alliance healthcare, inc
TRANSCRIPT

Employment Application
NameLast First Middle Initial
Current Address:Street Address City CA Zip Code
Please list previous address and dates from the past seven years:1).2).3).
Home Phone: Work Phone: Cell Phone:
Professional Discipline: Specialty:
DL#: State: DL Expiration:
SS#: Date of Birth:
Has your professional license or certification ever been investigatedor suspended? Yes No If yes, attach separate sheet with explanation.
Have your ever been convicted of a crime other than a minor traffic violation? Yes No If yes, attach separate sheet with explanation.
Have you ever been named as adefendant in a professional liability action? Yes No
Can you submit verification of your legal right to work in the United States? Yes No
Person to notify in case of emergency:Name Relationship
Street address City State Zip Code Phone
LICENSURE (Include photo copies of licenses held.)
License #: State: Expir. Date:
License #: State: Expir. Date:
CERTIFICATION (Include photocopies of certification held.)
Check one: Certified Registered Registry Eligible Other
Certificate/Registration: # Expir. Date:
EDUCATION Name & Location of School Month/Year Diplomas,Graduated Degrees received
College
Graduate School
Other School(if applicable)
How did you learn aboutAlliance Healthcare, Inc?
Alliance Healthcare, Inc.

Employment History(Begin with most recent employer)
From: / / To: / /
Position/Specialty: Ending Salary:
Employer:
Address:
City: State: Zip:
Phone: Contact:
Duties:
Reason for leaving:
From: / / To: / /
Position/Specialty: Ending Salary:
Employer:
Address:
City: State: Zip:
Phone: Contact:
Duties:
Reason for leaving:
From: / / To: / /
Position/Specialty: Ending Salary:
Employer:
Address:
City: State: Zip:
Phone: Contact:
Duties:
Reason for leaving:
Page 2
Alliance Healthcare, Inc.

Relationship: Relationship: Relationship:
CERTIFICATION
BCLS: EXP: ACLS: EXP: PALS: EXP:
NALS: EXP: CCRN: EXP: MICN: EXP:
Number of years as: Respiratory Therapist Years: Months:Registered Nurse Years: Months:
Months:
ICU/CCU TELE: ER: MED/SURG: L&D: NICU: PEDS: OR: HOMEHEALTH: OTHER:
Willing to work in: ICU/CCU TELE: ER: MED/SURG: L&D: NICU: PEDS: OR: HOMEHEALTH: OTHER:
Shift Preferences: 12 hr: 8 hr: F/T P/T PD: Traveler: Days: PM: Nights: Wkends:
Hospital Location Preferences:
First Date Available for Work:
Co-Worker References
:emaN :emaN :emaN
Phone: ( ) Phone: ( ) Phone: ( )
Page 3
Alliance Healthcare, Inc.
Years:

EMPLOYMENT REFERENCE FORM
Employee: Please complete the top portion of this form, sign the authorization below, and give it the reference contact person you have indicated below to verity your reference. The completed form may be FAXED to ALLIANCE HEALTHCARE, INC. at (559)291-2422.
References must be from a Person in a MANAGERIAL POSITION or from a HUMAN RESOURCES DEPARTMENT. Any other source may result in disqualification of an employment offer:
References must be from an Acute Care Facility.
APPLICANT NAME: SSN#
REFERENCE: Name of Person to Contact: PHONE:
Name of Facility: Dates of Employment: From: To:
Position Held: Reason for leaving:
Area of Work: Clinical Specialty:
AUTHORIZATION FOR RELEASE OF INFORMATION
I have read the forgoing release and authorization, understand its contents, and understand that I have a right to receive a copy of any findings resulting from this authorization.
Signature of Applicant: Dated:
REFERENCE CONTACT PERSON: Please complete this section and return this form to the applicant or fax to the above fax number.
Please indicate whether the above information is correct, including dates of employment Yes No
Is the person available for re-hire? Yes No
Additional comments regarding the applicant's professional abilities:
Title and Position of Reference Person:
Page 4
Alliance Healthcare, Inc.
I specifically authorize the persons listed above to release information for the purpose of verifying my past employment and any related information I have stated herein. I hereby release ALLIANCE HEALTHCARE, INC. and the persons or institutions listed above from any claims, damages, or liabili-ties that I, my heirs and assigns may have which may arise from the release of any of the above informa-tion.

Statement of Physical Examination andAuthorization for Release of Information
I, hereby authorize the person(s) and/or organization below (Name of Applicant or Employee)
I have read the foregoing release and authorizations, understand its contents, and understand that I have a right to receive a copy of this authorization.
Signature of Applicant or Employee Date
Examining Person*: Please complete the following or attach your facility's standard evaluation form.
"I have performed a medical physical examination of the person named above, and have determined she/he is capable of performing the essential functions of the job."
Name: Title*
Authorized Signature Date
Name of Facility or Organization
Please attach a separate sheet listing any accommodations required for the person named above to safely perform the essential job functions.
*Physician, Physician's Assistant or Nurse Practitioner
Page 5
Alliance Healthcare, Inc.
Title 22 of the State of California requires that all persons who work in the health care industry complete a Statement of Physical Examination upon hire and each year thereafter. The release of medical information related to the performance of your job to ALLIANCE HEALTHCARE, INC., and client facilities must also be authorized. Medical Examinations must be performed by a Physician, Physician's Assistant or Nurse Practitioner.
to release to ALLIANCE HEALTHCARE, INC. medical information relative to my being physically able to perform the functions of the job. I further authorize ALLIANCE HEALTH-CARE, INC. to release by medical information to its client hospitals.

PROOF OF MEDICAL
Forms need to be signed or copies of proof need tobe returned to ALLIANCE HEALTHCARE, INC.
Physical Exam: Proof of Physical Exam annually that you are fit to work according to your job description.
PPD: Proof of PPD every six months.
TB Questionnaire: Proof annually, only if you are positive.
Chest X-Ray: Proof every five years if you are TB positive.
Measles: Positive measles titer or certification of two doses of measles vaccine.
Mumps: Positive mumps titer or certification of mumps vaccine.
Rubella: Positive Rubella titer or certification of Rubella vaccine.
Varicella: Positive Varicella titer or certification of two doses of Varicella vaccine.
Hep B: Consent or declination form signed. Proof every five years.
Tetanus: Proof every ten years.
Drug Test*: Provide proof of successfully passing ten-panel drug screen as applies to position and facility worked.
*Drug Test is for certain hospitals only, call office for details. Page 6
Alliance Healthcare, Inc.

Please Read Carefully:
1) Physical examination results indicating fitness to work.
2) Proof of immunization for Rubella, Varicella and Mumps.
3) Tuberculosis screening and related health information, and indicate my consent to or decline of Hepatitis B vaccination.
4) My authorization to release the results of my physical exam toALLIANCE HEALTHCARE, INC. and its client hospitals.
5)
6) Completionof a 1 year trial period priorto being considered a designated employee of ALLIANCEHEALTHCARE, INC. benefits available following 90 days from date of hire.I understand that, at the end of my trial period, my job performance and qualifications will bereviewed by ALLIANCE HEALTHCARE, INC. and my final employment statuswill be determined.
7) Tetanus
I understand and agree that any and all items placed in my personnel file may be released toALLIANCE HEALTHCARE, INC. client hospitals where I have worked while employed byALLIANCE HEALTHCARE, INC..
By signing below, I certify that I have read the above statements and agree and understand them fully.
Signed DatePage 7
Alliance Healthcare, Inc. I hereby certify that the answers provided in the foregoing application, and skills checklist are true to the best of my knowledge and I agree to have all of the answers checked by ALLIANCE HEALTHCARE, INC. unless I have stated otherwise.
I understand that I have the right to request, and receive in writing, the results of any investigation by ALLI-ANCE HEALTHCARE, INC., regarding statements made by me on the foregoing application.
I understand that any falsification or misrepresentation of facts provided by me for the purpose of obtaining employment with ALLIANCE HEALTHCARE, INC. will be the basis for disqualification for hire or termination or employment should a job offer be made.
I understand that ALLIANCE HEALTHCARE, INC. has a two state hiring process, and that, upon acceptance of my application, I will receive a job offer letter from ALLIANCE HEALTHCARE, INC. stating my status at the time of hire, rate of pay, and conditions of employment. I understand the following will be required as a part of my successful completion of the hiring process:
I must read and agree to be bound by ALLIANCE HEALTHCARE, INC. Employee Handbook and Procedures.
I understand that any employment with ALLIANCE HEALTHCARE, INC. will be on an occasional per diem basis, which means that I may or may not receive assignments to work, depending on demand and my availability. I also understand that my acceptance of an offer of employment does not create a contrac-tual obligation upon ALLIANCE HEALTHCARE, INC. to continue to employ me in the future.

Proof of Immunization
Employees are required to complete the following regarding documentation of immunizations or exposures to the following diseases. If you have had the disease in the past, and vaccination certificates or titers are not provided, employees must provide location of medical records indicating vaccination or past exposure. Form for titers and vaccines must be completed by Physician, Physician's Assistant or Nurse Practitioner. "MMR" vaccines include Measles, Mumps, and Rubella.
I herby authorize the person and/or Organization Name of Applicant or Employee named below to release information regarding my immunization records to ALLIANCEHEALTHCARE, INC.
Employee Signature Date
Employee: Please complete the following if proof of titers or vaccines are not provided. "I certify I have had the following diseases in the past or have received vaccinations, and am immune to any exposure."
Signed:
Disease(s):
Location of medical records for proof of exposure:
Dates of exposure:
Medical Practioner: Please complete the following or provide standard form indicating immunizations or titers.
MEASLES (MMR): Vaccination Date(s): Results: Positive Rubeola titer or certification of two doses of measles vaccine Present Absent
MUMPS (MMR): Vaccination Date(s): Results: Positive Mumps titer or certification of two doses of measles vaccine Present Absent
RUBELLA (MMR): Vaccination Date(s): Results: Positive Rubella titer or certification of two doses of measles vaccine Present Absent
VARICELLA Vaccination Date(s): Results: Positive Varicella titer or certification of two doses of measles vaccine Present Absent
Signature of Physician, Physician's Assistant or Nurse Practitioner Date
Page 8
Alliance Healthcare, Inc.

Tuberculosis Health Questionnaire Only if PPD is positive
This questionnaire is for applicants/employees who have tested positive on the TB skin test. A positive skin test generally means that sometime during your life, you have come in contact with the tuberculosis bacteria. It does not mean you have tuberculosis disease now.
In the past, a yearly chest x-ray was thought to be sufficient follow-up. However, some persons may develop an active tuberculosis infection (relapse or reinfection) with a normal chest x-ray. Also, yearly chest x-rays may expose you to excess radiation over the course of a working career.
Consequently, this brief questionnaire is very important. You should answer all of the questions on this page. When you are finished, please return this form to ALLIANCE HEALTHCARE, INC.
DO YOU HAVE: Yes No
1. Productive cough which has lasted at least three weeks?
2. Persistent weight loss without dieting?
3. Persistent low-grade fever?
4. Night sweats?
5. Loss of appetite?
6. Swollen glands, usually in the neck?
7. Coughing up blood?
8. Shortness of breath?
9. Chest pain?
Employee name Date
Nurse Practitioner Date Or
Physician Date
Page 9
Alliance Healthcare, Inc.

Positive Chest X-Ray Only if PPD is positive
Employees with a documented" positive" PPD Skin Test history must have a current clear chest x-ray (defined as negative for active tuberculosis).
Employee Name: Date:
CHEST X-RAY: DATE:
RESULTS:
*Authorized Signature Date
*Physician, Physician's Assistant or Nurse Practitioner
Page 10
Alliance Healthcare, Inc.

HEPATITIS B VACCINE CONSENT/DECLINE FORM
Hepatitis B virus (HBV) is an important cause of viral hepatitis. An important method of transmission is from the blood of acutely or chronically infected people. Health care workers are at increased risk of HBV infection because of contact with blood products. The serious complications and results of HBV infection include liver damage, cirrhosis of the liver, chronic active hepatitis, cancer of the liver and death. Between 6% and 10% of young adults with HBV infection become carriers of hepatitis B virus. Chronic active hepatitis develops in over 25% of such carriers and often progresses to cirrhosis of the liver. Hepatitis B related liver cancer is developed by 4% of carriers. There is no specific treatment for hepatitis B infection.
The hepatitis B virus vaccine is 80-95% effective in preventing hepatitis in susceptible people. The vaccine is given intramuscularly in three doses, with the second and third doses given one and six months after the first dose. Recombinant hepatitis B vaccine is contraindicated in the presence of hypersensitivity to yeast or any component of the vaccine. The most common side effect has been limited to soreness or redness at the injection site. Systemic complaints could include fatigue/weakness, fever, headache, and malaise. Because of the long incubation period of hepatitis B it is possible for unrecognized infection to be present at the time the vaccine is given and vaccination may not prevent hepatitis B in these cases. The duration of protection is probably more than five years, but this or the need for boosters, has yet to be determined.
PLEASE INITIAL THE FOLLOWING TO INDICATE YOUR STATUS REGARDING HEPATITIS B VACCINATION.(You may decline the vaccination, or indicate that you have already received the vaccination)
HEPATITIS B VACCINE DECLINATION
I understand that due to my occupational exposure to blood or other potentially infectious material I may be at risk of acquiring hepatitis B virus (HBV) infection. I have been given the opportunity to be vaccinated with hepatitis B vaccine, at no charge to myself. However, I decline the hepatitis B vaccination at this time. I understand that by declining this vaccine, I continue to be at risk of acquiring hepatitis B, a serious disease. If in the future I continue to have occupational exposure to blood or other potentially infectious material and I want to be vaccinated with hepatitis B vaccine. I can receive the vaccination series at no charge to me.
I presently decline the hepatitis B vaccine or have already had the hepatitis B vaccine.
Date of previous vaccination (if applies)
PLEASE SIGN AND DATE THE FOLLOWING:I, the undersigned have read the above. I have had the opportunity to have my questions answered satisfactorily andhave indicated my preferences regarding vaccination. I understand the risks of exposure to hepatitis B and hold ALLIANCE HEALTHCARE, INC. , its employees, agents and clients harmless should I contract hepatitis B through my work activities as an employee of ALLIANCE HEALTHCARE, INC. I understand the risks and benefits of the hepatitis B vaccine and hold ALLIANCE HEALTHCARE, INC., its employees, agents and clients harmless should any complications or illness results from the vaccine being administered to me.
SIGNATURE DATE
Page 11
Alliance Healthcare, Inc.

AUTHORIZATION FOR JOB-RELATED DRUG TESTING AND RELEASE OF INFORMATION
Applicant's Name:
Social Security Number
I, , herby agree to submit to ALLIANCE HEALTHCARE , INC., the results from a ten-panel drug test by a NIDA-Certified laboratory to verify that I do not use illegal drugs or abuse prescription drugs as a condition of employment with certain clients of to ALLIANCE HEALTHCARE, INC.
I, specifically authorize the disclosure of the results of the drug test, to Employer, and to Employer's clients which require drug testing, for the purpose of ascertaining (1) whether I am able to safely perform all of the essential functions of the position, and (2) my compliance with any applicable drug free policies of Employer and of its clients.
I understand that the results will be confidential and, if I am hired, will be placed in my personnel file. I agree that this authorization shall remain valid for six (6) months, or for the duration of my employment by Employer, whichever is longer. I agree that a copy of this authorization is of the same force and of effect as the original and may be used as the original.
I herby release Employer from any and all claims, damages, or liabilities of any kind that I, my heirs and assigns may have, which may arise in any way out of the (1) drug testing, and (2) release to Employer or to its clients of the drug testing information and results. I herby authorize release of the results of the drug testing to Employer and to its clients, which require drug testing.
I have read the foregoing release and authorization, understand its contents, agree to its terms and understand that I have a right to a copy of this authorization.
Date: Signature of Employee
Page 12
Alliance Healthcare, Inc.

Respiratory Care Practitioner Skills Proficiency Checklist
Directions: By accurately filling out this checklist, you will help us match your skills and interest with available assignments at our client hospital. For "Work Settings", place an "X" in the column that most accurately indicates your number of years experience in each area. For "Work Activities", indicate your level of experience in the appropriate column. Skills checklists are renewed annually. Be sure to place your name and date on each page.
Years of Experience 1. WORK SETTINGS 6 mos-2 years 2-5 years 5-10 years 10 +years
tinU eraC evisnetnI .1 tinU eraC yranoroC .2 tinU eraC orueN .3 mooR ycnegremE .4 cirtaideP .5 UCI cirtaideP .6 UCI latanoeN .7
8. General Medical/Surgical Services 9. Pulmonary Function Lab
)tnafnI( tropsnarT .01 )tludA(
11. Skilled Nursing Facility/Transitional Care eraC emoH .21
13. Pulmonary Rehabilitation tinU eraC nruB .41 baL peelS .51
Applicant/Employee Name: Date:
Page 13
Alliance Healthcare, Inc.

LEVEL ECNEIREPXE SEITIVITCA KROW .2
A. Basic RT Extensive/ Current
Frequent/Recent
Infrequent/ Occasional
Noexperience
1. Incentive Spirometry tnemtaerT BPPI .2
3. Hand Held Nebulizer 4. Ultrsonic Nebulizer-Sputum Induction 5. Postural Drainage & Percussion
gnitnilpS .6 7. Purse-Lip Breathing 8. Diaphragmatic Breathing 9. Bedside PFT (List Types)
yparehT PEP .01 evlaV rettulF .11 etaR wolF kaeP .21
B. Airway Management yawriA laegnyrahP .1 yawriA larO .2
3. Tracheostomy Tubes 4. Esophageal Obturator
ffuC maoF .5 6. Fenestrated Tracheostomy Tube
nottuB hcarT .7 noitabutxE .8
9. Intubation/Assist/Taping For Securing 10. Check Intracuff Pressure 11. Nasal & Endotracheal Suction
nottuB fo noitresnI .21 evlaV riuM yssaP .31 klaT hcarT .41 eraC hcarT .51
C. Ventilators Neg. & Pos. Pressure gnuL norI .1 ssariuC tsehC .2
3. Bennett MA - 1 & 2 nahganoM .4
5. Seimens Servo 900B/900C/300/300A 5 ,3 ,2 ,1 - sraeB .6 seireS 0027 BP .7
8. Bird 6400 ST/ST 8400 notlimaH .9
10. Drager Evita/Evita Dura 2 /Evita 4 11. BIPAP12. Nasal /Mask CPAP 13. Infrasonics Adult Star
Extensive/Current = Have extensive experience and is currently working in activity. Frequent/Recent = Frequently performs activity and have performed in last six months. Infrequent/Occasional = Work activity performed occasionally over past two years, not in last six months. No Experience = Have not performed work activity.
Applicant/Employee Name: Date:
Page 14
Alliance Healthcare, Inc.
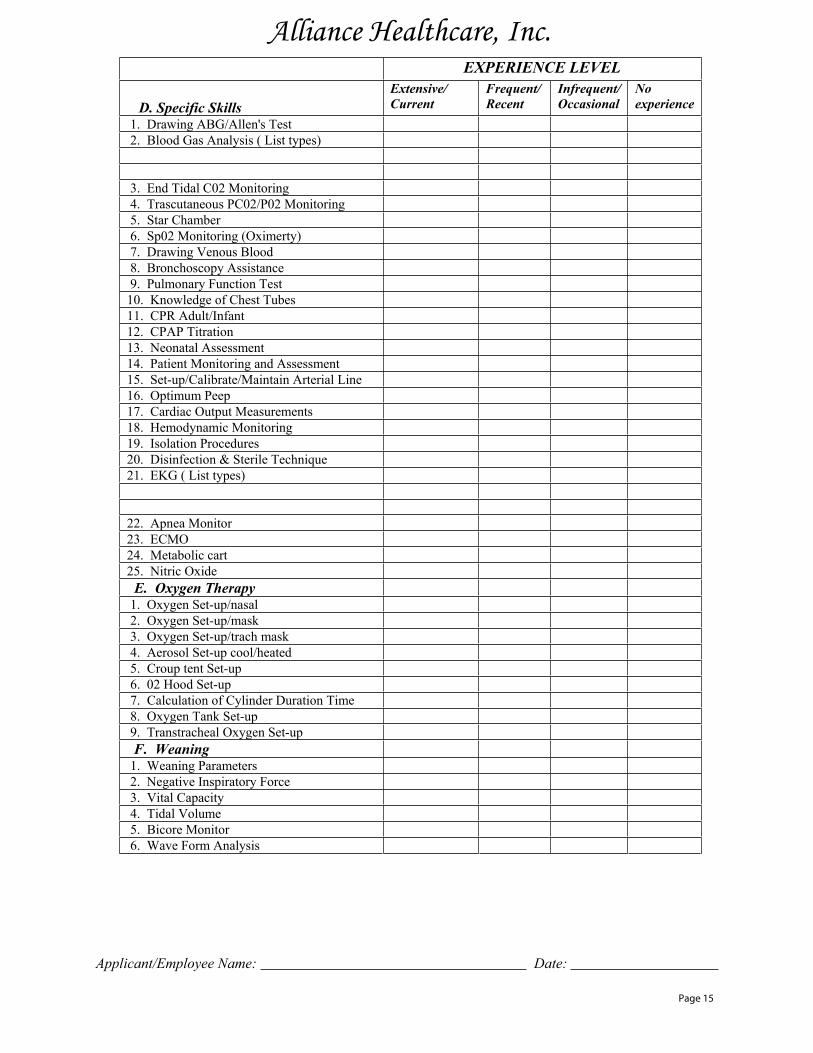
LEVEL ECNEIREPXE
D. Specific Skills Extensive/ Current
Frequent/Recent
Infrequent/ Occasional
Noexperience
1. Drawing ABG/Allen's Test 2. Blood Gas Analysis ( List types)
3. End Tidal C02 Monitoring 4. Trascutaneous PC02/P02 Monitoring
rebmahC ratS .5 6. Sp02 Monitoring (Oximerty) 7. Drawing Venous Blood 8. Bronchoscopy Assistance 9. Pulmonary Function Test 10. Knowledge of Chest Tubes
tnafnI/tludA RPC .11 noitartiT PAPC .21
13. Neonatal Assessment 14. Patient Monitoring and Assessment 15. Set-up/Calibrate/Maintain Arterial Line
peeP mumitpO .6117. Cardiac Output Measurements 18. Hemodynamic Monitoring 19. Isolation Procedures 20. Disinfection & Sterile Technique
)sepyt tsiL ( GKE .12 rotinoM aenpA .22 OMCE .32 trac cilobateM .42 edixO cirtiN .52
E. Oxygen Therapy 1. Oxygen Set-up/nasal 2. Oxygen Set-up/mask 3. Oxygen Set-up/trach mask 4. Aerosol Set-up cool/heated
pu-teS tnet puorC .5 pu-teS dooH 20 .6
7. Calculation of Cylinder Duration Time 8. Oxygen Tank Set-up 9. Transtracheal Oxygen Set-up F. Weaning 1. Weaning Parameters 2. Negative Inspiratory Force
yticapaC latiV .3 emuloV ladiT .4 rotinoM erociB .5
6. Wave Form Analysis
Applicant/Employee Name: Date:
Page 15
Alliance Healthcare, Inc.

Alliance Healthcare, Inc. LEVEL ECNEIREPXE
G. Neonatal/Pediatric Ventilators Extensive/ Current
Frequent/Recent
Infrequent/ Occasional
Noexperience 051-401 SL sunoB .1 driB ybaB .2 002 PB snruoB .3
4. Bear Cub Infant BP 2001 5. Sechrist IV - 100 & 100B
A2 driB ybaB .6 7. Infrasonics Infant Star/High Freq/Star Sync.
goL ybaB regarD .8 9. Sensormedics 3100/3100 A
driB PIV .01 H. Transport and Homecare Ventilators
01-6 PL tscudorP efiL .1 2. Life Care PVV/PLV 100-102
33 raeB .3 4. Puritan -Bennett Companion/PB 740
tropweN .5 I. Medications
1. Racemic Epinephrine (vaponephrine) 2. Isopreterenol (Isuprel) 3. Isoetharine (Bronkosol) 4. Metaproteronal (Alupent) 5. Salbutamol (Albuterol, Proventil, Ventolin) 6. Levalbuterol (Xopenex)
niravobiR .7 relahnI esoD dereteM .8 tnev-olF .9
10. Terbutaline Sulfate (Bricanyl) etafluS eniportA .11 etanobraciB .21 tsymocuM .31
14. Cromolyn Sodium (Intal) 15. Beclomethasone (Aerobid/Vanceril) 16. Atrovent (Ipatroprium Bromide)
tnevoreS .71 trocamzA .81 tnevibmoC .91 enidimatneP .02
21. Aerosolized Antibiotics Vancomycin Tobramycin Amphotericin J. Computers
noisivinilC .1 )sepyt tsiL( srehtO .2
Applicant/Employee Name: Date:
Page 16

Form W-4 (2007) Purpose. Complete Form W-4 so that youremployer can withhold the correct federal incometax from your pay. Because your tax situationmay change, you may want to refigure yourwithholding each year.
Head of household. Generally, you may claimhead of household filing status on your taxreturn only if you are unmarried and pay morethan 50% of the costs of keeping up a homefor yourself and your dependent(s) or otherqualifying individuals.
Exemption from withholding. If you areexempt, complete only lines 1, 2, 3, 4, and 7and sign the form to validate it. Yourexemption for 2007 expires February 16, 2008.See Pub. 505, Tax Withholding and EstimatedTax.
Check your withholding. After your Form W-4takes effect, use Pub. 919 to see how thedollar amount you are having withheldcompares to your projected total tax for 2007.See Pub. 919, especially if your earningsexceed $130,000 (Single) or $180,000(Married).
Basic instructions. If you are not exempt,complete the Personal AllowancesWorksheet below. The worksheets on page 2adjust your withholding allowances based on
Two earners/Multiple jobs. If you have aworking spouse or more than one job, figurethe total number of allowances you are entitledto claim on all jobs using worksheets from onlyone Form W-4. Your withholding usually willbe most accurate when all allowances areclaimed on the Form W-4 for the highestpaying job and zero allowances are claimed onthe others.
Personal Allowances Worksheet (Keep for your records.) Enter “1” for yourself if no one else can claim you as a dependent
A
A ● You are single and have only one job; or
Enter “1” if:
B
● You are married, have only one job, and your spouse does not work; or
B ● Your wages from a second job or your spouse’s wages (or the total of both) are $1,000 or less.
$ % Enter “1” for your spouse. But, you may choose to enter “-0-” if you are married and have either a working spouse ormore than one job. (Entering “-0-” may help you avoid having too little tax withheld.)
C C
Enter number of dependents (other than your spouse or yourself) you will claim on your tax return
D
D E
E F
F
Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.) ©
H
H ● If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions
and Adjustments Worksheet on page 2.
For accuracy,complete allworksheetsthat apply.
● If you have more than one job or are married and you and your spouse both work and the combined earnings from all jobsexceed $40,000 ($25,000 if married) see the Two-Earners/Multiple Jobs Worksheet on page 2 to avoid having too little tax withheld.
● If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.
$ Cut here and give Form W-4 to your employer. Keep the top part for your records.
OMB No. 1545-0074 Employee’s Withholding Allowance Certificate
W-4
Form Department of the TreasuryInternal Revenue Service
© Whether you are entitled to claim a certain number of allowances or exemption from withholding issubject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
Type or print your first name and middle initial.
1
Last name
2
Your social security number
Home address (number and street or rural route)
Married
Single
3
Married, but withhold at higher Single rate.
City or town, state, and ZIP code
Note. If married, but legally separated, or spouse is a nonresident alien, check the “Single” box.
5
5
Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) $ 6
6
Additional amount, if any, you want withheld from each paycheck 7
I claim exemption from withholding for 2007, and I certify that I meet both of the following conditions for exemption.
● Last year I had a right to a refund of all federal income tax withheld because I had no tax liability and ● This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.
7
If you meet both conditions, write “Exempt” here ©
8
Under penalties of perjury, I declare that I have examined this certificate and to the best of my knowledge and belief, it is true, correct, and complete. Employee’s signature(Form is not validunless you sign it.) ©
Date ©
9
Employer identification number (EIN)
Employer’s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.)
Office code (optional)
10
Enter “1” if you have at least $1,500 of child or dependent care expenses for which you plan to claim a credit
4
If your last name differs from that shown on your social security card,check here. You must call 1-800-772-1213 for a replacement card. ©
Cat. No. 10220Q
Enter “1” if you will file as head of household on your tax return (see conditions under Head of household above)
Note. You cannot claim exemption fromwithholding if (a) your income exceeds $850and includes more than $300 of unearnedincome (for example, interest and dividends)and (b) another person can claim you as adependent on their tax return. Nonwage income. If you have a large amount
of nonwage income, such as interest ordividends, consider making estimated taxpayments using Form 1040-ES, Estimated Tax
G
Child Tax Credit (including additional child tax credit). See Pub 972, Child Tax Credit, for more information.
G
● If your total income will be between $57,000 and $84,000 ($85,000 and $119,000 if married), enter “1” for each eligible child plus “1” additional if you have 4 or more eligible children.
● If your total income will be less than $57,000 ($85,000 if married), enter “2” for each eligible child.
(Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.)
Tax credits. You can take projected taxcredits into account in figuring your allowablenumber of withholding allowances. Credits forchild or dependent care expenses and thechild tax credit may be claimed using thePersonal Allowances Worksheet below. SeePub. 919, How Do I Adjust My TaxWithholding, for information on convertingyour other credits into withholding allowances.
Nonresident alien. If you are a nonresidentalien, see the Instructions for Form 8233before completing this Form W-4.
For Privacy Act and Paperwork Reduction Act Notice, see page 2.
Form W-4 (2007)
2007
itemized deductions, certain credits,adjustments to income, or two-earner/multiplejob situations. Complete all worksheets thatapply. However, you may claim fewer (or zero)allowances.
for Individuals. Otherwise, you may oweadditional tax. If you have pension or annuityincome, see Pub. 919 to find out if you shouldadjust your withholding on Form W-4 or W-4P.

Page 2
Form W-4 (2007)
Deductions and Adjustments Worksheet Note. Use this worksheet only if you plan to itemize deductions, claim certain credits, or claim adjustments to income on your 2007 tax return.
Enter an estimate of your 2007 itemized deductions. These include qualifying home mortgage interest,charitable contributions, state and local taxes, medical expenses in excess of 7.5% of your income, and miscellaneous deductions. (For 2007, you may have to reduce your itemized deductions if your incomeis over $156,400 ($78,200 if married filing separately). See Worksheet 2 in Pub. 919 for details.)
1
$ 1 $10,700 if married filing jointly or qualifying widow(er)
$ $ 7,850 if head of household
2
Enter:
2 $ 5,350 if single or married filing separately
%
$
$ 3
Subtract line 2 from line 1. If zero or less, enter “-0-”
3 $ Enter an estimate of your 2007 adjustments to income, including alimony, deductible IRA contributions, and student loan interest
4 $ 5
Add lines 3 and 4 and enter the total. (Include any amount for credits from Worksheet 8 in Pub. 919)
5 $ 6
Enter an estimate of your 2007 nonwage income (such as dividends or interest)
6 $ 7
Subtract line 6 from line 5. If zero or less, enter “-0-”
7 Divide the amount on line 7 by $3,400 and enter the result here. Drop any fraction
8
8 Enter the number from the Personal Allowances Worksheet, line H, page 1
9
9 Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet,
also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1
10 10
Two-Earners/Multiple Jobs Worksheet (See Two earners/multiple jobs on page 1.) Note. Use this worksheet only if the instructions under line H on page 1 direct you here.
1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet)
1 2
Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $50,000 or less, do not enter more than “3.”
2 3
If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter“-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet
3 Note. If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4–9 below to calculate the additional
withholding amount necessary to avoid a year-end tax bill. Enter the number from line 2 of this worksheet
4
4 Enter the number from line 1 of this worksheet
5
5 Subtract line 5 from line 4
6
6 $ Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here
7
7 $ Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed
8
8 Divide line 8 by the number of pay periods remaining in 2007. For example, divide by 26 if you are paid
every two weeks and you complete this form in December 2006. Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck
9
$ 9
Privacy Act and Paperwork Reduction Act Notice. We ask for the informationon this form to carry out the Internal Revenue laws of the United States. TheInternal Revenue Code requires this information under sections 3402(f)(2)(A) and6109 and their regulations. Failure to provide a properly completed form willresult in your being treated as a single person who claims no withholdingallowances; providing fraudulent information may also subject you to penalties.Routine uses of this information include giving it to the Department of Justice forcivil and criminal litigation, to cities, states, and the District of Columbia for use inadministering their tax laws, and using it in the National Directory of New Hires.We may also disclose this information to other countries under a tax treaty, tofederal and state agencies to enforce federal nontax criminal laws, or to federallaw enforcement and intelligence agencies to combat terrorism.
The average time and expenses required to complete and file this form will varydepending on individual circumstances. For estimated averages, see theinstructions for your income tax return.
4
Table 1 All Others
Married Filing Jointly
If wages from LOWESTpaying job are—
Table 2 All Others
Married Filing Jointly
If wages from HIGHESTpaying job are—
Enter online 7 above
If wages from HIGHESTpaying job are—
Enter online 7 above
Enter online 2 above
If wages from LOWESTpaying job are—
You are not required to provide the information requested on a form that issubject to the Paperwork Reduction Act unless the form displays a valid OMBcontrol number. Books or records relating to a form or its instructions must beretained as long as their contents may become material in the administration ofany Internal Revenue law. Generally, tax returns and return information areconfidential, as required by Code section 6103.
Enter online 2 above
0123456789
10
If you have suggestions for making this form simpler, we would be happy to hearfrom you. See the instructions for your income tax return.
$0 -4,501 -9,001 -
18,001 -22,001 -26,001 -32,001 -38,001 -46,001 -55,001 -60,001 -65,001 -75,001 -95,001 -
105,001 -
$4,5009,000
18,00022,00026,00032,00038,00046,00055,00060,00065,00075,00095,000
105,000120,000 120,001 and over
0123456789
101112131415
$0 -6,001 -
12,001 -19,001 -26,001 -35,001 -50,001 -65,001 -80,001 -90,001 -
$6,00012,00019,00026,00035,00050,00065,00080,00090,000
120,000 120,001 and over
$0 -65,001 -
120,001 -170,001 -
$510850950
1,1201,190
300,001 and over
$65,000120,000170,000300,000
$0 -35,001 -80,001 -
150,001 -
$510850950
1,1201,190
340,001 and over
$35,00080,000
150,000340,000

A citizen or national of the United States
Please read instructions carefully before completing this form. The instructions must be available during completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work eligible individuals. Employers CANNOT specify which document(s) they will accept from an employee. The refusal to hire an individual because of a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Verification. To be completed and signed by employee at the time employment begins.
Print Name: Last First Middle Initial Maiden Name
Address (Street Name and Number) Apt. #
(month/day/year)
Date of Birth (month/day/year)
StateCity Zip Code Social Security #
CERTIFICATION - I attest, under penalty of perjury, that I have examined the document(s) presented by the above-named
Address (Street Name and Number, City, State, Zip Code)
and that to the best of my knowledge the employee
I attest, under penalty of perjury, that I am (check one of the following): I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
A Lawful Permanent Resident (Alien # AAn alien authorized to work until / /
(Alien # or Admission #)
is eligible to work in the United States. (State employment agencies may omit the date the employee began
Employee's Signature Date (month/day/year)
Preparer and/or Translator Certification. (To be completed and signed if Section 1 is prepared by a personother than the employee.) I attest, under penalty of perjury, that I have assisted in the completion of this form and that to the best of my knowledge the information is true and correct.
/
Print NamePreparer's/Translator's Signature
/
Date (month/day/year)
Section 2. Employer Review and Verification. To be completed and signed by employer. Examine one document from List A ORexamine one document from List B and one from List C, as listed on the reverse of this form, and record the title, number and expiration date, if any, of the document(s)
ANDList B List CORList A
Document title:
Issuing authority:
Document #:
Expiration Date (if any):
Document #:
//
Print Name TitleSignature of Employer or Authorized Representative
Address (Street Name and Number, City, State, Zip Code) Date (month/day/year)Business or Organization Name
Section 3. Updating and Reverification. To be completed and signed by employer.
B. Date of rehire (month/day/year) (if applicable)A. New Name (if applicable)
C. If employee's previous grant of work authorization has expired, provide the information below for the document that establishes current employmenteligibility.
Document #: Expiration Date (if any):Document Title:
l attest, under penalty of perjury, that to the best of my knowledge, this employee is eligible to work in the United States, and if the employee presented document(s), the document(s) l have examined appear to be genuine and to relate to the individual.
Date (month/day/year)Signature of Employer or Authorized Representative
Form I-9 (Rev. 11-21-91)N Page 2
Employment Eligibility Verification
employee began employment on
employment.)
OMB No. 1115-0136U.S. Department of JusticeImmigration and Naturalization Service
Expiration Date (if any): / /
/ / / /
employee, that the above-listed document(s) appear to be genuine and to relate to the employee named, that the
/ /
Page 19

Alliance Healthcare, Inc.
LISTS OF ACCEPTABLE DOCUMENTS
LIST A LIST B LIST C
Documents that Establish Documents that Establish
OR Identity AND
(INS Form N-560 or N-561)2. Certi�cate of U.S. Citizenship
Identity and EmploymentEligibility
7. Unexpired employment
1. Driver's license or ID card 1. U.S. social security card issued
9. Driver's license issued by a Canadian government authority
1. U.S. Passport (unexpired or
I-688A)
issued by a state or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color and address
by the Social Security Administration (other than a card stating it is not valid for employment)
Card (INS Form I-688)
expired)
photograph
Form I-327)
Document (INS Form I-571)
Employment Eligibility
(INS Form N-550 or N-570)
2. Certi�cation of Birth Abroad3. Certi�cate of Naturalization 2. ID card issued by federal, state issued by the Department of
State (Form FS-545 or Form DS-1350)
or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color and address
4. Unexpired foreign passport,with I-551 stamp or attached INS Form I-94 indicating unexpired employment authorization
3. Original or certi�ed copy of abirth certi�cate issued by a state, county, municipal authority or outlying possession of the United States bearing an o�cial seal
3. School ID card with a
5. Permanent Resident Card orAlien Registration Receipt Card
with photograph (INS Form I-151 or I-551)
4. Voter's registration card
5. U.S. Military card or draft record
6. Military dependent's ID card 4. Native American tribal document6. Unex pired Tem porar y Resident
7. U.S. Coast Guard Merchant Mariner Card
5. U.S. Citizen ID Card (INS Form7. Unexpired Employment
I-197)8. Native American tribal documentAuthorization Card (INS Form
6. ID Card for use of Resident8. Unexpired Reentry Permit (INS Citizen in the United States
(INS Form I-179)are unable to present a document listed above:
For persons under age 18 who
9. Unexpired Refugee Travel
authorization document issued by the INS (other than those listed under List A)
10. School record or report card10. Unexpired EmploymentAuthorization Document issued by the INS which contains a photograph (INS Form I-688B)
11. Clinic, doctor or hospital record
12. Day-care or nursery schoolrecord
Form I-9 (Rev. 10/4/00)Y Page 3
Illustrations of many of these documents appear in Part 8 of the Handbook for Employers (M-274)
Documents that Establish Both
Page 20

ALLIANCE HEALTHCARE, INC.
2763 East Shaw Avenue, Suite 106 Fresno CA 93710 877-753-8517
Authorization for Direct Deposit
This authorizes Alliance Healthcare, Inc. (the Company) to send credit entries (and appropriate debit and adjustment entries), electronically or by any other commercially accepted method to my (our) account(s) indicated below and to other accounts, I (we) identify in the future (the “Account”). This authorizes the financial institution holding the Account to post all such entries.
ACCOUNT #1 ____________________________ _______________________________ Name of Bank Type of Account – Checking or Savings ________________________________________________________________ Address of Bank City, State ____________________________ _______________________________ Bank Routing # Account #
ACCOUNT #2
____________________________ _______________________________ Name of Bank Type of Account – Checking or Savings ________________________________________________________________ Address of Bank City, State ____________________________ _______________________________ Bank Routing # Account #
This authorization will be in effect until the Company receives a written termination notice from myself and has a reasonable opportunity to act on it.
_____________________________ _________________________________ Signature Printed Name Date
Alliance Healthcare, Inc. 9/05