advances in the prenatal diagnosis of hematologic diseases · pdf fileprenatal diagnosis of...
TRANSCRIPT

Blood, Vol 64, No 2 (August), 1984: pp 329-340 329
REVIEW
Advances in the Prenatal Diagnosis of Hematologic Diseases
By Blanche P. Alter for the WHO International Registry for Prenatal Monitoring of Hereditary Anemias
T HE MODERN ERA ofprenatal testing for hema-
tologic diseases began in 1974. Prior to that time,
the only test available consisted of determination of
fetal sex following amniocentesis in cases at risk for
sex-linked disorders, such as the hemophilias. Methods
for obtaining fetal blood in utero in ongoing pregnan-
cies were initiated in 1974, and these developments led
to the possibility of prenatal diagnosis of any blood
disorder that was expressed in utero and for which the
assay could be miniaturized. The first group of diseases
for which such testing was utilized was the hemoglo-binopathies. Recent advances in molecular biology
have now resulted in a return to the use of amniocente-
sis for many of these prenatal tests (see Orkin’ for a
recent review), although sampling of fetal blood
remains the method of choice for detection of hemato-
logic diseases in utero for which deoxyribonucleic acid
(DNA) probes are not yet available.
The World Health Organization (WHO) supports
an International Registry for Prenatal Monitoring of
Hereditary Anemias, which attempts to document all
cases examined in utero by fetal blood or DNA studies
for hematologic diseases. This Registry is maintained
on PROPHET, a computer resource sponsored by the
Division of Research Resources of the National Insti-
tutes of Health. Analyses of the Registry data are
complete for the period of June 1974 through Decem-
ber 1982 and will be referred to here.
Prenatal diagnosis of hemoglobinopathies was last
reviewed two years ago,2 and relevant references maybe found there, as well as in a detailed chapter.3 Theprevious review cited data from the Registry that
ended in March 1981 and included 1,856 cases that
had been studied by fetal blood analysis because of therisk of hemoglobinopathies. The current Registry
includes 4,1 33 cases studied for hemoglobinopathies,
or more than 2,000 additional cases, as well as more
than 300 cases investigated for other hematologic
disorders. A total of 4,47 1 prenatal studies were
reported through December 1982. The centers partici-
pating in the Registry are listed in Table 1 , and the
physicians of record at each center are listed in the
Acknowledgment section. All but the Scandinavian
centers began with examination of fetal blood in casesat risk for thalassemia. Several have now begun to
examine the DNA in such cases, which is obtainedcurrently by amniocentesis and, in the near future, will
be obtained from chorionic villi. Some centers have
also extended their studies of fetal blood to include
disorders other than hemoglobinopathies. This review
will summarize the major techniques and results
reported to the Registry.
FETAL BLOOD FOR HEMOGLOBINOPATHIES
Fetal Blood Sampling
Fetal blood can be obtained during the midtrimester
by several methods. Most of the procedures are done
with local anesthetic. The first technique involves
aspiration of blood from the placenta under ultrasound
guidance.4 A long 20-gauge spinal needle is introduced
transabdominally into the placenta, and several small
samples of blood are aspirated. The red cell size
distribution of the samples is analyzed immediately
with a Coulter Channelyzer (Coulter Electronics,
Hialeah, Fla) to determine the proportion of fetal cells,
because fetal erythrocytes have a mean corpuscular
volume (MCV) of 140 fi, while adult cells are less than
100 fl.5 As soon as an adequate sample is obtained, the
placentocentesis needle is removed. This method often
produces samples of mixed fetal-maternal blood (see
Fig 1), which can be enriched in fetal cells (see below),
and usually suffice for globin chain synthesis studies.
Samples with maternal and/or amniotic fluid contami-
nation are not optimal for determination of fetal blood
counts, coagulation factors, or many other examina-
tions.
A more successful technique for obtaining pure fetal
blood is fetoscopy.6 A fiberoptic endoscope (Dyonics
Needlescope, Dyonics mc, Andover, Mass) is inserted
transabdominally into the amniotic cavity, and a sam-
pie of fetal blood is taken under direct visualization by
passing a long 27-gauge needle through the sidearm of
the fetoscope cannula. Specimens were initially
obtained from fetal vessels on the chorionic plate,
which were punctured and bled into the amniotic fluid,
From the Polly Annenberg Levee Hematology Center, Depart-
ments ofMedicine and Pediatrics, Mount Sinai School of Medicine,
New York.
Supported in part by the World Health Organization, NIH grant
HL26132. and an Irma T. Hirsch! Career Scientist Award.
Submitted Nov 14, 1983; accepted March 16, 1984.
Address reprint requests to Dr Blanche Alter, Division of Hema-
tology, Mount Sinai School of Medicine, One Gustave L. Levy
Place, New York, NY 10029.
© 1 984 by Grune & Stratton, Inc.
0006-4971/84/6402-0002$03.00/0
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

.
A
0
0
.
330 BLANCHE P. ALTER
Table 1 . Center S for Prenatal Diagnosis of Hemat ologic Diseases
Fetal Blood. Fetal DNA. Fetal Blood.Hemoglobin- Hemoglobin- Other
Country City opathies opathies Diseases
Australia
Canada
Melbourne
Queen Victoria
Royal Women’s
Sydney
Montreal
Toronto-Hamilton
+
+
+
+
+
+
+
Cyprus Nicosia +
Denmark Copenhagen +
England
France
London
University College
King’s College
Oxford
Paris
+
+
+
+
+
+
+
Germany Munich + +
Greece Athens +
Israel Jerusalem + +
Italy Ferrara
Milan
Rome
Sardinia
+
+
+
+
+ +
Sweden Malmo +
United States Baltimore
Boston
New Haven
NewYork
San Francisco
+
+
+
+
+
+
+
+
+
from which the blood was aspirated. Recent modifica-
tions have led to blood being drawn directly from the
umbilical vein at the placental insertion of the cord.7’8
These samples contain pure fetal blood, with neither
maternal blood nor amniotic fluid contamination, and
are suitable for all hematologic tests involving cells,
serum, or plasma. Figure 1 compares the proportion of
fetal cells obtained by several centers by fetoscopy andby placental aspiration. More centers use the former
method, and the weighted mean percentage of fetal
cells is 96%, compared with 56% by aspiration.
A recent modification has used ultrasound without
‘4
FFTAL
lee.
80.
6e.
4e.
20.
0.
0.
FETOSCOPY ASPIRATION
2.
Fig 1 . Percentage of fetal red blood cells in samples obtained
by fetoscopy (�) or aspiration ( � ). Each point represents themean value reported by each center. Closed symbols indicate less
than 40 cases and open symbols more than 40 cases.
fetoscopy to obtain pure fetal blood from the umbilical
vein and has succeeded in more than 50 cases.9 A
20-gauge long needle was used, which is larger than
the 27-gauge needle used through the fetoscope, and
the risks to the fetus of this modification are not yet
known. Another group has used transvaginal place-
ment of the fetoscope in cases with extensive anterior
placentas.’#{176} Other infrequently used approaches have
included ultrasound-guided placement of a needle into
the hepatic portion of the umbilical vein” and ultra-
sound-guided fetal cardiac puncture.’2 The safety and
necessity of some of these techniques are open to
question.
Method of Analysis
The proportion of fetal erythrocytes, initially esti-mated with the Coulter Channelyzer, is subsequently
confirmed with the acid elution slide test.’3 The fetal
blood (and a maternal sample as a control) is incu-
bated with 3H-leucine to radiolabel newly synthesized
globin chains, which are then analyzed by carboxyme-
thyl cellulose (CMC) chromatography. Details of
these techniques are provided elsewhere.’4”5 Mutant
f3-globins, such as 5, C, E, 0-Arab, and Lepore, are
detected because they separate chromatographically
from the normal f.�-chain.
The diagnosis of thalassemia is made when the
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

N0
0F�
CASFS
tame
000
t 00
to. -
0
00
0�
A’
0�
20 40 60 80 tOO 20
TOTAL MONTHS
PRENATAL DIAGNOSIS OF HEMATOLOGIC DISEASES 331
normal a- or j3-chain is absent or substantially reduced
in amount. Cividalli et aV6 suggested calculation of the
ratio of fl/7-globin synthesis. This value increases
slowly during the first and midtrimesters and is 0. 1 1 ±
0.05 (mean ± 2 SD) at 16 to 23 weeks in normal
fetuses)7 We found that the fl/”y-ratio in fetuses subse-
quently proven to have fl-thalassemia trait was 0.06 ±
0.04. The important aspect is the distinction of homo-zygotes from heterozygotes. In our experience, /3-
thalassemia major was diagnosed if the f3/’y-ratio was
below 0.025. Throughout the world, however, the
specific cutoff point ranges from 0.010 (where only
/3#{176}-thalassemia occurs) to 0.035 (where f3�-thalassemia
predominates). Each center has determined its own
value, depending on the “plusness” of the /3-thalasse-
mia in that region and the technical aspects of the
separation of /3- and �y-globin in its laboratory.
One problem that decreased with increasing obstet-nc experience is that of impure samples of placental
blood. Details of the many approaches that have been
used to enrich such samples for fetal red cells are
provided elsewhere)5 In the current WHO Registry,
many centers indicated that they now routinely obtain
pure fetal samples. Over the preceding years, I ,008
samples required enrichment, and 77% were done with
the �rskov procedure. This is a method for selective
hemolysis of adult red cells, which contain carbonic
anhydrase, and lyse in the presence of NH4C1 and
NH4HCO3. Fetal cells, with low levels of carbonic
anhydrase, do not lyse.’t In the past year, this was the
only method used when samples were impure.
Fetal Blood Studies for Hemoglobinopathies
Three thousand nine hundred fifty-nine cases werereported to the WHO Registry from June 1974
through December 1982, in which fetal blood was
examined because the fetus was at risk for a hemoglo-
binopathy. The most recent summary reported in the
literature from each center is included in references 19
to 3 1 . The number of cases tested increased signifi-cantly each year (Fig 2). Logarithmic transformation
of these data results in almost a straight line, with a
case number doubling time of approximately 15
months. By the end of 1982, 100 cases were being
studied each month worldwide. The disorders for
which the fetuses were examined are listed in Table 2.
Ninety-two percent were at risk for thalassemias, and
the rest were for sickle disorders. Of the thalassemias,
98% were /3 (j3#{176}and fl� are combined here, because the
specific genetic defect was often unknown), and 60% of
the sickle group were at risk for homozygous 55.
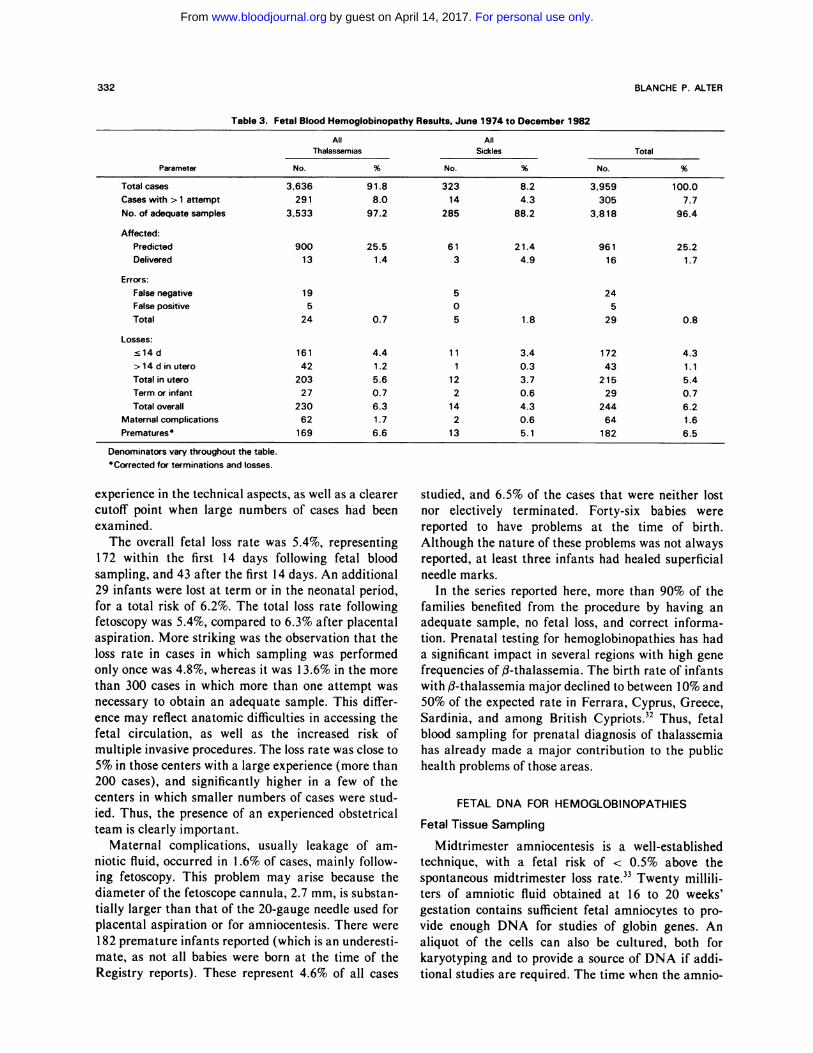
The results of the fetal blood studies for hemoglo-binopathies are shown in Table 3. Three hundred five
of the 3,959 cases required more than one attempt to
Fig 2. Log plot of cumulative number of cases reported to
each Registry. The first Registry ended in December 1 978. thesecond in March 1 980, the third in March 1 981 , the fourth inDecember 1981, and the fifth in December 1982. (-0-) Hemo-globinopathies by fetal blood. (---a---) other diseases by fetal
blood. ( . . . � . . . ) hemoglobinopathies by DNA.
obtain an adequate sample, but only 54 of the almost
2,000 cases studied in the past two years were in this
category, reflecting improved obstetric experience.
Three thousand eight hundred eighteen, or 96% of
cases, did result in an adequate sample eventually. Of
the adequate samples, 25% led to diagnosis of the
disease for which the fetus was at risk, which is the
proportion expected for autosomal recessive disorders.
Of the 961 fetuses found to be affected, only 1 6 (1.7%)
did not request an elective termination.
Errors were reported in 29 cases (0.8% of adequate
samples), of which 24 were false negatives. In these,
the fetal /3/’y-synthetic ratio exceeded the cutoff value
for the respective centers. Technical problems with the
/3- and 7-chain separations on the columns could be
implicated in only a few cases. Most of the errors
occurred in fetuses with f3�-thalassemia major, in
whom the fl/-y-ratio fell within the heterozygote range.
However, the error rates were slightly higher in centers
that had studied only small numbers of cases, perhaps
indicating some benefit from extensive laboratory
Table 2. Fetal Blood Testing for Hemoglobinopathies: Fetal Risks,
June 1 974 to December 1982
Disorder No. Percent
Thalassemia:
�3 3,548 97.6
#{244}�3 49 1.3
a 12 0.3
a+fl 6 0.2
E/fi-Thal 6 0.2
Lepore 15 0.4
Total 3,636 91.8 (of total)
Sickle:
55 193 59.8
S/fl-ThaI 126 39.0
SC 3 0.9
S/O-Arab 1 0.3
Total 323 8.2 (of total)
Total 3,959 100.0
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom
332 BLANCHE P. ALTER
TabI e 3. Fetal Blood Hemogl obinopathy Results, Ju ne 1974 t o December 1982
All All
Parameter
Thalassemias
No.
Sickles
%
Total
No. %No. %
Totalcases 3,636 91.8 323 8.2 3,959 100.0
Cases with > 1 attempt 291 8.0 14 4.3 305 7.7
No.ofadequatesamples 3,533 97.2 285 88.2 3,818 96.4
Affected:
Predicted 900 25.5 61 21.4 961 25.2
Delivered 13 1.4 3 4.9 16 1.7
Errors:
False negative 1 9 5 24
False positive 5 0 5
Total 24 0.7 5 1.8 29 0.8
Losses:
sl4d 161 4.4 11 3.4 172 4.3
>l4dinutero 42 1.2 1 0.3 43 1.1
Totalinutero 203 5.6 12 3.7 215 5.4
Termorinfant 27 0.7 2 0.6 29 0.7
Total overall 230 6.3 14 4.3 244 6.2
Maternal complications 62 1 .7 2 0.6 64 1.6
Prematures 169 6.6 13 5.1 182 6.5
Denominators vary throughout the table.
Corrected for terminations and losses.
experience in the technical aspects, as well as a clearercutoff point when large numbers of cases had been
examined.The overall fetal loss rate was 5.4%, representing
172 within the first 14 days following fetal blood
sampling, and 43 after the first 14 days. An additional
29 infants were lost at term or in the neonatal period,
for a total risk of 6.2%. The total loss rate following
fetoscopy was 5.4%, compared to 6.3% after placental
aspiration. More striking was the observation that the
loss rate in cases in which sampling was performed
only once was 4.8%, whereas it was 13.6% in the more
than 300 cases in which more than one attempt was
necessary to obtain an adequate sample. This differ-
ence may reflect anatomic difficulties in accessing the
fetal circulation, as well as the increased risk of
multiple invasive procedures. The loss rate was close to
5% in those centers with a large experience (more than
200 cases), and significantly higher in a few of the
centers in which smaller numbers of cases were stud-
ied. Thus, the presence of an experienced obstetrical
team is clearly important.
Maternal complications, usually leakage of am-
niotic fluid, occurred in I .6% of cases, mainly follow-
ing fetoscopy. This problem may arise because the
diameter of the fetoscope cannula, 2.7 mm, is substan-
tially larger than that of the 20-gauge needle used for
placental aspiration or for amniocentesis. There were
182 premature infants reported (which is an underesti-
mate, as not all babies were born at the time of the
Registry reports). These represent 4.6% of all cases
studied, and 6.5% of the cases that were neither lost
nor electively terminated. Forty-six babies were
reported to have problems at the time of birth.
Although the nature of these problems was not alwaysreported, at least three infants had healed superficial
needle marks.
In the series reported here, more than 90% of the
families benefited from the procedure by having an
adequate sample, no fetal loss, and correct informa-
tion. Prenatal testing for hemoglobinopathies has had
a significant impact in several regions with high gene
frequencies of /3-thalassemia. The birth rate of infants
with /3-thalassemia major declined to between 10% and
50% of the expected rate in Ferrara, Cyprus, Greece,
Sardinia, and among British Cypriots.32 Thus, fetal
blood sampling for prenatal diagnosis of thalassemia
has already made a major contribution to the public
health problems of those areas.
FETAL DNA FOR HEMOGLOBINOPATHIES
Fetal Tissue Sampling
Midtrimester amniocentesis is a well-established
technique, with a fetal risk of < 0.5% above the
spontaneous midtrimester loss rate.33 Twenty millili-
ters of amniotic fluid obtained at 16 to 20 weeks’
gestation contains sufficient fetal amniocytes to pro-
vide enough DNA for studies of globin genes. An
aliquot of the cells can also be cultured, both for
karyotyping and to provide a source of DNA if addi-
tional studies are required. The time when the amnio-
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom
PRENATAL DIAGNOSIS OF HEMATOLOGIC DISEASES 333
centesis is performed and the approximate two weeks
required for the analysis result in midtrimester termi-
nations of affected fetuses, as is the outcome when
fetal blood sampling is performed.
A new method is now being developed for obtaining
fetal tissue, which involves aspiration or biopsy of
chorionic villi at eight to 1 2 weeks’ gestation. This is an
outpatient procedure and is guided by real-time ultra-
sound. Sufficient DNA is obtained from the villi
(usually 10 to 20 �.ig) for examination of the globin
genes. This method has been reported in nine cases at
risk for hemoglobinopathies.3�36 In pooled early results
from centers just beginning to develop this technique,
the loss rate in 1 13 cases in which samples wereobtained for a variety of reasons was cited at 1 �
Although higher than that which occurs with amnio-
centesis or with fetal blood sampling, this rate may
decline with obstetric experience. A first-trimester test
has obvious psychologic and medical advantages.
Method of Analysis
The recombinant DNA technologies used to detect
hemoglobinopathies in utero were reviewed recently in
this journal, by Orkin.’ Globin gene deletion is the
cause of many cases of a-thalassemia, �f3-thalassemia,
rare /3#{176}-thalassemia (deletion of the 3’ end), and
Lepore. Linked restriction fragment length polymor-
phisms can be used to detect /35 and �C genes (HpaI),
/3#{176}-thalassemia in Sardinia (BamHI), and many other
fl-thalassemias.38 Extensive and time-consuming fam-
ily studies are often required to establish these link-
ages, however. A few DNA point mutations that cause
hemoglobinopathies are themselves restriction enzyme
cleavage sites, and thus can be diagnosed directly with
the appropriate enzymes. Examples of these are thediagnosis of flS with Dde!, MstII, or CvnI,36 all of
which cleave at the normal /36 codon, � with
EcoRI, and a few uncommon /3-thalassemia genes with
other enzymes. The most useful tool of molecular
biology will be the in vitro synthesized oligonucleotides
(19-mers), which are specific for each thalassemic
mutation. These probes identify either the mutant or
the normal /3-gene and have been used for prenatal
testing of cases at risk for the Sardinian /339 nonsense
mutation.39 Such methods can identify the most com-
mon Mediterranean fl�-thalassemia due to a mutation
in the first intervening sequence.”#{176} In families in which
the specific genetic defect is known, the oligonucleo-
tide method will be the most useful and accurate.
Fetal DNA Studies for Hemoglobinopathies
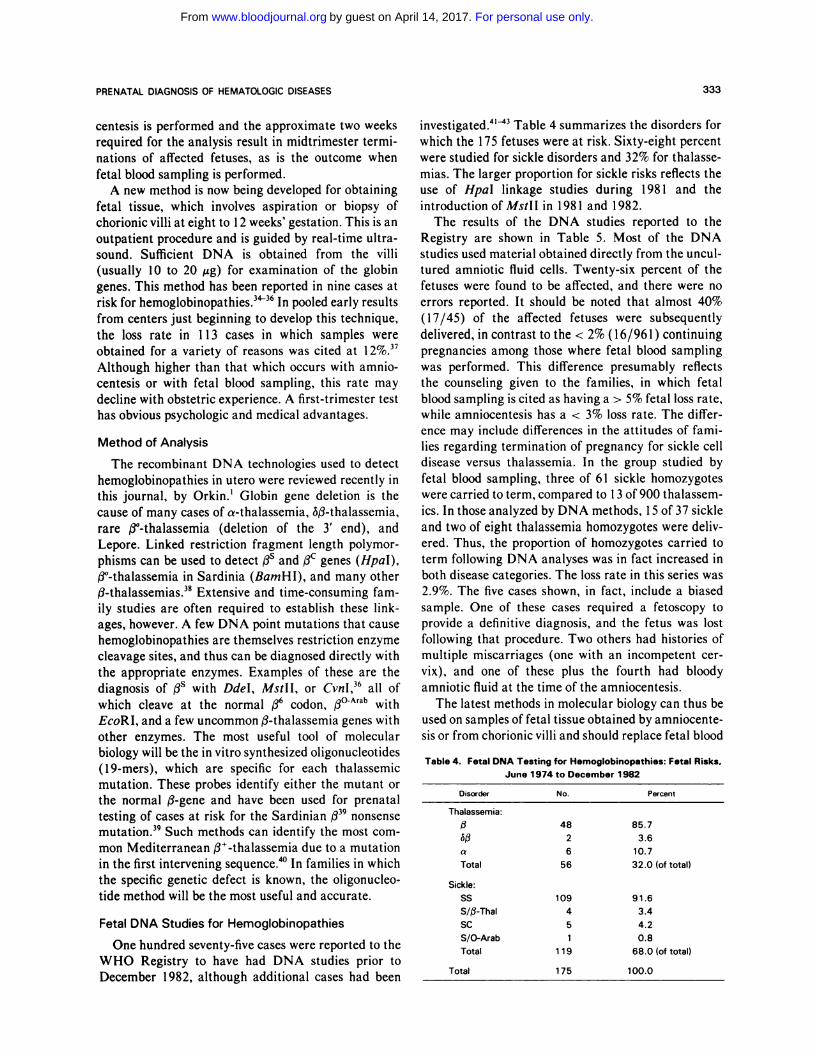
One hundred seventy-five cases were reported to the
WHO Registry to have had DNA studies prior to
December 1982, although additional cases had been
investigated.41�3 Table 4 summarizes the disorders for
which the 1 75 fetuses were at risk. Sixty-eight percent
were studied for sickle disorders and 32% for thalasse-
mias. The larger proportion for sickle risks reflects the
use of HpaI linkage studies during 1981 and the
introduction ofMstll in 1981 and 1982.
The results of the DNA studies reported to theRegistry are shown in Table 5. Most of the DNA
studies used material obtained directly from the uncul-
tured amniotic fluid cells. Twenty-six percent of the
fetuses were found to be affected, and there were no
errors reported. It should be noted that almost 40%
(17/45) of the affected fetuses were subsequently
delivered, in contrast to the < 2% (16/961) continuing
pregnancies among those where fetal blood sampling
was performed. This difference presumably reflects
the counseling given to the families, in which fetal
blood sampling is cited as having a > 5% fetal loss rate,
while amniocentesis has a < 3% loss rate. The differ-
ence may include differences in the attitudes of fami-
lies regarding termination of pregnancy for sickle cell
disease versus thalassemia. In the group studied by
fetal blood sampling, three of 61 sickle homozygotes
were carried to term, compared to 1 3 of 900 thalassem-
ics. In those analyzed by DNA methods, 1 5 of 37 sickle
and two of eight thalassemia homozygotes were dcliv-
ered. Thus, the proportion of homozygotes carried to
term following DNA analyses was in fact increased in
both disease categories. The loss rate in this series was
2.9%. The five cases shown, in fact, include a biased
sample. One of these cases required a fetoscopy to
provide a definitive diagnosis, and the fetus was lost
following that procedure. Two others had histories of
multiple miscarriages (one with an incompetent cer-
vix), and one of these plus the fourth had bloody
amniotic fluid at the time of the amniocentesis.
The latest methods in molecular biology can thus be
used on samples of fetal tissue obtained by amniocente-
sis or from chorionic villi and should replace fetal blood
Table 4. Fetal DNA Testing for Hemoglobinopathies: Fetal Risks,
June 1 974 to December 1982
Disorder No. Percent
Thalassemia:
fi 48 85.7
#{244}fl 2 3.6
a 6 10.7
Total 56 32.0 (of total)
Sickle:
SS 109 91.6
S/fl-ThaI 4 3.4
SC 5 4.2
5/0-Arab 1 0.8
Total 119 68.0 (of total)
Total 175 100.0
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

Table 5. Fetal DNA Hemoglobinopathy Results,
June 1 974 to December 1982
Table 6. Fetal Blood Testing for Other Diseases: Fetal Risks.
334 BLANCHE P. ALTER
All
ThalassemiasAll
Sickles Total
Parameter No. % No. % No. %
Totalcases 56 32.0 119 68.0 175 100.0
Affected:
Predicted
Delivered
8 1 4.3
2 25.0
37 3 1 .0
15 40.5
45
17
25.7
37.8
Errors 0 0 0 0 0 0
Losses:
sl4d
>14d
Totalfetal
2
1
3 5.4
1
1
2 1.7
3
2
5 2.9
Prematures 0 0 0 0 0 0
sampling for prenatal detection of many of the hemo-
globinopathies. These methods can now be routinely
and reliably applied to cases at risk for sickle cell
anemia, Sardinian /339 nonsense mutation thalassemia,
gene deletion a- and #{244}$-thalassemias, and certain types
of /3#{176}-and /3�-thalassemia. The specific mutations in
the /3-thalassemias, or specific linked polymorphisms,
must be known for the successful application of the
recombinant technology. Thus, newly diagnosed thal-
assemic families may still require fetal blood globin
synthesis analyses until rapid methods for identifica-
tion of thalassemic defects are developed, such as
panels of oligonucleotides.
FETAL BLOOD FOR OTHER DISEASES
A large variety of hematologic and nonhematologic
disorders can now be detected in fetal blood. Diseases
other than hemoglobinopathies were first studied in
1979, and 338 cases were reported to the WHO
Registry through December 1 982. Of these cases, 243,
or 72%, were at risk for coagulopathies (Table 6),
mostly the hemophilias. The next largest group was at
risk for muscular dystrophies, followed by studies of
white cell disorders. For the sex-linked disorders, an
amniocentesis was performed first for fetal sex deter-
mination. Fetal blood sampling was then only done
from male fetuses.
For most of the disorders listed in Table 6, pure fetalblood was optimal, if not absolutely required. Assays of
clotting factor activity must be done with pure fetal
plasma, because amniotic fluid contains thromboplas-
tic activity. In fact, the need for pure fetal blood for the
coagulation diagnoses provided some of the impetus
for the development of techniques for sampling from
the umbilical vein. VIIICAS, VIIIRA5 and IXAg can be
measured by immunologic techniques in the presence
of amniotic fluid, provided the relative dilution of the
fetal plasma is known.
June 1 974 to December 1982
Disorder No. Percent
Coagulation:
Hemophilia A 208 85.6
Hemophilia B 19 7.8
von Willebrand 4 1.6
Amegakaryocytic 1 0.4
TAR 1 0.4
Wiskott-Aldrich 1 0.4
Alpha 1-antitrypsin 9 3.7
Total 243 7 1 .9 (of total)
Red cells:
HEMPAS 1 50.0
Rh 1 50.0
Total 2 0.6 (of total)
White cells:
CGD 3 6.8
lmmunodeficiency 3 6.8
Neutropenia 1 2.2
Rubella 2 4.5
Chromosomes 35 79.5
Total 44 13.0 (of total)
Other:
DMD
BMD
Total
Total
48 98.0
1 2.0
49 14.5 (of total)
338 100.0
TAR. thrombocytopenia with absent radii; HEMPAS, hereditary
erythroblastic multinuclearity with positive acidified serum test; CGD,
chronic granulomatous disease; DMD, Duchenne muscular dystrophy;
BMD, Becker muscular dystrophy.
Most of the hemophilia diagnoses were obtained in
three centers.’2’44�6 Two hundred eight cases were at
risk for hemophilia A (factor VIII deficiency), 19 for
hemophilia B (factor IX deficiency), and four for
homozygous von Willebrand’s disease (inherited as a
dominant). There was one error (Table 7), in which a
case with hemophilia was not detected in utero. There
were seven losses (3%), which indicates that the risk of
hemophilia does not increase the risk of fetal loss in
utero.
Two fetuses were studied for the possibility of
autosomal recessive thrombocytopenias by obtaining
platelet counts in fetal blood. One of these fetuses, at
risk for thrombocytopenia with absent radii, could
have been examined by ultrasound alone. This diag-
nosis has been reported in the past by means of fetal
x-ray studies.47’48 Another platelet disorder that has
been sought in utero recently is the Wiskott-Aldrich
syndrome.49 This diagnosis was excluded by the find-
ings of a normal fetal blood platelet count and normal
mean platelet volume in a male fetus whose affected
brother had thrombocytopenia and small platelets.
Red cell disorders other than hemoglobinopathies
can be detected in utero. Red cell grouping and typing
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

PRENATAL DIAGNOSIS OF HEMATOLOGIC DISEASES 335
Table 7. Fetal Blood Other Disease a Results, June 1 9 74 to D ecember 1982
Muscular
Coagulation WBC + RBC Dystrophies Total
Parameter No. % No. % No. % No. %
Totalcases 243 71.9 46 13.6 49 14.5 338 100.0
Caseswith>1 attempt 5 2.1 0 0.0 8 16.3 13 3.8
Adequatesamples 236 97.1 46 100.0 45 91.8 327 96.7
Affected:
Predicted 80 33.9 13 28.3 5 11.1 98 30.0
Delivered 3 3.8 0 0.0 0 0.0 3 3.1
En’ors:negative 1 0.4 1 2.2 3 6.7 5 1.5
Losses:
�14d 4 1.6 2 4.3 3 6.1 9 2.7
>14d 3 1.2 1 2.2 2 4.1 6 1.8
Total 7 3.0 3 6.5 5 10.2 15 4.4
Prematures 10 6.3 1 3.3 2 5.1 13 5.7
WBC. white blood cells; RBC, red blood cells.5C�ected for terminations and losses.
can be performed adequately on fetal blood for diag-
nostic purposes,5#{176} for questions of paternity,5’ and for
treatment of hemolytic disease due to isoimmuniza-
tion.52 Intrauterine intravenous exchange transfusion
can be performed to treat the latter condition, using
fetoscopy and a needle placed in the umbilical vein.
Red cell enzyme deficiencies might be detected in
utero. Normal fetal red cell levels of several enzymes
were reported by Lestas et al53 in anticipation of
requests for diagnoses. In one case, the diagnosis of
galactosemia was ruled out by measurement of red cell
UDPgal.54 Fetal congenital anemias might be diag-
nosed, as fetal blood counts can be compared with
normal values for 20 weeks’ gestation (2.5 x 106
RBC/�sL, 37% hematocrit55). Defects in erythroid
stem cells could be detected, as Linch et al have shown
that normal fetuses have increased circulating cry-
throid progenitor cells (BFU-E, burst-forming units).56
Only hereditary erythroblastic multinuclearity with
positive acidified serum test (HEMPAS) and Rh
determinations were reported to the Registry.
Fetal white blood cells can be used to diagnose
several types of diseases. The first example involved
chronic granulomatous disease, usually an X-linked
disorder in which granulocytes and monocytes fail to
kill certain types of bacteria due to an inability to
generate superoxide radicals. The white cells of
affected fetuses were unable to reduce nitroblue tetra-
zolium on a slide test.57’58 Newburger and Latt noted
that samples of mixed fetal-maternal blood could be
used, because the male cells could be identified by
Y-chromatin fluorescence.59 Three such studies were
reported to the Registry. Since adequate numbers of
granulocytes are present by 20 weeks’ gestation, the
diagnosis of neutropenia could also be made, and one
such case was studied.
Another major category of white cell disorders
involves the immunodeficiency syndromes. Some
forms of severe combined immunodeficiency are asso-
ciated with adenosine deaminase (ADA) deficiency,and one affected fetus was detected by low levels of
fetal red cell ADA.�#{176}The risk of fetoscopy can usually
be avoided in these cases, because amniotic fluid cell
ADA is also reduced in affected cases.61’62 A more
general approach to the immunodeficient diagnoses
involves determination of the numbers and proportions
of fetal lymphocytes and T and B subsets, using
fluorescent antibodies and microscopic immunofluo-rescence assays or a fluorescence-activated cell sorter.
Four cases at risk for severe combined immunodefi-
ciency have been reported in the literature (three to the
Registry), and one was found to be affected.63�5
Fetal white cells obtained by fetoscopy can be
cultured, thus providing a source of chromosomal
analyses by 72 hours, much more rapidly than the two
weeks required to culture amniotic fluid cells.66 This is
particularly helpful when the amniotic culture fails or
the pregnancy is quite advanced when the test is
requested. This method was used to diagnose the
syndrome of mental retardation associated with fragile
x.67 Other chromosome defects would easily be deter-
mined from cultured fetal white cells, although in most
cases, amniotic cells should suffice (see below). Fetal
white cells were used for karyotyping in 35 cases
reported to the Registry, and eight were abnormal.
Fetal white cells were recently reported to be used to
exclude the diagnosis of Hurler’s disease by measure-
ment of leukocyte a-L-iduronidase.68 As with red cells,
many enzymes can be measured and diagnoses made
depending on the values obtained in relation to normal
fetal values.
Fetal serum or plasma is available if pure fetal blood
can be obtained. This material was used to measure
creatine phosphokinase levels in 49 fetuses at risk for
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

336 BLANCHE P. ALTER
muscular dystrophies reported to the Registry (Tables
6 and 7)69.70 but false negative results were obtained in
three cases, and the assay is not considered to be
reliable.71’72 Current attempts to define restriction
enzyme polymorphisms that are closely linked to the
genes for the muscular dystrophies will be more valu-
able than fetal blood sampling.73’74
Fetal serum was used to diagnose Tay-Sachs disease
by measurement of hexosaminidase activities,75 but
this is a diagnosis that can be made with amniotic
fluid. Fetal plasma was reported to provide the diag-
nosis of alpha,-antitrypsin deficiency,76 and the investi-
gators indicated that this was necessary because most
of the alpha,-antitrypsin in amniotic fluid is derived
from the mother. Such studies were performed in nine
cases reported to the Registry.
The WHO Registry data, which extend through
December 1982, do not include all of the conditions
discussed above, because the use of fetal blood for
many other diagnoses is a rapidly growing area. The
summarized numbers of cases are small (Table 7). If
the cases at risk for muscular dystrophies are excluded,
the error rate is < I %, and the fetal loss rate is under
4%. This low loss rate may reflect the fact that most of
the nonhemoglobinopathy prenatal testing is per-
formed in only a few of the 1 1 centers that do any such
studies, and these centers have experienced obstetri-
cians.
OTHER HEMATOLOGIC DISEASES DIAGNOSED BY
AMNIOCENTESIS
The development of molecular probes for detection
of the hemoglobinopathies is advancing rapidly. Clon-
ing of the genes that code for the important coagula-
tion proteins and for red cell enzymes is also underway,
and has been accomplished for factor IX,7779 anti-
thrombin 111,80.81 and phosphoglycerate kinase.82’83
Prenatal diagnosis of deficiencies for these proteins has
not been performed with these probes and awaits
determination of whether the diseases are due to gene
deletion or whether mutant genes are linked to poly-
morphic restriction sites. The molecular approach to
prenatal diagnosis is under active investigation in
many laboratories, for both hematologic and nonhema-
tologic diseases.
Several hematologic diseases can currently be diag-
nosed by amniocentesis and nonrecombinant DNA
technology. One group in this category is the chromo-
some breakage syndromes, which have autosomal
recessive inheritance. The disorder with major hemato-
logic disease in this group is Fanconi’s anemia, in
which most patients develop aplastic anemia and/or
leukemia in childhood. All patients have increased
chromosome breakage, which is further increased fol-
lowing culture of cells with diepoxybutane (DEB), a
DNA crosslinker. Twenty-two pregnancies at risk for
Fanconi’s anemia have been monitored, and seven
affected fetuses were identified by the presence of
increased spontaneous and DEB breakage in cultured
amniotic fluid cells.84 Only four of the seven had
physical anomalies (two at birth and two of the five
terminated), and thus, ultrasound examination alone
would not have been diagnostic. One very recent case
had Fanconi’s anemia excluded in the first trimester by
the observation of no increase in breakage following
culture of chorionic villi alone or with DEB.85
Other chromosome breakage syndromes have an
increased incidence of neoplasia. Patients with ataxia
telangiectasia have immunodeficiencies and lymphoid
malignancies. One fetus was found to be affected,
based on finding a clastogenic factor in the amniotic
fluid that produced chromosome breaks in normal
lymphocytes, as well as increased breakage of the fetal
amniotic cells plus a translocation involving chromo-
some 14 in those cells.86 Patients with Bloom’s syn-
drome show growth retardation and develop leukemia
and other malignancies at an early age. Cultured cells
have increased breakage plus very high numbers of
sister chromatid exchanges (SCEs). Several pregnan-
cies at risk have been monitored by ultrasound and
amniotic cell SCE, but all were normal.87 Xerodermapigmentosum is characterized by skin sensitivity to
sunlight and ocular and cutaneous malignancies. Cells
from such patients fail to repair ultraviolet irradiation-
induced damage. Three pregnancies have beenreported to be monitored for xeroderma pigmentosum,
and two fetuses were found to be affected.88’89 All of
these conditions in which amniotic fluid cultures were
assayed might be detected in cultured chorionic villi.
Amniotic cells have been used to identify disorders
affecting cellular enzymes. One example is glucose
phosphate isomerase deficiency, which results in severe
congenital nonspherocytic hemolytic anemia. A fetus
at risk was diagnosed in utero by assay of the amniotic
cell enzyme level, and then was treated immediately
following birth by exchange transfusionsY#{176} Severe
methemoglobinemia due to cytochrome b5 reductase
deficiency was detected in amniotic fluid cells.9’ Both
of these enzyme deficiency disorders could presumably
have been diagnosed from studies of fetal blood or from
chorionic villi, if sufficient material were available.
Porphyria can also be diagnosed by analysis of
enzymes in amniotic cells. Sassa et al diagnosed auto-
somal dominant acute intermittent porphyria due to
deficiency in uroporphyrinogen I synthetase,92 and
Deybach et al excluded autosomal recessive congenital
erythropoietic porphyria by observing normal levels of
uroporphyrinogen III cosynthetase.93
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

PRENATAL DIAGNOSIS OF HEMATOLOGIC DISEASES 337
Properties of white cells that are expressed in
amniotic cells can be used to diagnose nonhematologic
conditions as well. Pollack Ct al used HLA typing of
amniotic fibroblasts to determine paternity, assess
whether fetuses could be bone marrow transplant
donors or recipients, and diagnose HLA-linked dis-
eases, congenital adrenal hyperplasia due to 21-
hydroxylase deficiency, and complement C4 deficien-
cy.94 Forest et al also used HLA linkage, combined
with amniotic fluid hormone levels, to diagnose con-
genital adrenal hyperplasia in utero.95 HLA typing can
also be performed on white cells obtained from fetal
blood and perhaps on chorionic villi cells as well.
It should be stressed that the reliability of prenatal
testing for many of the hematologic and nonhemato-
logic disorders discussed here awaits the test of time.
The numbers of cases studied are often small. The
experience with muscular dystrophy (Table 7) has
shown that in utero tests may not be error-free. The
proper role of prenatal testing requires a reliable assay
that distinguishes affected from unaffected fetuses;
such assays are still being developed for some of the
conditions summarized in this review.
SUMMARY
Prenatal diagnosis of hematologic diseases can now
be performed with fetal blood, fetal amniotic fluid cell
DNA, and fetal chorionic villi DNA. Some hemoglo-
binopathies can be detected by all three methods, and
the choice will depend on the available obstetric and
laboratory techniques, as well as the time of presenta-
tion of the pregnancy. Hopefully, further development
of molecular probes and techniques will soon expand
these options to all of the globin disorders.
Detection of coagulation disorders in utero currently
requires samples of pure fetal blood. Gene cloning is
accomplished for some (factor IX and antithrombin
III) and is underway for others (factor VIII), and
further investigation is necessary to determine whether
deficiencies in these gene products are due to gene
deletion or to mutant genes linked to polymorphic
restriction enzyme sites of diagnostic use. Thus, molec-
ular biology may be applied to prenatal diagnosis of
the clotting problems, but this has not yet been accom-
plished.
Disorders affecting the number and/or function of
erythrocytes, leukocytes, and platelets can be diag-
nosed by analysis of fetal blood. Blood samples will
continue to be required until more is known about the
molecular biology of hematopoiesis.
Syndromes that can be diagnosed by chromosome
studies should be revealed in cultures of amniotic fluid
cells, fetal blood lymphocytes, and chorionic villi cells.
Cultured cells can be examined for karyotypes, Y-
chromatin, spontaneous or induced chromosome
breakage, DNA repair, SCEs, and translocations. The
techniques for culturing amniotic cells and fetal blood
white cells are established, and those for growing cells
from chorionic villi are improving rapidly. Direct prep-
arations of cells from villi only may suffice for some of
the above analyses.
The study of hematologic disease in utero has thus
come full circle, from the use of amniotic cells to
determine the sex in X-linked disorders, to fetal blood
sampling for the analysis of gene products, then back
to amniocentesis for DNA, and now earlier in gestation
to chorionic villi. All of this has occurred in less than
ten years, and it is anticipated that developments in the
next ten years will be equally dramatic. The future
should bring all prenatal testing into the first trimester,
use molecular probes, and provide for both early
diagnosis and early treatment of genetic hematologic
disease.
ACKNOWLEDGMENT
I am grateful to Dr Anver Kuliev for arranging for support from
the World Health Organization. Principal members of previous and
current International Registries are as follows, listed alphabetically
by country:
Australia: Melbourne, Queen Victoria Hospital, R. Matthews,
R. Sharma, W. Walters; Melbourne, Royal Women’s Hospital,
M. Cauchi, FR. Betheras; Sydney, V. Berdoukas. Canada: Mon-
treal, F. Congote, T. Perry; Toronto, R. Benzie; Hamilton,
S.C. Wong. Cyprus: Nicosia, M. Angastiniotis. Denmark: Copenha-
gen, i. Bang. England: London, King’s College Hospital, C. Rodeck,
R. Mibashan; University College Hospital, B. Modell, D. Fairweath-
er, R.H.T. Ward; Oxford, i. Old, Di. Weatherall. France: Paris,
M. Goossens. Germany: Munich, M. Jensen. Greece: Athens,
D. Loukopoulos, A. Antsaklis. Israel: Jerusalem, E. Rachmilewitz.
Italy: Ferrara, M. Lucci, C. Vullo; Milan, B. Brambatti, M. Ferrari;
Rome, A. Pachi, L. Tentori; Sardinia, A. Cao. Sweden: Malmo,
B. Gustavii, L. Holmberg, R. Ljung. United States: Baltimore,
H.H. Kazazian, Jr.; Boston, D.G. Nathan, S.H. Orkin; Hartford,
L. Hoyer; New Haven, Mi. Mahoney, iC. Hobbins, B.G. Forget;
New York, B.P. Alter, A. Bank; San Francisco, Y.W. Kan,
MS. Golbus.
REFERENCES
1. Orkin SH: Prenatal diagnosis of hemoglobin disorders by
DNA analysis. Blood 63:249, 1984
2. Alter BP: Prenatal diagnosis of haemoglobinopathies: A status
report. Lancet 2:1 152, 1981
3. Alter BP: Antenatal diagnosis of fetal hematologic diseases, in
Cherry S. Kase NG, Berkowitz R (eds): Rovinsky and Guttmacher:
Medical, Surgical and Gynecological Complications of Pregnancy
(ed 3). Baltimore, Williams & Wilkins, 1984 (in press)
4. Kan YW, Valenti C, Carnazza V, Guidotti R, Rieder RF:
Fetal blood-sampling in utero. Lancet I :79, 1974
5. Kan YW, Golbus MS. Klein P, Dozy AM: Successful applica-
tion of prenatal diagnosis in a pregnancy at risk for homozygous
�9-thalassemia. N Engi i Med 292:1096, 1975
6. Hobbins iC, Mahoney Mi: In utero diagnosis of hemoglobino-
pathies. Technic for obtaining fetal blood. N Engl i Med 290:1065,
I 974
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

338 BLANCHE P. ALTER
7. Rodeck CH: Fetoscopy guided by real-time ultrasound for
pure fetal blood samples, fetal skin samples, and examination of the
fetus in utero. Br J Obstet Gynaecol 87:449, 1980
8. MacKenzie lZ, Maclean DA: Pure fetal blood from the
umbilical cord obtained at fetoscopy: Experience with I 25 consecu-
tive cases. Am i Obstet Gynecol 138:1214, 1980
9. Daffos F, Capella-Pavlovsky M, Forestier F: A new procedure
for fetal blood sampling in utero: Preliminary results of fifty-three
cases. Am i Obstet Gynecol 146:985, 1983
10. Gustavii B, Cordesius E: Transvaginal fetoscopy in anterior
placentas. Acta Obstet Gynecol Scand 59:231, 1980
I I . Bang i, Bock iE, Trolle D: Ultrasound-guided fetal intrave-
nous transfusion for severe rhesus haemolytic disease. Br Med i
284:373, 1982
I 2. Ljung R, Holmberg L, Gustavii B, Philip J, Bang i: Haemo-
philia A and B-Two years experience of genetic counselling and
prenatal diagnosis. Clin Genet 22:70, 1982
I 3. Kleihauer E, Braun H, Betke K: Demonstrationem von
fetalem Hamoglobin in den Erythrocyten eines Blutausstrichs. Klin
Wochenschr 35:637, 1957
14. Alter BP, Modell CB, Fairweather D, Hobbins iC, Mahoney
Mi, Frigoletto FD, Sherman AS, Nathan DG: Prenatal diagnosis of
hemoglobinopathies. A review of 15 cases. N Engl J Med 295:1437,
1976
I 5. Alter BP: Antenatal diagnosis using fetal blood, in Weath-
erall Di (ed): Methods in Hematology: The Thalassemias.
Edinburgh, Churchill Livingstone, 1983, p 1 14
16. Cividalli G, Nathan DG, Kan YW, Santamarina B, Frigo-
letto F: Relation of beta to gamma synthesis during the first
trimester: An approach to prenatal diagnosis of thalassemia. Pediatr
Res 8:553, 1974
17. Alter BP: Prenatal diagnosis of hemoglobinopathies, in
Schwartz E (ed): Progress in Pediatric Hematology/Oncology, vol
III, Hemoglobinopathies in Children. Littleton, PSG Publishing,
1980, p 123
18. Alter BP, Metzger iB, Yock PG, Rothchild SB, Dover Gi:
Selective hemolysis of adult red blood cells: An aid to prenatal
diagnosis of hemoglobinopathies. Blood 53:279, 1979
19. Golbus MS: The use of fetal blood for the prenatal diagnosis
of genetic defects. Monogr Hum Genet 9:222, 1978
20. Alter BP, Orkin SH, Forget BG, Nathan DG: Prenatal
diagnosis of hemoglobinopathies: The New England approach. Ann
NY Acad Sci 344:151, 1980
21. Ward RHT, Modell B, Fairweather DVI, Shirley IM, Rich-
ards BA, Hetherington CP: Obstetric outcome and problems of
mid-trimester fetal blood sampling for antenatal diagnosis. Br i
Obstet Gynaecol 88:1073, 1981
22. Rodeck CH: Fetal blood sampling. Birth Defects 18:255,
1982
23. Cao A, Furbetta M, Galanello R, Melis MA, Angius A,
Rostelli C, Ruggeri R, Addis M, Tuveri T, Falchi AM, Maccioni L,
Paglietti E, Scalas MT: Control of homozygous �3-thalassemia by
carrier screening and antenatal diagnosis in Sardinia. Birth Defects
18:303, 1982
24. Tentori L, Pachi A, Bresadola M, Bilotta P. Alvino E,
Paesano R, Massa A, Marinucci M, Vignetti M, Sposi NM,
Dallapiccola B: Prenatal diagnosis of /3-thalassemia: The experience
of the center of Rome. Birth Defects 18:313, 1982
25. Ferrari M, Cantu-Rajnoldi A, Crema A, Pietri 5, Travi M:
Prenatal diagnosis of thalassemia and fetal red cell microcytosis.
Prenat Diag 2:143, 1982
26. Loukopoulos D, Antsaklis A, Aleporou-Marinou V. Panour-
gius i, Karabara P. Fessas P: Prenatal diagnosis of $-thalassemia:
The Greek experience. Birth Defects 18:293, 1982
27. Blouquit Y, Beuzard Y, Varnavides L, Chabret C, Dumez Y,
iohn PN, Rodeck C, White iM: Antenatal diagnosis of haemoglo-
binopathies by Biorex chromatography of haemoglobin. Br i Hae-
matol 50:7, 1982
28. iensen M: Fetal globin synthesis and prenatal diagnosis of
thalassemia. Adv Physiol Sci 6:153, 1981
29. Cividalli GG, Antebi 5, Klein R, Kerem H, Rachmilewitz
EA: Prenatal diagnosis of heterozygous fi-thalassemia. Isr i Med Sci
12:1313, 1976
30. Congote LF, Hamilton EF, Chow JCW, Perry TB: Prenatal
diagnosis of hemoglobinopathies: Evaluation of techniques for ana-
lysing globin-chain synthesis in blood samples obtained by fetoscopy.
Can Med Assoc i 127:843, 1982
31. Matthews RN, Walters WAW, Sharma RS, Malios i:
Antenatal diagnosis of thalassemia. Med i Aust 2:440, 1978
32. Cao A: Community control ofthalassemia major in developed
countries. Clin Gen 24:284, 1983
33. NICHD National Registry for Amniocentesis Study Group:
Midtrimester amniocentesis for prenatal diagnosis. JAMA
236:1471, 1976
34. Williamson R, Eskdale i, Coleman DV, Niazi M, Loeffler
FE, Modell BM: Direct gene analysis of chorionic villi: A possible
technique for first-trimester antenatal diagnosis of haemoglobinopa-
thies. Lancet 2:1 125, 1981
35. Old iM, Ward RHT, Petrou M, Karagozlu F, Modell B,
Weatherall Di: First-trimester fetal diagnosis for haemoglobinopa-
thies: Threecases. Lancet 2:1413, 1982
36. Goossens M, Dumez Y, Kaplan L, Lupker M, Chabret C,
Henrion R, Rosa i: Prenatal diagnosis of sickle-cell anemia in the
first trimester of pregnancy. N Engl i Med 309:83 1 , I 983
37. Hobbins iC: Determination of fetal sex in early pregnancy. N
Engl i Med 309:979, 1983
38. Orkin SH, Kazazian HH Jr. Antonarakis SE, Goff SC,
Boehm CD, Sexton iP, Waber PG. Giardina PJV: Linkage of
f3-thalassemia mutations and 13-globin gene polymorphisms with
DNA polymorphisms in human �-globin gene cluster. Nature
296:627, 1982
39. Pirastu M, Kan YW, Cao A, Conner Bi, Teplitz RL, Wallace
RB: Prenatal diagnosis of $-thalassemia. Detection of a single
nucleotide mutation in DNA. N EngI i Med 309:284, 1983
40. Orkin SH, Markham AF, Kazazian HH Jr: Direct detection
of the common Mediterranean fl-thalassemia gene with synthetic
DNA probes. An alternative approach for prenatal diagnosis. i CIin
Invest 71:775, 1983
41. Jones JR. McCormack M, Dietzel C, Tricomi V, Ramirez F:
Antenatal diagnosis of sickle cell disease: Amniotic fluid cell DNA
analysis. Obstet Gynecol 59:484, 1982
42. Chang JC, Golbus MS, Kan YW: Antenatal diagnosis of
sickle cell anaemia by sensitive DNA assay. Lancet 1:1463, 1982
43. Boehm CD, Antonarakis SE, Phillips JA III, Stetten G,
Kazazian HH Jr: Prenatal diagnosis using DNA polymorphisms.
Report on 95 pregnancies at risk for sickle-cell disease or $-thalassemia. N Engl J Med 308:1054, 1983
44. Firshein SI, Hoyer LW, Lazarchick J, Forget BG, Hobbins
JC, Clyne LP, Pitlick FA, Muir WA, Merkatz IR, Mahoney Mi:
Prenatal diagnosis of classic hemophilia. N Engl i Med 300:937,
1979
45. Mibashan RS, Peake IR, Rodeck CH, Thumpston iK, Fur-
long RA, Gorer R, Bains L, Bloom AL: Dual diagnosis of prenatal
haemophilia A by measurement of fetal factor VIIIC and VIIIC
antigen (VIIICAg). Lancet 2:994, 1980
46. Mibashan R, Rodeck C, Thumpston i: Prenatal diagnosis of
the hemophilias, in Bloom AL (ed): Methods in Hematology: The
Hemophilias. Edinburgh, Churchill Livingstone, 1982 p 176
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

PRENATAL DIAGNOSIS OF HEMATOLOGIC DISEASES 339
Prenatal exclusion of Hurler’s disease by leucocyte a-L-iduronidase
assay. Prenat Diag 3:61, 1983
47. Omenn GS, Figley MM, Graham CB, Heinrichs WL: Pros-
pects for radiographic intrauterine diagnosis-The syndrome of
thrombocytopenia with absent radii. N EngI i Med 288:777, 1973
48. Luthy DA, Hall iG, Graham CB: Prenatal diagnosis of
thrombocytopenia with absent radii. Clin Genet I 5:495, 1979
49. Holmberg L, Gustavii B, ionsson A: A prenatal study of fetal
platelet count and size with application to fetus at risk for Wiskott-
Aldrich syndrome. i Pediatr 102:773, 1983
50. Philip J, Brandt NJ, Fernandes A, Freiesleben E, Trolle D:
ABO and Rh phenotyping of foetal blood obtained by foetoscopy.
ClinGenet 14:324, 1978
51. Golbus MS. Stephens iD, Cann HM: In utero paternity
testing utilizing fetal blood obtained by midtrimester fetoscopy. Am
i Hum Genet 32:88, 1980
52. Rodeck CH, Kemp JR. Holman CA, Whitmore DN, Kar-
nicki i, Austin MA: Direct intravascular fetal blood transfusion by
fetoscopy in severe rhesus isoimmunisation. Lancet 1:625, 1981
53. Lestas AN, Rodeck CH, White iM: Normal activities of
glycolytic enzymes in the fetal erythrocytes. Br J Haematol 50:439,
1982
54. Fensom AH, Benson PF, Rodeck CH, Campbell 5, Gould
JDM: Prenatal diagnosis of a galactosaemia heterozygote by fetal
blood enzyme assay. Br Med J 1:21, 1979
55. Oski FA, Naiman JL: Hematologic Problems in the Newborn
(ed 3). Philadelphia, WB Saunders, 1982, p4
56. Linch DC, Knott Li, Rodeck CH, Huehns ER: Studies of
circulating hemopoietic progenitor cells in human fetal blood. Blood
59:976, 1982
57. Newburger PE, Cohen Hi, Rothchild SB, Hobbins iC,
Malawista SE, Mahoney Mi: Prenatal diagnosis of chronic granu-
lomatous disease. N Engl i Med 300: 178, 1979
58. Borregaard N, Bang i, Berthelsen iG, iohansen KS, Koch C,
Philip J, Rasmussen K, Schwartz M, Therkelsen Ai, Valerius NH:
Prenatal diagnosis of chronic granulomatous disease. Lancet I : 1 14,
1982
59. Newburger PE, Latt SA: Improved fluorescent staining of
interphase nuclei for prenatal diagnosis. Lancet 1:1 144, 1979
60. Simmonds HA, Fairbanks LD, Webster DR. Rodeck CH,
Linch DC, Levinsky Ri: Rapid prenatal diagnosis of adenosine
deaminase deficiency and other purine disorders using foetal blood.
Biosci Rep3:31, 1983
61. Hirschhorn R, Beratis N, Rosen FS, Parkman R, Stern R,
Polmar S: Adenosine-deaminase deficiency in a child diagnosed
prenatally. Lancet 1:73, 1975
62. Ziegler iB, Van Der Weyden MB, Lee CH, Daniel A:
Prenatal diagnosis for adenosine deaminase deficiency. i Med Genet
18:154, 1981
63. Levinsky Ri, Linch DC, Beverly CL, Rodeck C: Prenatal
exclusion of severe combined immunodeficiency. Arch Dis Child
57:958, 1982
64. Durandy A, Oury C, Griscelli C, Dumez Y, Oury iF,
Henrion R: Prenatal testing for inherited immune deficiencies by
fetal blood sampling. Prenat Diag 2: 109, 1982
65. Durandy A, Dumez Y, Guy-Grand D, Oury C, Henrion R,
Griscelli C: Prenatal diagnosis of severe combined immunodeficien-
cy. i Pediatr 101:995, 1982
66. Cordesius E, Gustavii B, Mitelman F: Prenatal chromosomal
analysis of fetal blood obtained at fetoscopy. Br Med i 1:1107,
1980
67. Webb T, Butler D, Insley i, Weaver iB, Green S, Rodeck C:
Prenatal diagnosis of Martin-Bell syndrome associated with fragile
site at Xq27-28. Lancet 2:1423, 1981
68. Rodeck CH, Tansley LR, Benson PF, Fensom AH, Ellis M:
69. Mahoney Mi, Haseltine FP, Hobbins JC, Banker BQ, Cas-
key CT, Golbus MS: Prenatal diagnosis of Duchenne’s muscular
dystrophy. N EngI i Med 297:968, 1977
70. Dubowitz V, Van Iddekinge B, Rodeck CH, Campbell 5,
Singer iD, Scheuerbrandt G, Moss DW: Prenatal diagnosis in
Duchenne muscular dystrophy: Salvage of normal male fetus. Lan-
cet 1:90, 1978
7 1. lonasescu V, Zelleger H, Cancilla P: Fetal serum-creatine-
phosphokinase not a valid predictor of Duchenne muscular dystro-
phy. Lancet 2:1251, 1978
72. Golbus MS. Stephens JD, Mahoney Mi, Hobbins iC, Hasel-
tine FP, Caskey CT, Banker BQ: Failure of fetal creatine phosphoki-
nase as a diagnostic indicator of Duchenne muscular dystrophy. N
EngI i Med 300:860, 1979
73. Harper PS, O’Brien T, Murray iM, Davies KE, Pearson P.
Williamson R: The use of linked DNA polymorphisms for genotype
prediction in families with Duchenne muscular dystrophy. i Med
Genet 20:252, 1983
74. Kingston HM, Thomas NST, Pearson PL, Sarfarazi M,
Harper PS: Genetic linkage between Becker muscular dystrophy
and a polymorphic DNA sequence on the short arm of the X
chromosome. i Med Genet 20:255, 1983
75. Perry TB, Hechtman P. Chow JCW: Diagnosis of Tay-Sachs
disease on blood obtained at fetoscopy. Lancet 1:972, 1979
76. ieppsson JO, Cordesius E, Gustavii B, Lofberg L, Franzen B,
Stromberg P, Sveger T: Prenatal diagnosis of alpha�-antitrypsin
deficiency by analysis of fetal blood obtained at fetoscopy. Pediatr
Res 15:254, 1981
77. Choo KH, Gould KG, Rees DiG, Brownlee GG: Molecular
cloning of the gene for human anti-haemophilic factor IX. Nature
299:178, 1982
78. Kurachi K, Davie EW: Isolation and characterization of a
cDNA coding for human factor IX. Proc Nat) Acad Sci USA
79:6461, 1982
79. iaye M, de Ia Salle H, Schamber F, Balland A, Kohli V.
Findeli A, Tolstoshev P, Lecocq i-P: Isolation of a human anti-
haemophilic factor IX cDNA clone using a unique 52-base synthetic
oligonucleotide probe deduced from the amino acid sequence of
bovine factor IX. Nucleic Acid Res I 1:2325, 1983
80. Chandra 1, Stackhouse R, Kidd Vi, Woo SLC: Isolation and
sequence characterization of a cDNA clone of human antithrombin
III. Proc Nati Acad Sci USA 80:1845, 1983
81 . Prochownik EV, Antonarakis S, Bauer KA, Rosenberg RD.
Fearon ER, Orkin SH: Molecular heterogeneity of inherited anti-
thrombin III deficiency. N EngI i Med 308:1549, 1983
82. Michelson AM, Markham AF, Orkin SH: Isolation and
DNA sequence of a full-length cDNA clone for human X chromo-
some-encoded phosphoglycerate kinase. Proc Natl Acad Sci USA
80:472, 1983
83. Singer-Sam J, Simmer RL, Keith DH, Shively L, Teplitz M,
Itakura K, Gartler SM, Riggs AD: Isolation of a cDNA clone for
human X-linked 3-phosphoglycerate kinase by use of a mixture of
synthetic oligonucleotides as a detection probe. Proc Natl Acad Sci
USA 80:802, 1983
84. Auerbach AD: Diagnosis of diseases of DNA synthesis and
repair that affect the skin using cultured amniotic fluid cells, in Rook
Ai, Maibach HI (eds): Prenatal Diagnosis of Inherited Skin Dis-
ease. New York, Thieme-Stratton, 1984 (in press)
85. Auerbach AD, Pergament E, Alter BP: Unpublished observa-
tions
86. Shaham M, Voss R, Becker Y, Yarkoni 5, Ornoy A, Kohn G:
Prenatal diagnosis of ataxia telangiectasia. i Pediatr 100:134, 1982
87. Passarge E: Bloom’s syndrome, in German J (ed): Chromo-
some Mutation and Neoplasia. New York, AR Liss, 1983, p 1 1
88. Ramsay CA, Coltart TM, Blunt 5, Pawsey SA, Giannelli F:
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

340 BLANCHE P. ALTER
Prenatal diagnosis of xeroderma pigmentosum. Report of the first
successful case. Lancet 2:1 109, 1974
89. Halley DL, Keijzer W, iaspers NGJ, Niermeijer MF, Kleijer
WJ, Boue J, Boue A, Bootsma D: Prenatal diagnosis of xeroderma
pigmentosum (group C) using assays ofunscheduled DNA synthesis
and postreplication repair. Clin Genet 16:137, 1979
90. Whitelaw AOL, Rogers PA, Hopkinson DA, Gordon H,
Emerson PM, Darley JH, Reid C, Crawfurd Md’A: Congenital
haemolytic anaemia resulting from glucose phosphate isomerase
deficiency: Genetics, clinical picture, and prenatal diagnosis. J Med
Genet 16:189, 1979
91. Junien C, Leroux A, Lostanlen D, Reghis A, Boue i, Nicolas
H, Boue A, Kaplan iC: Prenatal diagnosis of congenital enzymo-
penic methaemoglobinaemia with mental retardation due to general-
ized cytochrome b5 reductase deficiency: First report of two cases.
Prenat Diag 1:17, 1981
92. Sassa 5, Solish G, Levere RD. Kappas A: Studies in por-
phyria. IV. Expression of the gene defect of acute intermittent por-
phyria in cultured human skin fibroblasts and amniotic cells: Prena-
tal diagnosis of the porphyric trait. J Exp Med 142:722, 1975
93. Deybach J Ch, Grandchamp B, Grelier M, Nordmann Y,
Boue J, Boue A, de Berranger P: Prenatal exclusion of congenital
erythropoietic porphyria (Gunther’s disease) in a fetus at risk. Hum
Genet 53:217, 1980
94. Pollack MS. Heagney SD, Braun D Jr, O’Neill GJ: Technical
and theoretical considerations in the HLA typing of amniotic fluid
cells for prenatal diagnosis and paternity testing. Prenat Diag I :183,
1981
95. Forest MG, Betuel H, Couillin P. Boue A: Prenatal diagnosis
of congenital adrenal hyperplasia (CAH) due to 21-hydroxylase
deficiency by steroid analysis in the amniotic fluid of mid-pregnan-
cy: Comparison with HLA typing in 17 pregnancies at risk for CAH.
Prenat Diag 1:197, 1981
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom

1984 64: 329-340
BP Alter Advances in the prenatal diagnosis of hematologic diseases
http://www.bloodjournal.org/content/64/2/329.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on April 14, 2017. by guest www.bloodjournal.orgFrom