addiction and bipolar disorder - academia.cat · • patients with bipolar disorder were...
TRANSCRIPT

l
Addiction and Bipolar Disorder
Ana González-PintoIP CIBERSAM-G10
Hospital Santiago ApóstolUniversidad del País VascoCIBERSAM

SCHEME
EpidemiologyAnxiety, and alcohol and drug abusePolarity of episodes and alcohol and drug abuseUsing and quiting alcohol and drug abuse, and relation with outcomeTreating comorbidity Conclusions

Comorbid conditions: baseline data from STEP-BD
0,4
5
8
48
0 10 20 30 40 50 60
Current SubstanceUse Treatment
Current NonalcoholSUD
Current Alcohol UD
Lifetime SUD
Simon NM et al.J Clin Psychopharmacol 2004; 24(5): 512Simon NM et al.J Clin Psychopharmacol 2004; 24(5): 512--20.20.

Pharmacotherapy and comorbidity in bipolar disorder
Substance use disorders in bipolar patients
0
10
20
30
40
50
60
Current substanceuse treatment
Current nonalcoholSUD
Current alcohol UD Lifetime SUD
Patie
nts
(%)
• The STEP-BD trial examined the association between comorbidity and pharmacotherapy in patients with bipolar disorder
• A lifetime substance disorder was diagnosed in 48% of the sample; however, only 0.4% were receiving substance abuse- specific medications
• Use of ‘comorbidity-specific’ pharmacotherapy for anxiety disorders, substance use disorders, and attention deficit disorder was limited, suggesting comorbidity in bipolar disorder may be under-treated
Simon NM, et al. J Clin Psychopharmacol 2004;24:512-520SUD, substance use disorder; UD, use disorder
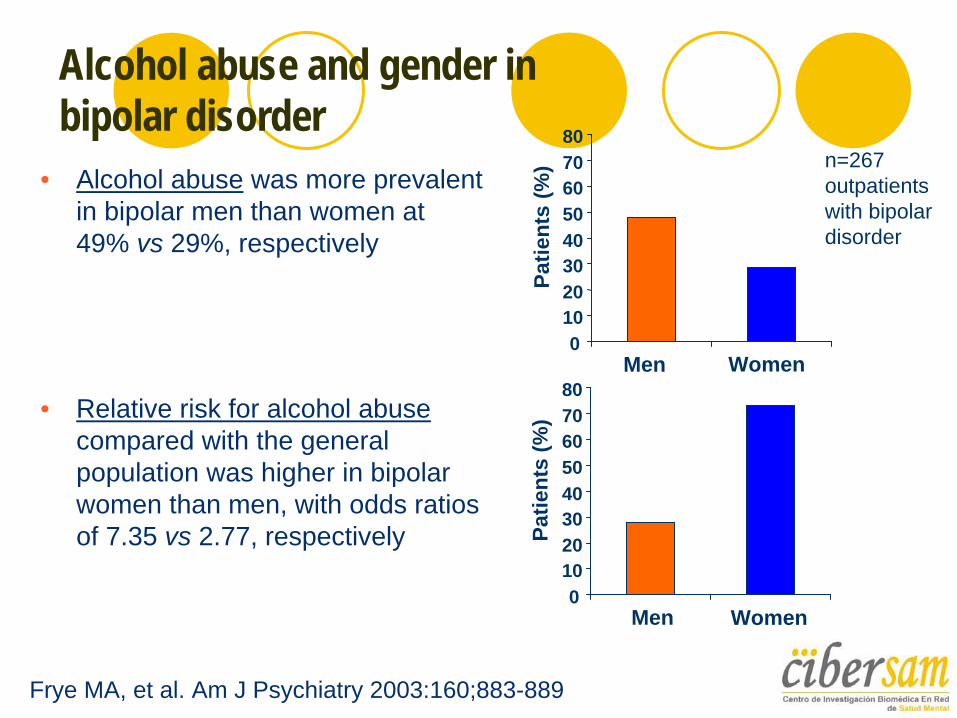
Alcohol abuse and gender in bipolar disorder
Frye MA, et al. Am J Psychiatry 2003:160;883-889
• Alcohol abuse was more prevalent in bipolar men than women at 49% vs 29%, respectively
Men Women
n=267 outpatients with bipolar disorder
• Relative risk for alcohol abuse compared with the general population was higher in bipolar women than men, with odds ratios of 7.35 vs 2.77, respectively
Men Women0
1020304050607080
Patie
nts
(%)
01020304050607080
Patie
nts
(%)

Substance abuse in Mania: EMBLEM study data
Alcohol (25%)More compulsory admissionsMore rapid cyclingMore abuse of other substances
Cannabis (14%)Greater severityMore psychosisMore hospitalizationsMore compulsory admissionsMore abuse of alcohol and other substancesMore first episodes
EMBLEM. N=3536 manic patients across Europe. Haro et al, in 2006; Goetz et al, 2007; Vieta et al 2007.

Clinical characteristics of bipolar patients with versus those without substance and/or alcohol abuse
• More mixed episodes and rapid cycling• Slower recovery• More hospitalisations• Earlier age of onset• More suicide attempts• Increased aggressivity/criminality• Poor treatment adherence: 75% of non adherent
patients were substace users (González-Pinto et al, 2006)
Keller MB, et al. JAMA 1986;n. Vieta E, et al. Bipolar Disord 2001;. Colom F, et al. J Clin Psychiatry 2000;González-Pinto et al.,Bipolar Disord 2006
0
50
100
Adherent
Substance abuse

Effect of compliance to lithium prophylaxis on bipolar disorder
0
10
20
30
40
50
60
70
80
Substanceabuse
Married Women Suicidalacts
Patie
nts
(%)
Compliant Non-compliant
• Up to 10 years of lithium prophylaxis demonstrated a 5.2-fold greater risk of suicide attempts among patients with poor compliance vs those compliant with treatment
• Non-adherence was significantly associated with:– Being male– Being unmarried– Having a history of comorbid
substance use– Having breakthrough episodes– Having psychiatric hospitalisation
Gonzalez-Pinto A, et al. Bipolar Disord 2006;8:618-624
** * *
* p≤0.002
• At 10 years, poor treatment compliance was significantly associated with risk of suicidal acts (p=0.016)
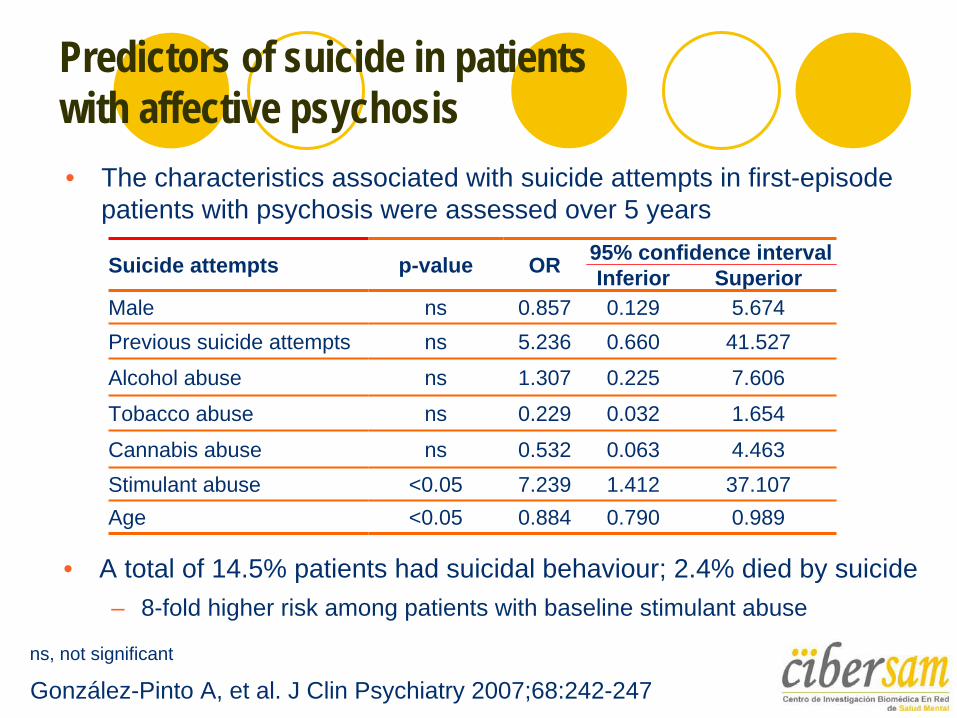
Predictors of suicide in patients with affective psychosis• The characteristics associated with suicide attempts in first-episode
patients with psychosis were assessed over 5 years
Suicide attempts p-value OR 95% confidence intervalInferior Superior
Male ns 0.857 0.129 5.674Previous suicide attempts ns 5.236 0.660 41.527
Alcohol abuse ns 1.307 0.225 7.606
Tobacco abuse ns 0.229 0.032 1.654
Cannabis abuse ns 0.532 0.063 4.463Stimulant abuse <0.05 7.239 1.412 37.107Age <0.05 0.884 0.790 0.989
• A total of 14.5% patients had suicidal behaviour; 2.4% died by suicide– 8-fold higher risk among patients with baseline stimulant abuse
González-Pinto A, et al. J Clin Psychiatry 2007;68:242-247ns, not significant

Reasons for comorbidity between bipolar disorder and substance abuse
Genetic diathesisGenetic diathesis with a common mediator (anxiety)Common neurobiological mechanisms (dopamine, etc.)Overlap of diagnostic criteriaSocial diathesisSelf-medicationTreatment side-effectsInduction of mania or depression by substances
Vieta E, presented at the IX Symposium on Bipolar Disorders, Barcelona, Spain, Januar

Comorbid anxiety disorders in bipolar patients with alcohol and substance use
Anxiety disorders are more common in bipolar disorder patients with alcohol abuse vs patients with cocaine abuse2
Patients with early onset anxiety disorders have an increased lifetime prevalence of bipolar disorder3
1. Mitchell JD, et al. J Affect Disord 2007;102:281-2872. Goldstein BI, et al. J Affect Disord 2007;103:187-195



Antidepressant-induced mania in bipolar patients with substance misuse• Patients with bipolar disorder were interviewed to investigate the
relationship between psychoactive substance use and mania
• Patients with a history of substance abuse and/or dependence had a significantly greater risk of mania than those with no such history (OR=6.99, p=0.007)
Reproduced with permissionGoldberg JF, Whiteside JE. J Clin Psychiatry 2002;63:791-795
Variable Present Absent p-value
Female, n (%) 12/21 (57.1) 19/32 (59.4) 1.000Age at illness onset, mean years (SD) 20.7 (11.9) 18.1 (8.8) 0.532
Comorbid substance abuse/dependence, n (%) 12/20 (60.0) 5/28 (17.8) 0.005
Depressed polarity at first episode, n (%) 19/20 (95.0) 22/27 (81.4) 0.221
Bipolar II, n (%) 8/19 (42.1) 10/25 (40.0) 0.887Antidepressant trials/year, estimated mean (SD) 0.20 (0.14) 0.12 (0.10) 0.041Bipolar family history, n (%) 10/18 (56) 10/22 (46) 0.525

A new specifier: Predominant polarity
Depressive polarity60% bipolar patientsMore bipolar IIMore depressive onsetMore seasonal patternMore suicide attemptsBetter long-term response to lamotrigineMore antidepressant use
Manic polarity40% bipolar patientsMore bipolar IMore manic onsetYounger and earlier onsetMore substance misuseBetter long-term response to atypical antipsychotics
Colom F, Vieta E, Daban C, Pacchiarotti I, Sánchez-Moreno J. Clinical implications of predominant polarity in bipolar disorder. J Affect Disord, 2006.
Polarity is also related to tretament

Ten years follow-up of 169 bipolar patients. Depressive polarity:
More relapses.More hospitalizations.More suicide attempts
More difficulties in quitting .
González-Pinto y cols., J Affect Dis 2009

González-Pinto y cols., J Affect Dis (2009)

González-Pinto y cols., J Affect Dis 2009

LONG TERM IMPROVEMENT AFTER CANNABIS WITHDRAWAL
G Pinto et al. Schizophrenia Bull., 2009

Lithium for adolescent bipolar disorders with secondary substance dependency
• 25 adolescent patients with bipolar disorder and SSD received lithium or placebo • Randomised, double-blind, placebo-controlled pilot study
• Addiction to both alcohol and cannabis was the most frequent category of SSD• The mean scheduled weekly serum lithium level of active responders was
0.9 mEq/L • Lithium treatment significantly improved:
• Psychopathology measures• Weekly random urine drug assays
• The mean 6-year interval between the onset of BD and onset of SDD strongly suggested that early recognition of BD may enable effective prevention of comorbid substance dependency
Geller B, et al. J Am Acad Child Adolesc Psychiatry 1998;97:171-178BD, bipolar disorder; SDD, substance dependency disorder

Add-on valproate semisodium in bipolar I disorder with alcohol abuse
n=59, 44 male, mean age 38 yearsRecently detoxedBRMS 15.3, HRSD-25 20.8All received lithium; valproate semisodium vs placebo added for 24 weeksValproate semisodium improved % heavy drinking days, drinks per heavy drinking day (HD), time to relapse
Salloum IM, et al. Arch Gen Psychiatry 2005;62:37-45
0 20 40 60 80
Heavy drinking days (%)
No. drinks per HD
Days to relapse
Lithium + placeboLithium + valproate semisodium
BRMS, Bech-Rafaelsen Mania Scale; HRSD-25, Hamilton Rating Scale for Depression

ValproateBoth groups improved equally on mania and depression scoresCompared with placebo group. Divalproex (valproate) group had
Fewer heavy-drinking daysFewer drinks per heavy-drinking dayFewer drinks per drinking day
Outcome was correlate with complianceDivalproex group had better liver function test scores
Salloum IM et al. Arch Gen Psychiatry 2005; 62(1): 37-45.


Efficacy of naltrexone in patients with bipolar disorder and alcoholism• A 16-week, open-label pilot study was conducted to assess the effect
of naltrexone in patients with bipolar disorder and alcohol dependence • Assessments included:
• 17-item Hamilton Rating Scale for Depression (HRSD-17)• Young Mania Rating Scale (YMRS)• Brief Psychiatric Rating Scale (BPRS)• Alcohol craving scale
• Significant improvement observed in HRSD-17, YMRS and days of alcohol use and craving
• Other drugs tried in small, open label studies for bipolar disorder with substance abuse, include gabapentin, lamotrigine, quetiapine and aripiprazole
Brown ES, et al. Depress Anxiety 2006;23:492-495

Group therapy for bipolar disorder and substance dependence
A RCT assessed integrated group therapy (addresses the two disorders simultaneously) vs group drug counselling (focused on substance use)
62 patients with bipolar disorder and current substance
Intention-to-treat analysis showed:
Significantly fewer days of substance use for integrated group therapy vs drug counselling during treatment and follow-up
Number of weeks ill with bipolar disorder during treatment and follow-up similar in both groups
More depressive and manic symptoms in integrated group therapy patients vs drug counselling patients
Data suggest that integrated group therapy is a promising approach to reduce substance use in patients with bipolar disorder
Weiss RD, et al. Am J Psychiatry 2007;164:100-107RCT, randomised controlled trial

J Clin Psychiatry 2000; 61: 361J Clin Psychiatry 2000; 61: 361--367.367.

Am J Psychiatry 2007; 164:100–107.

Group Therapy
Population21 adults received integrated group therapy24 adults received usual care
Integrated group therapy was associated withSignificantly (p<0,02) greater decrease in Addiction Severety Index drug and alcohol composite scoresHigher probability of longer (at least 2-month or 3-month) periods of abstinence

Conclusions
The prevalence of substance use disorders is very high in patients with bipolar disorderSubstance use comorbidity carries worse outcome of bipolar disorderBipolar patients with substance misuse have higher suicide risk and less adherence to treatmentAnxiety is frequently a mediator between alcohol and drug abuse and bipolar disorderTreatment of anxiety is crucial, but antidepressants are associated with induced mania in BD with comorbid SUD

Conclusions
Evidence-base for treatment is limited, but withdrawal improves dramatically outcome in the long, but not in the short-term.Valproate, lithium, and naltrexone can be used to treat bipolar patients with substance use disordersPsycoeducation and psychosocial interventions are crucial for patients with comorbidity

CHRISTMAS LUNCH