addressing diversity in govt health policies n health insurance regulatory frameworks for effective...
TRANSCRIPT

Addressing Diversity in Government Health Policies and Health Insurance Regulatory Frameworks for Effective Business Development
6th Annual Health Insurance Asia, 2012
1
Regulatory Frameworks for Effective Business Development
July 17, 2012
Dr. Milind Sabnis, MD, MBA
Principal Consultant
Healthcare, Asia Pacific

2

Agenda
• INTRODUCTION
• KEY GLOBAL TRENDS IMPACTING HEALTHCARE
• HEALTHCARE SPENDING IN ASIA
• HEALTHCARE INSURANCE
3
• HEALTHCARE INSURANCE
• FUTURE OF HEALTHCARE

KEY GLOBAL TRENDS IMPACTING HEALTHCARE
4
KEY GLOBAL TRENDS IMPACTING HEALTHCARE

Globalization, consumerism, and prosperity are the 3 major trends that will impact healthcare…
Globalization
Globalization:
• World is becoming smaller: cheap air- travel, connectivity,
internet, medical tourism
• Increased healthcare awareness because of multiple media
Consumerism:
• Increased awareness of medical conditions; potential
treatments, best physicians, hospitals to treat these conditions
• Increased decision making in choosing physicians,
hospitals, and insurance plans
1
31
5
ConsumerismProsperity
hospitals, and insurance plans
Prosperity:
• Increasing disposable income, financial independence
leading to exploring more choices
• Increased health awareness has led to consumers spending
more on health prevention
2
2 3
Source: Frost & Sullivan
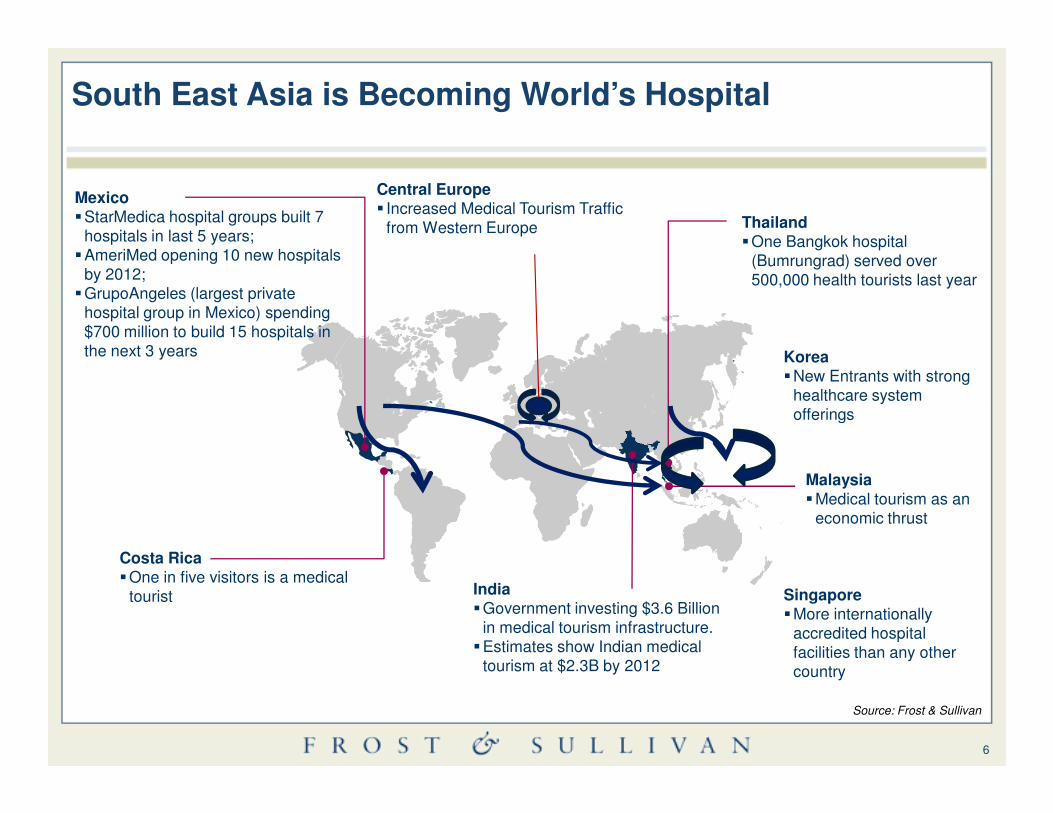
South East Asia is Becoming World’s Hospital
Thailand�One Bangkok hospital
(Bumrungrad) served over 500,000 health tourists last year
Mexico�StarMedica hospital groups built 7
hospitals in last 5 years;�AmeriMed opening 10 new hospitals
by 2012; �GrupoAngeles (largest private
hospital group in Mexico) spending $700 million to build 15 hospitals in the next 3 years
Central Europe� Increased Medical Tourism Traffic
from Western Europe
Korea�New Entrants with strong
healthcare system offerings
6
Costa Rica�One in five visitors is a medical
tourist
Malaysia�Medical tourism as an
economic thrust
India�Government investing $3.6 Billion
in medical tourism infrastructure.�Estimates show Indian medical
tourism at $2.3B by 2012
offerings
Singapore�More internationally
accredited hospital facilities than any other country
Source: Frost & Sullivan

Increased Prosperity and Middle Class Consumption will Fuel Healthcare Expenditure
Other Asia9%
India4%
China2%
Japan8%
EU30%
US21%
Other26%
Middle Class Consumption (2009)
Other Asia14%
India23%
China18%
Japan4%
EU14%
US7%
Other20%
Middle Class Consumption (2030)
7
•Middle class consumption in China and India will surpass that of EU and US by 2030
•APAC will contribute to 59% of global middle class consumption by 2030, rising from 23% in 2009
•Over half of the middle class will be from the APAC region by 2020
•Both factors will be a major growth driver for HC expenditure and the growth of the HC delivery market as demand increases across the region
1810
36
22
28
53
2 26 5
0
20
40
60
80
100
2010 2020
Origins of Global Middle Class (%)
Middle East and North Africa
Sub-Saharan Africa
Asia Pacific
Central and South America
EU
North America
Source: OECD, Smith Barney, Frost & Sullivan

2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
50.0
100.0
150.0
200.0
250.0
300.0
350.0
400.0
Pe
rce
nta
ge
of
Ag
ed
65
an
d A
bo
ve
to
Tota
l Po
pu
lati
on
(%
)
Po
pu
lati
on
(M
illi
on
)By 2020, two-third of the Asia-pacific population over 65 years will have at least one chronic disease
Healthcare Industry: Population Aged 65 and Above, (Asia Pacific), 2009-2020
The Burden of Disease in elderly, Asia Pacific
8
0.0%
2.0%
-
50.0
2010 2015 2020
Pe
rce
nta
ge
of
Ag
ed
65
an
d A
bo
ve
to
Tota
l Po
pu
lati
on
(%
)
Year
Aged 65 and Above (Million)
Percentage of Aged 65 and Above to Total Population (%)
� In 2010, 7.6% (241.7 million) of the Asia Pacific population was aged 65 and above.
� By 2020, this will be more than 9.7% (333.95)
� 65.2% of those aged 65+ have one chronic condition
Source: WHO, Frost & Sullivan

HEALTHCARE SPENDING IN ASIA
9
HEALTHCARE SPENDING IN ASIA

3.9
4.1
4.34.8
5.9
7.2
6.5
8.3
8.5
9.4
16.2
Singapore
Laos
Thailand
MalaysiaCambodia
Vietnam
KoreaJapan
Australia
UKUSA
Total expenditure on health as a % of GDP, 2009
Compared with the developed countries, most Asian countries spend smaller proportion of their GPD on health…
AS
EA
N C
ou
ntr
ies
De
ve
lop
ed
C
ou
ntr
ies
10
2.6
3.4
44.2
4.6
5.5
5.8
2
2.4
2.93.8
3.9
0 2 4 6 8 10 12 14 16 18
PakistanBangladesh
Sri Lanka
IndiaChina
Bhutan
Nepal
Myanmar
Indonesia
Brunei
PhilippinesSingapore
%
Most countries in Asia spend less than 5% of their GDP on healthcare
AS
EA
N C
ou
ntr
ies
Oth
er
As
ian
C
ou
ntr
ies
Source: WHO

7.17.2
7.58.9
9.814
12.317.9
15.118.3
18.7
MalaysiaPhilippinesCambodia
Viet NamSingapore
Thailand
KoreaJapan
UKAustralia
USA
AS
EA
N C
ou
ntr
ies
De
ve
lop
ed
C
ou
ntr
ies
General government expenditure on health as a % of total government expenditure, 2009
Most developed governments spend >15% of their budgets on healthcare, while most Asian governments don’t spend half as much...
11
3.64.1
7.37.9
8.610.3
13.3
0.83.8
6.86.97.1
0 2 4 6 8 10 12 14 16 18 20
PakistanIndia
Sri LankaBangladesh
NepalChina
Bhutan
MyanmarLaos
Brunei IndonesiaMalaysia
AS
EA
N C
ou
ntr
ies
Oth
er
As
ian
C
ou
ntr
ies
%
Most Governments in Asia spend <8% of their budget on healthcare Source: WHO
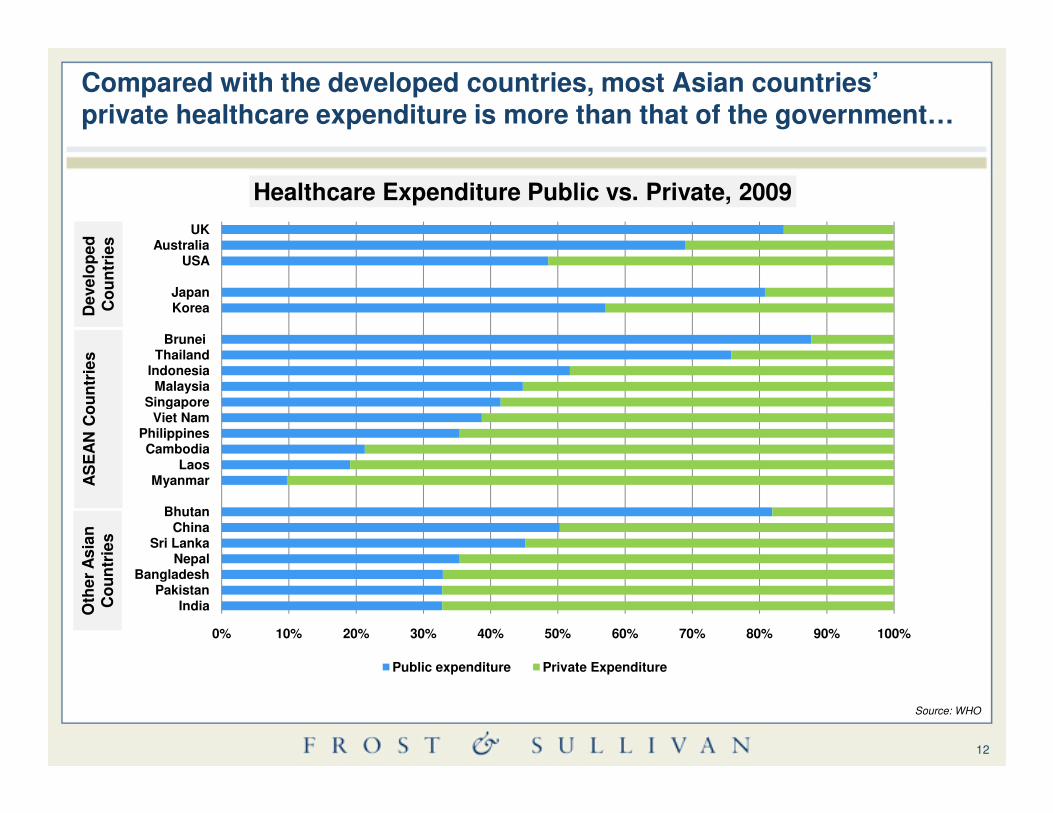
SingaporeMalaysia
IndonesiaThailand
Brunei
KoreaJapan
USAAustralia
UK
Healthcare Expenditure Public vs. Private, 2009
AS
EA
N C
ou
ntr
ies
De
ve
lop
ed
C
ou
ntr
ies
Compared with the developed countries, most Asian countries’ private healthcare expenditure is more than that of the government…
12
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
IndiaPakistan
BangladeshNepal
Sri LankaChina
Bhutan
MyanmarLaos
CambodiaPhilippines
Viet NamSingapore
Public expenditure Private Expenditure
AS
EA
N C
ou
ntr
ies
Oth
er
As
ian
C
ou
ntr
ies
Source: WHO

Viet NamSingaporeIndonesia
PhilippinesMalaysiaThailand
KoreaJapan
UKAustralia
USA
Components of Private Expenditure, 2009
AS
EA
N C
ou
ntr
ies
De
ve
lop
ed
C
ou
ntr
ies
In most Asian countries most people pay for health out-of-pocket; PHI is restricted to certain part of the societies in these countries…
13
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
BhutanPakistan
BangladeshNepalIndia
ChinaSri Lanka
CambodiaMyanmar
LaosBrunei
Viet Nam
PHI OOP Other
OOP=Out of pocket; PHI=Private Health Insurance; Others=charity, aids, etc Source: WHO
AS
EA
N C
ou
ntr
ies
Oth
er
As
ian
C
ou
ntr
ies
There is a huge potential for PHI in the Asian market…

HEALTHCARE INSURANCE
14
HEALTHCARE INSURANCE

Government PHI Out- of-pocket
15
Government PHI Out- of-pocket
• Greater bargaining power• Risk is distributed
• Monopoly• Hinders creative products and responsiveness
In countries like Canada, there is one government insurance…
Government PHI Out- of-pocket
16
Government PHI Out- of-pocket
• More choice and customization• Easier to move from one to another
• Complex to manage• Difficult for patients to understand
In countries like Egypt, there are more than one government insurance schemes, with minimal private…
Government PHI Out- of-pocket
17
Government PHI Out- of-pocket
• PPP• Core policy with top-ups
• Overlaps• Lack of coverage
In countries like the UK, there is one government insurance with multiple supplementary private players…
Government PHI Out- of-pocket
18
Government PHI Out- of-pocket
• Fosters innovation through competition
• State insurer with higher risk• Overhead duplication
In countries like the US, there is one government insurance competing with other private players…
Government PHI Out- of-pocket
19
Government PHI Out- of-pocket

• Fosters responsiveness, innovation through competition
• More complex• Overhead duplication• Risk selection (need risk-equalization)
In countries in the West Indies, there are multiple private players, with no government player…
Government PHI Out- of-pocket
20
Government PHI Out- of-pocket

Key Markets Healthcare Insurance Environments in Asia Pacific
India China Indonesia Malaysia Thailand Australia Singapore
Aging Population No Yes No Yes Yes Yes Yes
Dominant Distributer ofPHI
Life/ Non Life/ Health
Life/ Non Life/ Health
Life Life Life Health Life
Tax Incentives for PHI Yes Group No Yes No Yes Yes
Restrictions on PremiumRates
Notify No No No No Yes notify
Guaranteed Renewal Some Some No No No Yes
21
Guaranteed Renewal Some Some No No No Yes
Portability of PHI policy In Discussion No No No No Yes
Group biz as % of totalportfolio
45% 30% >20% 30% 20% <10% 25%
Minimum BenefitsSchedule
YES NO
Medical Underwritingallowed
Yes No Yes

The 3 elements of healthcare: High quality, reasonable cost, and ease of access…
Quality
Cost
Access
Situation Challenges Opportunities
Ac
ce
ss
• Increasing elderly population• Increasing medical travellers• High quality healthcare • Efficient schemes [Medisave, Medical Shield, Medifund, Eldershield]
Access constraint: • Shortage of hospital bed space (2.2/1000, ideal 3/1000)• High cost of healthcare
Improved access: Medisave covers 12 private hospitals in Malaysia; offer international medical insurance• High premium specialized packages that cover eg. BUPA Pregnancy; … preventive
22
Qu
ali
ty
Co
st
• Flat subsidy per patient of US$80 paid to the hospital/doctor regardless on the disease treated• Popular with public
• 39% population covered by government insurance, 5% covered by private; ~56% uninsured
Pregnancy; … preventive
Cost constraints: • Not sustainable as cost incurred by hospitals is higher leading to deteriorating service and quality in overburdened public hospitals• Cost constraints in other part of the world eg. Middle east, Singapore
Cost-effective options:• Packages for middle & high income groups who would prefer to pay for high quality • Opportunities for foreign (ME) insurance companies to lower their reimbursement costs [60-70% cheaper than US, 50% cheaper than Singapore
Quality constraints: • Inadequate quality; wealthy go to Malaysia and Singapore• Middle class relies on private; less pressure on the government to provide good quality healthcare
Improved quality options:•High premium packages that cover medical travel •Packages that incentivize local treatment at JCI accredited hospitals

FUTURE OF HEALTH CARE
23
FUTURE OF HEALTH CARE

From...
Provider Centric Focus Patient Centric
Centralized – Hospital Monitor De-Centralized – Shift to Community
...To
A modern healthcare system is on the horizon, demanding a paradigm shift
Healthcare Paradigm Shift
24
Invasive in general hospitals Treatment Less invasive in specialized hospitals
Treating Sickness Objective Preventing Sickness – “Wellness”
Source: Frost & Sullivan
F
M
T
O

Focus: moving from physicians to patientsF
M
T
O
25
Physician PatientsPatients are becoming:
• Aware of treatment/medicine choices
• Informed decision makers
• Responsible for their own health
Source: Frost & Sullivan

Hospital based careHospital based care Community based careCommunity based care
Innovation in hospital business models: Hospitals go virtual; development of community based care
F
M
T
O
26
Centralized model
Patient overload
Increased costs
Strain on health care resources
Decentralized model
Reduced patient load
Reduced cost
Optimum utilization of health care resources
Source: Frost & Sullivan
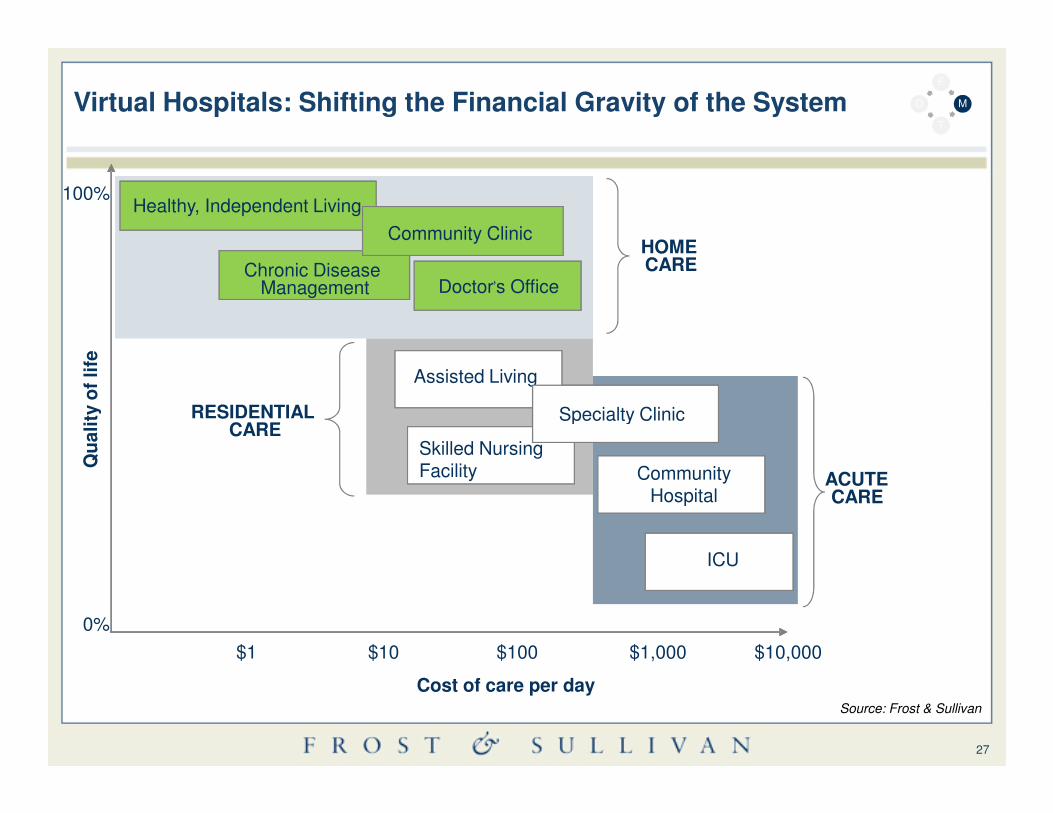
Virtual Hospitals: Shifting the Financial Gravity of the System
Healthy, Independent Living
Chronic Disease Management
Community Clinic
Doctor’s Office
100%
Assisted Living
HOME CARE
RESIDENTIAL
Qu
ali
ty o
f li
fe
Healthy, Independent Living
Chronic Disease Management
Community Clinic
Doctor’s Office
Assisted Living
Specialty Clinic
F
M
T
O
27
Cost of care per day
$1 $10 $100 $1,000 $10,000
0%
Skilled Nursing Facility
Specialty Clinic
Community Hospital
ICU
RESIDENTIAL CARE
Qu
ali
ty o
f li
fe
Skilled Nursing Facility
Specialty Clinic
Community Hospital
ICU
ACUTE CARE
Source: Frost & Sullivan
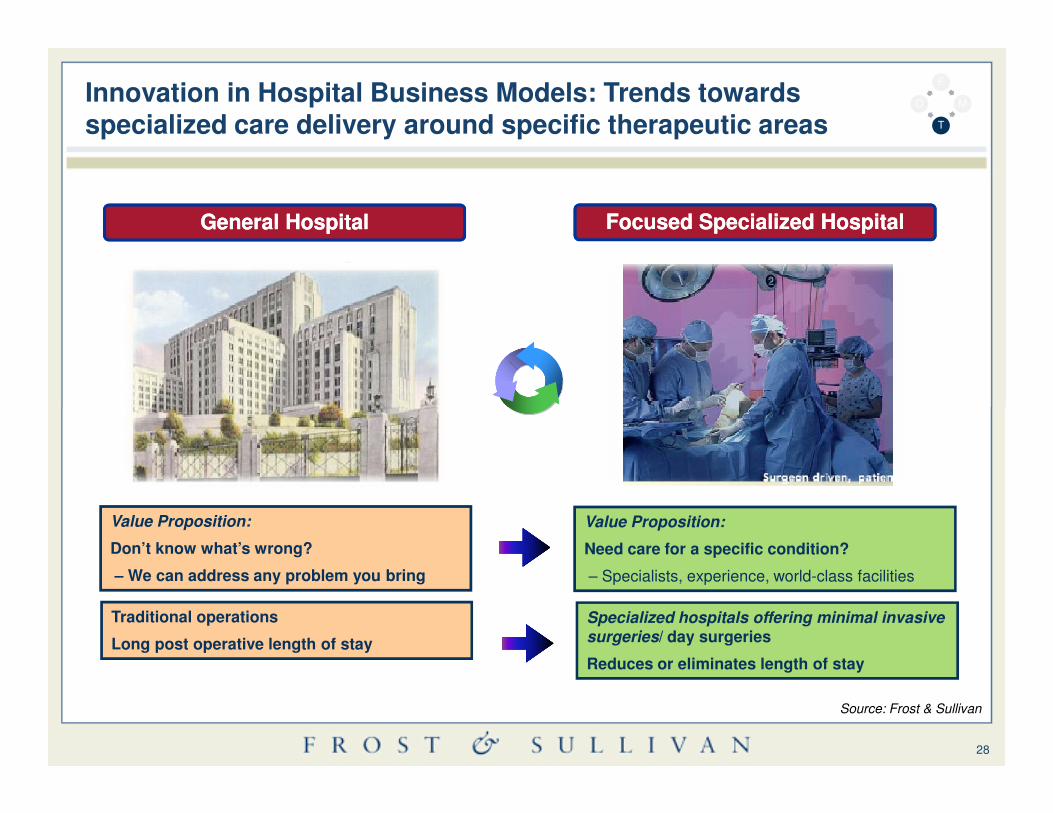
General HospitalGeneral Hospital Focused Focused Specialized HospitalSpecialized Hospital
Innovation in Hospital Business Models: Trends towards specialized care delivery around specific therapeutic areas
F
M
T
O
28
Value Proposition:
Don’t know what’s wrong?
– We can address any problem you bring
Value Proposition:
Need care for a specific condition?
– Specialists, experience, world-class facilities
Traditional operations
Long post operative length of stay
Specialized hospitals offering minimal invasive surgeries/ day surgeries
Reduces or eliminates length of stay
Source: Frost & Sullivan

Wellness of the body, the mind and the soul
Mind
Mood
Stress levels
Mental health
Sense of optimism
Attitude
Security
Safety
F
M
T
O
29
Body SoulPersonal values
Personal fulfilment
Self image / self actualization
Sight / vision
Touch & feel
Smell / breathing
Sound
Temperature
Wellness
Source: Frost & Sullivan

Why Wellness?
50% Percent of all diseases can be avoided and prevented by lifestyle changes
Only 31% of healthcare expenditure in organization is spent on direct medical costs
Medical Costs
Direct = 31%
Medical Costs
Workers
Indirect = 69%
Lost Productivity:- Absenteeism
Employee & Customer Dissatisfaction:
F
M
T
O
30
69% of medical costs are due to productivity loss
50% of all medical costs can be saved with integrated and comprehensive health management.
Workers Compensation
Salary Continuation
Dissatisfaction:- Turnover + Temporary Staffing- Poor Quality
Replacement Workers:- Training Interim Employee- Administrative re-work
75% caused by chronic diseases that are preventable
Source: An Unhealthy America: The Economic Burden of Chronic Disease, The Milken Institute Center for Health Economics
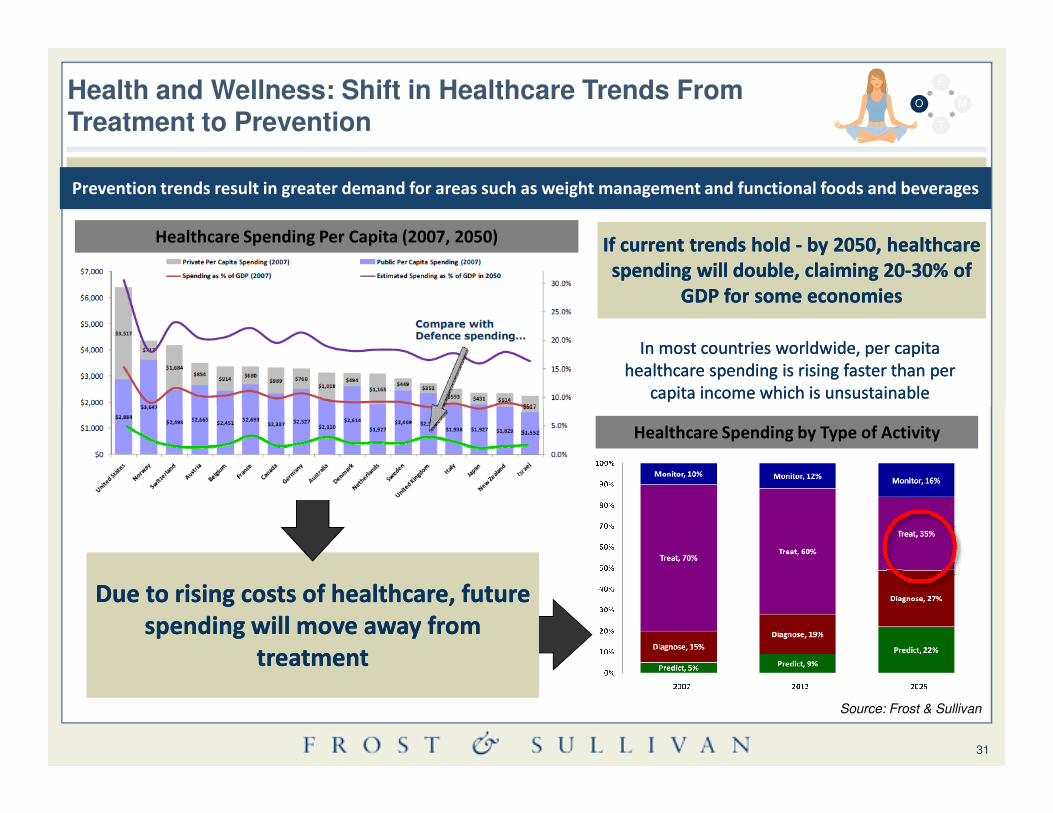
Health and Wellness: Shift in Healthcare Trends From Treatment to Prevention
Healthcare Spending Per Capita (2007, 2050)
In most countries worldwide, per capita In most countries worldwide, per capita
healthcare spending is rising faster than per healthcare spending is rising faster than per
capita income which is unsustainable capita income which is unsustainable
If current trends hold If current trends hold -- by 2050, healthcare by 2050, healthcare
spending will double, claiming 20spending will double, claiming 20--30% of 30% of
GDP for some economies GDP for some economies
Prevention trends result in greater demand for areas such as weight management and functional foods and beverages
F
M
T
O
31
Due to rising costs of healthcare, future Due to rising costs of healthcare, future
spending will move away from spending will move away from
treatment treatment
Healthcare Spending by Type of Activity
Source: Frost & Sullivan

What does that mean for the insurance companies….
From...
Provider Centric Focus Patient Centric
Centralized – Hospital Monitor De-Centralized – Shift to Community
...To
Customized Insurance products
Insurance products incentivising community care
32
Community
Invasive in general hospitals
Treatment Less invasive in specialized hospitals
Treating Sickness Objective Preventing Sickness –“Wellness”
Specialized insurance products that cover less invasive surgeries
Insurance products that cover and incentivize preventive care, regular monitoring, vaccinations, healthy habits…
The key is to manage quality, cost, and access…
Government PHI Out- of-pocket
33
Government PHI Out- of-pocket

Thank you
Dr. Milind Sabnis, MD, MBA
Principal ConsultantHealthcare, Asia [email protected]
Donna Jeremiah
Director Corporate Communications, Asia [email protected]: +61 (02) 8247 8927
34
Jessie Loh
ManagerCorporate Communications, Asia [email protected]. (65) 6890 0942
Carrie Low
ExecutiveCorporate Communications, Asia [email protected]. (603) 6204 5910