adjusting for treatment switching in rcts identifying ... · identifying, analysing and justifying...
TRANSCRIPT
Adjusting for Treatment Switching in RCTs –
Identifying, analysing and justifying
appropriate methods:
a case study in metastatic melanoma
Bell H1 , Lat imer N 1 , Amonkar M 2, Swann S 2
1University of Shef field, 2Novar t is

Overview
• What is treatment switching?
• Direct and indirect switching
• Treatment switching adjustment methods for direct switching
• Applying adjustment methods to the BREAK-3 trial
• Assessing the validity of the assumptions
• Indirect switching to other post-study treatments
• Conclusions

What is treatment switching?
Survival time
Control Treatment
Intervention
Control Intervention
PFS
PFS
PFS
PPS
PPS
PPS
True OS difference
RCT OS difference
Switching can be “direct” or “indirect”

Treatment switching adjustment methods for direct switching
• Rank preserving structural failure time (RPSFT) model Robins and Tsiatis (1991), White, et al (1999)
• Iterative parameter estimation (IPE) algorithm Branson and Whitehead (2002)
• Inverse probability of censoring weights (IPCW) Robins and Finkelstein (2000), Hernan et al. (2001), Fewell, et al (2004)
• Two-stage accelerated failure time model Latimer, et al (2014)

Treatment switching adjustment methods for direct switching
• Rank preserving structural failure time (RPSFT) model Robins and Tsiatis (1991), White, et al (1999)
• Iterative parameter estimation (IPE) algorithm Branson and Whitehead (2002)
• Inverse probability of censoring weights (IPCW) Robins and Finkelstein (2000), Hernan et al. (2001), Fewell, et al (2004)
• Two-stage accelerated failure time model Latimer, et al (2014)
RPSFTM and IPE
make the common
treatment effect
assumption

Treatment switching adjustment methods for direct switching
• Rank preserving structural failure time (RPSFT) model Robins and Tsiatis (1991), White, et al (1999)
• Iterative parameter estimation (IPE) algorithm Branson and Whitehead (2002)
• Inverse probability of censoring weights (IPCW) Robins and Finkelstein (2000), Hernan et al. (2001), Fewell, et al (2004)
• Two-stage accelerated failure time model Latimer, et al (2014)
IPCW and Two-stage
method are reliant on no
unmeasured confounders
assumption

Treatment switching adjustment methods for direct switching
• Rank preserving structural failure time (RPSFT) model Robins and Tsiatis (1991), White, et al (1999)
• Iterative parameter estimation (IPE) algorithm Branson and Whitehead (2002)
• Inverse probability of censoring weights (IPCW) Robins and Finkelstein (2000), Hernan et al. (2001), Fewell, et al (2004)
• Two-stage accelerated failure time model Latimer, et al (2014)
Two-stage is reliant on the
existence of a disease-
related secondary baseline

Treatment switching adjustment methods for direct switching
• Rank preserving structural failure time (RPSFT) model Robins and Tsiatis (1991), White, et al (1999)
• Iterative parameter estimation (IPE) algorithm Branson and Whitehead (2002)
• Inverse probability of censoring weights (IPCW) Robins and Finkelstein (2000), Hernan et al. (2001), Fewell, et al (2004)
• Two-stage accelerated failure time model Latimer, et al (2014) RPSFTM, IPE and two-stage are generally applied with
recensoring, but this may cause bias if the treatment
effect is time-dependent

0
10
20
30
40
50
60
70
Open
High
Low
Close
Applying adjustment methods to the BREAK-3
trial (August 2014 data-cut)
• Dabrafenib vs DTIC chemotherapy 187 patients randomised to dabrafenib, 63 patients randomised to DTIC
• Switching was permitted after disease progression 37 (58.7%) DTIC group patients had switched onto dabrafenib as of August 2014
• Time from randomisaton to switch Median time-to-switch was 93 days,
80% of switchers had switched by approximately 169 days,
90% of switchers had crossed over by approximately 281 days
0
10
20
30
40
50
60
70
Open
High
Low
Close
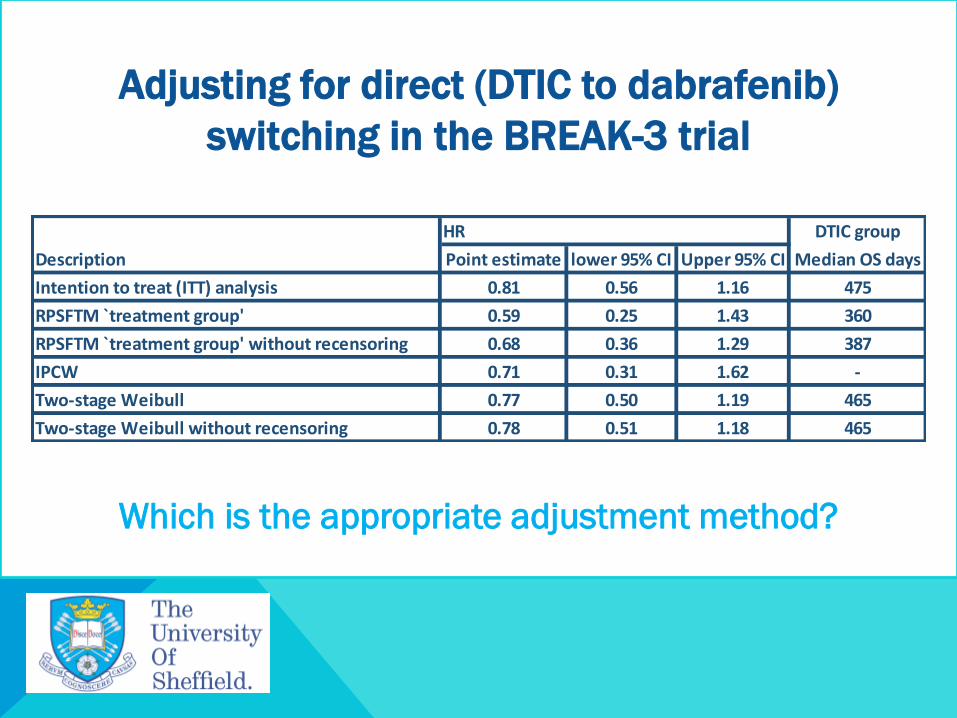
Adjusting for direct (DTIC to dabrafenib)
switching in the BREAK-3 trial
HR DTIC group
Description Point estimate lower 95% CI Upper 95% CI Median OS days
Intention to treat (ITT) analysis 0.81 0.56 1.16 475
RPSFTM `treatment group' 0.59 0.25 1.43 360
RPSFTM `treatment group' without recensoring 0.68 0.36 1.29 387
IPCW 0.71 0.31 1.62 -
Two-stage Weibull 0.77 0.50 1.19 465
Two-stage Weibull without recensoring 0.78 0.51 1.18 465
Which is the appropriate adjustment method?

YOU Assessing the validity of assumptions
• Common treatment effect (RPSFTM and IPE)
• Median time-to-switch was 93 days
• Comparisons of PFS as randomised and comparisons of PFS of first and
second progression for switchers indicated that switchers do benefit from
switching treatment – no strong evidence to reject common treatment effect
• No unmeasured confounders (IPCW and Two-stage)
• Data on EQ5D and EORTC was not collected beyond the June 2012 data-cut
• Time to switch from secondary baseline (Two-stage)
• Median time from progression to switch for switching patients was 16 days
X

YOU Assessing model performance
• Counterfactual HR (RPSFTM and IPE)
• Counterfactual HRs were 1.00 for RPSFTM treatment group and 1.35 for IPE
treatment group using a Weibull model
• Model convergence
• IPE algorithm with recensoring did not converge when applied to BREAK-3
• EORTC covariates were excluded to achieve convergence in the IPCW and
Two-stage model (the EQ-5D utility score was retained)
• Sample size and number of switchers and non-switchers
• 187 patients randomised to dabrafenib, 63 patients randomised to DTIC
• 37 (58.7%) DTIC group patients switched onto dabrafenib
• Maximum stabilised weight (IPCW) - Highest weight was 17.99

YOU Assessing model performance
• Extent of data loss due to recensoring (RPSFTM, IPE and Two-stage)
• Longest follow -up time was reduced by 35% from 1236 days to 781 days
• Data analysis indicated that the treatment effect was time-dependent
RPSFTM incorporating recensoring RPSFTM without recensoring

YOU Ruling out the least appropriate adjustment
analyses for BREAK-3
• All adjustment analyses produced lower HRs than the ITT HR
• IPE – model did not converge and counterfactual HR was not equal to 1
• IPCW – small sample size, convergence issues, some missing data
• Two-stage - convergence issues and some missing data
• RPSFTM with recensoring – large amount of data lost which is likely to lead to
bias due to the changing treatment effect over time
Preferred direct switching adjustment analysis:
RPSFTM without recensoring
X
X
X
X

Indirect switching - other post-study treatments
• BREAK-3 was further confounded by patients switching onto
other post-study treatments 43 patients switched onto other small molecule therapy
27 of these patients were in the dabrafenib group and 16 were in the DTIC group
HR
Description Point estimate lower 95% CI Upper 95% CI
Intention to treat (ITT) analysis 0.81 0.56 1.16
RPSFTM (direct and indirect) + Two-stage Weibull 0.68 0.33 1.63
RPSFTM `treatment group' without recensoring 0.68 0.36 1.29

YOU Conclusions
• All adjustment analyses produced lower HRs than the ITT HR, and hence,
a larger treatment effect.
• It is necessary to assess the validity of the key assumptions and
performance of each of the models in relation to the trial data, to find the
most appropriate method of adjusting for treatment switching.
• Of the analyses applied to the BREAK-3 trial, we preferred the
RPSFTM+two-stage adjustment analysis that adjusts for direct and
indirect switching, because we believe it was necessary to attempt to
adjust for indirect switching and direct switching in the BREAK-3 trial.

Thank you for your attention T h e e n d

References
• Branson M, Whitehead J. Estimating a treatment effect in survival studies in which patients
switch treatment. Statistics in Medicine 2002; 21(17):2449-2463.
• Fewell Z, Hernan MA, Wolfe F, Tilling K, Choi H, Sterne JAC. Controlling for time-dependent
confounding using marginal structural models. The Stata Journal 2004; 4(4):402-420.
• Hernan MA, Brumback B, Robins JM. Marginal structural models to estimate the joint causal
effect of nonrandomized treatments. J Am Statist Assoc. 2001; 96(454):440-448.
• Latimer N, Abrams KR, Lambert PC, Crowther MJ, Wailoo AJ, Morden JP, Akehurst RL,
Campbell MJ. Adjusting survival time estimates to account for treatment switching in
randomised controlled trials – an economic evaluation context: Methods, limitations and
recommendations. Medical Decision Making, online first Jan 2014
• Robins JM, Finkelstein DM. Correcting for noncompliance and dependent censoring in an
AIDS clinical trial with inverse probability of censoring weighted (IPCW) log-rank tests.
BioBREAKs 2000; 56(3):779-788.
• Robins JM, Tsiatis AA. Correcting for Noncompliance in Randomized Trials Using Rank
Preserving Structural Failure Time Models. Commun Stat Theory Methods. 1991;
20(8):2609-2631.
• White IR. Estimating treatment effects in randomized trials with treatment switching.
Statistics in Medicine 2006; 25(9):1619-1622.