adrenal tumors
TRANSCRIPT
ADRENAL MASSES
PREPARED BY :DR.TALAL BALLOUTSUPERVISED BY:DR.WALED ZALLOUM

ANATOMY
-The right and left adrenal glands are located within Gerota fascia at the levels of the 11th and 12th ribs.
- The right adrenal is bounded medially by the inferior vena cava and anteriorly by the liver, while the left adrenal gland is bounded medially by the aorta and anteriorly by the stomach, pancreas, and splenic vessels.
-The arterial supply of each adrenal gland may arise from three main sources: superior adrenal arteries (branches from the inferior phrenic arteries), middle adrenal arteries (direct visceral branches from the aorta), and inferior adrenal arteries (branches from the ipsilateral renal artery.
- The short right adrenal vein drains directly into the vena cava. On the left, the adrenal vein is
long compared with the right and is joined by the inferior phrenic vein prior to draining into the left renal vein.
HISTOLOGY
Each adrenal gland is enclosed within a fibrous capsule Directly beneath the capsule is the cortex, which comprises three zones:
-zona glomerulosa. - zona fasciculata.-zona reticularis.

-The essential function of the glomerulosa is the production of mineralocorticoids, predominantly aldosterone.
-zona fasciculata responsible for the production
of glucocorticoids such as cortisol.-The zona reticularis, the inner mostlayer of the cortex, predominantly produces
sex steroids, such as adrenal estrogens and androgens .
The medulla secretes epinephrine (80%), norepinephrine(19%), and dopamine (1%).
ADRENAL DISORDERS
Disorders of Increased Adrenal Function Cushing Syndrome-Hypercortisolism secondary toexcessive production of
glucocorticoids by the adrenal cortex is defined as Cushing syndrome.
-The zona fasciculata of the adrenal cortex secretes more than 20 mg of cortisol every day . Regulation of this secretion is controlled through the hypothalamicpituitary-adrenal (HPA) axis.
Causes of Cushing syndrome can be divided intothree main groups: (1) exogenous, (2) ACTH-dependent,and (3) ACTH-independent.

ACTH-DEPENDENT CUSHING SYNDROME-Most cases (80%) are due to bilateral adrenocortical
hyperplasia stimulated by overproduction of pituitary adrenocorticotropic hormone (corticotropin, ACTH), known as Cushing’s disease.
-10% of cases are due to the ectopic production of ACTH from nonpituitary tumors. Ectopic ACTH production occurs most frequently in small-cell lung carcinoma; other tumors producing ACTH include carcinoids (lung, thymic, gastrointestinal tract), islet cell tumors of the pancreas, medullary thyroid carcinoma, pheochromocytoma,and small-cell carcinoma of the prostate.
-Adrenal adenoma is the cause in 5% of cases and carcinoma
in 5%.

CLINICAL FINDINGS OF CUSHING SYNDROME
1. Obesity (with sparing of the extremities), moon face, and fat pads of the supraclavicular and dorsocervical areas (buffalo hump).
2. Striae (red and depressed) over the abdomen and thighs.3. Hypertension (almost always present).4. Proximal myopathy with marked weakness, especiallyin the quadriceps femoris, making unaided rising from a chair
difficult.5. Emotional lability, irritability, difficulty in sleeping,and sometimes psychotic personality.6. Osteoporosis (common), with back pain from compressionfractures of the lumbar vertebrae as well as rib fractures.7. In 80% of cases, postprandial hyperglycemia ispresent, and in 20% there is an elevated fasting plasma glucose
level.

-Blood chemical analyses may show an increase inserum Na+ and CO2 levels and a decrease in serum K+levels. Hyperglycemia may occur.1. Specific tests for Cushing’s syndromea. 24-hour urinary cortisol level—Urine cortisol ismeasured in a 24-hour urine collection (normal range,
10–50 μg/24 h). A urine cortisol value more than twofold
elevated is typical of Cushing’s syndrome. False-positive elevations can occur in acute illness, depression, and alcoholism.
b. Suppression of ACTH and plasma cortisol bydexamethasone—Dexamethasone in low doses is used to
assess the feedback suppression of ACTH and cortisol production by glucocorticoids.
The procedure is to give 1 mg of dexamethasone by mouth at 11 pm and to draw blood at 8–9:00 am for measurement of plasma cortisol. If the level is <5 μg/dL (normal is 5–20 mg/dL), Cushing’s syndrome can be ruled out. If the value is >10 μg/dL, Cushing’s syndrome is present.
2. Specific tests for differentiation of causes of
Cushing’s syndromea. Plasma ACTH level b. Plasma androgen
levels
TREATMENT
A. CUSHING’S DISEASEA pituitary microadenoma, which is the
most common cause of bilateral adrenocortical hyperplasia, must be located and removed surgically. Transsphenoidal resection.
THE HYPERTENSIVE, HYPOKALEMICSYNDROME (PRIMARYALDOSTERONISM)
Etiology:A- benign unilateral adrenal adenoma
(Conn’s Syndrome) [Most Common Cause].
B-Unilateral or Bilateral hyperplasia of adrenals.
C-Adrenal carcinoma (rare).Signs and symptoms :Hypertension
(typically moderate and diastolic) Hypokalemia Polyuria Muscle weakness Fatigue Headache
LABORATORY FINDINGS
Aldosterone to Plasma Renin Assay ratio:# If ratio < 24 – excludes primary
aldosteronism.# If ratio >30 Order 24-hour urine
collection which is assayed for aldosterone, free cortisol,
and creatinine.#Low PRA (< 5mcg/L/h) with an elevated
urine aldosterone (>20 mcg/24h) indicates primary aldosteronism .
LOCALIZATION
CT scan is the initial procedure and willlocalize an adenoma in approximately
90% of patients. If no adenoma is visualized, adrenal vein sampling of aldosterone and cortisol will correctly differentiate adenoma from hyperplasia in virtually all cases.

TREATMENT
#Unilateral Adenoma – laparoscopic surgical excision.
#Bilateral hyperplasia (and pt who don’t want surgery for adenoma):
A-Dietary sodium restriction. B-Spironolactone (aldosterone antag).
PHEOCHROMOCYTOMA
DEFINITION: catecholamine-producing tumor derived from the sympathetic and parasympathetic nervous system, usually located in the adrenal gland .
Pheo = Dusky Chromo = Color Cytoma = Cell Tumor
The name refers to the color the tumor cells acquire when stained with chromium salts

EPIDEMIOLOGY
-Rare Occurs in 2-8 out of 1 million persons/ yr
-< 0.1% of hypertensive patients harbor a pheochromocytoma.
-Mean age at diagnosis is 40 years

SIGNS AND SYMPTOMS
#Classic triad Episodes of headache, profuse perspiration, and palpitations.
#Hypertension in is the dominant sign May be sustained or episodic.
#MEN 2
LOCALIZATION :ADRENAL 90% EXTRAADRNAL 10%

PHEOCHROMOCYTOMA BIOCHEMICAL TESTING
24 hour Urinary vanillylmandelic acid (VMA)
EPI-,NOR-,META-NEPHRENEPINPHREN AND NORPINEPHREN.:
PLASMA

PHEOCHROMOCYTOMA IMAGING STUDIES
- CT SCAN- MRI( METHOED OF CHIOC TO LOCALAIZ
PHEOCHROMOCYTOMA)- MIBG (metaiodobenzylguanidine):-- (1) small lesions, (2) extraadrenal- lesions, (3) bilateral lesions, and (4)
metastatic- deposits in patients with malignant
tumors.

DIAGNOSTIC STRATEGY
#Patients in whom there is a high index of clinical suspicion and those who have a greater than twofold elevation of urine catechols should undergo an adrenal CT scan.
#If the CT scan reveals a unilateral tumor and the contralateral adrenal is normal, the diagnosis is established.
#Patients with familial syndromes and those in whom cancer is suspected should undergo MIBG scanning to determine the extent of disease.
#If the adrenal CT is negative, MIBG scanning or MRI of the chest and abdomen is indicated to localize the tumor. This approach localizes virtually all tumors.
#If the clinical suspicion is low and urine catechols arenormal, imaging procedures are not indicated.
THERAPYA. PREOPERATIVE MANAGEMENT#Once the diagnosis of pheochromocytoma is established,the patient
should be prepared for surgery to reduce the incidence of intraoperative complications and postoperative hypotension.
#alpha-adrenergic blocker phenoxybenzamine, andits use has minimized surgical mortality and morbidity, The initial dosage
is 10 mg twice daily.#The dose may then be titrated upward every 2–3 days over several
weeks until the blood pressure is <160/90 mm Hg and symptoms are abolished.
#Metyrosine (alpha-methylparatyrosine), an inhibitor of catecholamine synthesis, is also useful for preoperative management although current experience is limited. Initial dosage is 250 mg every 6 hours, and total daily dosages of 2–4 g are required. Preoperative treatment for 1–2 weeks appears to be sufficient to prevent operative complications.

B. SURGERY
#Intraoperatively, hypertension is controlled with nitroprusside, and antiarrhythmics are used as needed.
#If CT and MIBG show only a solitary adrenal lesion in patients with sporadic disease, a unilateral laparoscopic approach may be used.
#Bilateral or malignant disease may require a transabdominal approach, and even if total resection
is not feasible, debulking of tumor mass facilitatessubsequent medical management of catecholamine
excess.

MALIGNANT PHEOCHROMOCYTOMA
#All patients should undergo serial follow-up to detect early recurrences.
#Despite encouraging reports of chemotherapy or 131I-MIBG therapy, it appears that only a minority of patients have sustained remissions.
INCIDENTALOMA#The most common presentation of adrenal masses is incidental observation
on cross-sectional imaging performed for other reasons.Differential Diagnosis of Adrenal Incidentaloma:-Adenoma-Metastasis-Lymphoma-Pheochromocytoma-Neuroblastoma-Adrenocortical carcinoma-Hematoma-Myelolipoma-Adrenal hyperplasia-Adrenal cyst-Granulomatous disease.
#systematic approach is required to differentiate functional adrenal masses that deserve removal and those lesions with a significant risk of carcinoma from the more common benign nonfunctional adenoma.
IMAGING#Lesions that are primarily cystic on CT or MRI are typically
benign and can be followed with serial imaging.#Benign adrenal cysts are characterized by thin nonenhancing
walls; fluid attenuation on CT and thin calcifications may be present peripherally in about 50%.
#Characteristics suspicious for malignancy include solidmasses that are large, hemorrhagic, or necrotic. MRI isusually heterogeneous on T1- and T2-weighted imagesdue to internal bleeding.#Masses with gross fat on CT (Hounsfield unit [HU]<30) are myelolipomas , benign nonfunctionaladrenal lesions with lipid and myeloid components.Myelolipomas are usually asymptomatic or present withpain if they bleed.
DIAGNOSTIC ALGORITHM#Percutaneous CT-guided biopsy may be
appropriate for adrenal masses with imaging characteristics suspicious for metastasis or in patients with known malignancy.
#All functional adrenal masses and those >5 cm should be removed.
#Laparoscopic adrenalectomy is the preferred technique andis used in most cases except very large masses suspicious for malignancy or with evidence of local extension.
#Nonfunctional adrenal masses <5 cm should be assessed for radiographic features concerning for malignancy and removed if they are irregular or hemorrhagic or have demonstrated growth.
#Those <3 cm can generally be followed up with serial CTs every 6 months initially, then yearly if
stable.
DISORDERS OF DECREASEDADRENAL FUNCTION
Adrenal insufficiency (addisonian state)Causes of adrenal insufficiency.:Primary:
-Infectious adrenalitis (e.g., tuberculosis)-Autoimmune adrenalitis.-Adrenal infiltration (e.g., metastasis,sarcoidosis)-Bilateral or pharmacologic adrenalectomy-Bilateral adrenal infarction/hemorrhage.Secondary:-Congenital ACTH deficiency.-Pituitary abnormality.-Hypothalamic abnormality.

CLINICAL CHARACTERISTICS
#Clinical signs and symptoms of Addison disease are generally nonspecific.
#pt may c\o fatigue and anorexia.#Hyperpigmentation, a hallmark of primary
adrenal insufficiency, results from high serum concentrations of ACTH in response to increased hypothalamic release of proopiomelanocortin (POMC)-derived peptides that stimulate the
melanocortin (MC-1) receptor of the skin.

#Acute adrenal insufficiency, or adrenal crisis, is a lifethreatening condition often preceded by hypotension unresponsive to fluid resuscitation. Patients are easily and often misdiagnosed with an acute abdomen, whereas abdominal pain, nausea, vomiting, and fever frequently
accompany hypovolemia in these individuals. Pediatric patients can exhibit hypoglycemic seizures.
#Adrenal insufficiency (an addisonian state) following
adrenalectomy in the setting of a normally functioning contralateral adrenal gland is unlikely, but possible.
TREATMENTThe treatment of Addison disease
involves adrenal hormonal repletion. Cortisol is replaced with hydrocortisone (15 to 25 mg per day) or with cortisone acetate (25 to 37.5 mg per day).
CONGENITAL ADRENAL HYPERPLASIA
disorder that is characterized by low cortisol production due to a metabolic enzymatic
abnormality in the cholesterol-steroid biosynthesis pathway.
#The disorder is autosomal recessive and associated with a deficiency in the enzyme 21-hydroxylase in over 95% of cases.
#In the absence of negative feedback, ACTH production by the pituitary is increased, resulting in hyperplasia of the adrenal cortex and overproduction of adrenal androgens.
#high propensity for developing benign adrenal cortical adenomas.
ADRENAL LESIONS:Malignant Adrenal CarcinomaEpidemiology:#is a rare malignancy with an incidence
of 0.5 to 2 per million.#peaks in children in the first decade of
life and adults in the fourth to fifth decades of life.
#slight female predominance.#The majority of ACCs are sporadic and
unilateral.
PATHOPHYSIOLOGY
Two hereditary disorders, Li-Fraumeniand Beckwith-Wiedemann syndrome, have
provided valuable insight into the tumorigenesis of sporadic ACC.
#squamous cell carcinoma–related oncogene (SCCRO),
#Inhibin or activin,epidermal growth factor receptor,
# vascular endothelial growth factor (VEGF).
CLINICAL CHARACTERISTICSIncidental detection of adrenal cortical carcinoma has
increased with the routine use of cross-sectional imaging.#The majority of patients still present withadvanced disease and tumor-related symptoms.#The most common hormone secreted by adrenal cortical
carcinoma is cortisol, resulting in the clinical manifestations of Cushing syndrome.
#Androgen-secreting tumors in women can lead to virilization.
#hypersecretion of aldosterone is rarely associated with ACC, when present, it is associated with profound hypertension and hypokalemia.
#Nonfunctional ACC may present with more generalized tumor related symptoms, such as abdominal fullness, back pain, nausea, vomiting….
DIAGNOSTIC TESTS#When considering the functional status of a tumor suspicious for adrenal cortical
carcinomas, glucocorticoid, mineralocorticoid,catecholamine, sexual steroid, and steroid precursor excesses should be evaluated.#Functional Evaluation of Adrenal Tumors Suspicious for Adrenal Cortical CarcinomaTYPE OF ADRENALHYPERSECRETION FUNCTIONAL EVALUATIONGlucocorticoid excess Low-dose dexamethasone suppression test Or
Late night salivary or 24-hour urine cortisolSexual steroids andsteroid precursors DHEA-S \\ 17-OH-progesterone\\
Androstenedione Testosterone 17β-estradiol (only in men and
postmenopausal women)Catecholamine excess Serum or urinary metanephrines
Mineralocorticoid excess Aldosterone to renin ratio (only in patients with hypertension or hypokalemia
#On cross-sectional imaging, adrenal cortical carcinomas tend to be larger than benign adrenal tumors with an average size of 10 to 12 cm on presentation. Indeed over 90% of ACCs are greater than 5 cm.
#Common radiographic characteristics of adrenal carcinomas on CT imaging include the presence
of irregular borders, irregular enhancement,calcifications,
and necrotic areas with cystic degeneration.Mean attenuation on noncontrast CT scan in ACC is
significantly higher (39 HU) compared with adenomas
(8 HU).#They will not demonstrate the contrast washout
MRI provides valuable information when evaluating adrenal tumors. ACCs appear isointense relative to the liver or spleen on T1-weighted images.
detecting the presence of a tumor clot and delineating its extent.
FDG PET SCAN.

PATHOLOGIC EVALUATION
Weiss Pathologic Criteria for DifferentiatingBenign and Malignant Adrenal TumorsHigh nuclear grade (Furman grade 3 to 4)High mitotic rate (greater than 5 mitoses per HPF)Presence of atypical mitosesCharacter of cytoplasm (low percentage of clear cells)Diffuse architecture of tumor cellsPresence of necrosisInvasion of venous structuresInvasion of sinusoidal structuresInvasion of tumor capsule
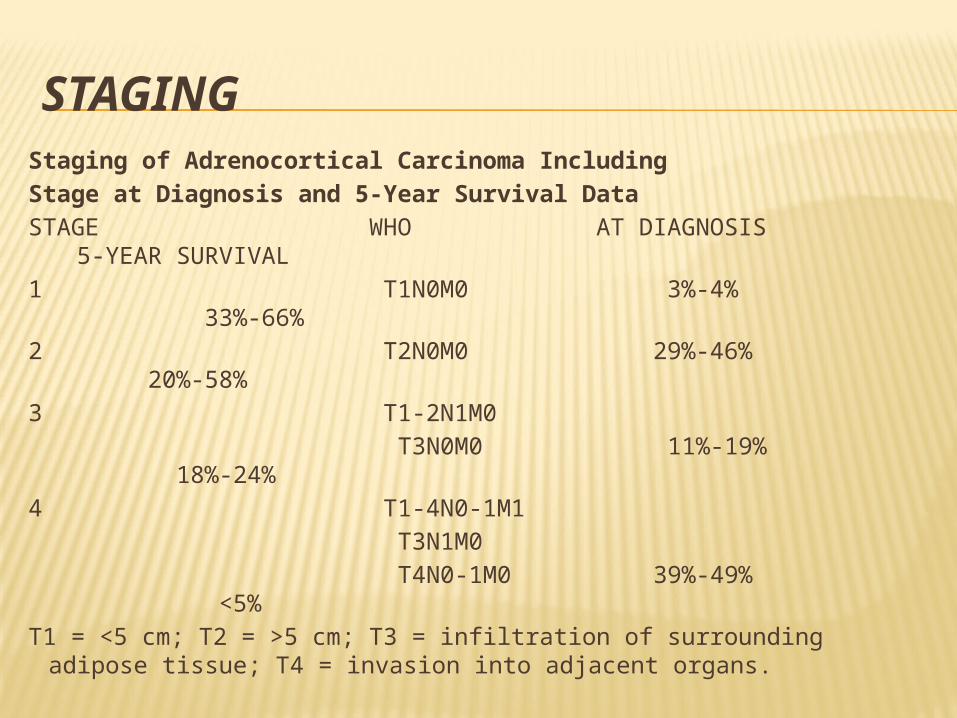
STAGINGStaging of Adrenocortical Carcinoma IncludingStage at Diagnosis and 5-Year Survival DataSTAGE WHO AT DIAGNOSIS 5-YEAR
SURVIVAL1 T1N0M0 3%-4% 33%-66%2 T2N0M0 29%-46% 20%-58%3 T1-2N1M0 T3N0M0 11%-19% 18%-24% 4 T1-4N0-1M1 T3N1M0 T4N0-1M0 39%-49% <5%T1 = <5 cm; T2 = >5 cm; T3 = infiltration of surrounding adipose
tissue; T4 = invasion into adjacent organs.
MANAGEMENT.#Despite aggressive surgical resection, adrenal
carcinoma is associated with a high rate (60% to 80%) of recurrent disease.
#radiation therapy remains the treatment of choice in the
management of bone and CNS metastasis.#Adjuvant radiation has been noted to decrease local
recurrence rates following complete tumor resection.MEDICAL THERAPY: Mitotane is an oral synthetic
derivative ofthe insecticide dichlorodiphenyltrichloroethane (DDT)
and is the most commonly used chemotherapeutic agent in the treatment of adrenal cortical carcinoma.
METASTASES
over 25% of patients with melanoma and lung carcinoma have metastases to their adrenals.

BENIGN
AdenomaEpidemiology:Adenomas are the most commonneoplasms arising from the adrenal gland and
are most often associated with the cortex.-The incidence of adenomas rises with age.-The essential evaluation of the small adrenal
massrequires differentiating the nonfunctional
benign adenoma from functional or malignant lesions.

PATHOPHYSIOLOGY AND CLINICAL CHARACTERISTICS.
-Adrenal adenomas are by definition benign and the
vast majority are metabolically silent.
-pathologists use a set of criteria proposed by Weiss
along with modern immunohistochemical methods to differentiate the two clinical entities

DIAGNOSTIC TESTS.
The goal in evaluating any adrenal lesion is twofold:(1) rule out the possibility of malignancy and (2) document metabolic inactivity of the lesion in
question.#Noncontrast CT scan is arguably the most valuableimaging study for the diagnosis of an adrenal
adenoma.<10 HU.#incidentalomas are evaluated for excess cortisol
and catecholamine secretion. In patients with history of hypertension, hyperaldosteronemia also should be ruled out

TREATMENT
#Adenomas that are metabolically active should undergo resection in acceptable surgical candidates.
#In patients with nonfunctional adenomas, the size of
lesion and its growth characteristics dictate management.
ONCOCYTOMA-It’s a very rare tumor.-histologically oncocytic adrenal lesions
are characterized by mitochondria-rich, large, eosinophilic cells with abundant granulations.
- Most lesions that are are metabolically inactive.
- proportion of lesions can exhibit malignant
potential.
MYELOLIPOMA-Myelolipoma is a rare lesion of the
adrenal gland that contains hematopoietic elements and
mature adipose tissues.-Surgery is indicated only forextremely large or symptomatic lesions.
GANGLIONEUROMA
are rare tumorstend to occur in the young and can grow
to encase critical structures.

ADRENAL CYSTSEpidemiology-account for 1% to 5%.- Cystic adrenal lesions can be diagnosed
throughout life and as early as the prenatal period.-range from mm to greater than 20
cm.- majority of adrenal cysts are unilateral.-women > men .
PATHOPHYSIOLOGY.
Four histologic types of adrenal cysts:
-pseudocysts: the most common and result from previous intra-adrenal hemorrhage or infarction.
-endothelial: lymphangiomatous and angiomatous subtypes.
-epithelial: characterized as glandular and embryonal cysts.
- parasitic cysts:associtd with Echinococcus infections.
THANK YOU !!!