acute ulcerativeendocarditis— briefresume … resume of the pathol-ogy of eight cases. ludwig...
TRANSCRIPT

Acute Ulcerative Endocarditis—A Brief Resume of the Path-
ology of Eight Cases.
Presented, with specimens, to the Illinois State Medical Society,May 17,1893.
BYLUDWIG HEKTOEN, M.D.
CHICAGO.
Reprinted from the‘‘Journal of the American Medical Association,”June 10, 1893.
CHICAGO:PUBLISHED AT THE OFFICE OP THE ASSOCIATION.
1893.


ACUTE ULCERATIVE ENDOCARDITIS ABRIEF RESUME OF THE PATHOL-
OGY OF EIGHT CASES.
LUDWIG HEKTOEN, M.D.CHICAGO.
The following eight cases of malignant or acuteulcerative endocarditis, the heart lesion of each ofwhich I have the honor to present to this society,occurred in the Cook County Hospital during thefifteen months ending April 1, 1893.
I wish to extend my thanks to all the members ofthe staff through whose hands these cases havepassed from time to time for their gracious permis-sion to utilize the material in this way; individualmention of names would embarrass the necessaryconcentration aimed at in this report.
These cases illustrate well the various forms ofacute ulcerative endocarditis from an etiological,clinical, as well as anatomical standpoint and theyparticularly emphasize the difficulties so frequentlyencountered in the diagnosis of this affection.
The cases are arranged in the following groups:I. One instance of primary endocarditis of a nor-
mal value.11. Two instances of acute ulceration developing
upon the sclerotic valves without any known infec-tion atrium.
111. Two instances of ulcerative endocarditis with

2
external lesions; in one infection of healthy valves,in the second infection of a sclerotic valve.
IV. Three instances of malignant endocarditisarising during the course of infectious processes else-where in the body.
GROUP I.
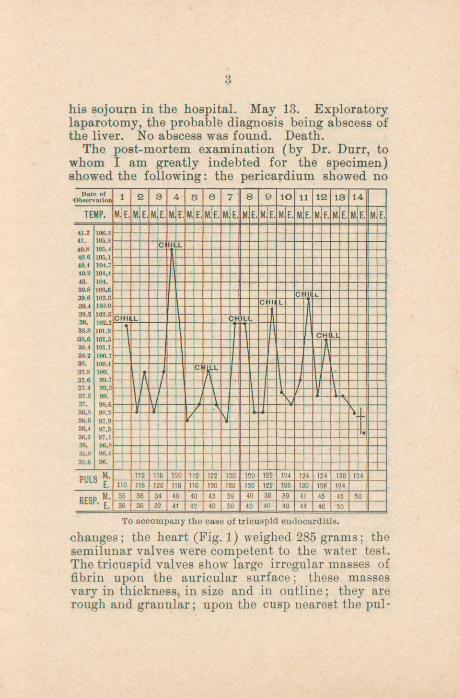
1. Primary Malignant Endocarditis of TricuspidValves; Pidmonary Infarct; Chills and IntermittentFever.—Man, aged twenty-eight, molder; enteredthe county hospital, April 29, 1892. His family andpersonal history was negative; he had always en-joyed good health ; he was taken ill six weeks beforeadmission with pain in the back, chills and vomiting;since that time there had been almost daily chillsfollowed by sweats. On entrance he was found tobe jaundiced, his skin showing numerous scratches.His pulse was 100, respiration 35, temperature 102.Over the lower lobe of the left lung there was dull-ness, bronchial breathing, crepitant rales; He lungswere otherwise negative on examination. There wasnothing unusual noticed about the heart. The liverand spleen were apparently normal. May 2. Crep-itant rales over left lung in mammary and infra-mammary regions, while in the axillary regionsthere were moist rales, broncho-vesicular respirationand some loss of resonance. May 6, Patient is dulland stupid; there are a few moist rales over leftlower lobe. May 11. Is getting weaker, has lostweight; the skin is dark and muddy, the sclerayellow; the spleen is palpable. The heart soundsappear normal, there is no increase in the area ofdullness. The upper border of the liver reaches thesixth sterno-costal junction and a little below costalarch. The bones and joints are normal. There ispain over the liver. There is constipation. Theannexed chart shows the pulse, respiration and tem-perature as well as the chills that occurred during
3
his sojourn in the hospital. May 13. Exploratorylaparotomy, the probable diagnosis being abscess ofthe liver. No abscess was found. Death.
The post-mortem examination (by Dr. Durr, towhom I am greatly indebted for the specimen)showed the following: the pericardium showed no
To accompany the case of tricuspid endocarditis.
changes; the heart (Fig. 1) weighed 285 grams; thesemilunar valves were competent to the water test.The tricuspid valves show large irregular masses offibrin upon the auricular surface; these massesvary in thickness, in size and in outline; they arerough and granular; upon the cusp nearest the pul-

4
monary orifice is a large mass, about one cm. inheight, projecting into auricle; in the center of thesummit of this mass is an irregular opening leadinginto a cavity formed by the aneurismal bulging orsacculation of the valve out into the auricle. Nearthis aneurism is a smaller one, two mm.in diameter,without any thrombatic deposits about the margins ;
many minute perforations and quite marked areasof ulceration can be made out in the endocardiumunder the thrombotic masses already described. Inboth pleural cavities were extensive fibrous adhe-sions. In the lower part of the left upper lobe was asolid, red wedge-shaped area over which there was afibrinous pleuritis. The other organs showed nogross changes.
GROUP 11.
1. Fibrous Endocarditis ofAortic and Mitral Valves;Acute Ulceration of Aortic Segments.—Colored man,teamster, forty-eight years old, had syphilis attwenty-eight; passed through an attack of rheuma-tism in the fall of 1891, but nothing could be learnedas to the character and duration of this illness; wasadmitted into the Cook County Hospital (homoeo-pathic service), February 17,1892, after a sickness offour weeks with swelling of the lower extremities andthe abdomen, scanty urine, anorexia, constipationand insomnia. The examination showed a mitralregurgitant murmur, much ascites, much oedema,and considerable dyspnoea. He died February 27th,1892, without having had any fever or other symp-toms of acute infection while in the hospital.
The post-mortem examination showed oedema,ascites, hydrothorax, compression atelectasis of theright lung, cyanotic atrophy of the liver, chronicgastro-adenitis, passive congestion of the spleen andthe following changes in the heart: it weighs 502grams and appears equally enlarged as to both ven-

5
tricles; there are no external changes; the endocar-dium in the right half is negative; the aortic valvesare incompetent to the water test; the mitral orificeadmits two finger tips; the free margins of this valveare thickened, rounded, stiff, fibrous and the cordactendinese are also stiff and thick, but there are no re-cent vegetations. The aortic valves are muchchanged (Fig 2) ; the free margins are thickenedandretracted and projecting from the ventricular sur-faces near the free edges are long, filamentous, fibrin-ous masses; in the intercoronary segment is a per-foration, about four mm. in diameter, with a crater-shaped mass of fibrin and calcareous granules aroundthe ventricular margins; upon the center of the ante-rior mitral leaflet is a mass of granular thromboticdeposit corresponding to the point where the marginsof the valve aneurism would touch the endocardiumduring systole. Finally there is a small loss of sub-stance in the endocardium below theattached marginof the perforated aortic cusp. The myocardiumshowed no other changes except those of hyper-trophy and dilatation already referred to. It wasnot possible to demonstrate any bacteria in the mar-gins of the valvular aneurism.
2. Chronic Changes in the Aortic Valves; Acute Ulcer-ative Aortic Endocarditis. Rupture of Acute Aneurismof Membranous Part of Interventicular Septum.—Man,age thirty, was admitted withhistory of having beensick for five weeks, but any accurate idea as to thenature of the disease could not be obtained. Hewas in a chill at the time of admission and ausculta-tion showed a rubbing, systolic murmur over theheart which could be followed into the great vessels ;
he had a high temperature, rapid pulse and respira-tion, and appeared moribund from exhaustion.Death after twenty-four hours. The post-mortem ex-amination showed the following changes in the heart:It was considerably increased in size, weighing 450

6
grams; the aortic valves were incompetent to thewater-test; the free margins of these valves werethick, stiff and retracted; upon their ventricularsurfaces were large fibrinous masses adherent tonecrotic areas in the endocardium; the thromboticdeposits were most marked upon the intercoronarysegment and in the mural endocardium immediatelybelow the attached margin of this valve was an open-ing surrounded by an irregular fibrinous mass; thisopening led into an aneurismal sacculation of themembranous part of the inter-ventricularseptum orundefended space which projected into the right aur-icle between the valves; upon its summit was a per-foration whose margins were covered with a hugefibrinous excrescence. In the spleen were threecharacteristic, medium sized, anaemic infarcts with-out any evidence of commencing suppurative soft-ening. The other organs in the body were macro-scopically normal with the exception of a few pleu-ritic fibrous adhesions and cloudy swelling in thekid-neys and the liver. Micrococci were found in thesections made from the aortic valves and the aneur-ism of the membranous part of the septum, but nocultivation experiments were made.
group in.
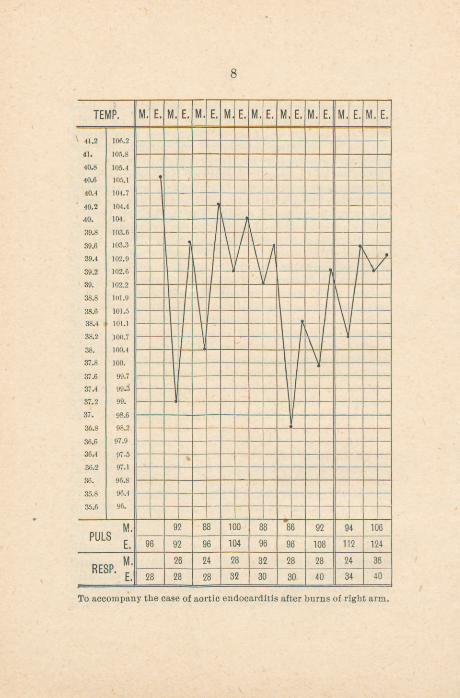
1. Fibrous Endocarditis of Aortic Valves; Superfi-cial Burn of Right Arm; Acute Aortic Ulceration;Sero-fibrinous Pericarditis.—Man, aged twenty-four,received a superficial burn of the right arm for whichhe was admitted to the hospital the next day. Thearm was enclosed in a wet boric acid dressing andthree days later this was changed to a boric acid andbismuth dusting powder, the burn being nearlyhealed. On the same day the patient was seizedwithheadaches ; he had chills ; the temperature wentup to 105.2, and there appeared severe pain in thelower part of left chest. The patient was transferred

7
to the medical service of Dr. R. H. Babcock; herephysical examination showed the man to be fairlywell nourished; dullness on percussion over upperportion of left lung anteriorly; auscultation did notyield any satisfactoryresult according to the record;the urine had a specific gravity of 1024, contained noalbumin and microscopic examination was negative.The pulse, respiration and temperature can be stud-ied from the annexed chart. Death Feb. 11, 1892.
The autopsy showed an anatomically typical acutesero-fibrinous pericarditis; a chronic aortic endo-carditis with thickening and retraction of the freemargins, valvular insufficiency, and some hyper-trophy and dilatation of the left ventricle, the heartweighing 480 grams. Upon the left coronary cuspwas a large mass of fibrin and crumbling materialcovering the ventricular surface, and in the centerof this area was a small perforation; the adjacentportion of the intercoronary leaflet showed a similarcondition with a smaller perforation ; in the myo-cardium just below the joint attachment of thesetwo valves was a small necrotic area and the intimalining the sinus valvular behind the left coronarycusp presented a gray, soft necrotic appearance. Nobacteriological examination was made.
2. Gangrene of Foot from Frost; Pulmonary Abscess;Acute Ulcerative Endocarditis; Septic Renal Infarct;Streptococci and Staphylococci in the Tissues.—Man,aged thirty-three, wr as admitted under Dr. J. B.Murphy’s care on Feb. 12, 1893, for frozen left foot;the foot was gangrenous and foul, and on Feb. 15the foot was amputated in front of ankle joint, theline of demarcation being fairly well developed. Thepatient at the time appeared to be suffering fromsaprsemic symptoms and on the 16th there was noteddullness over the upper right lobe in front and alsoconsiderable cough. At this time the temperaturewas 105, the pulse 108, respiration 38 and the record
8
To accompany the case of aortic endocarditisafter burns of right arm.

Fig.2,
Fig,4,
THEJOURNAL
OFTHE
AMERICANMEDICAL
ASSOCIATION.
Fig,I.
Fig.3.


9
shows the temperature to have remained high withsome morning intermissions until death occurred,Feb. 22, the pulse increasing in frequency. Thestump did not during life appear otherwise thanpursuing an aseptic healing. After death there wasfound the following:
The stump was free from suppuration and there wasno thrombo-phlebitis in its vicinity. In the rightupper lobe was found a cavity as large as a hen’segg, filled with thin, yellow, purulent fluid, withoutany distinct communication with the bronchi, thewall being quite thick, containing soft yellow foci.In the heart, which was otherwise quite normal, theaortic valves showed large thrombotic masses uponthe ventricular surfaces, quite firmly attached tonecrotic areas in the endocardium. The right kidneycontained a wedge-shaped infarct which was in pro-cess of purulent disintegration. There was an acutesplenic tumor.
Coyer glass preparations from the lung abscess, theaortic valves, and the softened infarct showed cocciin large numbers and especially streptococci; inocu-lation of gelatine and agar tubes produced cul-tures of staphylococcus aureus and streptococcus.Sections from the valves and from the wall of thepulmonary infarct, stained according to Gram orwith Loffler’s methylene blue, showed cocci in largenumbers, frequently arranged in rows; the sectionsof the valves, stained by other methods as well,showed the characteristic changes of acute ulcera-tive endocarditis.
GROUP IV.
1. Acute Malignant Endocarditis of Mitral ValvesSecondary to Lobar Pneumonia.—A man, forty-fiveyears old, was admitted moribund from a fibrinouspneumonia of the lobes of both lungs. The post-mortem examination showed the lower lobe of the

10
right lung to be in the stage of gray while the lowerleft lobe was in that of red pneumonic hepatization;there was also a fibrous, retracting endocarditis ofthe free aortic valve margins with valvular insuffi-ciency, hypertrophy and dilatation of the left ven-tricle. Upon the auricular surface of the mitralvalves were massive deposits of fibrin upon a necro-tic endocardium (Fig. 3) and in one place there wasa circular perforation of the valve, one cm. in diame-ter, which was covered with fibrin. There were noevidences of embolism in any of the organs. Unfor-tunately decomposition had so far advanced at thetime of the autopsy that no bacteriological examina-tion was attempted.
2. Lobar Pneumonia; Right Empysema; Operation;Acute Ulcerative Endocarditis of Aortic Valve Segmentand Adjacent Endocardium.—Man, porter, age thirty-eight, admitted February 28, 1893, with followinghistory ; He drinks beer and whisky every day; hehad pleurisy three months ago and malaria severalyears back. The present illness commenced eightdays ago with fever, cough, pain in upper part ofchest but now in lower right side; he can’t take adeep breath; has had no chill; the expectorationhas been white and yellow. Examination shows afairly well nourished man; conjunctivse a little yel-low, tongue clean, tremulous; respiration short andcatchy; over lung are numerous moist rales and overright lower lobe posteriorly are tine crackling rales.Pulse 108, temperature 102, respiration 32 on admis-sion. On March 8, the temperature had graduallyreached the normal figure, pulse was then 68, respir-ation 28. In two days there is noticed a slight even-ing temperature elevation ; on March 16, the temper-ature at 8 a. m. was 100, at 8 p. m. 102.6 and itcontinued at about this range until the 23d when thediagnosis of right empysema was made and the pa-tient was transferred to the surgical service of Dr.

11
Murphy where a portion of the sixth rib was re-moved just below the angle of the right scapula, thepleura incised with escape of pus, and drainage tubeinserted. The patient’s condition at the end of theoperation is noted as very poor and on the 25th ofMarch he died.
The autopsy showed two encapsulated pus massesin the upper posterior part of the cavity not reachedby the drainage tube; some atelectasis of the rightlung ; complete fibrous obliteration of the left pleuralcavity and a small area of broncho-pneumonia in thelower left lobe; also adhesions between the liver andthe diaphragm. In the heart the intercornary aorticsegment showed upon the ventricular aspect a crumb-ling, gray, friable mass, one cm. in height, two cm. indiameter with a crater-shaped opening into a valvu-lar aneurismal cavity; the endocardium below theattached margin of the valve was necrotic andcrumbling and showed irregular openings leadinginto spaces in the wall of the ventricle without anyperforations into any of the neighboring cavities;upon the auricular surface of the anterior mitral seg-ment was a small thrombotic deposit on a necroticarea in the endocardium which may be connectedwith the lesions described about the aortic valve;otherwise the heart was normal; it weighed 240grams. In each kidney was a small anaemic infarctwhich in the left kidney had commenced to disinteg-rate. There was an acute splenic tumor and thesolid organs showed parenchymatous degeneration.The bacteriological examination showed in the ne-crotic, mural and valvular endocardium both strep-cococci and staphylococci and also a bacillus whichappeared like the bacterium coli commune.
8. Acute Leptomeningitis; Ulcerative Endocarditis ofAortic Valves.—A man, thirty years old, was admittedunconscious with the history of becoming suddenlyill the previous day; his pulse was 120, temperature
12
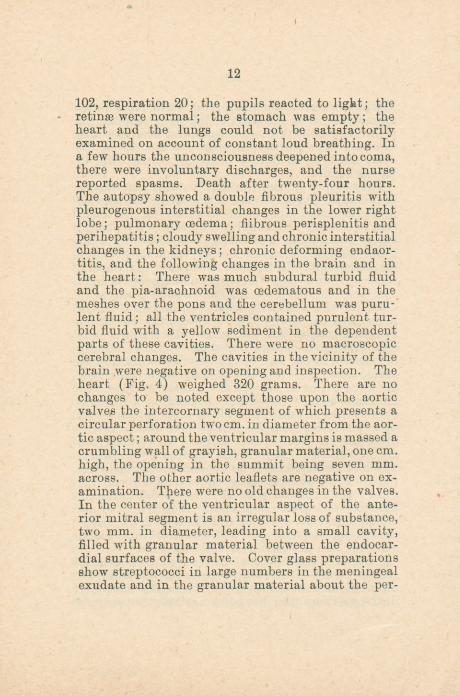
102, respiration 20; the pupils reacted to light; theretinae were normal; the stomach was empty; theheart and the lungs could not be satisfactorilyexamined on account of constant loud breathing. Ina few hours the unconsciousness deepened into coma,there were involuntary discharges, and the nursereported spasms. Death after twenty-four hours.The autopsy showed a double fibrous pleuritis withpleurogenous interstitial changes in the lower rightlobe; pulmonary oedema; fiibrous perisplenitis andperihepatitis ; cloudy swelling and chronic interstitialchanges in the kidneys ; chronic deforming endaor-titis, and the following changes in the brain and inthe heart: There was much subdural turbid fluidand the pia-arachnoid was cedematous and in themeshes over the pons and the cerebellum was puru-lent fluid; all the ventricles contained purulent tur-bid fluid with a yellow sediment in the dependentparts of these cavities. There were no macroscopiccerebral changes. The cavities in the vicinity of thebrain were negative on opening and inspection. Theheart (Fig. 4) weighed 320 grams. There are nochanges to be noted except those upon the aorticvalves the intercornary segment of which presents acircular perforation two cm. in diameter from the aor-tic aspect; around theventricular margins is massed acrumbling wall of grayish, granular material, one cm.high, the opening in the summit being seven mm.across. The other aortic leaflets are negative on ex-amination. There were no old changes in the valves.In the center of the ventricular aspect of the ante-rior mitral segment is an irregular loss of substance,two mm. in diameter, leading into a small cavity,filled with granular material between the endocar-dial surfaces of the valve. Cover glass preparationsshow streptococci in large numbers in the meningealexudate and in the granular material about the per-
foration in theaortic valve. No culture experimentswere made.
ResumS:—Of these eight cases the instance of tri-cuspid endocarditis appears to be, as far as observa-tions go, an example of primary or cryptogeneticdisease of the healthy tricuspid valves. There aretwo cases of the not so very infrequent engraftmentof an acute ulcerative process upon the scleroticvalves of chronic heart disease without the knownpresence of any wound, septic process or acute infec-tious disease. Then there are two cases connectedwith external lesions through which the infectionmight have occurred; in one the probable atrium wasa superficial burn, but this case was further compli-cated by a sero-fibrinous pericarditis whose exactrelation to the malignant endocarditis can not atthis time be established; in the second case it isquite clear that a streptococcus infection took placefrom a gangrenous foot causing a pulmonary abscess,acute aortic ulceration, and a suppurative anaemicrenal infarct.
The three remaining cases are associated withacute diseases elsewhere in the body; one with adouble fibrinous pneumonia, one with an acute lep-tomeningitis, the infection comingfrom an unknownsource; the third case of thiskind occurred in a manwho died with the diagnosis of empysema followinglobar pneumonia.
All the cases occurred in men belonging to thelaboring class; the youngest being twenty-four, theoldest fifty years of age.
There was one instance of tricuspid and one ofmitral disease: in the other six cases the aorticvalves were primarily involved and in three themural endocardium showed areas of necrosis andulceration which, in one instance led to the produc-tion of an aneurism of the undefended space andrupture into the right auricle; in one case the aorta

14
was attacked by the extension of the process fromone of the valves. It is also of interest to note thespot of vegetation or necrosis in the center of theventricular surface of the anterior mitral flap whereit would come in contact with the vegetating mass oraneurismal bulging of the aortic valves; this spotconsequently appears to be due to contact infectionand was present in three of the six instances of aor-tic disease. In three of the aortic cases the valveswere the seat of a chronic endocarditis upon whichthe acute process implanted itself; in one of thesecases the bacteriologic examination failed to revealany bacteria and it would seem that the inflamma-tory and necrotic changes in the endocardium hadfallen into temporary or permanent quiet suggestingthe probability of recovery from the acute symptoms;this corresponds well with the clinical facts in thecase which show that the patient died from theeffects of an uncompensated valvular lesion ratherthan from an acute infection (Group I, Case I). Inone of these instances of acute, destructive changesdeveloping upon sclerotic valves was a history ofprevious attack;of rheumatic fever obtained, to whichthe chronic endocarditis could be traced.
Otherwise the anatomic and histologic changespresented by these specimens are so typical andcharacteristic of ulcerative endocarditis as to requirelittle elucidation; they show vegetative and necroticchanges in profusion with the production of typicalvalvular aneurisms and subsequent rupture. It isquite noticeable that in only four of the cases werethere evidences of embolism and infarcts and herethe embolic changes were quite limited; as a rulethe showers of infected emboli from the endocardialvegetations and ulcerations constitute a strikingfeature in the clinical as well as the anatomic man-ifestations of this form of endocarditis.
A number of facts and considerations in regard to

15
the etiology and pathology of acute ulcerative endo-carditis may be summarized as follows :
1. The disease is caused by the localization ofmicrobes in the blood upon the endocardium. Thestreptococcus pyogenes, the micrococcus lanceolatus(pneumococcus), the staphylococcus pyogenes arefound most frequently and in the order named.Various other microbes have been found also, suchas the pus microbes, the bacterium coli commune,the gonococcus, the bacillus typhosus, as well asbacteria that have not been found in other diseasesand are in so far as yet peculiar to malignant endo-carditis. Recently the bacillus diphtherias wasfound in the endocardial lesion (Howard, J. Hopk.Hosp. Bull., April, 1893). Experimentally the dis-ease can be produced by first causing some mechan-ical or chemical injury to the valvular endocardiumand subsequently injecting cultures of various bac-teria into the blood, or by intravenous injections ofcultures of staphylococcus pyogenes aureus on potatosuspended in water with scrapings from the potatowhen the micrococcous agglomerations attach them-selves to the endocardium more readily than thesingle cocci (Rosenbach, Wyssokowitch, Weichsel-baum, Prudden, Frankel and Sanger, Netter, Gerar-ieu, Ribbert).
2. Acute ulcerative endocarditis is met with as asecondary lesion in the acute infectious diseases,notably and most frequently pneumonia, also inmeningitis, acute articular rheumatism, the specificfevers, gonorrhoea, dysentery and so on. It is fre-quently incorporated into suppurative, septic andpysemic processes. Finally it may occur as a pri-mary or cryptogenetic affection, developing withoutany known or demonstrable infection atrium. Fromthe mycotic endocardial foci, microbes and infectedfragments may be carried away by the blood currentand give rise to embolism in the various parts of

16
the body, local necroses, and secondary pus accu-mulations.
3. In over one-half of the cases (three-fourthsaccording to Osier), the acute ulceration is implant-ed on an old valvular lesion, the absence of endo-thelium and the roughness presenting assailablepoints for microbic invasion. This is the onlycompetent reason for the occurrence of an over-whelming majority of the instances in the left heartbut the explanation is not complete, because of thecases affecting primarily healthy valves; over two-thirds occur in the left side and about one-third inthe right half.*
EXPLANATION OF PLATE :
Fig. 1. Acute ulcerative endocarditis of tricuspid valvewith rupture of valve aneurism through which match hasbeen passed. Group I.
Fig. 2. Acute ulcerative endocarditis engrafted on scle-rotic aortic valves; perforated aneurism; necrotic spot incenter of anterior mitral flap. Chronic mitral endocar-ditis. Group 11, Case I.
Fig. 3. Acute ulcerative endocarditis of mitral valvesfollowing lobar pneumonia. Group IV, Case I.
Fig. 4. Acute ulcerative endocarditis of aortic valves;ruptured aneurism; necrotic spot in center of anteriorcusp. Group IV, Case 8. Acute leptomeningitis.
*Out of seventy-eight cases of ulcerative endocarditis of healthyvalves, twenty-four were right sided and fifty-four left sided.
Note.—ln Hamilton’s Text-Book of Pathology, Vol. I. will be foundreferences to the more important literature on ulcerative or malignantendocarditis.

