addictions 101: understanding, recognizing, and treating the disease state criminal justice...
TRANSCRIPT

Addictions 101:Understanding, Recognizing,
and Treating the Disease State
www.OverdoseFreePA.orgCriminal Justice Personnel Curricula
Core Component 1© 2014, Overdose Prevention Coalition

The OverdoseFreePA website is brought to you by the Overdose Prevention Coalition, a
collaborative between:
The Pennsylvania Department of Drug and Alcohol Programs (DDAP)
The Single County Authorities (SCAs) of:
Allegheny CountyBlair County
Bucks CountyButler County
Dauphin CountyDelaware County
Westmoreland County
The Allegheny County Medical Examiner’s Office
The Program Evaluation Research Unit, University of Pittsburgh School of Pharmacy
The project is supported by a generous grant from the Pennsylvania Commission on Crime and Delinquency.
Background Photo for Slide Set by そらみみ (Own work) [CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons

What is Substance Use Disorder (SUD)?
SUD is a broad term that includes abuse of and dependence on drugs and
alcohol.
Substance Abuse and Mental Health Services Administration (SAMHSA), 2011

SUDs
• In the U.S., an estimated 22.2 million persons aged 12 or older were classified with substance dependence or abuse in 2012.
• This represents 8.5 % of the population.
National Survey on Drug Use and Health (NSDUH), 2012

SUDs (cont’d)• Of these individuals:
– 2.8 million had dependence or abuse of both alcohol and illicit drugs.
– 4.5 million had dependence or abuse of illicit drugs but not alcohol.
– 14.9 million had dependence or abuse of alcohol but not illicit drugs.
NSDUH, 2012

Co-Occurring Disorders
Mental health disorders and SUD often co-occur.
In other words, individuals with SUD often have a mental health condition at the same time and
vice versa.
SAMHSA, 2014

Co-Occurring Disorders (cont’d)
• Co-occurring disorders can further complicate the lives of individuals with SUDs.
• Approximately 8.9 million adults are diagnosed with co-occurring disorders.
• Only 7.4% of people receive treatment for both conditions.
• 55.8 % of do not receive any treatment.
SAMHSA, 2014

Recovery = Hope
People with SUDs and their families must maintain the hope that recovery
is possible.
SAMHSA, 2012
By Walter Rumsby from Queenstown, New Zealand (Tuis in a Tree Uploaded by Richard001) [CC-BY-SA-2.0 (http://creativecommons.org/licenses/by-sa/2.0)], via Wikimedia Commons

Overdose
• An overdose means having too much of a drug or alcohol, or a mix of drugs and/or alcohol for your body to safely handle.
• Overdose can result in permanent brain damage, permanent organ damage or death.
• Overdose symptoms can look different depending what kinds of drugs were used.
DDAP, 2014; Centers for Disease Control and Prevention (CDC), 2012

What is Overdose? (cont’d)
Overdose can result from:
• Legal substances (alcohol, Tylenol®, prescription pain medications, anxiety/depression medications).
• Illegal substances (illegally obtained prescription drugs, heroin, cocaine).
• Any combination of drugs or alcohol.
International Overdose Awareness Day (IOAD), 2014

Causes of Overdose
• Almost any drug can cause an overdose in large enough quantities.
• Overdose deaths have doubled in the U.S. over the past two decades, largely because of prescription opioids.
• Physicians are the leading source of prescription opioids for users with the highest risk of adverse events.
Centers for Disease Control and Prevention (CDC), 2014; Jones, 2014

What is an Opioid?
• Opioids are typically prescribed to help manage pain.
• Vicodin, Codeine, OxyContin, Percocet, Opana, Methadone, and Fentanyl are examples of these medications.
• Some illicit drugs, like heroin, are also opioids.
Project Lifeline, 2010

Naloxone (Narcan®)
The “Overdose Antidote” can save
a person’s life during opioid overdose by reversing the
overdose in the person’s brain.
Walley, 2013
Photo: http://www.recorder.com/home/11373037-95/narcan-now-available-through-greenfield-tapestry-health-office

Naloxone (Narcan®) (cont’d)
• Naloxone must be obtained through a prescription and filled at a pharmacy.
• Naloxone will only work for an opioid overdose – it won’t work for any other type of drug overdose.
• It can be administered via an injection or as a nasal spray.
Walley, 2013

Past-Year Initiates for Specific Illicit Drugs Among Persons Age 12 or Older,
2008
Overview of Substance and Drug Use
SAMHSA, 2009

Overdose Deaths in Pennsylvania
Based on Pennsylvania Department of Health data, overdose deaths have been on the rise over the last two decades with an increase in the rate of death from 2.7 to 15.4 per thousand Pennsylvanians
DRUG OVERDOSE DEATHS IN PENNSYLVANIA
YearNumber of
DeathsPA
PopulationRate per
1,000
2011 1,909 12,742,886 15.4
2010 1,550 12,702,379 12.5
2008 1,522 12,448,279 12.6
2006 1,344 12,440,621 11.2
2004 1,278 12,406,292 10.6
2002 895 12,335,091 7.5
2000 896 12,281,054 7.4
1998 628 12,001,451 5.4
1996 630 12,056,112 5.4
1994 596 12,052,410 5.1
1992 449 11,995,405 3.8
1990 333 11,881,643 2.7
DDAP, 2014
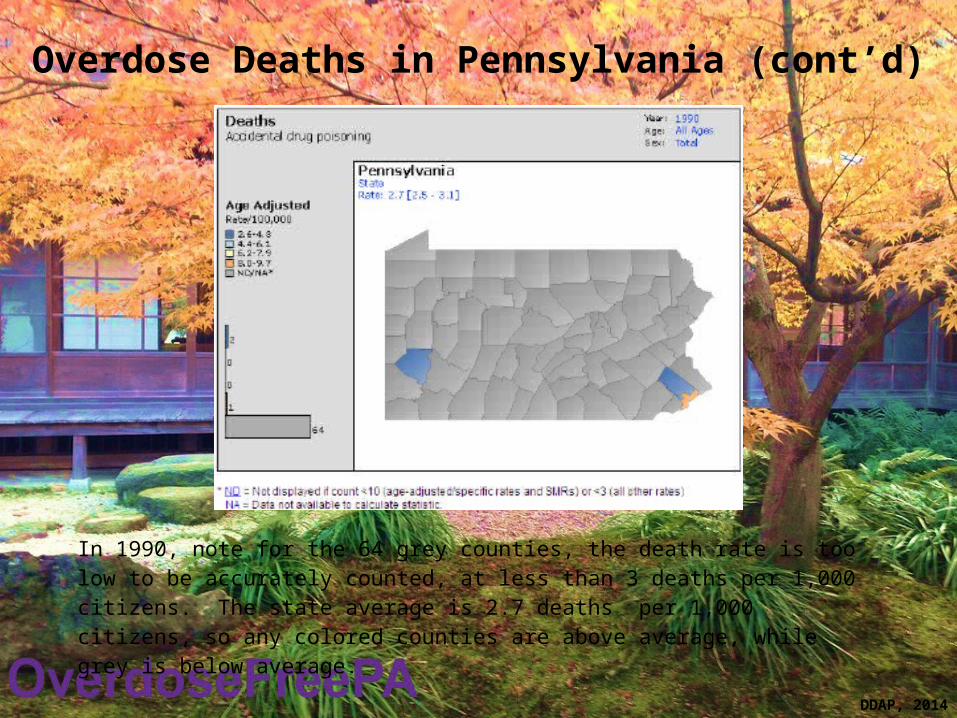
Overdose Deaths in Pennsylvania (cont’d)
In 1990, note for the 64 grey counties, the death rate is too low to be accurately counted, at less than 3 deaths per 1,000 citizens. The state average is 2.7 deaths per 1,000 citizens, so any colored counties are above average, while grey is below average.
DDAP, 2014

Overdose Deaths in Pennsylvania (cont’d)
In 2000, note for the 52 grey counties, the death rate is too low to be accurately counted, at less than 3 deaths per 1,000 citizens. The state average is 7.4 per 1,000 citizens, so the light blue, yellow and orange counties are above average, while grey and dark blue are below average.
DDAP, 2014

Why Drug Misuse Occurs
– Experimental– Social-recreational– Circumstantial-situational– Adaptive– Self-medication– Intensive– Compulsive– Unintentional

Etiology of Chemical Dependency
• Social rebellion– Peer group influence and questioning societal
values
• Symptom relief– Self medication hypothesis
• Learned behavior– Drive – cue-response – reinforcement– Tolerance – dependency-response – reinforcement
• Personality traits– Addictive personality
• Disease

Chemical Dependency: Epidemiology
Alcohol dependence• Annual Prevalence; males=10.7%, females=3.7%• Lifetime Prevalence; males 20.1%, females=8.2%
Drug dependence• Annual Prevalence; males=3.8%, females=1.9%• Lifetime Prevalence; males=9.2%, females=5.9%
Kessler, 1997

Humanistic–Reintegrate into daily life without the burdens of drug use
–Prevention of or increased compliance with treatment in coexisting risk associated diseases
–“De-stigmatize” the patient
–Increase patient’s quality of life through employability and responsibility
–Increase the quality and availability of services provided to patients

Societal
• Decrease in crime and drug diversion
• Decrease in cost burden to health care system
• Increase in work productivity and/or decrease in absenteeism

Economic
• Decrease in substance-related treatment admissions
• Decrease utilization of emergency and chronic services (trauma, HIV related, hepatitis related, TB related, social services, criminal justice)
• Cost of agonist therapy vs. cost of repeated drug treatment
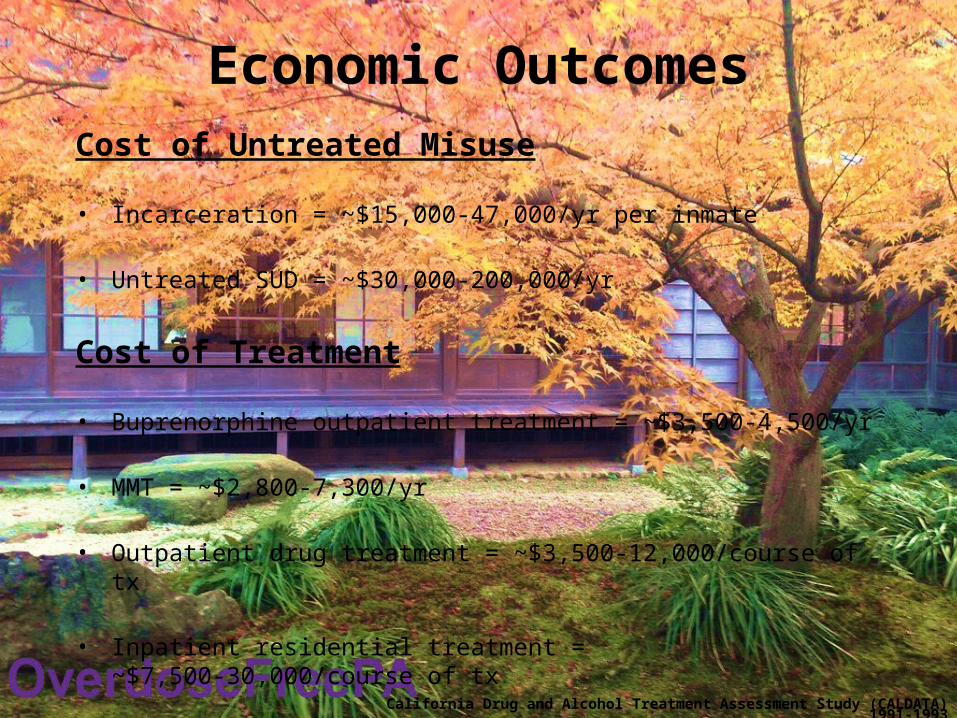
Economic OutcomesCost of Untreated Misuse
• Incarceration = ~$15,000-47,000/yr per inmate
• Untreated SUD = ~$30,000-200,000/yr
Cost of Treatment
• Buprenorphine outpatient treatment = ~$3,500-4,500/yr
• MMT = ~$2,800-7,300/yr
• Outpatient drug treatment = ~$3,500-12,000/course of tx
• Inpatient residential treatment = ~$7,500-30,000/course of tx
California Drug and Alcohol Treatment Assessment Study (CALDATA) 1991-1993

Cost Benefit of Treatment
• For every $1 spent on treatment, $7 is realized through decrease in crime, employability, decrease in utilization of emergency and social services
• Continual abstinence 3 and 5 years after treatment approached 50% for all treated patients
CALDATA, 1993

Cost Savings from SUD Services
Criminal Justice System Impact
Health System Savings