adherence to cpap in osas by ahmad younes professor of thoracic medicine mansoura faculty of...
TRANSCRIPT

Adherence to CPAP in OSAS
BY
AHMAD YOUNES
PROFESSOR OF THORACIC MEDICINEMansoura faculty of medicine

Establishing a Successful CPAP Adherence Program

Studies show that patients having OSA typically go undiagnosed for up to 10 years with steadily increased use of healthcare resources
• Co-morbidities associated with OSAS:• Diabetes• Hypertension • Heart Disease• Stroke

CPAP TREATMENT FOR OSAS• OSAS occurs in an estimated 5% of the adult population.• CPAP is a first line treatment for moderate to severe OSA. • CPAP is almost 100% effective when used regularly but
adherence with treatment poses problems for many patients.
• The provision of CPAP involves more than simply selling a CPAP device and mask: it involves education, support and ongoing care including the monitoring of treatment adherence.
• This is often a shared responsibility between the patient, the sleep physician, the sleep clinic and organization which provides CPAP equipment

CPAP adherence• Adherence like compliance refers to the degree
that an individual follows a recommended illness-related recommendations, but while compliance suggests a passive role, adherence emphasizes an active role.
• Adherence failure : use of CPAP for less than 4 h / night on 70% of nights and or lack of
symptomatic improvement.• Internationally 5-50% of OSA reject CPAP treatment
option or discontinue use within the first week .• 12 to 25% of the remaining patients may be expected
to have discontinued its use at 3 years

CPAP adherence Outcomes• CPAP reduces objective daytime sleepiness ,
improves some measures of cognitive performance ,reduces depression, reduces cardiovascular mortality and morbidity , reduces the risk of motor vehicle crashes and improves perceptions of quality of life,
• Reduces healthcare utilization • Adherence to CPAP treatment is the largest
factor impacting on the effectiveness of treatment

The basic requirements are:• Staff who are appropriately trained • A choice of CPAP equipment sufficient to meet
individual patient needs • A CPAP initiation service which provides patients
with adequate information and education to instill confidence in their treatment.
• A CPAP follow-up service which comprises an appropriate number of follow-up contacts and the opportunity for patients to access the service on an as-needed basis.
• An infrastructure that enables timely and efficient communication with sleep clinics and referring doctors about their patients

Assessment of CPAP adherence
• To assess CPAP adherence and treatment efficacy, CPAP manufacturers have implemented tracking systems that monitor CPAP efficacy (residual sleep-disordered breathing, hours of CPAP use, and mask leak ).
• Despite the fact that CPAP adherence tracking systems have not yet been rigorously tested to show measurably improved outcomes, their use seems clinically sound.
• In fact, CPAP adherence tracking now is a requirement for Medicare and other payers to continue reimbursement for CPAP beyond the first three months of treatment. Moreover, we can track CPAP use better than almost any other therapy for a chronic disease and we have the ability to specifically link patterns of use to OSA outcomes.

Why do we care about CPAP adherence and hours of use?
• Because studies have shown that increasing hours of CPAP use results in better outcomes.
• Patients routinely overestimate their CPAP usage with self report .Thus, objective monitoring of CPAP use has become the standard of care for managing patients with sleep apnea.
• The tracking systems are not limited to conventional CPAP alone, but also can be utilized in patients being treated with auto-CPAP, bi-level, auto-bi-level, or adaptive servo-ventilation.
• Adherence tracking systems can collect data that measures the date ranges of CPAP usage, the total number of nights the CPAP was utilized (and not utilized); sort the data to the percent of nights CPAP was utilized, percent of nights CPAP was used > 4 hours/night,
• In general, the CPAP adherence-tracking systems are accurate in objectively determining CPAP use.

Unfortunately, sleep-disordered breathing event detection and leak data are more problematic to interpret than hours of use.
• CPAP tracking systems provide averaged data (over many nights, so these data may not reflect the last week or month) for the residual AHI while using CPAP.
• Currently CPAP devices use a reduction in airflow (measured with a pneumotachograph) to estimate the residual AHI . In contrast, during polysomnography, apnea or hypopnea determination is based on more robust data, including respiratory flow patterns (nasal pressure and a thermistor), EEG arousal, thoraco-abdominal effort, and oxyhemoglobin desaturations.
• Thus, residual AHI measured from a CPAP download is not a true surrogate of the AHI measured during a sleep study. Caution therefore must be used in interpreting OSA resolution or persistence from CPAP adherence data reports.

Event detection data should be used in the management of OSA patients if the data are at either end of the spectrum [normal AHI(< 5 events/hour) or very high AHI (> 30 events/hour).
• Intermediate residual AHI data can be difficult to interpret and should be examined within the clinical context of the patient.
• Reduction in CPAP mask leak can improve adherence and improved adherence can improve OSA outcomes,
• Mask leaks depend on both the mask (nasal pillows, or full face) and the pressure being delivered.
• What is a clinically significant mask leak? There are no data to answer this question but there may be no leak threshold that is "clinically acceptable," as even a small leak directed into a patient's eyes can be a problem.

Mask leak data are averaged measurements and may not reflect recent changes in the CPAP interface.
• Mask leak may be secondary to leaking through the mouth or around the mask.
• If the CPAP unit is running when a patient goes to the bathroom, this may appear as large leak in the download even though there is not a true mask leak.
• Leak data, like event detection data, must be examined within the clinical context of a patient; extreme measurements on the spectrum are more likely to be valid than middle of the road numbers.
• If the patient's mask leak is significantly greater than the leak threshold specified by the specific CPAP manufacturer, the interface could be changed.
• The new CPAP adherence tracking devices measure many other respiratory signals data , including periodic breathing (Cheyne-Stokes pattern), vibratory snoring, flow limitation, clear airway apnea (central sleep apnea). Unfortunately there are essentially no examining the validity, reliability, reproducibility, or utility of these signals.

There are several different methods to transmit CPAP adherence tracking data
• Most systems use cards (smart card-SD cards), memory sticks, download cable or wireless transmission.
• CPAP adherence profiles are not standardized between the different proprietary tracking systems and the reports are not yet easily exportable to electronic medical records.

• DOWNLOAD CABLES CONNECT YOUR MACHINE TO YOUR COMPUTER SO THAT YOU MAY DOWNLOAD YOUR SLEEP METRICS TO YOUR COMPUTER FOR VIEWING. SOFTWARE IS NEEDED TO RETRIEVE THIS DATA.
• IF YOU DON'T WANT TO DEAL WITH MOVING YOUR MACHINE CLOSE TO YOUR COMPUTER, CHECK TO SEE IF YOUR MACHINE HAS A CARD READER INSTEAD
• DATA CARDS FIT INTO YOUR MACHINE TO COLLECT YOUR SLEEP DATA. THESE CARDS CAN BE TAKEN OUT AND READ BY A CARD READER THAT HOOKS UP TO YOUR COMPUTER. SOFTWARE IS STILL NECESSARY FOR DATA TO BE DOWNLOADED.

• This USB Smart Stick Memory Card is designed for use with all Fisher & Paykel Sleep Style 242 (HC242), Sleep Style 244 (HC244) and Sleep Style 254 (HC254) CPAP Machines.
• The Smart Stick works as a miniature USB drive capable of transferring therapy data from a Smart Stick enabled Sleep Style CPAP to a computer without the need for a separate card reader.
• To review data on the card software, like Fisher & Paykel's ,Performance Maximizer Software, is required. Fisher & Paykel - 900HC611

How to Read a CPAP Adherence Report
• Check nightly usage hours • Check leak data. This is usually shown as L/sec.
Values significantly greater than 0.4 L/sec are an indication that the patient is using an inappropriate or poorly-fitting CPAP mask.
• Check apnea events. This indicates the number of times the patient has stopped breathing and is shown as events per hour (or e/hr.) These values should be at or near zero if the patient is receiving sufficient airway pressure; multiple apnea events per hour are an indication that the patient's CPAP pressure needs to be adjusted .

In conclusion1-CPAP adherence must be followed consistently
over time.
2-CPAP adherence, in terms of hours of use / night, has been shown to improve clinical outcomes.
3-CPAP usage can be reliably obtained from CPAP tracking systems and these data are robust.
4-The residual events (apnea / hypopnea) and leak data from CPAP tracking systems are not as easy to interpret and standards need to be developed to optimally utilize these data.

Barriers to CPAP Adherence

Barriers to CPAP Adherence
Equipment Related
Patient Related
Clinician Related
CPAP Adherence
Therapy Related

Equipment Related Barriers
• Complexity of therapy/device
• Excessive mask leak
• Portability/Battery backup
• Device noise
• Hose length
• Improper mask fit



Therapy Related Barriers
• Adverse reactions that go unaddressed– Nasal dryness or dry eyes– Nasal congestion– Skin irritation– Bloody nose
• Expense of therapy
• Governmental policies ( funding, licenses of drivers )
• Adherence decreases over time

Nasal prongs

Nasal pillow

Nasal mask

Oral CPAP Mask

Full face mask

Total face mask

Patient Related Barriers• Health literacy
• Ambivalence
• Lack of family or other social support.
• Patient economics
• Lack of reimbursement
• Psychological variables - claustrophobia
• Physical limitations
• Less severe factors/Little or no perceived benefit from therapy
• Use of prescription/non-prescriptions drugs or alcohol

Claustrophobia
• Claustrophobia is a form of specific phobia that entails extreme anxiety and panic elicited by situations such as tunnels, elevators, or other settings in which the individual experiences a sense of being closed in or entrapped.
• Almost one-third of sleep apnea patients endorse CPAP-related claustrophobia and may lead to treatment abandonment.
• CPAP-related claustrophobia was perceived as one of the largest deterrents to CPAP therapy.

Clinician Related Barriers
• Poor patient relationship
• Lack of clinician follow-up
• Expression of doubt concerning therapeutic potential or creating falsely elevated expectations
• Unwillingness to educate patient
• Lack of knowledge on patient’s medical history, and other medication the patient may be taking


Intervention
Equipment Related
Patient Related
Clinician Related
CPAP Adherence
Therapy Related

Equipment/Therapy Interventions• Heated humidification to relieve nasal dryness, running
nose, nose bleeds
• Nasal spray
• CPAP modalities: auto-titrating or bilevel PAP
• Refit interface
• Change mask type• Comfort features
– Ramp
– Quieter blower
– Battery backup
– Expiratory pressure relief
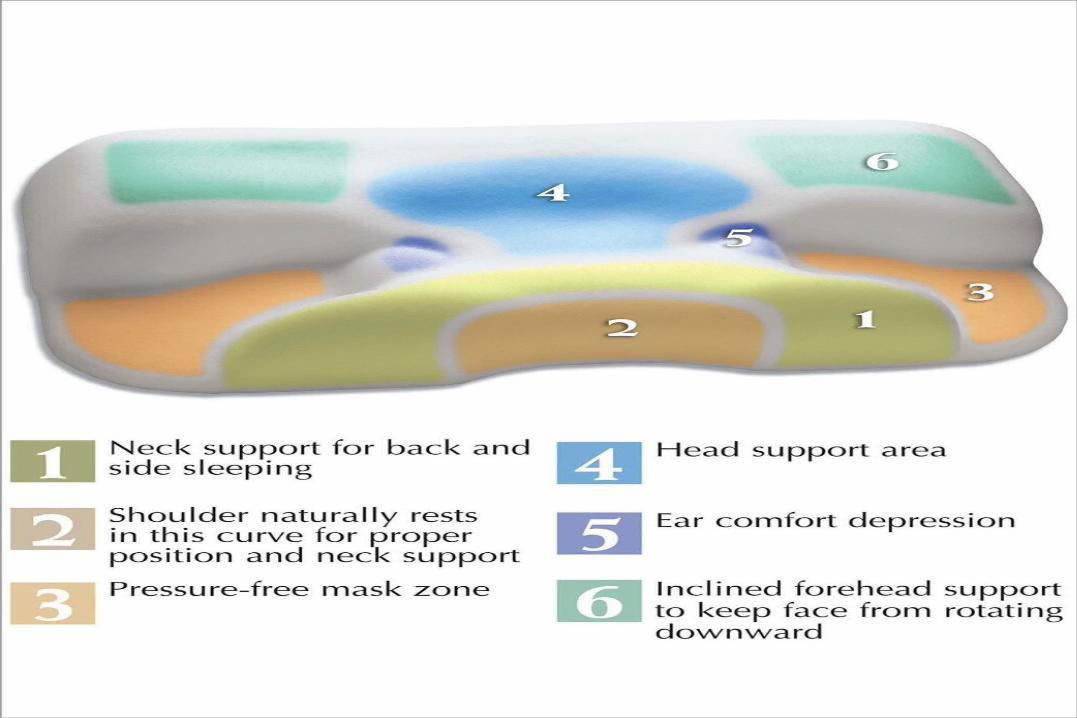
Contour CPAP Compliance Pillow

The Contour CPAP Pillow works with all major brands of CPAP masks!

The Contour CPAP Pillow Improves:• CPAP Ease of use• Sleep Comfort for all CPAP users• CPAP Compliance -• Neck support and spine alignment• Airway alignment
The Contour CPAP Pillow Reduces:• Mask leaks• Pressure on mask and face• Mask discomfort

Patient/Clinician Intervention• Family/social support
• Bed partner’s acceptance
• Suitable education and training on equipment• Cognitive behavioral therapy, motivational
enhancement therapy
• Rapid response to difficulties

Compliance Program Options• Physician/Sleep Lab follow-up programs
• Support meetings (CPAP clinics)
• Home care therapist-driven programs
• Internet programs
• Follow up cards
• Telephone (Hotline)

Compliance Program • Why this Protocol…Critical 1st Days
• “Failure to adhere with treatment has been reported to be as high as 50%, with patients typically abandoning therapy during the first 2 to 4 weeks of treatment.”
• “Those patients who manifested good adherence during the first week of treatment continued using CPAP for the entire first year.
• Hours of use the first week was correlated to hours of use the first year.”

Compliance Program• “Patient education, close follow-up and intervention
appear to improve long-term tolerance.” • Education
1-Disease state– What is their diagnosis – How severe is their OSA– How will it impact their lives– What are the potential co-morbidities– What should they expect2-Equipment
– How it works
– How to inspect and replace when required
– What support is available to ensure the patients success in therapy.

Vigilance Testing
Reaction time • The lapse of time between stimulation and the beginning
of response.• Click the large button on the right to begin. • Wait for the stoplight (red) to turn green. • When the stoplight turns green, click the large button
quickly! • Click the large button again to continue. • The stoplight may take up to seven seconds to change.
The amount of time is random. • You may press any key, instead of clicking the mouse
button, if you prefer. • You will be tested five times, and your average reaction
time will be calculated.

Conner’s Continuous Performance Test
• Test vigilance in all subjects before CPAP use and again 12 weeks after use had been initiated.
• Letters are flashed on a computer screen in rapid succession. Subjects are asked to press a response key when they see the letter X, but only when it is preceded by the letter A.
• This AX condition is thought to maximize the cognitive load of vigilance over and above that of simple reaction time.
• The test lasts about 12 minutes, and provides measures of accuracy and speed of target detection.
• Dependent measures include the total number of hits, average reaction time to targets, d´ (a measure of signal sensitivity), and the total number of target omissions.

Psychomotor vigilance testing of professional drivers in
the occupational health clinic



Initiation of CPAP treatment should also include
general advice on lifestyle and medical issues
• Patients who smoke should be advised to stop. • Alcohol should be avoided. • Avoided nocturnal sedatives or sleeping tablets.• Advice regarding body weight and its interaction
with OSA should be provided if appropriate. • Patients should be informed about the impact of
sleeping position on sleep apnea severity. • Relief of nasal obstruction should be viewed as an
adjunct to CPAP therapy, potentially improving adherence.

Initiation of treatment:
• Education and reassurance are critical components of the initiation of therapy. This process must be interactive with the patient having opportunity to have their questions answered and concerns addressed. The involvement of the patient’s partner in this process is important to encourage acceptance and subsequent adherence.
• The interface fit shall be assessed while the patient lying down in supine and lateral postures.
• The patient shall be given the opportunity to try a variety of CPAP interfaces to ensure optimal fit and comfort and minimal leak.

SESSION 1
• Review subject’s sleep data • Review symptoms noticeable to the subject ( fatigue,
excessive daytime sleepiness) • Review symptoms not apparent (hypertension, cardiac
problems) • Review results of performance on cognitive tests .• Rate the importance of treatment .• Review PSG with CPAP and specify how this might
address the above problems. • Discuss the advantages and disadvantages of treatment • Develop goals for therapy

Ongoing Management of CPAP Usage: • It is suggested that approximately 7, 30, 60 days and
approximately 12 months after treatment initiation are appropriate times.
• At this time the provider shall
1- Determine the patient’s usage from the meter of the CPAP device and calculate the average daily hours of CPAP usage.
2- Check the device and humidifier for satisfactory operation.
3- Check filters, mask and head-gear for satisfactory condition and advise the patient of any faults and suggested remedial actions.

SESSION 2
• Examine compliance data for the first week • Discuss noticeable changes with treatment .• Discuss changes not apparent
(hypertension ,cardiac problems) .• Troubleshoot discomfort .• Discuss realistic expectations of treatment .• Review treatment goals .

Exposure therapy for claustrophobic reactions to CPAP
• claustrophobia is composed of two “core” fears: fear of restriction, and fear of suffocation.
• Exposure therapy is indicated for individuals with sleep apnea who are unable to tolerate CPAP devices due to anxiety reactions.
• CONTRAINDICATIONS :unstable psychiatric symptoms (substance use, post-traumatic stress disorder, suicidal/homicidal ideation, psychosis), inability to maintain a therapeutic relationship, or economic/domiciliary instability

RATIONALE FOR INTERVENTION
• Because CPAP requires the patient to breathe pressurized air through a nasal or full-face mask strapped to the head, it is not difficult to understand how this treatment can tap into fears of suffocation and restriction.
• In some patients, this therapy may elicit memories of the original Unconditioned stimulus or set of circumstances that elicited the claustrophobic response to CPAP.
• some patients appear to develop claustrophobic reactions de novo, specifically in response to an unpleasant experience while using CPAP.
• The treatment of choice for specific phobias, including claustrophobia, is exposure therapy

RATIONALE FOR INTERVENTION
• The phobic individual confronts the feared object or situation either imaginally or in real life (in vivo).
• Typically, a hierarchy of fearful situations ranging from least to most anxiety-provoking is generated by the individual.
• The individual is supported in experiencing these feared situations in a gradual manner, and over time the anxiety decreases.
• The effectiveness of exposure therapy stems from learning to tolerate and manage anxiety without the need to escape or avoid the phobic stimulus,
• Exposure therapy increases the individual’s perception of control over fear

RATIONALE FOR INTERVENTION
• Exposure therapy for CPAP emerged as a means of breaking the link between anxiety (triggered by CPAP as the CS) and the avoidance response
• A deconditioning process based on those used for specific phobias is employed so that CPAP loses it value as a Condition stimulus for anxiety and avoidance.
• This goal is achieved through the gradual re-exposure of the patient to CPAP in a structured manner so as to extinguish the link between CPAP as the Condition stimulus , and the Uncondition stimulus that led to the initial problematic response.
• This link is often a symbolic one in that CPAP was never associated with the original Uncondition stimulus but merely mimics it and elicits memories of it.

STEP BY STEP DESCRIPTION OF PROCEDURES
• Exposure therapy for CPAP-related claustrophobia can be delivered effectively in one to six sessions over 1–3 months.
Initial Session (Session 1) • Assessment and history Claustrophobia (tolerating air pressure, having the
mask on the face, having the mask strapped over the head) claustrophobia in other situations and the presence of other anxiety disorders
• Patient education on sleep apnea and CPAP therapy • Build therapeutic trust • Implementation of exposure therapy Presentation of treatment rationale Establish exposure hierarchy Goal setting / homework

Patient handout describing exposure steps for home practice. • Do not try wearing CPAP during sleep until you are comfortable with it
during the daytime. • If your machine has a RAMP button, you may use this function to keep
the pressure at a low level during practices.1-Turn the CPAP airflow ON. Hold mask over your nose, and practice
breathing with machine on while awake. While you are doing this, keep your mouth closed and breathe regularly through your nose. Start with short periods of time (1–5 min) and gradually build up to longer periods of time.
2. Turn the CPAP airflow ON and wear the mask over your nose with the straps on your head. Practice breathing with CPAP on while awake. Wear CPAP for longer periods of time until you can have it on for 15–20 min comfortably.
3. Take a nap during the day with CPAP machine and mask on. It is not important whether you fall asleep or not – the goal is to rest comfortably in your bed with the CPAP on.
4. Wear CPAP at night when you go to sleep. If you experience claustrophobia or uncomfortable feelings, go to previous step until comfortable. Then proceed to next step.

Follow up Sessions (Sessions 2–6) • Assess adherence to homework (Monitor progress ) Patient self-report Objective CPAP data (CPAP card is read during the session)• Problem-solve obstacles • Conduct in-session exposure trial (If the patient continues
to report claustrophobic reactions while using CPAP at home) asking patients to apply their CPAP as they do at home. This reveales that, for some patients, “claustrophobia” is caused by an incorrectly applied or fitted mask. claustrophobia can sometimes be ameliorated by trying an alternative mask style,
• Provide feedback and support regarding CPAP use( once patients complete the exposure protocol and are using CPAP at home successfully, follow-up visits may be spaced at increasing intervals (e.g., 3 months, 6 months, 12 months), or as needed).

CPAP adherence• A team effort is needed to enhance CPAP adherence.
The team may consist of the patient , family/bed partner, medical-equipment provider, respiratory therapist, sleep center staff, sleep center physician, primary care physician, and a home nursing service if applicable.
• Adherence is dependent on layers of information providing the patient with ongoing education, written instructions, demonstration of equipment, and the timely addressing and troubleshooting of the patient’s concerns and problems.
• Adherence of patients are clear indicators of the quality of the service.
