advanced practice nursing report - arkansas general assembly
TRANSCRIPT

Advanced Practice Nursing
Interim Study Proposal 2007-238
December 18, 2008 Prepared for Rep. Sandra Prater and Rep. Clark Hall
Bureau of Legislative Research Project Number 08-286

Page i
Table of Contents About This Study ................................................................................................................................1
Executive Summary............................................................................................................................2
Background.........................................................................................................................................4
Advanced Practice Nurse ..................................................................................................................4 State Licensing..................................................................................................................................4 Prescriptive Authority ........................................................................................................................4 Collaborative Agreements .................................................................................................................5
State Laws and Policies .....................................................................................................................6
Arkansas ...........................................................................................................................................6 Alaska................................................................................................................................................7 Arizona ..............................................................................................................................................8 Idaho .................................................................................................................................................9 Iowa.................................................................................................................................................10 Maine ..............................................................................................................................................11 Montana ..........................................................................................................................................12 New Hampshire...............................................................................................................................13 New Mexico.....................................................................................................................................14 Oregon ............................................................................................................................................15 Utah.................................................................................................................................................16 Washington State ............................................................................................................................17 Washington D.C. .............................................................................................................................18 Wyoming .........................................................................................................................................19 Other States ....................................................................................................................................20
Health Care Expenditures ................................................................................................................21 Total Health Care Expenditures ......................................................................................................21 Expenditures: Hospital Care............................................................................................................22 Expenditures: Physician and Other Professional Services..............................................................23 Expenditures: Drugs and Other Medical Nondurables ....................................................................24
Access to Health Care ......................................................................................................................25
Population Lacking Primary Care, 2007 ..........................................................................................25 Population Lacking Primary Care, 1992 - 2007 ...............................................................................26 Rate of Physicians in Primary Care, 2006.......................................................................................27 Rate of Physicians in Primary Care, 1992 - 2006............................................................................28 Rate of Physicians in General/Family Practice, 2006......................................................................29 Rate of Physicians in General/Family Practice, 1992 - 2006...........................................................30 Primary Care Doctors as Percent of All Doctors..............................................................................31 Rate of Advanced Practice Nurses..................................................................................................32 Rate of Nurse Practitioners .............................................................................................................33 Arkansas's Medically Underserved Areas .......................................................................................34 Area Health Education Centers .......................................................................................................35 Community Health Centers of Arkansas .........................................................................................36 Family and General Practice Physicians per 10,000 Population .....................................................37 Nurse Practitioners with Prescriptive Authority per 10,000 Population............................................38 Adverse Actions for Advanced Practice Nurses ..............................................................................39 Adverse Actions in States That Repealed Collaborative Agreement Requirements........................40 Hospital Emergency Room Visits ....................................................................................................43

Page ii
State Health Indicators .....................................................................................................................44
State Health Ranking ......................................................................................................................44 Teen Births ......................................................................................................................................45 Births to Women Receiving Late or No Prenatal Care ....................................................................46 Low Birth Weight Babies .................................................................................................................47 Infant Mortality.................................................................................................................................48 Heart Disease Deaths .....................................................................................................................49

Page 1
About This Study
This study examines the policies and some general health indicators in the 12 states and Washington D.C. that do not require advanced practice nurses to enter collaborative agreements with physicians. This study also examines the policies in Arkansas, where collaborative agreements are required. The first section of this study provides some background on advanced practice nursing and describes how states typically license these healthcare professionals. The next section compares individual states' laws and policies regarding collaborative agreements and prescriptive authority. The remaining sections examine whether fewer restrictions on advanced practice nurses' authority (i.e., the elimination of collaborative agreements) has any real effect on a state's health expenditures, access to health care professionals and services, or overall health statistics. Representatives from the Arkansas Nurses Association and the Arkansas State Nursing Board helped develop the structure of this report and determined what types of information should be collected. The state health outcome indicators, such as the infant mortality rate, were selected as measures of each state's basic medical care. Advanced practice nurses, particularly nurse practitioners, focus on disease prevention and primary care. The Arkansas Medical Society was also asked to suggest additional health statistics that should be compared. David Wroten, Executive Vice President of the Arkansas Medical Society, objected to the study's structure, noting, "The primary problem with that analysis is that it requires making a determination that the differences in health statistics between these states is somehow related to whether or not advanced practice nurses are required to have a collaborative practice agreement." Instead he suggested comparing the health statistics within a state that previously had a collaborative practice requirement, then repealed it. However, he cautioned that such a study also would have to determine whether any other factors led to the change in statistical health data. Wroten also suggested examining access to primary care in rural counties in states that have repealed collaborative agreement requirements. He suggested looking at the county-by-county distribution of primary care physicians and advanced practice nurses in those states before and after a collaborative agreement has been repealed. Some of the data Wroten suggested obtaining was collected, and additional charts were included in this report. However, in many cases, the data either was not available or was too limited. Additional analyses may be warranted.

Page 2
Executive Summary Most states allow advanced practice nurses (APNs) to prescribe medications, including controlled substances. However, many, including Arkansas, grant prescriptive authority to APNs only if they enter into a written collaborative agreement with a physician. The nursing community sees this requirement as an unnecessary additional burden on an APN's practice. The nursing community believes that if APNs were given more autonomy, they could increase patients' access to care, especially in rural areas that struggle to attract physicians. Because it costs less to see an APN than a physician, APNs practicing more independently could offer access to more affordable care for the state's under-insured or uninsured, the nursing community believes. In Arkansas, 16.8% of the population is uninsured and nearly 23% of the population is enrolled in Medicaid. The physician community, on the other hand, contends that APNs have not had as much training as physicians and should not be allowed to prescribe dangerous medications, including controlled substances, without the oversight of a physician. The safety of patients could be compromised, the physician community believes. Twelve states and Washington D.C. either have never had collaborative agreement requirements, eliminated existing collaborative agreement requirements, or redefined collaboration in a way that effectively eliminated the restrictions they placed on APNs. Seven of the 12 states eliminated existing collaborative agreement requirements. Alaska was the first in 1984, and last year, the state of Washington became the latest state to eliminate its collaborative agreement requirement. This study also examined state health and health care data to see whether the states with the fewest practice restrictions on APNs did better or worse than the national average on selected measures. This study found few trends either way. On total health care expenditures, four states and the District of Columbia had higher costs than the national average, while eight states' costs were lower. In about half the states, a greater percentage of the population than the national average lives in an area considered to be underserved by primary care physicians, while in the other half of the states a smaller percentage than the national average lives in underserved areas. Not surprisingly, a similar state breakdown occurred for the number of primary care physicians per 100,000 population in each state. The term "primary care physicians" refers to family and general practice doctors, internists, pediatricians, obstetricians, and gynecologists. Data on the rate of general or family practice doctors exclusively presents a different picture. Only two of the 12 states — Utah and Arizona — have rates below the national average. That means that most of the states that do not have a collaborative agreement requirement have more general and family practice doctors to serve their population. There is no national average for the number of advanced practice nurses per 100,000 population because no organization reliably collects and analyzes that data. However, this study collected the information for the 12 states examined and the District of Columbia. Washington D.C., Alaska, and New Hampshire, which were the first to eliminate their collaborative agreement requirements, have some of the highest rates of APNs. Those two states and Washington D.C. also had the highest rates of nurse practitioners.

Executive Summary
Page 3
This study took a closer look at the primary care staffing patterns in Arkansas. The state Department of Health map on page 34 shows the areas of the state that are federally designated as being medically underserved. Fifty-nine of the state's 75 counties are designated as being medically underserved across the entire county, while portions of another 14 counties are medically underserved. Two counties have no medically underserved areas. Currently the number of nurse practitioners with prescriptive authority per 10,000 population is most heavily concentrated in central Arkansas. Pulaski, White, Izard and Pike counties had the highest rates of nurse practitioners. The rate of family and general practice doctors is more widely spread throughout the state, with the heaviest concentrations in south and northeast/north central Arkansas. The number of adverse actions—disciplinary sanctions, malpractice payments, and other similar issues—against advanced practice nurses is relatively low, according to data from the federal National Practitioner Data Bank and the Health Integrity and Protection Data Bank. The data banks do not document a rate of adverse actions for advanced practice nurses, nor a national average. Still, there were rarely more than 10 adverse actions reported annually for any of the states examined in this study. This study also examined the number of adverse actions in each state that previously had a collaborative agreement requirement and then repealed it. The data found no increasing or decreasing trend in the number of adverse actions after the collaborative agreement requirement was repealed. Eight of the 12 states had a lower rate of emergency room visits than the national average. In the ranking of the states in overall health, which is published annually by the UnitedHealth Foundation, the states without a collaborative agreement requirement ranked everywhere from 1st to 41st. However, all states ranked higher (i.e., healthier) than Arkansas. The states that eliminated collaborative agreements generally had lower teen birth rates, lower rates of mothers without prenatal care, lower percentages of low birth-weight babies, and lower infant mortality rates than the national averages. All 12 states examined in this study had lower heart disease deaths than the national average. Only the District of Columbia's rate exceeded the national average. While the data found that states without collaborative agreement requirements had similar statistics in child birth indicators and heart disease deaths, this study does not address whether those statistics are the result of fewer restrictions on advanced practice nurses.

Page 4
Background
Advanced Practice Nurse An advanced practice nurse (APN), also known as advanced practice registered nurse (APRN), is an umbrella term used to describe nurses with advanced clinical experience and a high level of nursing education — generally a master's degree or higher. These nurses are more advanced than licensed practical nurses (LPNs) and regular registered nurses (RNs). In many states advanced practice nurses can operate their own practices and bill for services, separate from a physician's clinic. They have the authority to diagnose and prescribe medications, including controlled drugs. Under this umbrella group, there are four types of nursing specialties/licenses that are commonly considered advanced practice.
• Nurse practitioners work in clinics, nursing homes, and hospitals to provide primary and preventive health care services, prescribe medication, and diagnose and treat common minor illnesses and injuries.
• Certified nurse midwives provide well-woman gynecological and low-risk obstetrical
care. They attend births in hospitals, birthing centers, and private homes.
• Clinical nurse specialists work in hospitals, clinics, and nursing homes and specialize in a particular area of medicine, such as geriatrics, cardiology, or critical care.
• Certified registered nurse anesthetists (or certified nurse anesthetists) administer
anesthesia in collaboration with surgeons, anesthesiologists, and dentists. They practice in every setting in which anesthesia is delivered, including hospitals, surgical centers, and dental offices.
State Licensing Each state licenses advanced practice nurses differently. Some states, like Arkansas, license each of the four types through one section of law dealing with advanced practice nursing. Others have no umbrella grouping spelled out in law, but license two or three types individually.
Prescriptive Authority In many states, advanced practice nurses are given the authority to prescribe medications, including controlled substances. Some states automatically grant prescriptive authority to advanced practice nurses when they become licensed, while others, including Arkansas, require advanced practice nurses to apply for prescriptive authority separately. Many states only grant prescriptive authority after APNs have fulfilled additional requirements, such as completing a course in pharmacology or a year prescribing under the direct supervision of a physician.

Background
Page 5
All states examined in this study, except Arkansas, allow advanced practice nurses to prescribe controlled substances for schedules II-V. Arkansas does not allow them to prescribe schedule II medications, which include Ritalin, OxyContin, methadone, and morphine.
Collaborative Agreements Some states, such as Arkansas, place restrictions on APNs' prescriptive authority by requiring them to document a "collaborative agreement" with a licensed physician. A collaborative agreement is meant to ensure that licensed physicians with the most extensive medical training are involved in the prescriptions that patients receive from APNs. At least one state, Vermont, requires nurses to enter collaborative agreements with physicians in order to be licensed as advanced practice nurses. Some states require APNs to be supervised by a physician if they want to prescribe. State laws typically define physician "supervision" as a more restrictive arrangement than "collaboration." While many states call for a collaborative agreement or collaboration, the actual level of physician involvement varies from state to state. Some states require minimal involvement — defining "collaborating" as simply consulting with a physician as needed. Others require APNs to sign a written agreement with a physician defining practice protocols the APN will use, the method and regularity of communication between the doctor and APN, and the level of oversight physicians will have over the APNs' prescriptions.

Page 6
State Laws and Policies
Arkansas
What categories of advanced practice nursing does the state recognize?
• Advanced registered nurse practitioner • Certified registered nurse anesthetist • Certified nurse midwife • Clinical nurse specialist
Total number of advanced practice nurses
• Advanced registered nurse practitioner: 900 • Certified registered nurse anesthetist: 414 • Certified nurse midwife: 21 • Clinical nurse specialist: 116
Total: 1,451 Number of APNs with prescriptive authority
• Advanced registered nurse practitioner: 794 • Certified registered nurse anesthetist: 0 • Certified nurse midwife: 14 • Clinical nurse specialist: 66
Total: 874 Statutory and regulatory history
In 1995, Arkansas began licensing advanced practice nurses and granting them prescriptive authority for controlled substances for schedules III-V. In order to prescribe, Arkansas law (17-87-310) requires APNs to have a collaborative practice agreement with a physician who has a practice comparable in scope, specialty, or expertise to that of the APN.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
APNs with prescriptive authority can prescribe controlled medications in schedules III-V controlled drugs. They cannot prescribe schedule II.
Educational requirements for prescriptive authority
APNs must complete pharmacology coursework, including three graduate credit hours of pharmacology from an accredited college or university, 45 contact hours in a pharmacology course, and three graduate credit hours of pharmacology included as part of an advanced practice nursing education program. They must also have had at least 300 hours of preceptorial experience in the prescription of drugs, medicines, and therapeutic devices with a qualified preceptor.
Source: Arkansas State Board of Nursing

State Laws and Policies
Page 7
Alaska
What categories of advanced practice nursing does the state recognize?
• Advanced nurse practitioner • Registered nurse anesthetist
Total number of advanced practice nurses
• Advanced nurse practitioner: 671 • Registered nurse anesthetists: 147
Total: 818 Number of APNs with prescriptive authority
Alaska does not track electronically the number of APNs with prescriptive authority. However, the Alaska Board of Nursing's executive administrator estimates that over 90% of the nurse practitioners (about 600) have prescriptive authority. She estimates that only about 20% of registered nurse anesthetists (about 30) have prescriptive authority.
Statutory and regulatory history
Alaska has no statute addressing the relationship between physicians and APNs. However, in 1984 new regulations took effect allowing independent practice for APNs, granting them prescriptive authority and abolishing the collaborative agreement requirement.
Does an APN need a separate certification to prescribe?
Yes. Advanced nurse practitioners automatically receive prescriptive authority for legend drugs when they receive a license if they request it. They can apply for prescriptive authority for controlled drugs after one year of prescribing. Mental health/psychiatric advanced nurse practitioners, however, can request an exemption and receive immediate authorization to prescribe controlled substances.
What schedule drugs can APNs prescribe?
Advanced practice nurses are limited to prescribing only legend drugs for the first year. Then they can prescribe controlled drugs schedules II-V.
Educational requirements for prescriptive authority
For authority to prescribe legend drugs, the regulations require 15 contact hours of education in pharmacology and clinical management of drug therapy within the two years before applying for prescriptive authority. For authority to prescribe controlled substances, the regulations require one year of experience prescribing legend drugs.
Source: Alaska Board of Nursing

State Laws and Policies
Page 8
Arizona What categories of advanced practice nursing does the state recognize?
• Registered nurse practitioners (including nurse midwives) • Clinical nurse specialists
Total number of advanced practice nurses
• Registered nurse practitioners (including nurse midwives): 3,170
• Clinical nurse specialists: 158 Total: 3,328 Arizona also has 557 certified registered nurse anesthetists, but unlike many other states, Arizona rules do not put certified nurse anesthetists under the advanced practice umbrella.
Number of APNs with prescriptive authority
• Registered nurse practitioners: 2,826 Clinical nurse specialists cannot prescribe medications. In Arizona, 478 certified registered nurse anesthetists also have prescriptive authority.
Statutory and regulatory history
Advanced practice nurses were formerly required to list the physician with whom they would be collaborating, but in 2001 the Nursing Board eliminated that requirement and changed the definition of "collaborate" in the administrative code. According to the new definition, "collaborate" means "to establish a relationship for consultation or referral with one or more licensed physicians on an as-needed basis. Direct or onsite supervision of the activities of a registered nurse practitioner by the collaborating physician is not required."
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
Registered nurse practitioners can prescribe medications within their specialty, including controlled substances schedules II-V. Clinical nurse specialists can prescribe durable medical equipment, but cannot prescribe any medications.
Educational requirements for prescriptive authority
To obtain prescriptive authority, advanced practice nurses must have a minimum of 45 contact hours of education within the last three years. The contact hours must include either pharmacology or clinical management of drug therapy.
Source: Arizona State Board of Nursing

State Laws and Policies
Page 9
Idaho Categories of APN • Certified nurse midwife
• Clinical nurse specialist • Nurse practitioner • Registered nurse anesthetist
Total number of advanced practice nurses
• Certified nurse midwives: 27 • Clinical nurse specialists: 33 • Nurse practitioners: 540 • Registered nurse anesthetists: 373
Total: 973 Number of APNs with prescriptive authority
• Certified nurse midwives: 27 • Clinical nurse specialists: 16 • Nurse practitioners: 535 • Registered nurse anesthetists: 50
Total: 628 Statutory and regulatory history
In 1998, Idaho gave advanced practice nurses prescriptive authority for all legend drugs and controlled substances schedules II-V, but all prescribing had to be done under the supervision of a physician. In 2004, the physician supervision requirement was removed.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
Advanced practice nurses can prescribe legend drugs and controlled substances schedules II-V.
Educational requirements for prescriptive authority
To obtain prescriptive authority, advanced practice nurses must complete 30 contact hours of post-basic education in pharmacotherapeutics.
Source: Idaho Board of Nursing

State Laws and Policies
Page 10
Iowa
What categories of advanced practice nursing does the state recognize?
There are four types of advanced registered nurse practitioners: • Certified clinical nurse specialist • Certified nurse midwife • Certified nurse practitioner • Certified registered nurse anesthetist
Total number of advanced practice nurses
• Certified nurse practitioners: 1,186 Family nurse practitioners: 636 Pediatric nurse practitioners: 180 School nurse practitioners: 2 Women's health care nurse practitioners: 153 Psychiatric/mental health nurse practitioners: 41 Adult nurse practitioner: 84 Gerontological nurse practitioners: 45 Neonatal nurse practitioners: 17 Acute care nurse practitioners: 27 Perinatal nurse practitioners: 1
• Certified nurse midwives: 75 • Certified registered nurse anesthetists: 464 • Clinical nurse specialists:105
Total: 1,830 Number of APNs with prescriptive authority
All 1,830 nurse practitioners, nurse midwives, nurse anesthetists and clinical nurse specialists have prescriptive authority for legend drugs. To prescribe controlled substances, advanced registered nurse practitioners must become registered with the Iowa Board of Pharmacy, which cannot separate out the number with a controlled substance registration.
Statutory and regulatory history
Advanced registered nurse practitioners have always been allowed to practice independently, but in 1992, they were given prescriptive authority for some medications. In 1994, they were granted authority to prescribe controlled substances. A Nursing Board rule still requires collaborative agreements when the advanced registered nurse practitioner performs "medically delegated functions," but it doesn't strictly define "collaborative agreement" nor "medically delegated functions."
Does an APN need a separate certification to prescribe?
No, not to prescribe legend drugs. However, advanced registered nurse practitioners must register with the Iowa Board of Pharmacy if they want to prescribe controlled substances.
What schedule drugs can APNs prescribe?
Once they are registered with the federal Drug Enforcement Administration and the Iowa Board of Pharmacy Examiners, they can prescribe controlled substances schedules II-V.
Additional educational requirements for prescriptive authority
All that is required is completion of a master's degree program in a nursing clinical specialty area and completion of an advanced practice educational program of study in a nursing specialty area. There is no additional requirement for prescriptive authority.
Source: Iowa Board of Nursing
State Laws and Policies
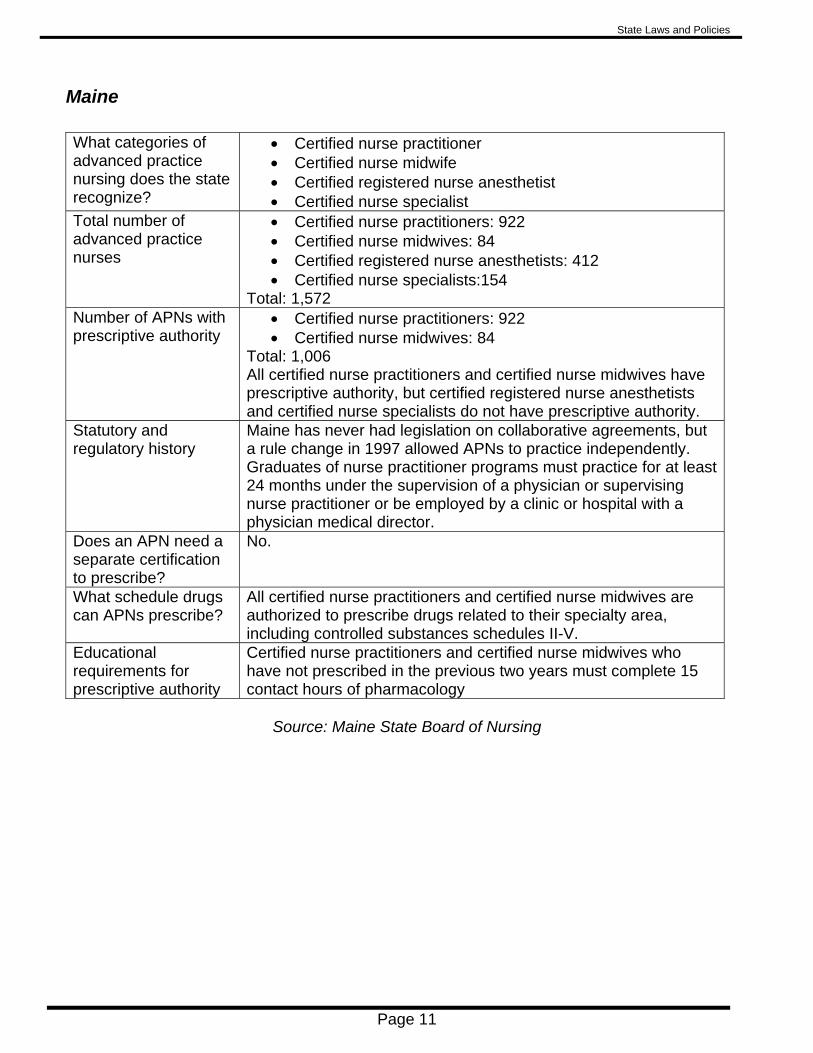
Page 11
Maine What categories of advanced practice nursing does the state recognize?
• Certified nurse practitioner • Certified nurse midwife • Certified registered nurse anesthetist • Certified nurse specialist
Total number of advanced practice nurses
• Certified nurse practitioners: 922 • Certified nurse midwives: 84 • Certified registered nurse anesthetists: 412 • Certified nurse specialists:154
Total: 1,572 Number of APNs with prescriptive authority
• Certified nurse practitioners: 922 • Certified nurse midwives: 84
Total: 1,006 All certified nurse practitioners and certified nurse midwives have prescriptive authority, but certified registered nurse anesthetists and certified nurse specialists do not have prescriptive authority.
Statutory and regulatory history
Maine has never had legislation on collaborative agreements, but a rule change in 1997 allowed APNs to practice independently. Graduates of nurse practitioner programs must practice for at least 24 months under the supervision of a physician or supervising nurse practitioner or be employed by a clinic or hospital with a physician medical director.
Does an APN need a separate certification to prescribe?
No.
What schedule drugs can APNs prescribe?
All certified nurse practitioners and certified nurse midwives are authorized to prescribe drugs related to their specialty area, including controlled substances schedules II-V.
Educational requirements for prescriptive authority
Certified nurse practitioners and certified nurse midwives who have not prescribed in the previous two years must complete 15 contact hours of pharmacology
Source: Maine State Board of Nursing

State Laws and Policies
Page 12
Montana What categories of advanced practice nursing does the state recognize?
• Nurse practitioner • Midwife • Anesthetist • Clinical specialist
Total number of advanced practice nurses
• Nurse practitioners: 468 • Midwives: 47 • Anesthetists: 185 • Clinical specialists: 41
Total: 741 Number of APNs with prescriptive authority
509 Montana does not track this statistic by type of advanced practice nurse.
Statutory and regulatory history
Montana has never required physician supervision or collaborative agreements.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
Montana Administrative Rules allow advanced practice nurses to prescribe "prescription drugs in the prevention of illness, the restoration of health, and/or the maintenance of health," including controlled substances schedules II-V.
Educational requirements for prescriptive authority
To obtain prescriptive authority, advanced practice nurses must complete 15 hours in pharmacology and/or the clinical management of drug therapy.
Source: Montana Board of Nursing

State Laws and Policies
Page 13
New Hampshire What categories of advanced practice nursing does the state recognize?
One category: advanced registered nurse practitioner
Total number of advanced practice nurses
1,350
Number of APNs with prescriptive authority
1,350
Statutory and regulatory history
New Hampshire advanced registered nurse practitioners have been allowed to practice independently since the 1980s, but until 1991 they could prescribe only under physician supervision. That year they were given independent prescriptive authority.
Does an APN need a separate certification to prescribe?
No.
What schedule drugs can APNs prescribe?
New Hampshire statute provides all advanced registered nurse practitioners with full prescriptive authority for controlled and non-controlled medications. However, a group known as the Joint Health Council produces an exclusionary formulary, which lists the drugs that advanced registered nurse practitioners cannot prescribe or can only prescribe within certain limitations.
Educational requirements for prescriptive authority
General advanced registered nurse practitioners certification requires completion of at least five hours in pharmacology.
Source: New Hampshire Board of Nursing

State Laws and Policies
Page 14
New Mexico What categories of advanced practice nursing does the state recognize?
• Certified nurse practitioners • Certified nurse specialists • Certified registered nurse anesthetists
Total number of advanced practice nurses
• Certified nurse practitioners: 710 • Certified nurse specialists: 146 • Certified registered nurse anesthetists: 199
Total:1,055 Number of APNs with prescriptive authority
The nursing board could not provide exact numbers of advanced practice nurses with prescriptive authority, but the associate director guessed that all nurse practitioners and certified registered nurse anesthetists have prescriptive authority, and about half of the certified nurse specialists have it.
Statutory and regulatory history
The New Mexico statute was changed in 1991 to establish independent practice for certified nurse practitioners, registered nurse anesthetists, and clinical nurse specialists. Nurse practitioners received the authority to prescribe controlled drugs in 1993. Clinical nurse specialists received that authority in 1997 and certified registered nurse anesthetists received it in 2001.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
All three categories can obtain authority to prescribe controlled substances, schedules II-V within their clinical specialty and practice setting.
Educational requirements for prescriptive authority
To be granted prescriptive authority, all APNs must complete 400 hours of work experience in which prescribing dangerous drugs has occurred within the two years prior to applying for prescriptive authority or 400 hours of prescribing in a preceptorship. In addition to the 400 hours, certified nurse specialists are required to complete a three-credit-hour pharmacology course, a three-credit-hour assessment course and a three-credit-hour pathophysiology course that are included as part of a graduate level advanced practice nursing education program.
Source: New Mexico Board of Nursing, New Mexico Legislative Council Service

State Laws and Policies
Page 15
Oregon What categories of advanced practice nursing does the state recognize?
• Nurse anesthetists • Clinical nurse specialists • Nurse practitioners (This category includes nurse
midwives.) Only nurse practitioners and clinical nurse specialists are granted prescriptive authority.
Total number of advanced practice nurses
• Nurse practitioners 2,150 • Certified registered nurse anesthetists: 440 • Clinical nurse specialists: 180
Total: 2,770 Number of APNs with prescriptive authority
• Nurse practitioners: 2,250 • Clinical nurse specialists: 12
Nurse anesthetists are not granted prescriptive authority. Statutory and regulatory history
Oregon has never had a collaborative agreement requirement. Clinical nurse specialists and nurse practitioners were granted prescriptive authority in 1979 for controlled drugs schedules III-V and in 2001 for schedule II.
Does an APN need a separate certification to prescribe?
Yes. Oregon Administrative Rules require all applicants for a nurse practitioner license to obtain prescribing authority.
What schedule drugs can APNs prescribe?
Schedules II-V
Educational requirements for prescriptive authority
For prescriptive authority, clinical nurse specialists and nurse practitioners must complete 45 contact hours of pharmacology and a directly supervised clinical practicum of at least 150 hours.
Source: Oregon State Board of Nursing

State Laws and Policies
Page 16
Utah What categories of advanced practice nursing does the state recognize?
Utah recognizes two types of advanced practice registered nurses:
• Advanced practice registered nurse • Advanced practice registered nurse-certified registered
nurse anesthetist
Total number of advanced practice nurses
• Advanced practice registered nurses: 1,209 • Advanced practice registered nurse-certified registered
nurse anesthetists: 398 Total: 1,607 Utah also licenses 131 certified nurse midwives, but does not consider these nurses to be advanced practice.
Number of APNs with prescriptive authority
• Advanced practice registered nurses: 1,147 • Advanced practice registered nurse-certified registered
nurse anesthetists: 0 (APRN-CRNAs do not have prescriptive authority. Instead, 189 of them are granted the authority to administer controlled substances.)
Total: 1,147 Additionally, five certified nurse midwives have prescriptive authority.
Statutory and regulatory history
Advanced practice registered nurses have had prescriptive authority for at least the last two decades. However, until about 13 years ago, they were required to prescribe controlled substances only in consultation with a physician. Since the law changed in 1995, advanced practice registered nurses have been allowed to prescribe controlled substances schedules IV and V without physician consultation. They still need a written physician consultation plan if they want to prescribe schedules II and III.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
Advanced practice registered nurses can independently prescribe schedules IV-V, and they can prescribe schedules II-III in accordance with a consultation and referral plan. "Consultation and referral plan" is defined as "a written plan jointly developed by an advanced practice registered nurse and a consulting physician."
Educational requirements for prescriptive authority
No additional requirement beyond those required for APRN licensing. Licensing requirements include three courses in diagnosis and treatment, patient assessment, and pharmacotherapeutics.
Source: Utah Division of Occupational and Professional Licensing

State Laws and Policies
Page 17
Washington State What categories of advanced practice nursing does the state recognize?
Washington recognizes advanced registered nurse practitioners (ARNPs) and designates 10 specialties, including certified registered nurse anesthetist and certified nurse midwife.
Total number of advanced practice nurses
• ARNP-acute care nurse practitioners: 43 • ARNP-adult nurse practitioners: 549 • ARNP-certified nurse midwifes: 345 • ARNP-certified registered nurse anesthetists: 683 • ARNP-family nurse practitioners: 1,709 • ARNP-geriatric nurse practitioners: 95 • ARNP neonatal nurse practitioners: 71 • ARNP-pediatric nurse practitioners: 248 • ARNP psychiatric mental health nurse practitioners: 496 • ARNP-women's health care nurse practitioners: 269
Total: 4,508 Number of APNs with prescriptive authority
1,413
Statutory and regulatory history
Washington first granted prescriptive authority in 1979. In 1988 the state began licensing advanced practice nurses, and in 1992 ARNPs obtained the ability to prescribe controlled substances. The statute was expanded in 2000 to allow ARNPs to prescribe schedule II drugs but only under a Joint Practice Agreement. The Joint Practice Agreement language was repealed by the legislature in 2007.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
Schedules II-V. Washington law specifically prohibits ARNPs from prescribing schedule I.
Educational requirements for prescriptive authority
Washington requires 30 contact hours of education in pharmacotherapeutics.
Source: Washington State Department of Health, Nursing Care Quality Assurance Commission

State Laws and Policies
Page 18
Washington D.C.
What categories of advanced practice nursing does the state recognize?
Four types of advanced practice nurse practitioners: • Nurse practitioner • Nurse anesthetist • Clinical nurse specialist • Nurse midwife
Total number of advanced practice nurses
• Nurse practitioners: 827 • Nurse anesthetists: 147 • Clinical nurse specialists: 46 • Nurse midwives: 81
Total: 1,101 Number of APNs with prescriptive authority
• Nurse practitioners: 827 • Nurse anesthetists: 147 • Clinical nurse specialists: 46 • Nurse midwives: 81
Total: 1,101 Statutory and regulatory history
Nurse anesthetists, certified nurse midwives, and nurse practitioners were first licensed as advanced practice nurse practitioners in 1984. Clinical nurse specialists were not included then because they were licensed and allowed to practice independently under another law. At that time, advanced practice nurses were required to practice in “collaboration” with physicians — direct, immediate, or general collaboration. They also were required to have a protocol agreement with a physician in order to prescribe. In 1994 that law was amended to included clinical nurse specialists and to allow advanced practice nurses to “perform actions of medical diagnosis, treatment, prescription.” It repealed the collaboration requirement. The District of Columbia now requires advanced practice nurses to “carry out acts of APRNs in collaboration with a licensed health care provider.” This does not require a collaboration agreement. It just requires APRNs to collaborate with other health professionals as appropriate in the course of their practice.
Does an APN need a separate certification to prescribe?
No.
What schedule drugs can APNs prescribe?
Schedules II-V
Educational requirements for prescriptive authority
In granting prescriptive authority, the District of Columbia does not require any additional education beyond that required for licensing.
Source: District of Columbia Board of Nursing
State Laws and Policies
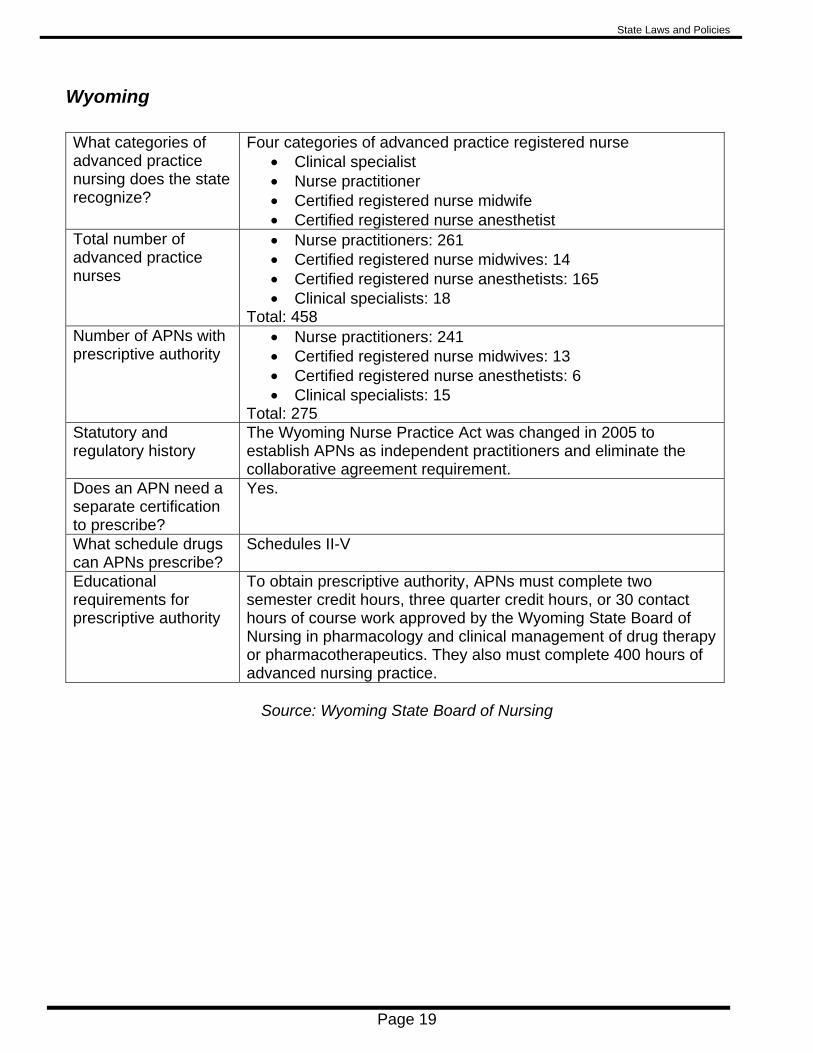
Page 19
Wyoming What categories of advanced practice nursing does the state recognize?
Four categories of advanced practice registered nurse • Clinical specialist • Nurse practitioner • Certified registered nurse midwife • Certified registered nurse anesthetist
Total number of advanced practice nurses
• Nurse practitioners: 261 • Certified registered nurse midwives: 14 • Certified registered nurse anesthetists: 165 • Clinical specialists: 18
Total: 458 Number of APNs with prescriptive authority
• Nurse practitioners: 241 • Certified registered nurse midwives: 13 • Certified registered nurse anesthetists: 6 • Clinical specialists: 15
Total: 275 Statutory and regulatory history
The Wyoming Nurse Practice Act was changed in 2005 to establish APNs as independent practitioners and eliminate the collaborative agreement requirement.
Does an APN need a separate certification to prescribe?
Yes.
What schedule drugs can APNs prescribe?
Schedules II-V
Educational requirements for prescriptive authority
To obtain prescriptive authority, APNs must complete two semester credit hours, three quarter credit hours, or 30 contact hours of course work approved by the Wyoming State Board of Nursing in pharmacology and clinical management of drug therapy or pharmacotherapeutics. They also must complete 400 hours of advanced nursing practice.
Source: Wyoming State Board of Nursing

State Laws and Policies
Page 20
Other States Three other states are considering or have recently considered a rule change or legislation to eliminate their collaborative agreement requirements. Vermont Since 1984, Vermont's administrative rules have required advanced practice registered nurses to have a collaborative agreement with a physician. (The state's laws do not address collaborative agreements.) Unlike in Arkansas, where APNs must have a collaborative agreement to prescribe, in Vermont, APRNs must have a collaborative agreement to be licensed as APRNs. The Vermont State Board of Nursing is currently trying to change its rules to eliminate the collaborative agreement requirement. The board, which anticipates opposition to the rule change, would like to eliminate the requirement for licensing and for prescriptive authority. Nebraska Nebraska law requires nurse practitioners who want to prescribe to have a written "integrated practice agreement" with a collaborating physician. The statute states that the nurse practitioner and the physician have "joint responsibility for patient care," and it gives the physician responsibility for the "supervision" of the nurse practitioner. The law defines supervision as "the ready availability of the collaborating physician for consultation and direction of the activities of the nurse practitioner." During the state's regular session earlier this year, the legislature considered a bill that would have eliminated the integrated practice requirement for nurse practitioners who have practiced as a nurse practitioner for at least five years. The bill did not pass and was "indefinitely postponed." New York New York law allows nurse practitioners to diagnose and treat patients "in collaboration with a licensed physician." It also requires nurse practitioners to have a "written practice agreement" and "written practice protocols." Any prescriptions written by the nurse practitioner must also be covered under the practice agreement and protocols. Two bills were introduced in the state's 2008 legislative session that would have eliminated the requirement that nurse practitioners collaborate with a physician. Both bills were sent to committees, where they remained through the session's end.

Page 21
Health Care Expenditures
Total Health Care Expenditures Per capita by state of residence, 2004
$5,080
$4,880
$4,863
$4,471
$4,444
$4,103
$3,972
$5,380
$5,283
$5,265
$5,092
$8,295$6,540
$6,450
$5,432
$3,000 $4,000 $5,000 $6,000 $7,000 $8,000 $9,000
UT
AZ
ID
NM
AR
OR
MN
WA
WY
U.S.
IA
NH
AK
ME
D.C.
Source: The Henry J. Kaiser Family Foundation, www.statehealthfacts.org

Health Care Expenditures
Page 22
Expenditures: Hospital Care Percent of each state's total health care expenditures, 2004
33.9%
34.3%
35.3%
35.7%36.1%
36.1%
37.1%37.7%
38.1%38.9%
39%40.2%
41.1%41.3%
49.2%
30 35 40 45 50
WA
OR
ME
NH
AZ
UT
ID
U.S.
AR
IA
MN
AK
WY
MT
D.C.
Source: The Henry J. Kaiser Family Foundation, www.statehealthfacts.org

Health Care Expenditures
Page 23
Expenditures: Physician and Other Professional Services Percent of each state's total health care expenditures, 2004
23.4%26.4%
26.9%27.7%
28.2%
28.2%
28.3%
28.3%28.3%
28.6%
29.6%32.7%32.8%
33%
33.4%
20 25 30 35
D.C.
NM
IA
ME
NH
U.S.
AR
MT
UT
ID
WY
AK
WA
AZ
OR
Source: The Henry J. Kaiser Family Foundation, www.statehealthfacts.org

Health Care Expenditures
Page 24
Expenditures: Drugs and Other Medical Nondurables Percent of each state's total health care expenditures, 2004
7.2%
9.9%
10.6%11.3%
11.7%12%
12.2%12.7%
13.3%13.5%
13.7%13.9%
14.3%14.5%
16.6%
5 10 15 20
D.C.
AK
MT
WY
OR
WA
ME
IA
NM
ID
NH
U.S.
AZ
AR
UT
Source: The Henry J. Kaiser Family Foundation, www.statehealthfacts.org

Page 25
Access to Health Care
Population Lacking Primary Care, 2007
This table shows the percent of the population living in an area designated by the U.S. Department of Health and Human Services (DHHS) as being underserved by primary care physicians in 2007. Primary care doctors include family or general practice physicians, internists, pediatricians, obstetricians, and gynecologists. An underserved area has a limited number of doctors for the population.
5.3%
5.9%6.4%
7.7%
9.1%
9.8%
10.6%11.1%
11.4%
13.1%
16.9%20.2%
20.5%
30%* N/A
0 5 10 15 20 25
NH
ME
OR
IA
WA
AR
AK
U.S.
UT
AZ
ID
MT
WY
NM
D.C.
Source: Health Care State Rankings 2008
*The Health Care State Rankings data did not include Washington D.C.

Access to Health Care
Page 26
Population Lacking Primary Care, 1992 - 2007 This table shows the percent of the population living in an area designated by the U.S. Department of Health and Human Services (DHHS) as being underserved by primary care physicians. Primary care doctors include family or general practice physicians, internists, pediatricians, obstetricians, and gynecologists. An underserved area has a limited number of doctors for the population. Data on this measure for 1997 was not included in the Health Care State Rankings series.
0
5
10
15
20
25
30
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
U.S.
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
Source: Health Care State Rankings series *The Health Care State Rankings data did not include Washington D.C.

Access to Health Care
Page 27
Rate of Physicians in Primary Care, 2006 Total primary care physicians per 100,000 population
7071
76
7682
84
91
9799
104
104
105
107
109
243
50 100 150 200
ID
IA
UT
AZ
AR
WY
MT
NM
U.S.
NH
AK
WA
OR
ME
*D.C.
Source: Health Care State Rankings 2008
*The Health Care State Rankings data did not include Washington D.C. Instead, the rate for the District of
Columbia was calculated by using data from the American Medical Association and the U.S. Census Bureau.

Access to Health Care
Page 28
Rate of Physicians in Primary Care, 1992 - 2006 Total primary care physicians per 100,000 population
50
60
70
80
90
100
110
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
U.S.
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
Source: Health Care State Rankings series
*The Health Care State Rankings data did not include Washington D.C.
Access to Health Care
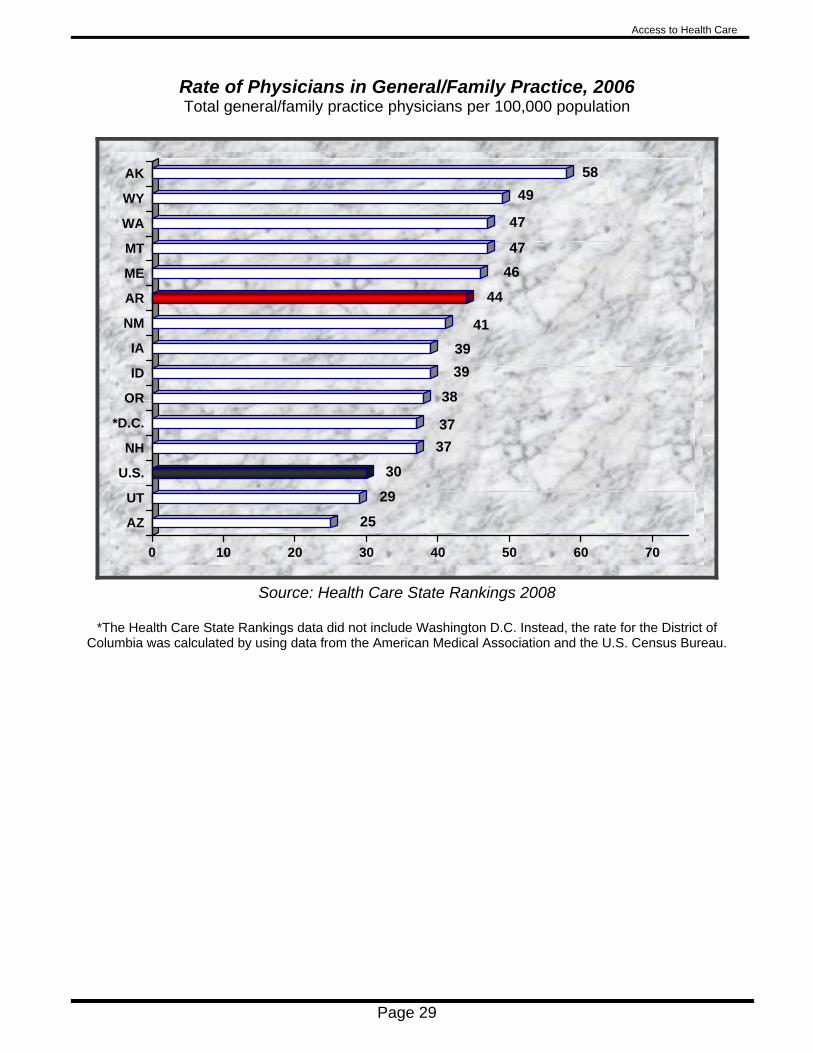
Page 29
Rate of Physicians in General/Family Practice, 2006 Total general/family practice physicians per 100,000 population
25
29
30
3737
38
3939
41
44
4647
47
4958
0 10 20 30 40 50 60 70
AZ
UT
U.S.
NH
*D.C.
OR
ID
IA
NM
AR
ME
MT
WA
WY
AK
Source: Health Care State Rankings 2008
*The Health Care State Rankings data did not include Washington D.C. Instead, the rate for the District of
Columbia was calculated by using data from the American Medical Association and the U.S. Census Bureau.

Access to Health Care
Page 30
Rate of Physicians in General/Family Practice, 1992 - 2006 Total general/family practice physicians per 100,000 population
20
25
30
35
40
45
50
55
60
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
U.S.
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
Source: Health Care State Rankings series
*The Health Care State Rankings data did not include Washington D.C.
Access to Health Care
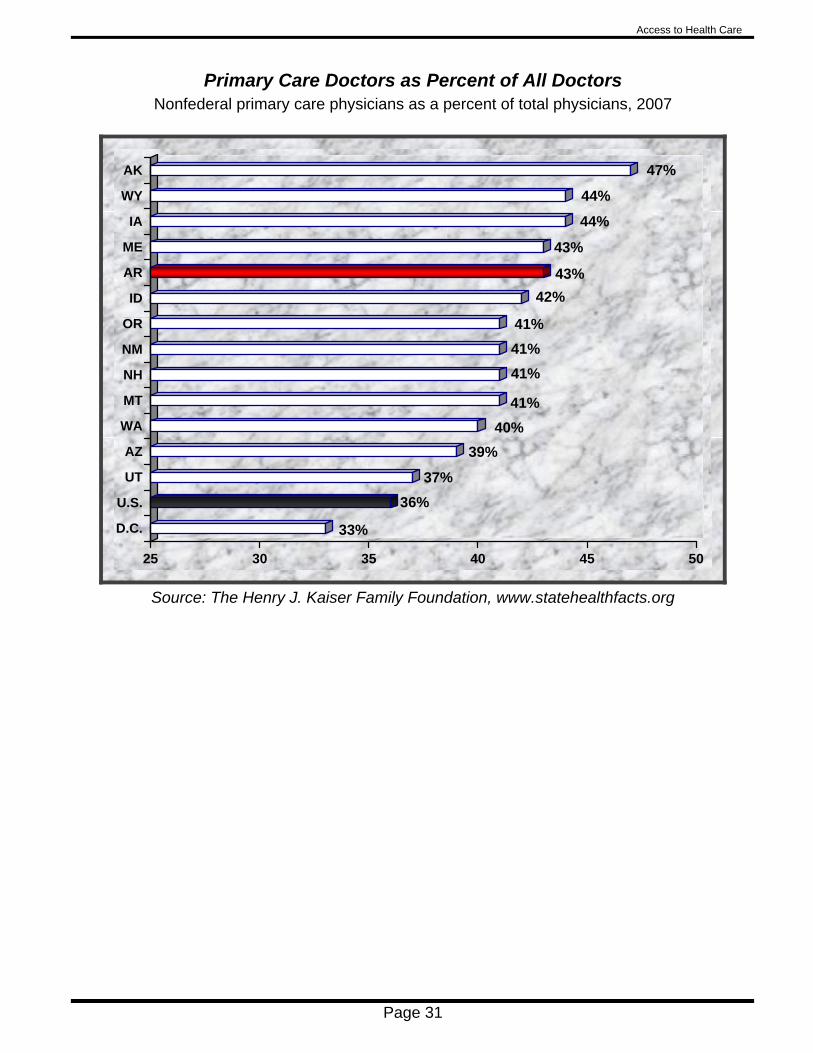
Page 31
Primary Care Doctors as Percent of All Doctors Nonfederal primary care physicians as a percent of total physicians, 2007
33%
36%37%
39%40%
41%
41%41%41%
42%43%
43%
44%
44%
47%
25 30 35 40 45 50
D.C.
U.S.
UT
AZ
WA
MT
NH
NM
OR
ID
AR
ME
IA
WY
AK
Source: The Henry J. Kaiser Family Foundation, www.statehealthfacts.org

Access to Health Care
Page 32
Rate of Advanced Practice Nurses Total per 100,000 population, 2008
51.2
53.6
61.2
61.364.9
65.7
72.673.9
77.4
87.6
102.6
119.3
119.7187.2
50 100 150 200
AR
NM
IA
AZ
ID
UT
WA
OR
MT
WY
NH
ME
AK
D.C.
Source: Each state's board of nursing provided the number of advanced practice nurses it licenses. Population
information came from the U.S. Census Bureau's July 1, 2007 population estimates. There is no national average for the number of advanced practice nurses per 100,000 population because no national organization
systematically collects and analyzes reliable data.
State APNs Population Alaska 818 683,478 Arizona 3,885* 6,338,755 Arkansas 1,451 2,834,797 Idaho 973 1,499,402 Iowa 1,830 2,988,046 Maine 1,572 1,317,207 Montana 741 957,861 New Hampshire 1,350 1,315,828 New Mexico 1,055 1,969,915 Oregon 2,770 3,747,455 Utah 1,738** 2,645,330 Washington 4,508 6,468,424 Washington D.C. 1,101 588,292 Wyoming 458 522,830
* The Arizona number includes 557 certified registered nurse anesthetists, though the state does not recognize them as advanced practice.
** The Utah number includes 131 certified nurse midwives, though the state does not recognize them as advanced practice.
Access to Health Care
Page 33
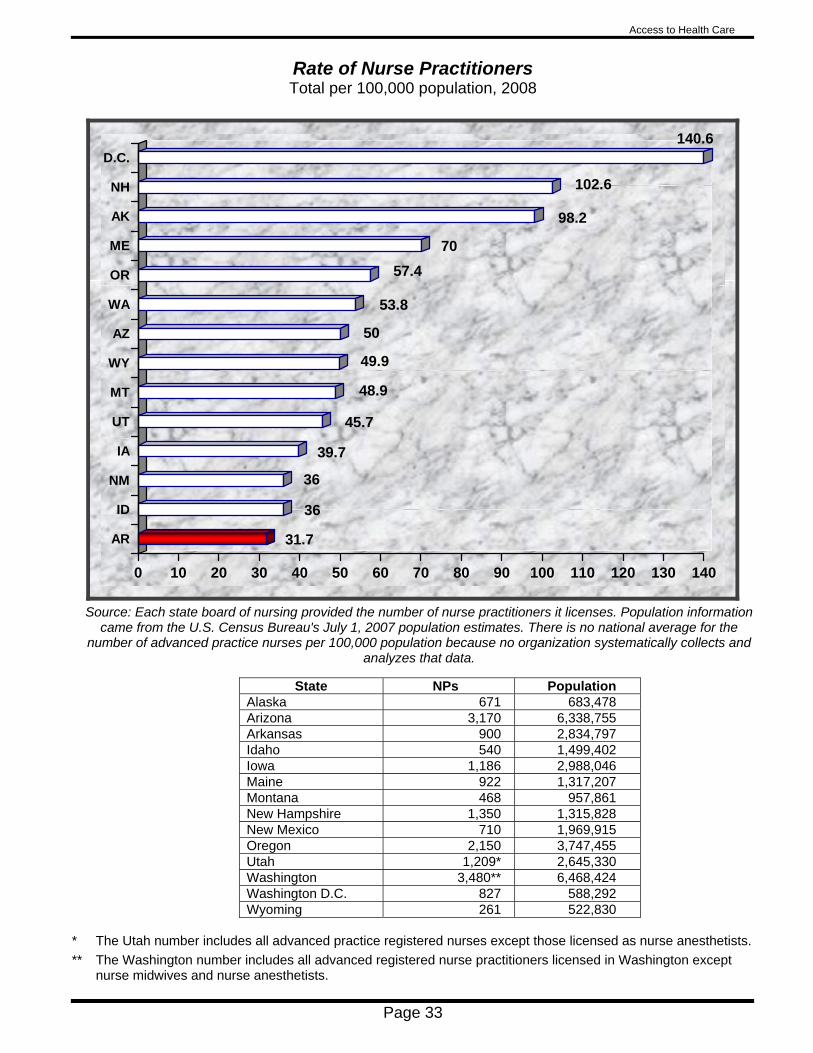
Rate of Nurse Practitioners Total per 100,000 population, 2008
31.7
36
36
39.7
45.7
48.9
49.9
50
53.8
57.470
98.2
102.6
140.6
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140
AR
ID
NM
IA
UT
MT
WY
AZ
WA
OR
ME
AK
NH
D.C.
Source: Each state board of nursing provided the number of nurse practitioners it licenses. Population information
came from the U.S. Census Bureau's July 1, 2007 population estimates. There is no national average for the number of advanced practice nurses per 100,000 population because no organization systematically collects and
analyzes that data.
State NPs Population Alaska 671 683,478 Arizona 3,170 6,338,755 Arkansas 900 2,834,797 Idaho 540 1,499,402 Iowa 1,186 2,988,046 Maine 922 1,317,207 Montana 468 957,861 New Hampshire 1,350 1,315,828 New Mexico 710 1,969,915 Oregon 2,150 3,747,455 Utah 1,209* 2,645,330 Washington 3,480** 6,468,424 Washington D.C. 827 588,292 Wyoming 261 522,830
* The Utah number includes all advanced practice registered nurses except those licensed as nurse anesthetists. ** The Washington number includes all advanced registered nurse practitioners licensed in Washington except
nurse midwives and nurse anesthetists.

Access to Health Care
Page 34
Arkansas's Medically Underserved Areas The U.S. Department of Health and Human Services Health Resources and Services Administration identified these areas of Arkansas as being medically underserved. Areas are designated as medically underserved based on four criteria: the ratio of primary care physicians per 1,000 population, the infant mortality rate, the percentage of the population with incomes below the poverty level, and percentage of the population age 65 or over. The term "primary care physicians" refers to family and general practice doctors, internists, pediatricians, obstetricians, and gynecologists.

Access to Health Care
Page 35
Area Health Education Centers Seven of the 12 UAMS Area Health Education Center locations operate medical clinics and family medicine residency programs. The two AHEC locations in the north central region and the three locations in the Delta region do not have clinics.
Source: UAMS Area Health Education Centers Annual Report August 2008
http://www.uams.edu/AHEC/Reports/AHECAnnualReport.pdf

Access to Health Care
Page 36
Community Health Centers of Arkansas Federally funded community health centers provide primary medical, dental, mental health and preventive health care services on a sliding-fee scale. The community health centers serve medically underserved areas. Arkansas currently has community health center sites in 59 communities.
Source: Community Health Centers of Arkansas http://www.chc-ar.org/health_maps_intro.html

Access to Health Care
Page 37
Family and General Practice Physicians per 10,000 Population

Access to Health Care
Page 38
Nurse Practitioners with Prescriptive Authority per 10,000 Population

Access to Health Care
Page 39
Adverse Actions for Advanced Practice Nurses This table shows the number of adverse actions taken against advanced practice nurses as reported to the federal National Practioner Data Bank (NPDB) and the Health Integrity and Protection Data Bank (HIPDB). Adverse actions include payments made to settle malpractice claims, any disciplinary measure taken by a state licensing board, and any hospital termination. The NPDB and the HIPDB did not provide a national average, but the national totals are provided along the top of the chart. It is important to note that one incident could result in multiple actions. For example, an egregious malpractice incident could result in a malpractice settlement payment and the termination of the nurse's license. It should also be noted that the numbers of adverse actions in each state are very small, making annual decreases or increases appear more significant. Since 1995, the Arkansas State Board of Nursing has taken just 17 licensure actions against advanced practice nurses.
U.S. 2003 2004 2005 2006 2007 275 327 382 355 625
0
5
10
15
20
25
30
2003 2004 2005 2006 2007
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
DC
Source: National Practitioner Data Bank and Healthcare Integrity and Protection Data Bank

Access to Health Care
Page 40
Adverse Actions in States That Repealed Collaborative Agreement Requirements The following tables show the number of adverse actions reported against advanced practice nurses in the states that had a collaborative agreement requirement, but repealed it. The large red square in each graph indicates the year in which the repeal occurred. Alaska, which repealed its collaborative agreement requirement in 1984, was excluded because the Data Banks only began collecting adverse action data in 1991. The state of Washington was also excluded because it repealed its collaborative agreement requirement in 2007 and there is no adverse action data available beyond 2007.
Idaho
0
1
2
3
4
5
6
7
8
9
10
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007

Access to Health Care
Page 41
New Hampshire
0
1
2
3
4
5
6
7
8
9
10
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Utah
0123456789
101112131415
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007

Access to Health Care
Page 42
Washington D.C.28
0
1
2
3
4
5
6
7
8
9
10
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Wyoming
0
1
2
3
4
5
6
7
8
9
10
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007

Access to Health Care
Page 43
Hospital Emergency Room Visits
Total visits per 1,000 population
250
275
300
325
350
375
400
425
450
475
500
525
550
575
600
625
650
675
700
1999 2000 2001 2002 2003 2004 2005 2006
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
D.C.
U.S.
Source: The Henry J. Kaiser Family Foundation, www.statehealthfacts.org

Page 44
State Health Indicators
State Health Ranking This table shows the ranking of the states each year from the UnitedHealth Foundation's annual America's Health Ranking report. The Foundation examines each state based on about 20 health indicators, such as the smoking rate, the percentage of people who are uninsured, and the infant mortality rate. The healthiest state ranks 1st, and the least healthy state ranks 50th.
0
5
10
15
20
25
30
35
40
45
50
2001 2002 2003 2004 2005 2006 2007
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
Source: UnitedHealth Foundation. The Foundation's annual state health rankings do not include Washington D.C.

State Health Indicators
Page 45
Teen Births Number of births per 1,000 females ages 15 to 19
0
25
50
75
2001 2002 2003 2004 2005
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
D.C.
U.S.
Source: Annie E. Casey Foundation, Kids Count Data Center

State Health Indicators
Page 46
Births to Women Receiving Late or No Prenatal Care Percent of births to mothers who received prenatal care only in the third trimester of their pregnancy or no prenatal care
Source: Annie E. Casey Foundation, Kids Count Data Center
0
1
2
3
4
5
6
7
8
9
10
2001 2002 2003 2004 2005
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
D.C.
U.S.

State Health Indicators
Page 47
Low Birth Weight Babies Percent of babies born who weighed less than 5.5 pounds
5
6
7
8
9
10
2001 2002 2003 2004 2005
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
D.C.
U.S.
Source: Annie E. Casey Foundation, Kids Count Data Center

State Health Indicators
Page 48
Infant Mortality Deaths occurring to infants under 1 year of age per 1,000 live births
3
4
5
6
7
8
9
10
2001 2002 2003 2004 2005
AK
AZ
AR
ID
IA
ME
MT
NH
NM
OR
UT
WA
WY
D.C.
U.S.
Source: Annie E. Casey Foundation, Kids Count Data Center

State Health Indicators
Page 49
Heart Disease Deaths Deaths per 100,000 population, 2005
162.6
162.6
164.7
169.4
174.3177.9
179.4
182.7
184.5
185
186.9
191.4211.1
249.5
268.2
150 175 200 225 250 275
AK
UT
OR
MT
WA
ID
NH
ME
NM
AZ
WY
IA
U.S.
AR
D.C.
Source: Annie E. Casey Foundation, Kids Count Data Center