advanced concepts the burning belly: an overview of gerd
TRANSCRIPT

7/23/2021
1
Advanced Concepts The Burning Belly: An Overview of GERD, Dyspepsia and Eosinophilic EsophagitisJason Domagalski, MD, FAAFP
Residency Director
Froedtert Menomonee Falls Hospital Family Medicine Residency
Activity DisclaimerThe material presented here is being made available by the American Academy of Family Physicians
for educational purposes only. Please note that medical information is constantly changing; the
information contained in this activity was accurate at the time of publication. This material is not
intended to represent the only, nor necessarily best, methods or procedures appropriate for the
medical situations discussed. Rather, it is intended to present an approach, view, statement, or
opinion of the faculty, which may be helpful to others who face similar situations.
The AAFP disclaims any and all liability for injury or other damages resulting to any individual using
this material and for all claims that might arise out of the use of the techniques demonstrated therein
by such individuals, whether these claims shall be asserted by a physician or any other person.
Physicians may care to check specific details such as drug doses and contraindications, etc., in
standard sources prior to clinical application. This material might contain recommendations/guidelines
developed by other organizations. Please note that although these guidelines might be included, this
does not necessarily imply the endorsement by the AAFP.
1
2

7/23/2021
2
Disclosure StatementIt is the policy of the AAFP that all individuals in a position to control content disclose any relationships with commercial interests upon nomination/invitation of participation. Disclosure documents are reviewed for potential conflicts of interest. If conflicts are identified, they are resolved prior to confirmation of participation. Only participants who have no conflict of interest or who agree to an identified resolution process prior to their participation were involved in this CME activity.
All individuals in a position to control content for this session have indicated they have no relevant financial relationships to disclose.
Learning Objectives
1. Identify the recommended treatment strategies to cost effectively management of GERD, dyspepsia and eosinophillic esophagitis.
2. Consider common strategies to address complicated cases and when to to consider surgical and endoscopic interventions.
3. Review the known complications associated with long-term PPI use and effective strategies of weaning patients off these medications.
3
4

7/23/2021
3
Say Hello to Tom
AES Question
5
6

7/23/2021
4
Question 1
Mr. Bernie Belly is a 41 year-old male who has chronic epigastric pain and found to have H. pylori infection which has failed to respond to clarithromycin based triple therapy. Which of the following is an appropriate next step in treatment?
A. Repeat the same triple therapy again
B. PPI+Bismuth+Metronidazole+Tetracycline
C. Antibiotic Sensitivity Testing
D. Rifabutin based therapy
Helicobacter pylori
One of the most common infections worldwide
Known carcinogen Associated with noncardia gastric adenocarcinoma
1-3% infected develop cancer
15% of total cancers worldwide 89% of gastric cancers
Linked to Peptic Ulcer Disease
7
8

7/23/2021
5
Refractory Infection
Positive test 4+ weeks after course completion
Multifactorial Etiologies Non-adherence Antibiotic Resistance
Shah S, et al. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastro. Apr 2021:.160 (5).
9
10

7/23/2021
6
Failure Recommendations
Shah S, et al. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastro. Apr 2021:.160 (5).
Shah S, et al. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastro. Apr 2021:.160 (5).
11
12
7/23/2021
7
AES Question
Question 2
Mrs. Anita Refill is a 42 year-old female who has been on the same dose of omeprazole for years presents for a routine physical and asks for a refill. When is long-term PPI use appropriate?
A. Patients with Barrett's esophagus
B. Patients with a history of PUD no longer taking NSAIDs
C. Patients with a history of eosinophilic esophagitis
D. Patients with B12 deficiency
13
14

7/23/2021
8
AGA Best Practice Recommendations
Patients with Erosive esophagitis or peptic strictures should should take PPIs for short term healing and long term symptom control Patients with Barrett’s esophagus and symptomatic GERD should
take a long-term PPI. Asymptomatic patients with Barrett’s esophagus should consider a
long-term PPI. Patients at high risk for ulcer-related bleeding from NSAIDs should
take a PPI if they continue to take NSAIDs. The dose of long-term PPIs should be periodically reevaluated so
that the lowest effective PPI dose can be prescribed to manage the condition.
PPI Problems
Hypomagnesemia
B12 Deficiency
Hip fractures
C. difficile infections
Community Acquired Pneumonia
Dementia Association?
Anderson WD, Strayer, SM, et al. Common Questions About the Management of Gastroesophageal Reflux Disease. Amer Fam Phys. 2015 May 15; 91(10): 692‐697El‐Serag HB, et al. Update on the epidemiology of gastroesophageal reflux disease: a systematic review. Gut. Jun 2014; 63(6):871‐880.
15
16

7/23/2021
9
Tapering Protocol
No standardized or evidence proven approach
Try reducing dose 50% every other day for 1 week
Then reduce daily dose by 50% for 1 week
Then reduce dosing to every other day for 1 week
Then Stop
Can try taking daily dose with biggest meal
Alternate with H2 blocker
Farell B, et al. Deprescribing proton pump inhibitors. Can Fam Phys. May 2017. 63 (5): 354-64.
17
18

7/23/2021
10
AES Question
Question 3
Mrs. Mia Chestahertz is a 37 year old female who presents with classic GERD symptoms, but had a recently normal EGD. Which is a NOT a recommended treatment for Functional Heartburn?
A. Proton Pump Inhibitors
B. H2 receptor antagonists
C. Nortriptyline
D. Sertraline
19
20
7/23/2021
11
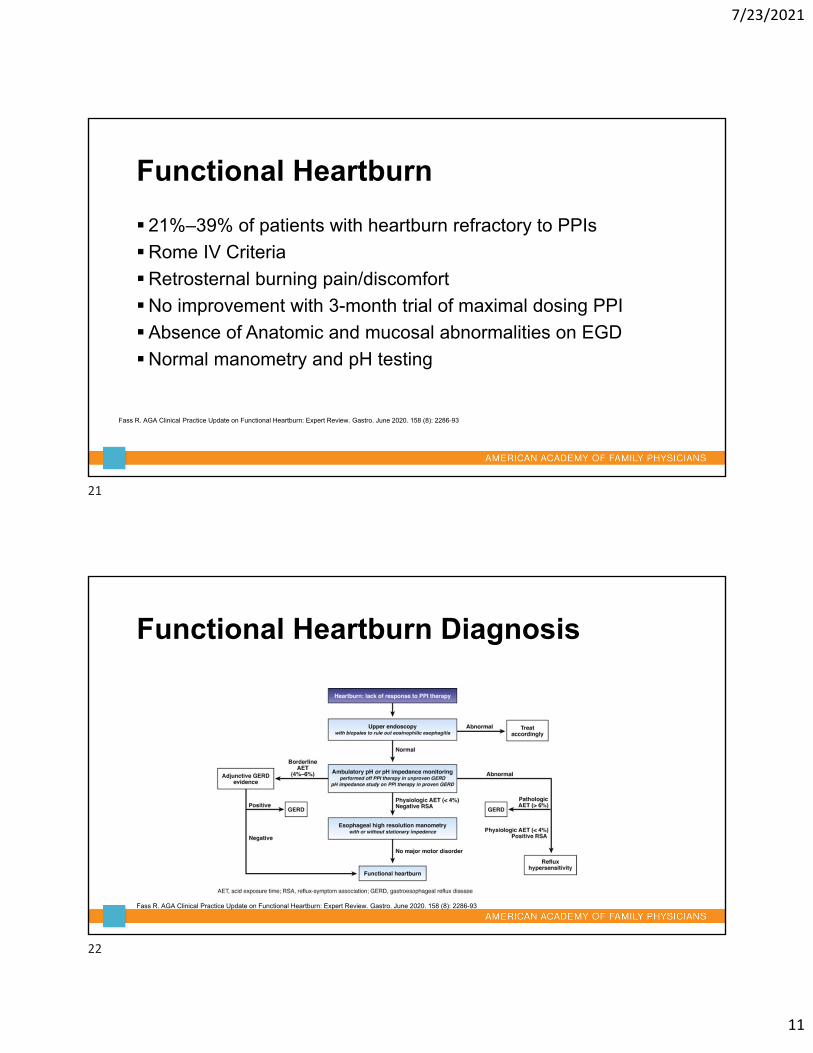
Functional Heartburn
21%–39% of patients with heartburn refractory to PPIs
Rome IV Criteria
Retrosternal burning pain/discomfort
No improvement with 3-month trial of maximal dosing PPI
Absence of Anatomic and mucosal abnormalities on EGD
Normal manometry and pH testing
Fass R. AGA Clinical Practice Update on Functional Heartburn: Expert Review. Gastro. June 2020. 158 (8): 2286-93
Functional Heartburn Diagnosis
Fass R. AGA Clinical Practice Update on Functional Heartburn: Expert Review. Gastro. June 2020. 158 (8): 2286-93
21
22

7/23/2021
12
Functional Heartburn Treatment
PPIs have no therapeutic value
TCAs, SSRIs and H2 antagonists proven benefit
Acupuncture and hypnotherapy have limited evidence
Anti-reflux surgery have no therapeutic benefit
Fass R. AGA Clinical Practice Update on Functional Heartburn: Expert Review. Gastro. June 2020. 158 (8): 2286-93
Functional Heartburn Therapeutics
Fass R. AGA Clinical Practice Update on Functional Heartburn: Expert Review. Gastro. June 2020. 158 (8): 2286-93
23
24
7/23/2021
13
AES Question
Question 4Mr. Max Doses is a 52 year-old male who has chronic GERD which has only partially responded to medications in the past. He is interested in additional treatments for his reflux. Which of the following is true in regards to patients with chronic GERD?A. 25% fail aggressive medical therapy
B. 40% fail aggressive medical therapy
C. Nissen Fundoplication is the only interventional procedure for chronic GERD
D. Up to 15% of patients with medication refractory GERD pursue fundoplication
25
26

7/23/2021
14
Treatment Gap 40% Fail aggressive medical therapy 5% undergo fundoplication
Fear of complications or treatment failure
Alternative treatment LINX EndoStim Stretta Medigus
Subramanian CR, Triadafilopoulos. Refractory Gastroesophageal Reflux Disease. Gastroenterology Report 3. 2014 Sep 30; 41‐53.
LINXSmall ring of magnetic beads
Augment LES function
Allows preserved belching/vomiting
Reduced ppi use at 4 wks
100% improved QOL at 4 yrs 80% cessation of PPI use
Subramanian CR, Triadafilopoulos. Refractory Gastroesophageal Reflux Disease. Gastroenterology Report 3. 2014 Sep 30; 41‐53.Permision Granted for reproduction by http://www.linxforlife.com. Accessed on May 30, 2015
27
28

7/23/2021
15
EndoStim Implantable Electrical stimulator
Increases resting pressure of LES
91% off ppi at 6 months
Reduced nocturnal heartburn symptoms
Subramanian CR, Triadafilopoulos. Refractory Gastroesophageal Reflux Disease. Gastroenterology Report 3. 2014 Sep 30; 41‐53.
StrettaRadiofrequency to remodel EGJ and LES
32 clinical trials and meta-analysis
Allows future interventions if needed
Subramanian CR, Triadafilopoulos. Refractory Gastroesophageal Reflux Disease. Gastroenterology Report 3. 2014 Sep 30; 41‐53.Permission granted for reproduction from http://www.stretta‐therapy.com. Accessed on May 30, 2015
29
30

7/23/2021
16
Endoscopic partial fundoplicationEndoscopic surgical
stapler64% reduction in GERD
patient scores Still in clinical trials
Medigus
Subramanian CR, Triadafilopoulos. Refractory Gastroesophageal Reflux Disease. Gastroenterology Report 3. 2014 Sep 30; 41‐53.Permission granted for reproduction from http://www.medigus.com. Accessed on May 30, 2015
AES Question
31
32

7/23/2021
17
Question 5
Mr. Hye Risk is a 36 year-old male with a history of Barrett’s Esophagus. He was found to have no dysplasia on his most recent surveillance EGD. When should his next EGD be scheduled?
A. 1-2 years
B. 3-5 years
C. 7-10 years
D. Never. No follow up is needed
Barrett’s Esophagus
Metaplastic columnar epithelium in lower esophagus
Predisposes cancer development
Annual incidence of esophageal cancer is 0.5% per year
Potentially increased risk of CV mortality
33
34
7/23/2021
18
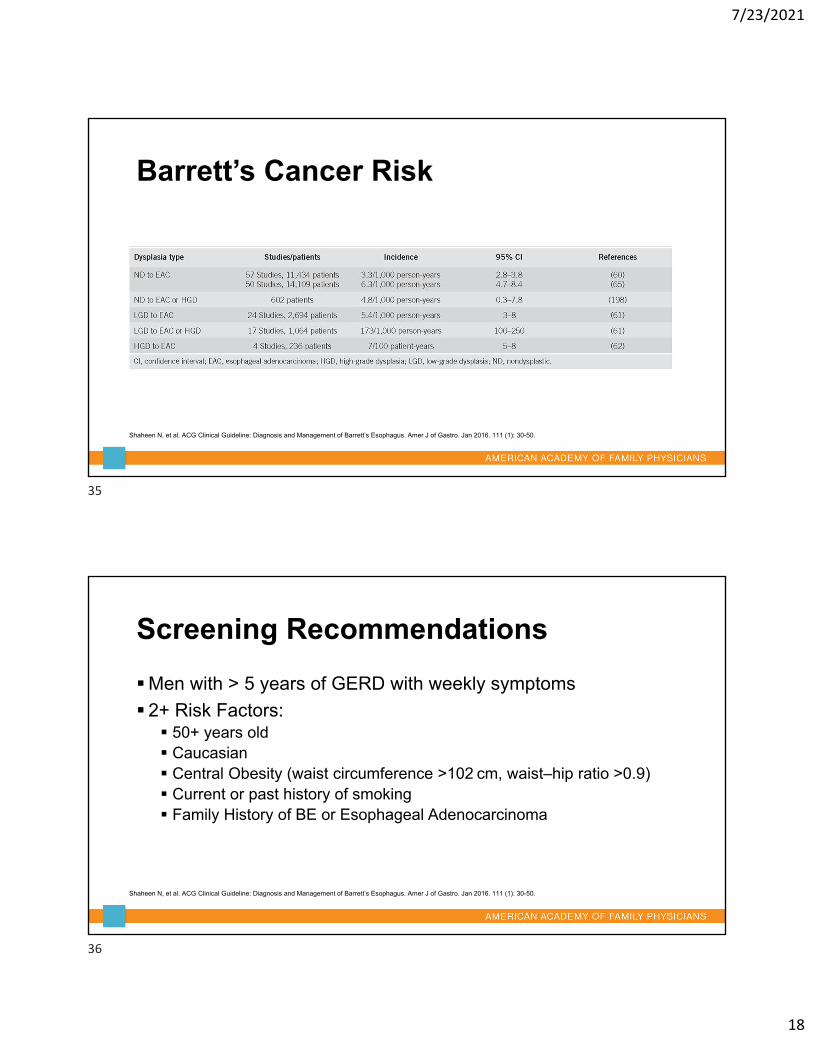
Barrett’s Cancer Risk
Shaheen N, et al. ACG Clinical Guideline: Diagnosis and Management of Barrett’s Esophagus. Amer J of Gastro. Jan 2016. 111 (1): 30-50.
Screening Recommendations
Men with > 5 years of GERD with weekly symptoms
2+ Risk Factors: 50+ years old Caucasian Central Obesity (waist circumference >102 cm, waist–hip ratio >0.9) Current or past history of smoking Family History of BE or Esophageal Adenocarcinoma
Shaheen N, et al. ACG Clinical Guideline: Diagnosis and Management of Barrett’s Esophagus. Amer J of Gastro. Jan 2016. 111 (1): 30-50.
35
36

7/23/2021
19
Surveillance Recommendations
No Dysplasia: 3-5 years 4 quadrant biopsies every 2 cm
Low Grade Dysplasia: 6-12 months
High Grade Dysplasia without intervention 3 months 4 quadrant biopsies every 1 cm
37
38

7/23/2021
20
Barrett’s Management
Acid Suppression No evidence to date for long term prevention of progression No evidence for doses greater than standard dosing
Chemoprevention Aspirin Not recommended for cancer prevention
Dysplasia Radiofrequency Ablation Photodynamic Therapy Endoscopic Mucosal Resection
Shaheen N, et al. ACG Clinical Guideline: Diagnosis and Management of Barrett’s Esophagus. Amer J of Gastro. Jan 2016. 111 (1): 30-50.
AES Question
39
40

7/23/2021
21
Question 6
Mr. M. Paction is a 34 year-old male with a history of Eosinophilic Esophagitis (EoE) with multiple ER visits for food impaction. Which of the following is true in regards to the management of EoE?
A. Dilation leads to symptom improvement in >80% of patients
B. There is a 5 % risk of perforation with dilation
C. Severe hemorrhage occurs in 1% of dilations
D. Dilation is higher risk for EoE than other strictures
EoE Management
Elemental Diets resolve inflammation in > 90% of children Poor compliance: taste, oral motor skills, potential gastrostomy tube
6 food Elimination Diet Resolves inflammation in 2/3 of patients Egg, wheat, milk, nuts, soy, fish and shellfish
Allergy Test guided restriction Resolves inflammation in 1/3 of patients
41
42

7/23/2021
22
Medication Management
PPIs resolve inflammation in 1/3 of patients
Topical Steroids Resolve inflammation in 2/3 of patients Risks: fungal/viral infections, adrenal suppression
Oral Steroids Similar to topical Adverse effects in 40%
Biologics No benefit
EoE Dysphagia Management
Caused by strictures
Symptom improvement in 87% of patients
Complications Perforation 0.4% Hemorrhage 0.1% Similar to other benign stricture dilation
Hirano I, et al. AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters Clinical Guidelines for the Management of Eosinophilic Esophagitis. Gastro. May 2020. 158 (6):1776-86.
43
44

7/23/2021
23
Practice Recommendations
The dose of long-term PPIs should be periodically reevaluated so that the lowest effective PPI dose can be prescribed to manage the condition. (SORT: C)
Bismuth based quadruple therapy should be considered for treatment refractory H. pylori. (SORT: B)
In patients with EoE topical steroids should be used rather than oral steroids(SORT: B)
References1. Subramanian CR, Triadafilopoulos. Refractory Gastroesophageal Reflux Disease. Gastroenterology Report 3. 2014 Sep 30; 41‐53.
2. Loyd RA, McClellan DA. Update on the Evaluation and Management of Functional Dyspepsia. Amer Fam Phys. 2011 March 1. 83(5): 547‐52.
3. Talley NJ, Vakil N. Guidelines for the Management of Dyspepsia. Amer J of Gastro. 2005: 2324‐35.
4. Anderson WD, Strayer SM, et al. Common Questions about the Management of Gastroesophageal Reflux Disease. Amer Fam Phys. 2015 May 15. 91(10): 692‐97.
5. Hirano I, et al. AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters Clinical Guidelines for the Management of Eosinophilic Esophagitis. Gastro. May 2020. 158 (6):1776-86.
45
46


7/23/2021
25
49