aim of masterclass
TRANSCRIPT

AIM OF MASTERCLASS
•Overview of the diabetic foot disease
•Modern approach to management
DIABETIC FOOT DISEASE
THROUGHOUT THE WORLD, THERE IS AN AMPUTATION EVERY 20 SECONDS
MOST OF THESE AMPUTATIONS ARE PREVENTABLE !!!!!!

DIABETIC FOOT DISEASE
What is the cause of these amputations?
• Natural history can be rapidly progressive quickly leading to necrosis
• This speed of progress coupled with any delay in diagnosis can result in overwhelming tissue destruction

WHY SUCH A SITUATION? Three great pathologies
Primary
• Neuropathy
• Ischaemia
Secondary
• Infection
Approx. 60 to 70 per cent
of people with diabetes
have some form of nerve
damage.
Diabetic neuropathy

PERIPHERAL NERVOUS SYSTEM
• Peripheral nervous system is an early warning system
• To detect external insults to the body and internal malfunctions within
• It is programmed to direct appropriate protective responses
• To maintain the homeostatic integrity of the body.

• The signs and symptoms of external physical insults and also internal malfunction are minimal
• Homeostasis is lost
• Diagnosis of disease is delayed
• Thus the window of opportunity for intervention is missed
• The end stage of tissue death is quickly reached.
Impact of Neuropathy

DIAGNOSIS
• Monofilaments
• Vibration threshold
Monofilaments
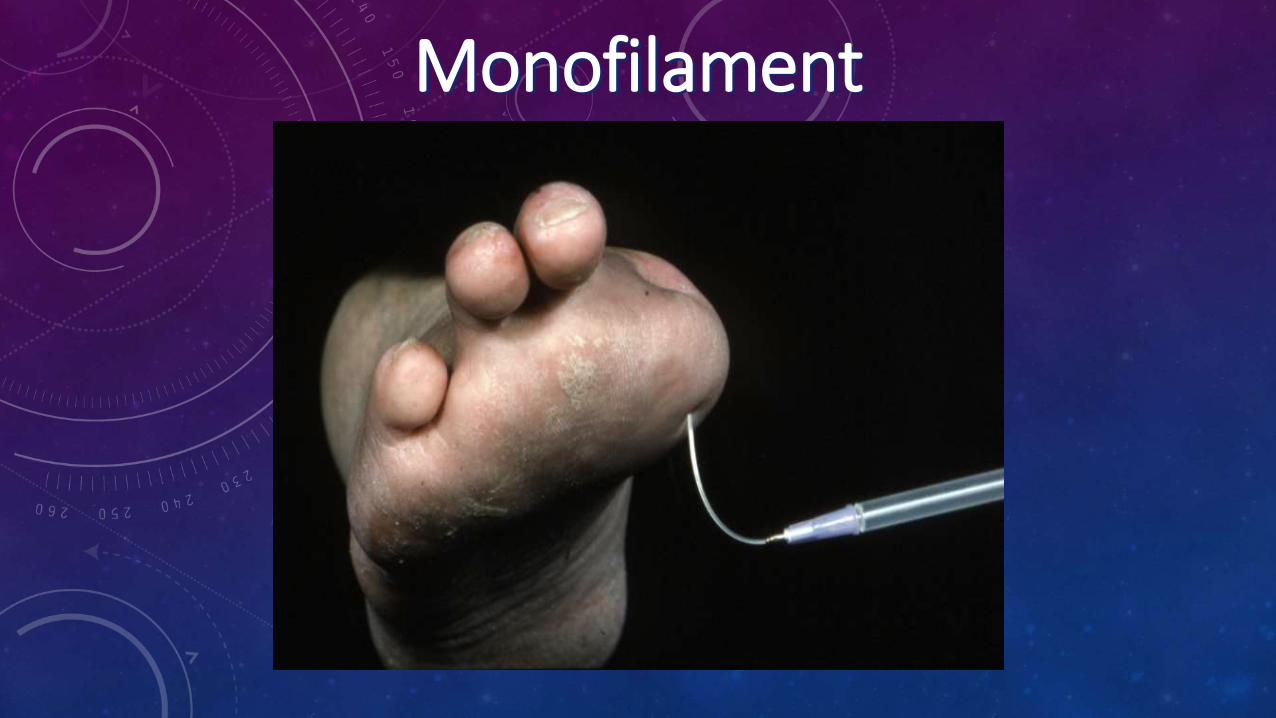
Monofilament

NEUROTHESIOMETER

IMPACT OF NEUROPATHY
• Inability to respond appropriately to stresses/ insults
• Physical trauma
• Bacterial invasion

NEUROPATHIC FOOT ULCER

Pathogenesis of neuropathic ulcer
CourtesyL. Delbridge,G. Ctercteko,

CALLUS IN NEUROPATHIC FOOT

NEUROPATHIC ULCER

CHARCOT FOOT



A Red Hot Swollen Foot should be considered as a Charcot
foot until proved otherwise!
High index of Clinical Suspicion

RESPONSE TO BACTERIAL INVASION
• No rubor
• No calor
• No dolor
• Diabetic foot infections do not always present with the classical signs of local infection as indicated by inflammation
RESPONSE TO BACTERIAL INVASION
Diabetic foot infections do not always
present with the classical signs of
systemic infection
Impaired innate immune response
No leucocytosis and fever

DIGITAL NECROSIS
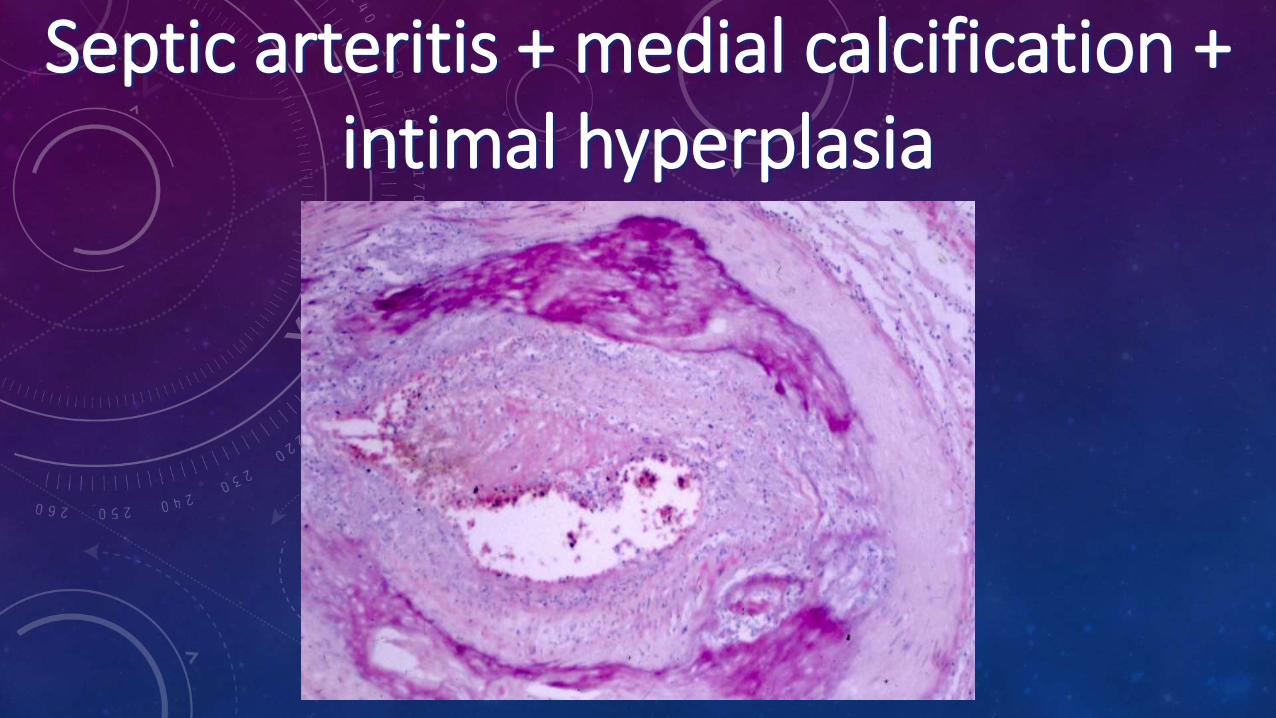
Septic arteritis + medial calcification + intimal hyperplasia
IMPACT OF NEUROPATHY
• Trauma No awareness
• Infection No tenderness or fever
• Gangrene No pain
• Heart attack No chest discomfort
• Hypoglycaemia No warnings

Classical Medicine
Symptoms and Signs
Investigations
Diagnosis
Treatment
Healing
Neuropathy
No Symptoms and Signs
No Investigations
No Diagnosis
No Treatment
Tissue Death
Neuropathic Medicine
Minimal Symptoms and Signs
Imaging/ Lab.Tests
Diagnosis
Treatment
Healing

NEUROPATHIC MEDICINE
• Meticulous assessment to recognise subtle symptoms and signs.
• Prompt use of imaging to provide “picture” of what is going on inside the body (in the presence of neuropathy, this information is absent )
• Attention to serum inflammatory markers.
ISCHAEMIA
• Macrovascular complications
• Ischaemic heart disease
• Cerebrovascular disease
• Peripheral vascular disease

DISTRIBUTION OF DISEASE
EJVS Diehm et al. 2005







ASSESSMENT OF ISCHAEMIA

Transcutaneous oxygenCritical ischaemia < 30mmHg

TOE PRESSURECRITICAL ISCHAEMIA < 30MMHG

Neuroischaemic Foot
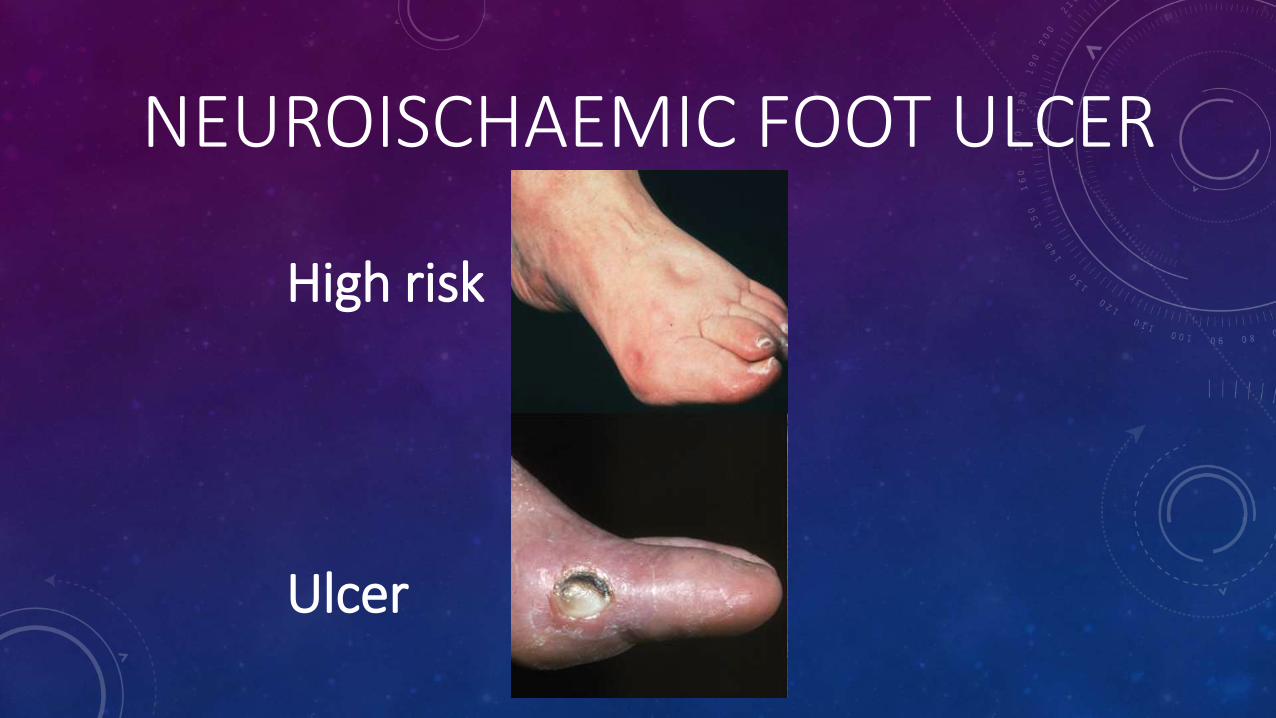
NEUROISCHAEMIC FOOT ULCER
High risk
Ulcer


Early neuroischaemic lesion


SIMPLE CLASSIFICATION
•Neuropathic foot
• Ischaemic foot
STRATIFICATION OF DIABETIC FOOT• Neuropathic Foot• Neuropathic ulcerated foot• Charcot foot
• Ischaemic Foot• Neuroischaemic foot• Critically ischaemic foot• Acutely ischaemic foot• Renal ischaemic foot

SIMPLE STAGING SYSTEM
1 Normal
2 High risk
3 Ulcerated
4 Infected
5 Necrotic

NeuroischaemicCharcot Criticalischaemic
Acuteischaemic
RenalischaemicStage
2
3
4
5
Neuropathic

DIABETIC FOOT TEAM• Podiatrist
• Nurse
• Orthotist
• Physiotherapist
• Surgeon
• Radiologist
• Diabetologist

MULTIDISCIPLINARY CARE
• Wound
• Vascular
• Microbiological
• Mechanical
• Metabolic
• Educational

TYPES OF ULCERATION
•Neuropathic Ulceration
•Neuroischaemic Ulceration

NEUROPATHIC ULCER
• Painless
• Apex of toe
• Prominent Plantar Metatarsal heads
• Heavy callus build up around the periphery
• Important to probe ulcer

NEUROPATHIC FOOT ULCERS
• Mechanical Control
• Redistribute plantar pressures

NEUROPATHIC ULCER

NEUROPATHIC ULCER

POST DEBRIDEMENT

REDISTRIBUTIVE PADDING

AIRCAST WALKER
• Prefabricated walking cast
• Bivalved cast with Velcro strapping lined with 4 air cells which can be inflated with a hand pump through 4 valves to ensure a close fit
• Flat plastazote insole which can be replaced with a cradled insole
• Won’t accommodate deformity
• Removable!!!

AIRCAST BOOT

TOTAL CONTACT CAST
• Gold standard treatment for the ulcerated neuropathic foot
• Very efficient method of redistributing plantar pressure
• Acute charcot osteoarthropathy
• Training required
• Kings Casting Course contact:
• Maureen Bates (0203 299 3223)

TOTAL CONTACT CAST


BIVALVED CAST

NEUROISCHAEMIC ULCER
•Margins of the foot•Apices of toes• Subungual Ulcers• Shallow Ulcers• Little callus build up

NEUROISCHAEMIC ULCER

NEUROISCHAEMIC ULCER

POST DEBRIDEMENT

NEUROISCHAEMIC ULCER

CRITICALLY ISCHAEMIC FOOT



TREATING PERIPHERAL CIRCULATION


Ulcer at 12 weeks


SCOTCH CAST BOOT
• Simple, removable boot made of stockinette, felt, softban and cast tape.
• Ideal for neuroischaemic ulcers as padded on borders/margins of the foot.
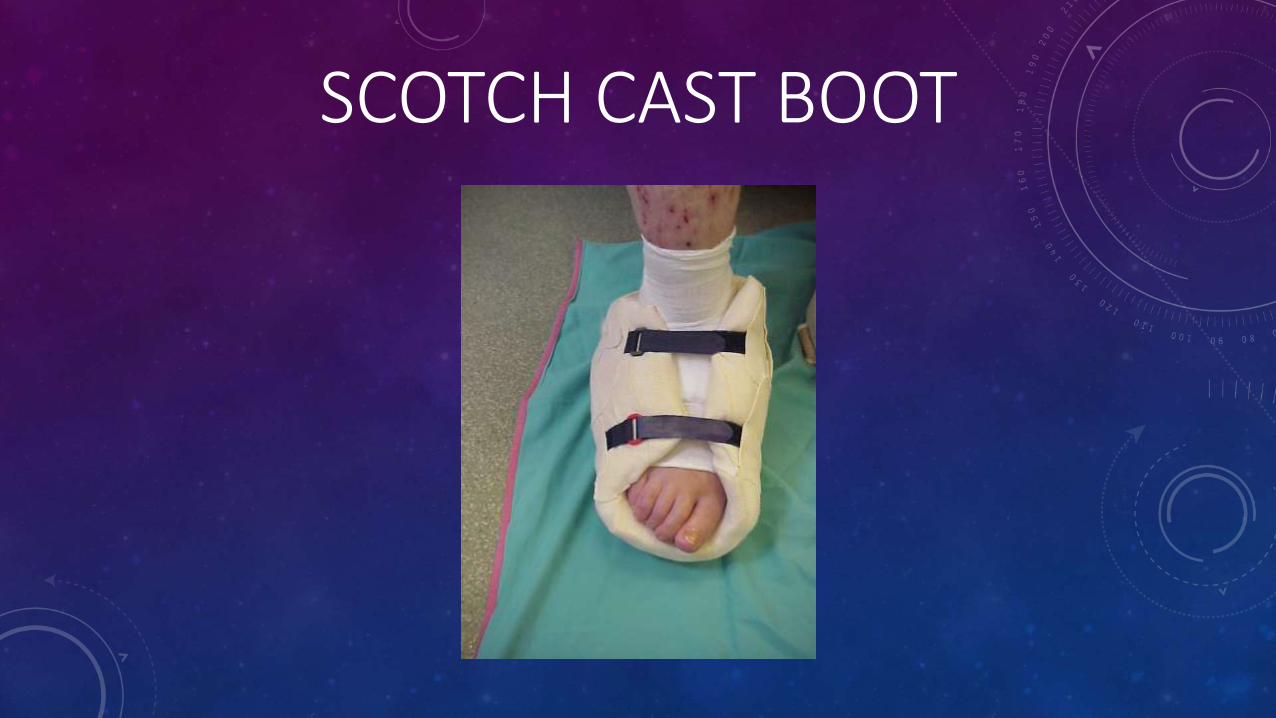
SCOTCH CAST BOOT

Scotchcast boot Bespoke Shoe

DARCO
ACUTE CHARCOT OSTEOARTHROPATHY
• CHARCOT
• Bone & joint destruction that occurs in the neuropathic foot
• 3 phases:
• Acute charcot
• Bony destruction/deformity
• Stabilization

ACUTE CHARCOT
• Red
• Hot
• Swollen
• Sometimes painful (30% patients)
• History of minor trauma
• Post surgical debridment

INVESTIGATIONS
• X Ray – normal
• Bone Scan – hot spots, early evidence of bone destruction
• MRI



CASE STUDY MALE, AGE 70, TYPE 2, DURATION OF DIABETES - 5 YEARS;
SWELLING OF LEFT FOOT
Hot swollen left foot Normal X -ray Hot bone scan



CASE STUDY TREATMENT: TOTAL CONTACT CAST (8 MONTHS)
Mid-tarsal bone sclerosis Preserved arch
ACUTE CHARCOT
•Total Contact Cast (TCC)
•Crutches
•Reduce Activity


CASE STUDY 1• Type 1- diagnosed 1983
• Female
• Age 49
• Smoker
• Hep C
• Right foot Charcot
• Chronic lateral malleoli ulceration since 1990
• Offered an amputation at another hospital
• Referred to King’s 1995
PROBLEM LIST
• Peripheral neuropthy
• Retinopathy
• CKD stage 3
• Chronic hep C

• Casting • Patient active• Had a young daughter• Foot became more unstable• Severely inverted and infected 2012• Occluded Superficial femoral artery• Superficial femoral artery endarterectomy
and femoral to popliteal artery bypass

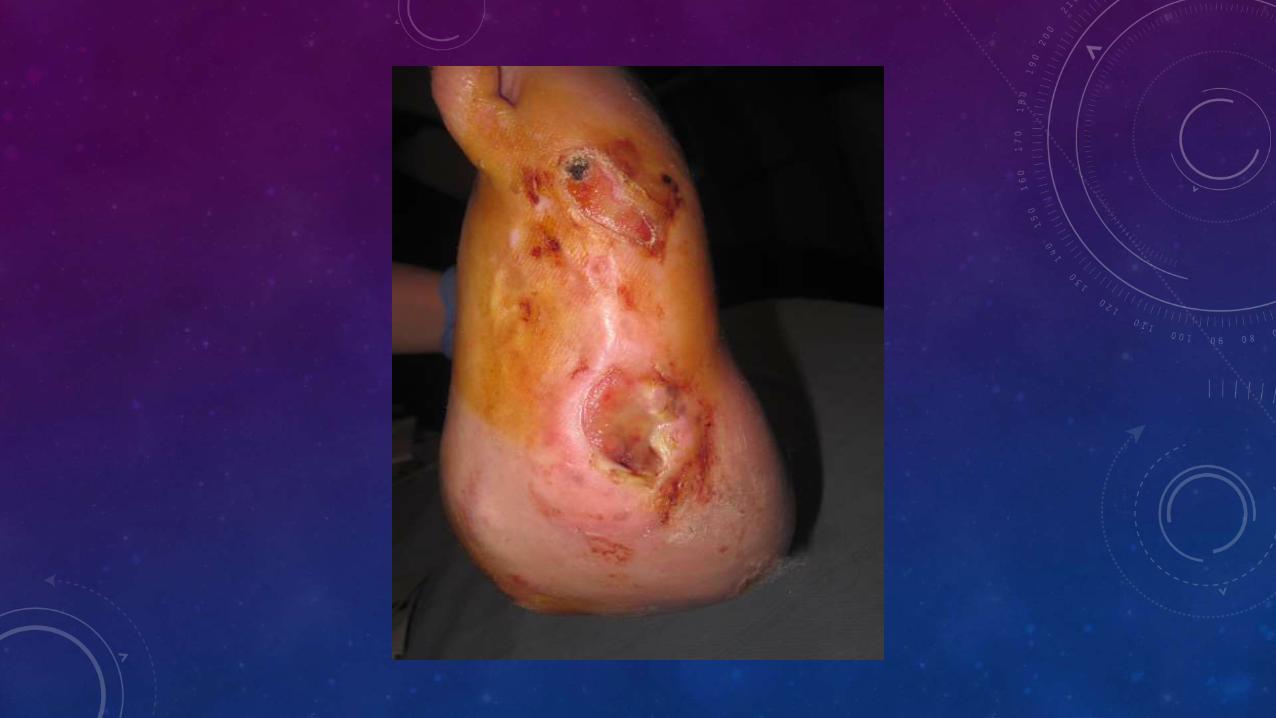





• Orthopaedic hind-foot and mid-foot corrective osteotomy and fusion. Achilles tendon release
• Ischaemic leg post op
• Graft blocked
• Emergency angiogram and anterior tibial to dorsalis pedis bypass

• Challenge
• Poor quality tissue
• Poorly perfused
• Involve deep structures
• Probing to bone and metal work
• Oedema









THE ULTIMATE CHALLENGE

INTRODUCTION
• There is a high rate of major amputation up to 30% of dialysis patients.1
• The annual rate of major and minor amputation is up to 13.8%. 2
• Major amputation accounts for more than 58% of the total amputations. 2
1 Morbach et al, 2001
2 Eggers et al, 1999
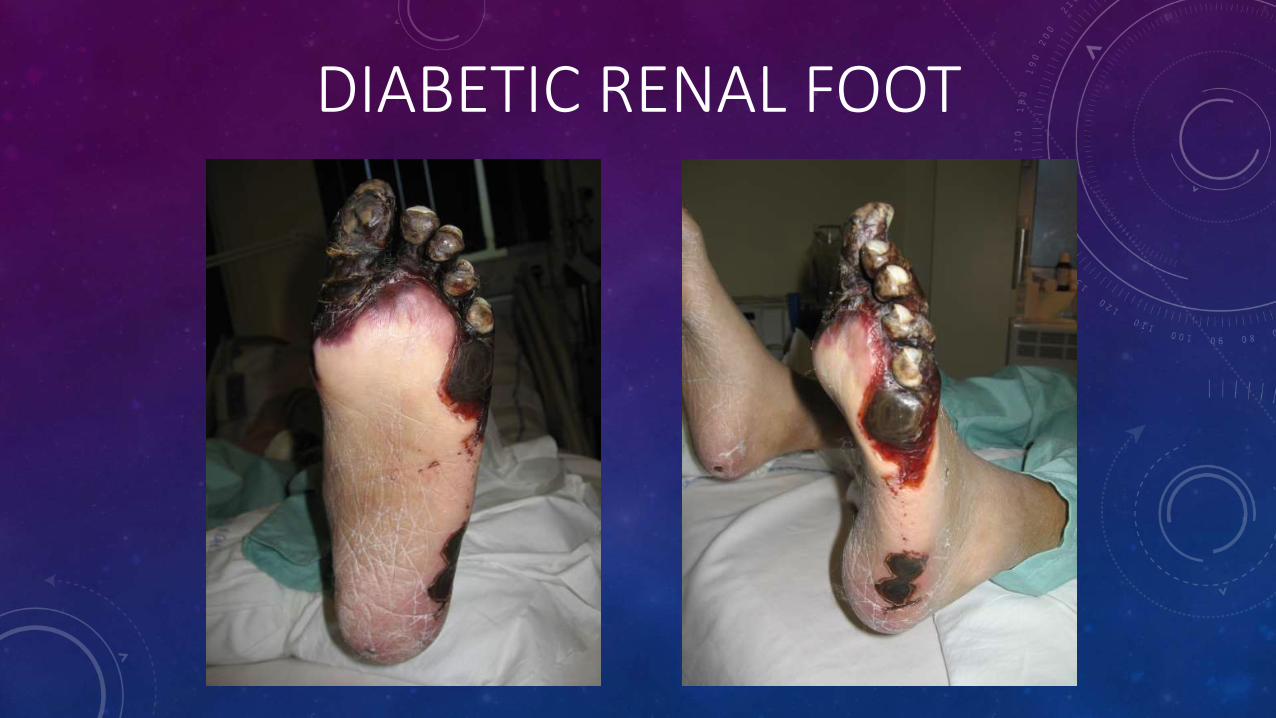
DIABETIC RENAL FOOT

CASE STUDY• Female
• Age 61 years
• Type 1 diabetic
• Chronic Renal Failure
• Peritoneal dialysis 4½ years duration, retinopathy, peripheral neuropathy & peripheral vascular disease
• Presented with infected left foot wound following
amputation of lesser toes 5 weeks previous

FOOT AT PRESENTATION
INTERVENTION
• IV antibiotics – Vancomycin
(MRSA positive swab)
• 2 downstream angioplasties of Popliteal & ATA stenosis
• Surgical debridement of devitalised tissue & bone
• VAC therapy commenced 24 hrs post-op

24 HRS POST DEBRIDEMENT

1 WEEK VAC THERAPY

2 WEEKS VAC THERAPY

4 WEEKS VAC THERAPY
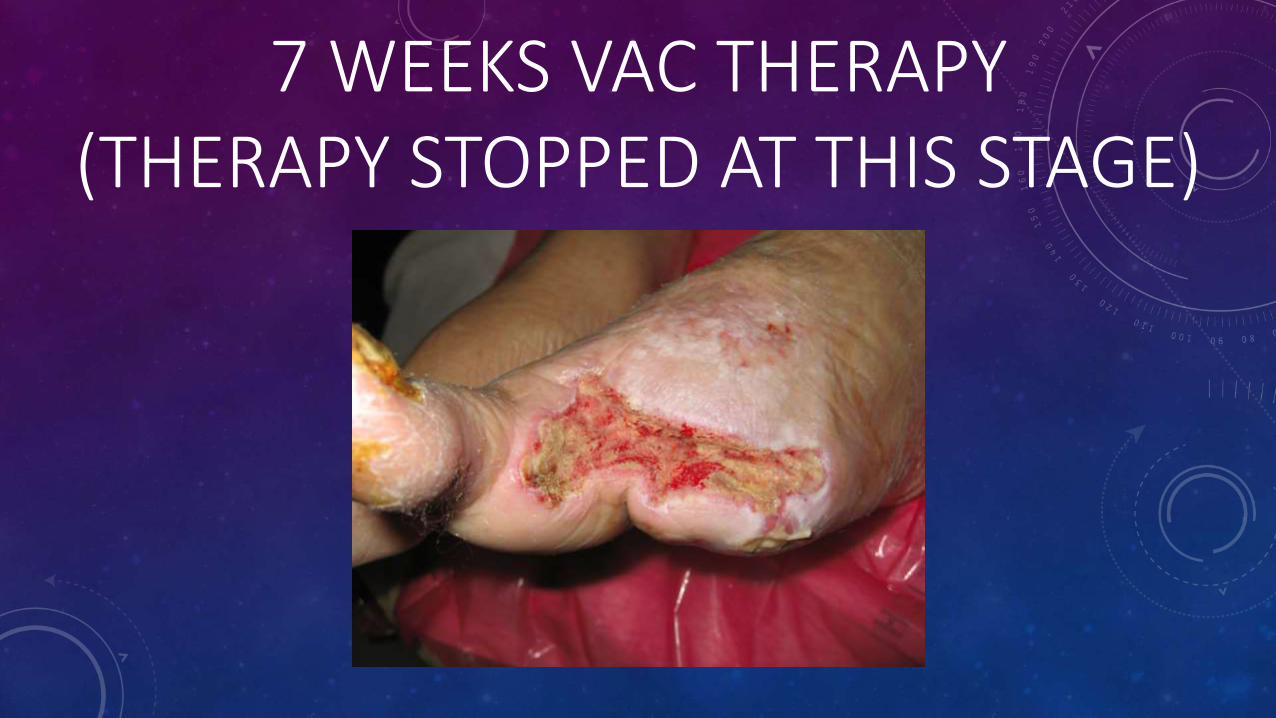
7 WEEKS VAC THERAPY(THERAPY STOPPED AT THIS STAGE)

7 WEEKS AFTER VAC STOPPED

16 WEEKS HEALED
SUMMARY
• Rapid treatment of sepsis
• Rapid revascularisation
• Angioplasty
• Intense follow up
• Aware of their co-morbidities

DIABETIC FOOT TEAM• Podiatrist
• Nurse
• Orthotist
• Physiotherapist
• Surgeon
• Radiologist
• Diabetologist



DIABETIC FOOT CLINIC
Post operative reviews
and follow ups
Emergency referrals
Orthopaedic diabetic clinics
Co-ordinate primary and secondary care
Wound care/orthotics/plasters
Vascular diabetic
clinics
Debridement/ minor surgery
Outpatient antibiotic service
Education / Research
Charcot foot clinics

Time Mon Tue Wed Thu Fri
08:00
08:30Ward Round for
AdmissionsWard Round for
AdmissionsWard Round for
AdmissionsWard Round for
AdmissionsWard Round for
Admissions
09:00 SOS Clinic
Joint Diabetic Foot/ Orthopaedic/Plastic Clinic & Ward Round
SOS Clinic
Joint Diabetic Foot/ Vascular Clinic & Ward
Round
SOS Clinic
Charcot Clinic
SOS Clinic
Ulcer Clinic
SOS Clinic
Joint Diabetic Foot/ Vascular Clinic
09:30
10:00
10:30
11:00
11:30
12:00
12:30Vascular Radiology MDT
13:00
Ulcer Clinic
(WARD ROUND)
Ulcer Clinic
(MDT on Ward)
Ulcer Clinic
(WARD ROUND)Ulcer Clinic
13:30
Charcot Clinic
14:00
14:30
15:00
15:30
16:00
16:30
17:00
17:30

Major AmputationsP
erce
nta
ge o
f to
tal p
atie
nts
Year
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
89/9
0
90/9
1
91/9
2
92/9
3
93/9
4
94/9
5
95/9
6
96/9
7
97/9
8
98/9
9
99/0
0
00/0
1
01/0
2
02/0
3
03/0
4
04/0
5
05/0
6
06/0
7
07/0
8
08/0
9
09/1
0
10/1
1
11/1
2
GOOD NEWS
• UP UNTIL RECENTLY, THE DIABETIC FOOT HAS DEFEATED EVERY HEALTH CARE
SYSTEM IN THE WORLD
• ADVANCES IN OUR UNDERSTANDING HAVE LEAD TO IMPROVEMENTS IN CARE
• ULCERS ARE NOW HEALED AND AMPUTATIONS PREVENTED
THE END

HANDS


PRESSURE RELIEVING ANKLE FOOT ORTHOSES (PRAFO)

NEUROPATHY
• Loss of nociceptive C fibres
• Loss of axon reflex
• Peptide mediators released from cutaneous C fibres are potent pro-inflammatory agents
• Failure of vasodilatation

PREVALON BOOT

NeuroischaemicCharcot Criticalischaemic
Acuteischaemic
RenalischaemicStage
2
3
4
5
Neuropathic

NeuroischaemicCharcot Criticalischaemic
Acuteischaemic
RenalischaemicStage
2
3
4
5
Neuropathic

THREE GREAT PATHOLOGIES
Primary
• Neuropathy
• Ischaemia
Secondary
• Infection




0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Pe
rce
nta
ge
REDUCTION IN MAJOR AMPUTATIONS

Diabetes Care 2007 30: 2064-2069

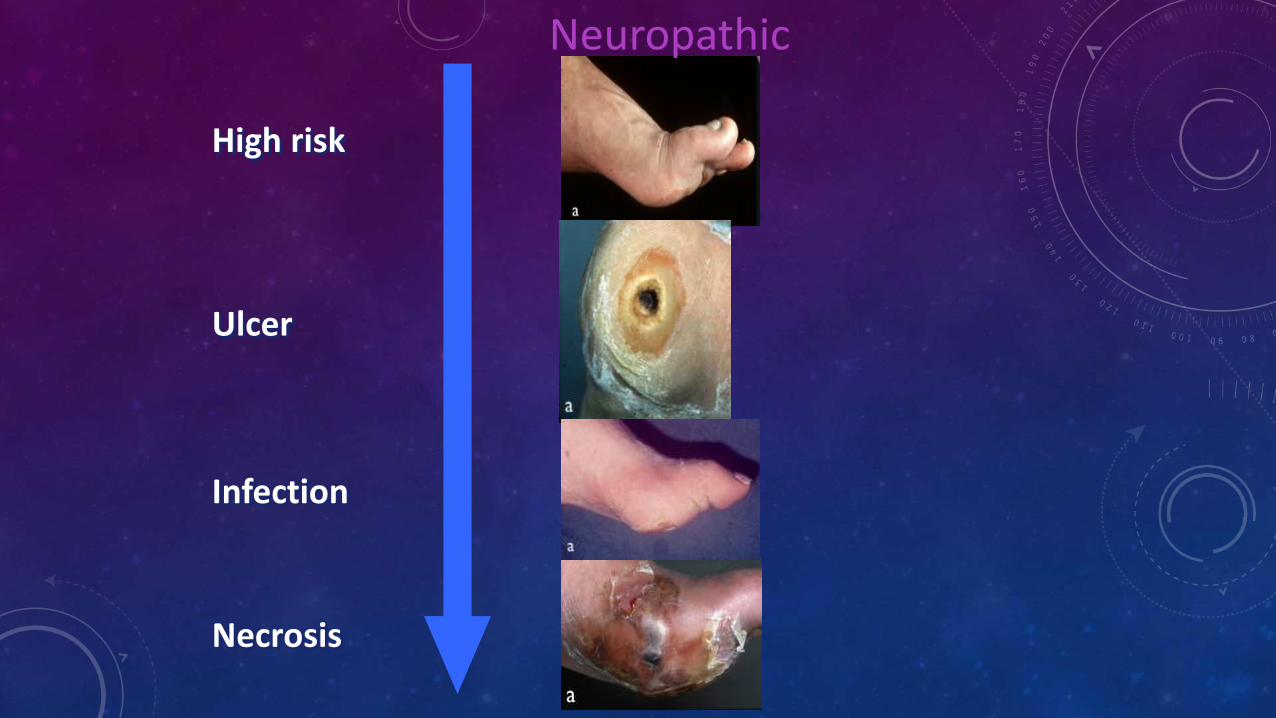
High risk
Ulcer
Infection
Necrosis
Neuropathic

Mechanical forces
Infection
Charcot Foot

LEUCOCYTOSIS
• Leucocytosis is a poor indicator of acute osteomyelitis of the foot in diabetic mellitus”
• 54% of patients with acute osteomyelitis had normal white blood cell count
Armstrong DG, 1996