adapting modern electronic health records to telehealth ... · adapting modern electronic health...
TRANSCRIPT

Adapting Modern Electronic Health Records to TeleHealthand new Healthcare Delivery Models
HIMSS Annual ConferenceChicago, Illinois
April 2015
Michael Minear, M.S., CHCIO, CPHIMSChief Information Officer

Speaker Disclosure
I have no personal financial relationships or interests in any entity producing, marketing, re-selling, or distribution health care goods and services consumed by, or used on patients.
Michael N. Minear, CHCIO, CPHIMS
Professional Affiliations
Chief Information Officer – University of California -Davis Health System
Associate Faculty - Johns Hopkins Bloomberg School of Public Health
Currently a member of - Board of Directors – California Telehealth Network (2012 – current)
Member - Healthcare Information & Management Systems Society (HIMSS)
Member - American College of Healthcare Information Administrators (CHIME)
Member - American Medical Informatics Association (AMIA)
Member of the American College of Clinical Engineering (ACCE)
2

Presentation Outline
1. Overview of UC Davis and the UC Davis Health System
2. UCDHS Information Technology
3. UCDHS Telehealth Program
4. Online Clinical Knowledge
5. Stages of Telehealth
6. Questions
3

1. Overview of the University of California Davis

Where is Davis California? A 1-4 hours drive from…
Napa image, winecountry.comLake Tahoe image, Tahoebest.comYosemite Valley image, NY TimesSan Francisco image, wall paper innBig Sur image, Stan Russell
SacramentoDavis
Lake Tahoe
Yosemite
Big Sur
San Francisco
Napa Valley
5

California Drought
Image, cironline.orgDrought impact map, U.S. Drought Monitor weekly report Road sign image, NBC NewsCalifornia agriculture statistics, Beachcalifornia.com
California has been the number one food and agricultural producer in the United States for more than 50 consecutive years
Over half of America’s fruit, nuts, and vegetables Produce more dairy products than any other state Leading export crop is almonds 80% of US ripe olives Leading producer of strawberries Nationally, products exclusively grown (99% or more) in
California include almonds, artichokes, dates, figs, kiwifruit, olives, persimmons, pistachios, prunes, raisins, clovers, and walnuts
California Drought Produces Tastier Wine Grapes
6

Member of 10-campus University of California system
Part of 6 campus UC health
UC Davis is the 9th ranked US public research university College of Agricultural & Environmental
Sciences ranked #1 in the world Ranked #1 in US for Veterinary Medicine Health System has 14 nationally ranked
clinical specialty programs
University of California Davis
UC Davis UniquenessHuman, Animal, Plant

UCDHS - ‘Improving lives and transforming health care’
Clinical Care− Leapfrog Hospital Group Top Hospital
award – 2013 and 2014
Research− $200+ million in annual funding− 34th ranking NIH research funding
(ranked 62nd in 2001)
Education− SOM ranked 24th for primary care Ranked 42nd for research
− Betty Irene Moore School of Nursing
8

UC Davis Health System and Medical Center
National Cancer Institute ‘comprehensive’ designation cancer center, one of only 41 in the country
UC Davis School of Medicine ranks among the nation's top medical schools for rural medicine, primary care and research
UC Davis Medical Center is nationally ranked in 10 adult and 4 pediatric specialties
‘A’ rating on the Leapfrog Group’s most recent Hospital Safety Score
Leapfrog Hospital Group Top Hospital award – 2013 and 2014 as one of the nation’s highest performing hospitals
Magnet recognized for quality patient care, nursing excellence and innovations in professional nursing practice

2. UC Davis Health System Information Technology
10
Information Technology
CCH
IT
Office of the National Coordinator
Cert
ifie
d EH
R
ICD-10-CM
phen
otyp
eEHR
LOINC
HITECH Act
EHR Certification
HIE
Accountable Care Act
Genotype
HL7
Meaningful Use
Online clinical knowledge
CPOE

UCDHS Information Technology Division
Annual operating budget of $105 million, annual capital budgets ranging from $11 million - $70 million depending on projects
Staffing - 430 FTE
Computing 1,314 servers (majority are virtual) 12,587 client computers 910 computers on mobile carts 620 mobile computers for BCMA 4,200 network attached printers
Networking and communications 45,000 IP network nodes 10 Gb links to CENIC, Internet, and Internet2 12,475 voice hand sets 4,195 Vocera VoIP badges, 4,105 pagers
Software Applications 488 applications in production use 220 interfaces
Primary and secondary data centers
13,500 faculty, staff, student customers
112,000 patient customers
2.3 million patient records
Half a billion clinic fact records
Shared 58,000+ medical records
Shared 6.5 billion ePrescription records
All types of clinical encounters
Clinical research
Clinical education
11

UC Davis Health System – Clinical Software Infrastructure
Specialty Clinical Software Radiology information System Transcription / Voice Recognition Radiation Oncology Pathology Dietary Pulmonary Function Holter Muse EKG Echo EMG – orders Respiratory care – orders Treadmill CAPS TPN pharmacy admixture
Clinical Equipment Pyxis Drug cabinets Hemodynamic monitors Telemetry EKG Fetal monitoring Echo Glucose Point of Care Cardiac Cath Monitors Bar code medication admin Digital Infusion pumps Bladder Scanner Ventilators
Paper Medical Records Scanned and Linked into EHR
Consent formsOutside paper medical recordsOnBase document management system
Digital Clinical Images Radiology – Philips PACS Ophthalmology PACS – Anka Endoscope PACS – nStream Outside Clinical Images loaded to
Radiology PACS via PACSGear Non Radiology PACS images TeleHealth Store & Forward Radiation Oncology PACS - Teremedica Pathology PACS - Aperio
In Production | In Process | Not yet started
Secondary Use EHR Content NIH i2b2 Cohort Discovery Many disease Registries:
Cardiology Burn Trauma Cancer Many others…
Tethered Meta Registry
InterfacedWith EHR:
Legend
Epic Electronic Health Record
(EHR)
Tethered Personal Health Record
12

UC Davis Health System – Clinical Software Infrastructure
Specialty Clinical Software
Clinical Equipment
Paper Clinical Records Scanned and Linked into EHR
Digital Clinical ImagesSecondary Use EHR Content
Epic EHR
2.3 million patient records
500+ million detail fact records
Fully digital Clinical records
3 PACS linkedto EHR
6 years of Experience
Tethered Meta Registry
Tethered Personal Health Record112,000+ patients
Millions of highly detailed
clinical data points
All clinical encounters in the EHR:inpatient, ED, ambulatory, home health, Telehealth
220 Production interfaces
13

Key Measures of UCDHS EHR Use
Epic EHR Clinical Encounter Support− 100% of Inpatient, Ambulatory, ED, Home Health, and Telehealth encounters
supported by EHR Inpatient CPOE
− 94.6% of inpatient clinical orders entered via CPOE− 96.9% of ED clinical orders entered via CPOE− 761+ order sets in production use − Pediatric and investigational chemotherapy and TPN only orders not done via CPOE
ePrescribing− All 5 federally mandated ePrescribing interfaces in use 6.5 million+ records shared
Online Clinical Documentation− Over 409 templates in production use− Over 335 physicians use voice recognition to create their clinical notes− 93.5% of inpatient notes and 91.5% of ambulatory clinical notes are created
through online documentation templates Epic is the foundational system to store patient data
− Now have over 2.3 million unique patients stored in Epic
14

UC Davis Health System is one of only 14 care providing organizations in the US that has earned both the Davies award and achieved Stage 7 in the EMR Adoption Model
UCDHS IT Awards
The HIMSS Nicholas E. Davies Award of Excellence recognizes outstanding achievement of organizations who have utilized health information technology to substantially improve patient outcomes while achieving return on investment
Healthcare organizations that attain Stage 7 of the EMR Adoption Model (EMRAM) demonstrate superior implementation and utilization of health IT systems. Their achievement has resulted in the true sharing, information exchange and immediate delivery of patient data to improve process performance, quality of care and safety
Most Wired hospitals have the highest level of Information Technology adoption. UCDHS has been named a Most Wired hospital in 2011, 2012, 2013, and 2014

3. UCDHS Center for Health and Technology

University of California Davis - Center for Health and Technology
The Center for Health and Technology's (CHT) Telehealth Program, was founded in 1992 by Dr. Thomas Nesbitt
CHT provides direct clinical care to patients at a distance
Since the inception of the program real-time consultation services have been offered in more than forty specialties linked to over 100 clinics and hospitals, the majority of which are located in, or provide services to rural areas
Dr. Nesbitt Center for Health & Technology
17

Telemedicine
Medically underserved areas in California have historically had inadequate geographic access to health care specialists. This disparity in access has led to adverse results for patients who might have otherwise had excellent outcomes
Through telemedicine, patients do not have to leave their community and can gain access to specialists located hundreds of miles away− The consultative model provides a bi-directional education and
communication occurring between the primary care provider and the specialist
− The primary care provider remains responsible for the patient's treatment plan which results in an improved coordination of care.
18

Pediatric Intensive Care Unit (PICU) Model
Telemedicine consultations from UCDHS specialists for critically ill pediatric patients in a rural ICU− Mortality and length of stay outcomes were equivalent to PICU
benchmarks− High satisfaction with the quality of care among physicians, parents,
and nurses
Marcin J, et al. (2004).Use of telemedicine to provide pediatric critical care inpatient consultations to underserved rural Northern California. J Pediatrics.144(3):375-80.
UC Davis PICU Rural California ICU
19

Simulation-based Education
UC Davis has trained nearly 1,875 community-based health care providers and administrators at CHT facility in Sacramento− Trained over 1,500 participants who have taken courses at the American
Telemedicine Association (ATA) Conferences− Created ehealth curriculum used internationally
Over 100,000 simulation-based education hours and over 32,000 learners with 8,271 hours last year
Safe environment for inter-professional learning Problem-based learning to improve patient outcomes
20

4. Evidence-based Clinical Knowledge Impacting Care
21
Evidence-based knowledge
EHR and Process Change
ImprovedClinical Results+ =

UC Davis Sepsis Collaborative Project
Priority goal defined by leadership UC Health goal Funding by the Gordon and Betty
Moore Foundation Large team that met twice weekly
for 6 months− 50+ clinicians - MD, RN, PharmD− Non-clinicians - lab, IT, quality
improvement− Multiple care settings - acute, ICU,
ER) met twice monthly for 6 months
Clear goal and Support Leadership and Communication
22

Sepsis Project Elements
Dellinger RP, et al. Critical Care Medicine. 2008; 36: 296-327
Evidence-based Knowledge Process / clinical workflow
Example clinical process changes Rapid turn around Lactic acid tests Nurses enter vitals into EHR 10 min or less Some clinical orders fire auto from data Clinical decisions made quickly or are escalated
17+ years to disseminate new knowledge… 23

Sepsis Project Elements
Policy changes EHR changes
Alerts Order setsRulesClinical documentation templates
24

Sepsis Measurement
Population Data and Visualization Results
Sepsis Registry In Tethered Meta Registry4137332925211713951
70.0%
60.0%
50.0%
40.0%
30.0%
20.0%
10.0%
0.0%
Observation (months)
Mor
talit
y Ra
te
_X=26.7%
2009 2010 2011 2012
SIC Mortality Rate by Calendar YearSevere Sepsis (995.92) and Septic Shock (785.52)
*Source Data from HIM
Since the 2009 baseline, UCDHS has reduced Sepsis Mortality by 36%...
The actual or observed rate for all sepsis related mortality was reduced over the course of about 1.5 years and has been maintained and still decreasing at a lower rate for 3+ years
Applying these techniques to other clinical goals… 25

5. Stages of Telehealth
26

Phase 1 - Vison
In the February 1925 issue of Science and Invention,
Hugo Gernsback wrote an article sharing his vision of the ‘teledactyl’ to support doctors to see their patients through a view screen and also touch them via robot arms
He effectively predicted telemedicine
Novak, M. (2012). Telemedicine Predicted in 1925. Smithsonium.com. Accessed from http://www.smithsonianmag.com/history/telemedicine-predicted-in-1925-124140942/?no-ist
1
27

Teledactyl’s Distant Controls
Novak, M. (2012). Telemedicine Predicted in 1925. Smithsonium.com. Accessed from http://www.smithsonianmag.com/history/telemedicine-predicted-in-1925-124140942/?no-ist
28

Gernsback’s Vision of teledactyl vs. da Vinci Surgical Robot
Novak, M. (2012). Telemedicine Predicted in 1925. Smithsonium.com. Accessed from http://www.smithsonianmag.com/history/telemedicine-predicted-in-1925-124140942/?no-istSurgery Robot Image – The Bethencourt Group. Cardiac & Thoracic Surgery, http://bethencourtgroup.com/500th-robotic-heart-surgery-performed-by-dr-bethencourt-on-his-birthday/
da Vinci Robotic surgery - 2015
Gernsback’s vison of the teledactyl - 1925
29

Phase 2 – Piloting
For many years people and technologies were focused on delivering the vision of telemedicine
Value was created and lessons learned
Many technical barriers – did not have: − High speed ubiquitous networks− Client devices with high speed computing and quality
resolution− Mobile technologies− Security technologies to protect transmissions− Integration of clinical equipment integrated with video and
networks (stethoscope, otoscope, testing devices…)− Ability to share patient records − Scheduling and process support for follow-up care and referrals
across continuum− Low cost technologies
Top Image, EMSWORLDBottom Image, In the Center, employee and student publication, the University of Kansas Medical Center
2
30

Piloting
Operational and legal barriers also existed: (at least in the US)− Clinician licensure across geographic boundaries (states)− Financial reimbursement for telemedicine encounters− Regulation and legal− Vested interests
The barriers limited the use of telemedicine
Right Image, ATT.comMiddle and Right Image, Howard Reis, Healthepractices 31
Nurse recording clinical encounter on TV camera at Boston Logan airport and transmitting to Mass General Hospital-1967
31

Phase 3 – Conversion to Digital
Healthcare has been trying to eliminate the paper medical record for many years
For 30+ years most care providers still used paper records augmented by partial clinical automation
Care providers are now moving to a fully digital record and finally eliminating paper records and film based clinical images− UC Davis achieved fully digital records in 2012 − All paper records removed from hospital− When patients bring in paper records from other care providers they
are quickly scanned and linked to UC Davis EHR
Achieving fully digital records is critical to telemedicine and other new types of encounters− The foundation for digital encounters− For many years at UC Davis this highest cost of providing a
telemedicine encounter was copying and faxing patient records
3
32

Phase 4 - Integration
Early clinical software was designed for one department− Pathology, Radiology, Ambulatory clinic, many others…
Niche software designs were the norm− Built to support a single function and/or department− Not designed to share data with other software
Huge challenges to share patient data within a single care provider With modern EHR software product suites, interface engines, and
improved standards – many organizations share clinical data well, typically using the EHR as the integration foundation
The UC Davis Health System has achieved almost total integration of clinical data − And an average of 127.4 million interface transactions per month− Takes a dedicated team of 21 FTEs UC Davis Health System
4
33

Why is Sharing Clinical Data Important?
Patients have many clinicians and transitions of care
In American healthcare, clinical care is provided by many clinicians in many different locations. During the years 2000-2002, the typical Medicare patient was treated by a median of 7 different physicians (2 primary care physicians and 5 specialists) who were located in 4 different offices each year. Patients with chronic illnesses were treated by even more physicians (Pham, et al, 2007)
51% of primary care encounters involved care transitions (excluding radiology and pathology encounters) between individual physicians, where 36% - 41% of visits involved transitions between different medical groups (Rudin, et al, 2011).
A Canadian study found that patient information was often not shared with other physicians treating the same patient, and found that patient information about previous visits was not available 88% of the time (van Walraven, et al, 2008).
Only 19% of hospitals reported in 2010 that they exchanged patient clinical information electronically with providers outside their system (Kirtane, 2012).
Only 13% of US hospitals exchanged information with other hospitals (not in their system), and only 28% of hospitals exchanged with ambulatory providers outside of their system (Agency for Healthcare Research and Quality, 2011).
34

But Current HIT Designs – Mostly Designed for one Organization
Many issues – separate organizational structures, competition, staff focus, standards, some legal barriers, software design…make it much harder to share data between organizations
All vendor EHRs are proprietary and closed software infrastructures
Data sharing standards only facilitate sharing clinical data between two different software applications – not fully integrate clinical data
Massive efforts have focused on creating effective clinical data sharing between organizations− Federal HITECH EHR meaningful use regulations− HITSP standards setting for US
HIT must support communities and populations not just an organization
Care Provider A Care Provider B Care Provider C
35

UC Davis Patient Records Shared with Other Providers
Health Information Exchange critical to clinical workflows and to avoid duplicate testing (valuable for Telehealth, referrals, and transfers)
Required by Federal HITECH regulations
0
500
1000
1500
2000
2500
3000
3500
UC Davis Health SystemContinuity of Care Documents (CCD) or Equivalent
Shared with other ProvidersDecember 2010 through March 2015
OCHIN
Kaiser North
All Other Providers
Veterans Affairs
Sutter Health
Social SecurityAdministration
58,000+ full patient records shared36

Other Care Providers UC Davis has Shared Patient Records With
# Organization Location
Other Providers Initiated
Total
UCDHS Initiated
TotalTotal
1 SUTTER HEALTH and AFFILIATES Sacramento, CA 9,086 27,838 36,924
2 KAISER PERMANENTE NORTHERN CALIFORNIA Northern CA 4,249 4,143 8,392
3 U.S. SOCIAL SECURITY ADMINISTRATION Washington, DC 6,388 - 6,388 4 DIGNITY HEALTH, MERCY HOSPITALS IN SACRAMENTO Sacramento, CA 51 1,726 1,777 5 VETERANS AFFAIRS (VA) UNITED STATES 1,215 79 1,294
6 UCSF MEDICAL CENTER San Francisco, CA 540 331 871
7 OCHIN ACROSS U.S. 501 142 643
8 STANFORD HOSPITAL & CLINICS Stanford, CA 303 178 481
9 KAISER PERMANENTE SOUTHERN CALIFORNIA SOUTHERN CA 15 133 148
10 STANFORD CHILDREN'S HEALTH Stanford, CA 76 26 102 779 57,799 Total
Total for all other care providers
104 organizations
37

Phase 5- Digital Clinical Care Environment
There has been a dream for many years to create a fully digital and integrated clinical care environment− There are many versions and opinions on what this may look like
Technology and care processes must be designed to support the full continuum of care
Home, WorkTraveling Nursing Home Clinic
EmergencyRoom
Hospital Critical CareUnit
Rural Urban
Poor Rich
5
38

Move away from specialty and organization centric designs
1. Put the patient at the center and focus on HIT design and connect clinicians/care teams with patients/families
2. Integrate all clinical data about a patient to support each clinical encounter and analytics
3. Apply evidence-based clinical knowledge through advanced analytics and decision models to support every care encounter and to proactively assess a patient’s or population’s health status and support relevant interventions
39

Future Care Scenarios
Cancer Diagnosis1. Patient receives a diagnosis of cancer2. Phenotype data fully integrated with genotype data3. Advanced analytics used to assess patient’s clinical data and unique
genotype to suggest optimal treatments fully tailored to that patient’s genotype mutations and create and help deliver am optimized plan of care
2 year old has sore throat at 3AM in the morning1. Patient has bad throat pain – parents use iPad to access child’s clinical data
and inputs new symptoms2. EHR uses guidelines to suggest parents use consumer home testing kit most
parents use at home to take throat swab, results transmitted to EHR3. EHR with embedded analytics diagnosis strep throat, suggests at home
treatment, automatically orders antibiotics to nearest all-night pharmacy, Dad drives to pharmacy to pick up the drug
Less about telemedicine, or mobile technologies, or EHRs…more about a complete digital health environment
or Digital Clinical Ecosystem40

Leverage EHR, PHR, Video, and Mobile Technologies
EHR to EHR telemedicine consult− Provider to provider, or to patient within one EHR
eConsult via video or messaging with urgent care type provider− Patient to urgent care center via video or secure message
Video encounters within tethered PHR− Patient to physician or nurse using PHR linked to EHR
Clinical call center encounters− Patient or family to clinical call center encounter
Patient and provider communication and data sharing through tethered PHR− Patient to Physician and care team via secure message
Store and forward − Specific clinical content such as retinal scan sent to ophthalmologist or
video psychiatric encounter sent to psychiatrist for review − Connection to Withings, Fitbit, or Apple Health Kit
41
Other EHR, PHR, Video, and Mobile Use Cases
Remote monitoring of ICU or other care provision− Dedicated video and connections to clinical monitors to monitor critical care
patients
Inpatient consults− Physician to physician or nurse to support inpatient care
Specialty video support – Tele Stroke, Tele Psych, Tele Derm− Providers broader service coverage often replacing local specialty care often
to support emergency department environments
Home monitoring− Video connection and collection of targeted clinical data elements for patient
support at home
Tele interpretation service− Provides remote language interpretation support for a clinical encounter
Mobile telemedicine (iPad, iPhone, Android)− Multiple mobile platforms supporting patients & providers to access EHR/ PHR
Social media− Use of social media tools for patient education and group support
42

Consumer Health Management Technologies
Scanadu Scanaflo™ - urine test kit in development that will empower people to monitor their health at home
AliveECG App
Electronic Sensors Printed Directly on the Skin
John Rogers, a materials scientist at the University of Illinois at Urbana-Champaign
Fitbit
Apple Health Kit
43
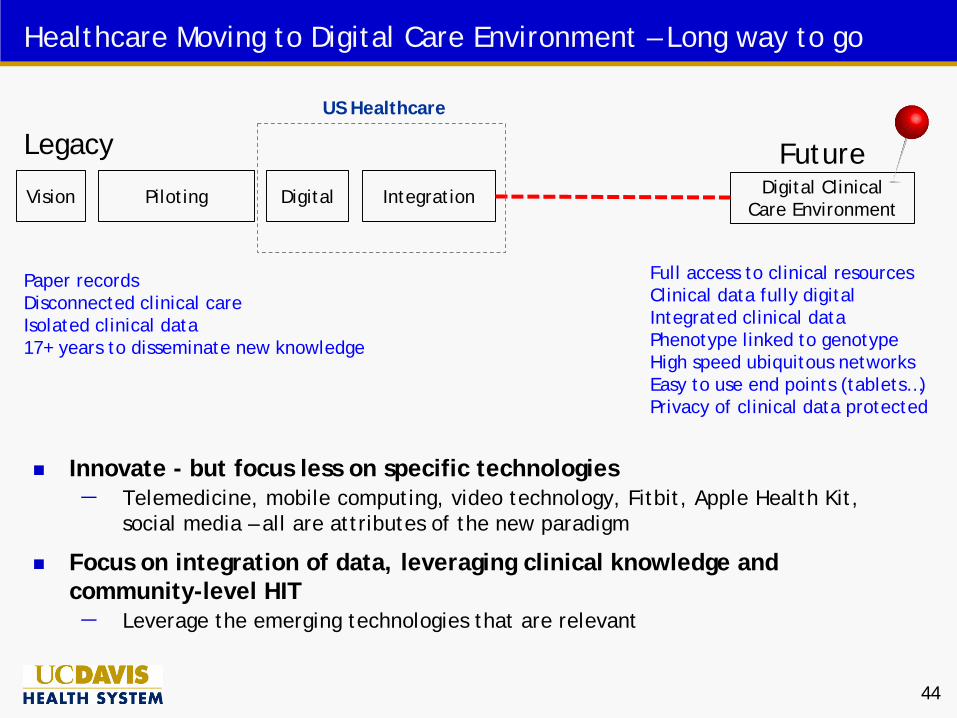
Healthcare Moving to Digital Care Environment – Long way to go
FutureVision
Paper recordsDisconnected clinical careIsolated clinical data17+ years to disseminate new knowledge
Piloting Digital Integration Digital Clinical Care Environment
Full access to clinical resourcesClinical data fully digitalIntegrated clinical dataPhenotype linked to genotypeHigh speed ubiquitous networksEasy to use end points (tablets…)Privacy of clinical data protected
Legacy
Innovate - but focus less on specific technologies − Telemedicine, mobile computing, video technology, Fitbit, Apple Health Kit,
social media – all are attributes of the new paradigm
Focus on integration of data, leveraging clinical knowledge and community-level HIT − Leverage the emerging technologies that are relevant
US Healthcare
44

6. Questions
?

References
Agency for Healthcare Research and Quality. (2011). National Healthcare Quality Report, 2011, Chapter 6, Care Coordination. AHRQ site on HHS website. Retrieved August 15, 2012 from http://www.ahrq.gov/qual/nhqr11/chap6.htm
Kirtane, J. (quoting the American Hospital Association - Hospital Survey, 2010). (2012) Putting the IT in Transitions: An Update from the Office of the National Coordinator for Health IT. Retrieved August 16, 2012 from http://www.techandaging.org/ASA_Care_Transitions_Technologies_Presentation.pdf
Pham, H., Schrag, D., O’Malley, A., Wu, B., Bach, P. (2007). Care Patterns in Medicare and Their Implications for Pay for Performance. The New England Journal of Medicine 356, 1130-1139.
Rudin, R., Salzberg, C., Szolovits, P., Volk, L., Simon, S., Bates, D. (2011. Care transitions as opportunities for clinicians to use data exchange services: how often do they occur? Journal of the American Medical Informatics Association. 18(6), 853-858.
Van Walraven, et al. (2008). Information Exchange among physicians caring for the same patient in the community. Canadian Medical Association Journal. 179(10), 1013-1018.
46

End