower in the family with IH. However, after the oral cal- cium load; a dramatic calcemic rise was noted in the family with IH as compared with control subjects (0.9 vs 0.4 mg/dl) (Fig. 2), values very similar to the Broadus study.6 In the present study, the TCa peaked at sixty minutes whereas in the study by Epstein, et al. l3 it peaked at one hundred twenty minutes. Compared to the Ep- stein study, the rise in TCa was less than ex- pected. The faster but blunted rise in TCa after the calcium load may be due to the fact that in this study the calcium load consisted of a cal- cium salt plus milk which, among other food- stuffs, is known to impair the absorption of cal- cium from the gastrointestinal tract.
The correlation between TCa and Ca+ + is at best a rough one. Even though there was a uni- form rise in TCa in both the normal and the family with IH, the changes in Ca’ + were less uniform. In a normal subject, CS, the Ca’ + in fact fell at sixty and at one hundred twenty min- utes. Also, DT’s Ca++ fell at one hundred twenty minutes. There is no good way to pre-
diet the serum Ca’ + from TCa even with for- mulas or normograms which correct for changes in serum protein or pH.14
Why do patients with absorptive hypercal- ciuria show such a dramatic calcemic response to oral calcium challenge? Up to one half of all the patients with absorptive hypercalciuria have elevated 1,25-dihydroxy-vitamin D3 levels.4 However, among those with normal 1,25-dihydroxy-vitamin D, levels, there is no correlation between intestinal calcium absorp- tion and serum 1,25-dihydroxy-vitamin D) levels. Basal parathyroid hormone levels in pa- tients with absorptive hypercalciuria are usually normal or low .5,6 Using an aminoter- minal parathyroid hormone assay, Pak et aL5 reported that none of their patients with ab- sorptive hypercalciuria had high parathyroid hormone levels. Broadus et aLe reported that except for 2 patients with renal hypercalciuria the other 19 patients with idiopathic hypercal- ciuria had normal parathyroid levels which did not change much after the same oral calcium load as used in this study. They speculated that the failure of the parathyroid hormone levels to fall after the calcium load in their patients was due to detection of inactive fragments of long half-life and/or inherent insensitivity of the multivalent assay to detect changes occurring within the normal range.6 However, they did observe a greater fall in nephrogenous CAMP in their patients with IH as compared with control subjects (54 vs 39 %), indicative of greater parathyroid hormone activity. Whether this fall in CAMP is due to increased secretion and/or de- creased degradation is unknown at this time. Thus, part of the calcemic response among the patients in the IH group is due to greater parathyroid activity.
In the present study, intact parathyroid hor- mone failed to change after the oral calcium load in the control subjects, whereas in the fam- ily with IH there was a tendency to fall at one hundred twenty minutes (Fig. 2). The urinary CAMP fell only in the family with IH and not in the control subjects (Table III). The calcium load brought about a striking fall (56 pgEq/ml) in the carboxyl-terminal parathyroid levels in the family with IH (Fig. 2). At one hundred twenty minutes, mean PTH, fell below baseline in the control group whereas in the family with IH the values began to rise toward baseline. Based on the study by Arnaud et ~1.‘~ dif- ferences in the suppressibility of PTH simply re- flects differences in the antiserum used. There is
166 UROLOGY / AUGUST 1984 i VOLUME XXIV, NUMBER 2

c
no ready explanation as to why the IH patients’ PTH response to oral calcium was different from control subjects. Whether or not postse- cretory proteolysis and/or catabolism in pa- tients with IH differs from normal subjects is an area that awaits future investigation.
In the eight-year-old child, MS, the response to calcium load was distinctly different (Table II). Unlike the adult members of the family, his TCa rose slightly (0.2 vs 0.6 mgldl) as did his Ca+ + (0.12 vs 0.39 mg/dl). In contrast to both normal control subjects and the other members of his family, his intact parathyroid hormone level rose dramatically (138 pgEq/ml) at one hundred twenty minutes. His baseline car- boxyl-terminal parathyroid hormone was on the lower limits of normal and rose modestly at one hundred twenty minutes. Whether or not these changes are peculiar to him as part of the idiopathic hypercalciuria family or are seen in other children of the same age is unclear at the present time.
The urinary calcium changes in the family with IH are difficult to explain. Their basal values are comparable to the ones reported in the literature.5,6,16 However, after the calcium load, the rise in urinary calcium in this family as well as in the control subjects was less than expected (Table III). Peacock, Knowles, and Nordin12 found good separation between nor- mal subjects and patients with IH two hours af- ter the calcium load. Since milk in the calcium load contains phosphorus, it was of interest to note that the difference in the rise in serum phosphorus at the end of two hours was dif- ferent between the family with IH and the con- trol subjects (mean 0.9 vs 0.2 mg/dl). The hypo- calciuric effect of a phosphorus load in these patients is well documented.17 The significant rise in serum phosphorus in the family with IH may have contributed to the blunted rise in urinary calcium.
Pak and Broadus have nicely demonstrated that the calcium tolerance test is a remarkably accurate and simple means of demonstrating in- creased calcium absorption in hypercalciuric patients especially those with subtle primary hyperparathyroidism .7,18 The present study ex- tends the usefulness of this test in detecting asymptomatic relatives of patients with idiopathic hypercalciuria. The clinical signifi- cance of this finding is that once these subjects are identified preventive measures could be in- stituted to delay or even avert the eventual de- velopment of calcium nephrolithiasis.
Northwestern Memorial Hospital Clinical Pharmacology Center
303 E. Superior Street Chicago, Illinois 60611
ACKNOWLEDGMENT. To John Wehmeister for his expert technical assistance. This study was sup- ported by the Douglas Foundation (Toledo, Ohio) and in part by the Veterans Administration research funds.
References
1. Albright F, Henneman P, Benedict PH, and Forbes AP: Idiopathic hypercalciuria, J Clin Endocrinol 13: 869 (1953).
2. Coe FL, Canterbury JM, Firpo JJ, and Reiss E: Evidence for secondary hyperparathyroidism in idiopathic hypercalciuria, J Clin Invest 52: 134 (1973).
3. Robertson WG, Peacock M, and Heyburn PJ: Clinical and metabolic aspects of urinary stone disease in Leeds, Stand J Urol Nephrol (Suppl):53 199 (1980).
4. Kaplan RA, et al: The role of 1,25-dihydroxy-vitamin D3 in the mediation of intestinal hyperabsorption of calcium in primary hyperparathyroidism and absorptive hypercalciuria, J Clin Invest 59: 756 (1977).
5. Pak CYC, Ohata M, Lawrence EC, and Snyder W: The hy- percalciurias: causes, parathyroid functions and diagnostic crite- ria, ibid 54: 378 (1974).
6. Broadus AE, Dominguez M, and Bartter FC: Pathophys- iologic studies in idiopathic hypercalciuria: use of an oral calcium tolerance test to characterize distinctive hypercalciuria sub- groups, J Clin Endocrinol Metab 47: 751 (1978).
7. Resnick M, Pridgen DB, and Goodman HO: Genetic predis- position to formation of calcium oxalate renal calculi, N Engl J Med 278: 1313 (1968).
8. Thomas J, Berge D, and Brunsschwig JE: Aboulker P Caracteres secuelsdet fasteurs genetizues des trois grandes varietes chimiques de lit&e renale; urique oxalique, phosphatique, Rem et Fore 8: 147 (1966).
9. Pybus J, Feldman FS, and Bowers GN Jr: Measurement of total calcium in serum by atomic absorption sprectrophotometry with use of a strontium internal standard, Clin Chem 16: 998 (1970).
10. Fiske CH, and Subbarrow Y: The calorimetric determina- tion of phosphorus, J Biol Chem 66:375 (1925).
11. Hawker CD, and DiBella FP: Radioimmunoassays for in- tact and carboxyl-terminal parathyroid hormone: clinical inter- pretation and diagnostic significance, Ann Clin Lab Sci 10: 76 (1980).
12. Peacock M, Knowles F, and Nordin BEC: Effect of calcium administration and deprivation on serum and urine calcium in stone-forming and control subjects, Br Med J 50: 729 (1968).
13. Epstein S, Micghan WV, Sage1 J, and Jackson WPW: Ef- fect of single large dose of oral calcium on serum calcium levels in the young and the elderly, Metabolism 22: 1163 (1976).
14. Ladenson JH, et al: Relationship of free and total calcium in hypercalcemic conditions, J Clin Endocrinol Metab 48: 393 (1979).
15. Arnaud CD, Goldsmith RS, Bordier PJ, and Sizemore GW: Influence of immunoheterogeneity of circulating parathy- roid hormone on results of radioimmunoassays of serum in man, Am J Med 56: 785 (1974).
16. Lau YK, et a/: Proximal tubular defects in idiopathic hy- percalciuria: resistance to phosphate administration, Min Elect Metab 7: 237 (1982).
17. Wikstrom B: Phosphate metabolism and renal calcium stone disease, Stand J Urol Nephrol (Suppl) 61: 1 (1981).
18. Broadus AF, Mahaffey JE, and Rasmussen H: Hyperpara- thyroidism with intermittent hypercalcemia: serial study and sim- ple diagnosis, Clin Res 25: 494A (1977).
UROLOGY / AUGUST 1984 i VOLUME XXIV, NUMBER 2 167