alpha/beta t-cell depletion – transforming pediatric hct
TRANSCRIPT

1
Alpha/Beta T-Cell Depletion –Transforming Pediatric HCT
Christopher C. Dvorak, MDProfessor and Chief
Division of Pediatric Allergy, Immunology, and Bone Marrow TransplantationUniversity of California San Francisco

Faculty Disclosure• Consulting for Alexion, Inc., Omeros Corp., and Jazz
Pharmaceuticals• Alpha-Beta TCR T-cell Depletion is made by Miltenyi
Biotec and is investigational in the US (all procedures done under an IND/IDE)
2
In compliance with ACCME policy,AABB requires the followingdisclosures to the session audience

Objectives• Describe how Alpha/Beta T-cell Depletion is
performed• Contrast the pros/cons of in vivo and ex vivo T-cell
depletion strategies in pediatric patients undergoing haploidentical HCT
3

For Allogeneic HCT, There are 4 Donor Options• Matched Sibling Donor (MSD)
– Historically, the gold standard– Rejection rare, GVHD uncommon– For cancer, MSD has least GVL effect, and for genetic diseases, some carrier issues
• Adult Unrelated Donor (URD)– Success depends on mainly on degree of match
• Unrelated Umbilical Cord Blood (UCB)– Success depends on mainly degree of match and cell dose
• Mismatched Related Donor (MMRD; Haploidentical)– Readily available for most patients– Success depends on degree of T-cell depletion (TCD)– TCD can be done either in vivo or ex vivo
4

Likelihood of Finding Unrelated Donor or UCB
Gragert L, et al. N Engl J Med. 2014; 371(4): 339-348.
0%10%20%30%40%50%60%70%80%90%
100%M
atch
like
lihoo
d
Ancestral group of searching patient for hematopoietic cell transplantation
8/8 HLA adult donor 7/8 HLA adult donor 6/6 HLA cord blood 5/6 HLA cord blood 4/6 HLA cord blood

MSD HCT has been flat for the last 20 years
MUD HCT has been flat for the last 8 years
Haplos are the cool new thing!
UCBT may be nearly extinct by 2025 (except for certain rare diseases)
6

Haplo HCT Has Gotten a Lot Better!
1991-1999 2000-2007• Early haplosdone mainly with CD34 selection
• Recent haplos done mainly with CD3 depletion
7

What is the Best Way to Prevent GVHD after HaploHCT Without Eliminating GVL?
CD4+ & CD8+ T Cells Mediate GVHD: These Have A/B TCRs
8

Different Haplo OptionsIn Vivo TCD: PTCYEx Vivo TCD
A/B TCDCD34 Selection
9

• PBSC Collection• Requires excellent stem
cell lab (and an IND)• Fast Count Recovery• No Pharmacologic
GVHD Prophylaxis needed
• No exposure of HSCs to alkylation
• BM Collection• Anyone can do it• Slower Count Recovery• Requires Tacro and
MMF• Exposes donor HSCs to
alkylation -> 2nd
malignancy?
A/B TCD vs. PTCY
10

A/B TCD: Processing
• You also need to co-remove CD19+ cells• Expect some CD34+ cell loss: Median recovery = 78% (range 49-93%)• We aim to collect 2x the goal CD34 target of 10x10^6/kg• This is typically not an issue with smaller kids (<20 kg) and parental
donors, but can be a problem with AYAs and when haploidentical siblings are used -> multi-day collections
• The A/B T-cell Depletion can be quite profound (final dose in the graft is typically <1 x 10^5 cells/kg) -> Add-back may be desirable
11

Optimizing Cell Dose: RejectionCD34 dose > or < 10 x 10^6/kg A/B T-cell dose > or < 8 x 10^4/kg
9% vs. 44% (p=0.006) 0% vs. 23% (p=0.044)
N=9
N=17
12
N=43N=34
Unpublished Data from 52 First Haplo HCTs for Heme Malignancy at UCSF

Is A/B TCD Worth All The Effort?• A/B TCD• Single Center Italian
Prospective Data (N=80, 2011-2014)
• Multi-Center US Prospective Data (N=51, 2015-2020)*
• Single Center UCSF Retrospective Data (N=52, 2015-2021)
• PTCY• Single Center US
Prospective Data (N=29, 2008-2016)
• Multi-Center European Retrospective Data (N=180, 2011-2019)
13*Presented as a best Abstract at ASTCT 2021

Is A/B TCD Worth All The Effort?Non-Relapse Mortality: A/B TCD
Locatelli, et al. 2017 5% (5 years)
PTCTC ONC1401 10% (2 years)
UCSF 4% (2 years)
Non-Relapse Mortality: PTCY
Symons, et al. 2020 7% (1 year)
Ruggeri, et al. 2021 20% (2 years)
14
Relapse: A/B TCD
Locatelli, et al. 2017 24% (5 years)
PTCTC ONC1401 17% (2 years)
UCSF 15% (2 years)
Relapse: PTCY
Symons, et al. 28% (3 years)
Ruggeri, et al. 42% (2 years)

Is A/B TCD Worth All The Effort?
15
Relapse-Free Survival: A/B TCD
Locatelli, et al. 2017 71% (5 years)
PTCTC ONC1401 67% (2 years)
UCSF 81% (2 years)
Relapse-Free Survival: PTCY
Symons, et al. 2020 65% (3 years)
Ruggeri, et al. 2021 39% (2 years)
Overall Survival: A/B TCD
Locatelli, et al. 2017 72% (5 years)
PTCTC ONC1401 76% (2 years)
UCSF 91% (2 years)
Overall Survival: PTCY
Symons, et al. 2020 79% (3 years)
Ruggeri, et al. 2021 51% (2 years)

A/B TCD Has Made Haplo Equivalent to Other Donors (in Terms of Safety)
16
Haplo (n=83)
MSD(n=38)
URD (n=59)
Unpublished Data from All First HCTs for Heme Malignancy at UCSF from 2016-2020

A/B TCD Haplos vs. Other Donors: NRM
Data courtesy of M. PulsipherItalian Data (Bertaina, Blood 2018)
17

There Is No Such Thing as a “Good Donor”• The likelihood of finding a perfectly matched donor
depends on the patient’s ancestry as compared to the donors in the registry, not offering BMT to patients without a perfect match is perpetuating a medical disparity
• “We’ll go to transplant if there is a matched sib or a good unrelated donor”
• All patients who need a BMT for best control of their underlying disease should be offered a BMT, regardless of their donor options
18

The Next Steps
• We have made haploidentical HCT as safe as other donors
• Could it actually be superior?• For patients with heme malignancies undergoing
HCT, the biggest problem is not TRM, but relapse• The HLA mismatches of haplo HCT induce a
powerful GVL effect
19
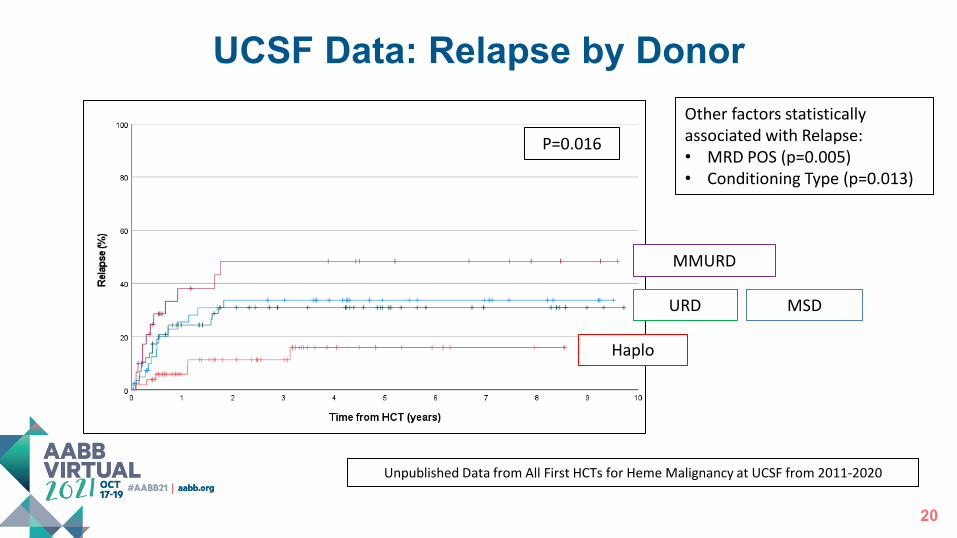
MMURD
UCSF Data: Relapse by Donor
MSDURD
Haplo
Other factors statistically associated with Relapse:• MRD POS (p=0.005)• Conditioning Type (p=0.013)
P=0.016
20
Unpublished Data from All First HCTs for Heme Malignancy at UCSF from 2011-2020

Haplo
MMURD
URD MSD
P<0.001
Other factors statistically associated with RFS:• MRD POS (p=0.006)• Conditioning Type
(p=0.009)• HCT-CI (p=0.031)
UCSF Data: RFS by Donor
21
Unpublished Data from All First HCTs for Heme Malignancy at UCSF from 2011-2020

A/B TCD Haplos vs. Other Donors: LFS
Data courtesy of M. Pulsipher
Italian Data (Bertaina, Blood 2018)
22

What Donor to Choose Based on MRD Status?
MSD URD MMURD Haplo
23Unpublished Data from All First HCTs for Heme Malignancy at UCSF from 2011-2020

24

Conclusions• Haploidentical HCT allows HCT for all patients, regardless of ancestry• A/B TCD Depletion is labor intensive, but has many attractive
qualities compared to in vivo TCD with post-transplant cyclophosphamide
• For patients with heme malignancies, A/B TCD Haplo HCT is as good, if not better, than MSD or URD HCT
– Especially if the patient is minimal residual disease positive (due to the strong GVL effect of haplo)
• A/B TCD Haplo can be a platform for other graft engineering techniques
25

Acknowledgments• Entire UCSF Pediatric HCT Team (MDs, NPs, RNs, SW, Pharmacy, etc.) • Mort Cowan – 1st Haplo on the West Coast in 1982• Mike Pulsipher (CHLA) – Said “Let’s do a A/B TCD HCT Trial in the US!”
– Hisham Abdel-Azim (CHLA) – Led data analysis of PTCTC ONC1401– Alice Bertaina (Stanford) – Led the Italian trials– NCI R01 CA181050 (Pulsipher)
• Apheresis Programs (Adult & Pediatric) – Collecting high numbers of CD34+ cells required is challenging!
• Importantly, PCTL Staff led by Sherman Bakabak and Jess Oh– A/B TCD is a LOT more work than just giving PTCY, but I think it’s worth it!
26
Thank You!
27

28

Pediatric Cellular Therapy: An Overview from Collections to Alpha/Beta DepletionsAlpha/Beta T-Cell Depletion –Transforming Pediatric HCT
17 October 2021 (1500-1600)

A Problem: OS Rates Have Mainly Stalled
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24
SUR
VIVA
L (%
)
MONTHS AFTER TRANSPLANT
2013–2016 (n=305)2009–2012 (n=216)2004–2008 (n=173)1987–2003 (n=140)
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24
SUR
VIVA
L (%
)
MONTHS AFTER TRANSPLANT
2013–2016 (n=235)2009–2012 (n=257)2004–2008 (n=196)1987–2003 (n=206)
ALL AML
SOURCE: CIBMTR®, the research program of NMDP/Be The Match
30

Is A/B TCD Worth All The Effort?
31
9.8 & 19.8%
CR1=39% of patientsCR2+=61% of patients

What Donor to Choose Based on HCT-CI?
MSD URD MMURD Haplo
32
Generally in Good Shape In Poor Shape
Unpublished Data from All First Haplo HCTs for Heme Malignancy at UCSF from 2011-2020