acute management of spinal cord injury · acute management of spinal cord injury dan rutigliano,...
TRANSCRIPT

Acute Management of Spinal Cord Injury
Dan Rutigliano, D.ODirector of Inpatient Trauma
Stony Brook Trauma Center

No financial disclosures

OVERVIEW
• Spinal anatomy/classification
• Evaluating a patient with suspected spinal injury
• Broad management principles of spinal injury
• Hypovolaemic vs neurogenic vs spinal shock

SPINAL CORD INJURY: EPIDEMIOLOGY
In the United States, the incidence of spinal cord injury in 2010 was approximately
40 per million persons per year, or approximately 12,400 annually
• Causes in the United States are:
- Motor vehicle accidents: 48 percent
- Falls: 16 percent
- Violence (especially gunshot wounds): 12 percent
- Sports accidents: 10 percent
- Other: 14 percent
Prior to 2000, the most frequent occurrence was a young male with a median age of
22. Since that time, the average age has increased to 37 years in 2010, presumably
as a reflection of the aging population.
Males continue to make up 77 to 80 percent of cases.
Alcohol plays a role in at least 25 percent of TSCI

ANATOMY
Location of Spinal Injuries
55% in cervical region
(mobile and exposed)
15% in thoracic region
(less mobile and protected)
15% in thoracolumbar region
(fulcrum)
15% in lumbosacral region

ANATOMY
• Upper cervical region is wide from foramen
magnum to lower part C3
- 1/3 die at scene from apnea
- those that survive are usually
neurologically intact when they reach
the hospital

ANATOMY
• Below C3 the diameter of the spinal canal is smaller
- vertebral column injuries are more likely to produce spinal
cord injuries
• Most thoracic spine fractures are wedge compression fractures
without spinal cord injury
- high association with a complete spinal cord injury because
of narrow thoracic canal
• Thoracolumbar junction is where the inflexible thoracic spine
meets the strong lumbar spine making it an area vulnerable to
injury

ANATOMY
• Multiple ascending and descending tracts
in the spinal cord
• 3 clinically relevant ones
- lateral corticospinal tract
- Controls motor functions on SAME side
- spinothalamic tract
- transmits pain and temp sensations
from the OPPOSITE side
- dorsal columns
- transmits proprioception and vibration
senses from the SAME side

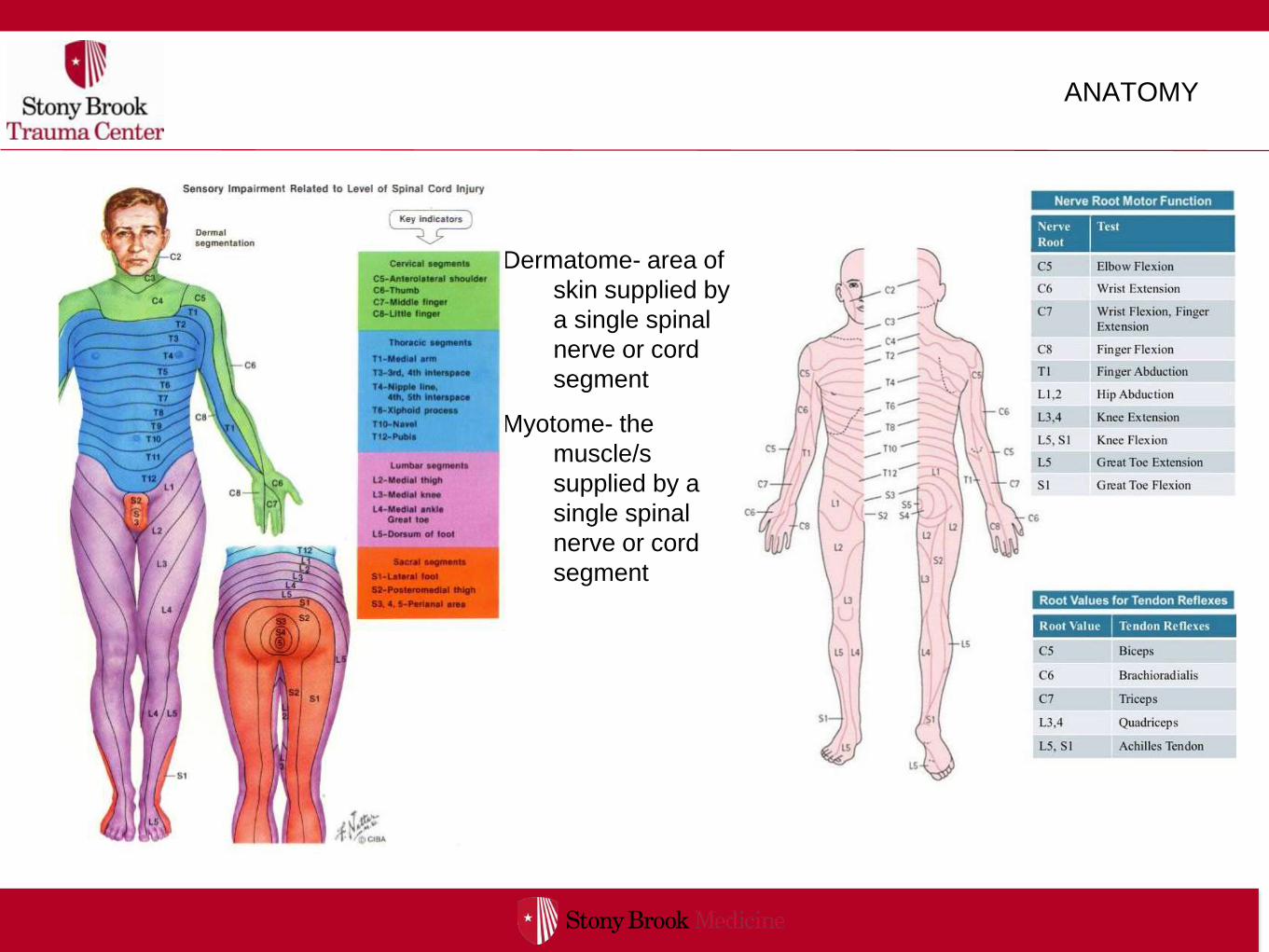
ANATOMY
Dermatome- area of
skin supplied by
a single spinal
nerve or cord
segment
Myotome- the
muscle/s
supplied by a
single spinal
nerve or cord
segment

SPINAL CORD INJURY: CLASSIFICATION
• Injuries to the spinal cord can be categorized in
numerous ways
- Incomplete paraplegia (incomplete thoracic injury)
- Incomplete quadriplegia (incomplete cervical
injury)
- Complete paraplegia
- Complete quadriplegia

SPINAL CORD INJURY: CLASSIFICATION
Injuries may have complete or incomplete
neurological symptoms
• Complete injury patients demonstrate total
and flaccid paralysis, total
anesthesia/analgesia, and no tendon reflexes
• Incomplete injury will demonstrate partial
paralysis w/ altered sensation and preserved
sacral function (sacral sparing)
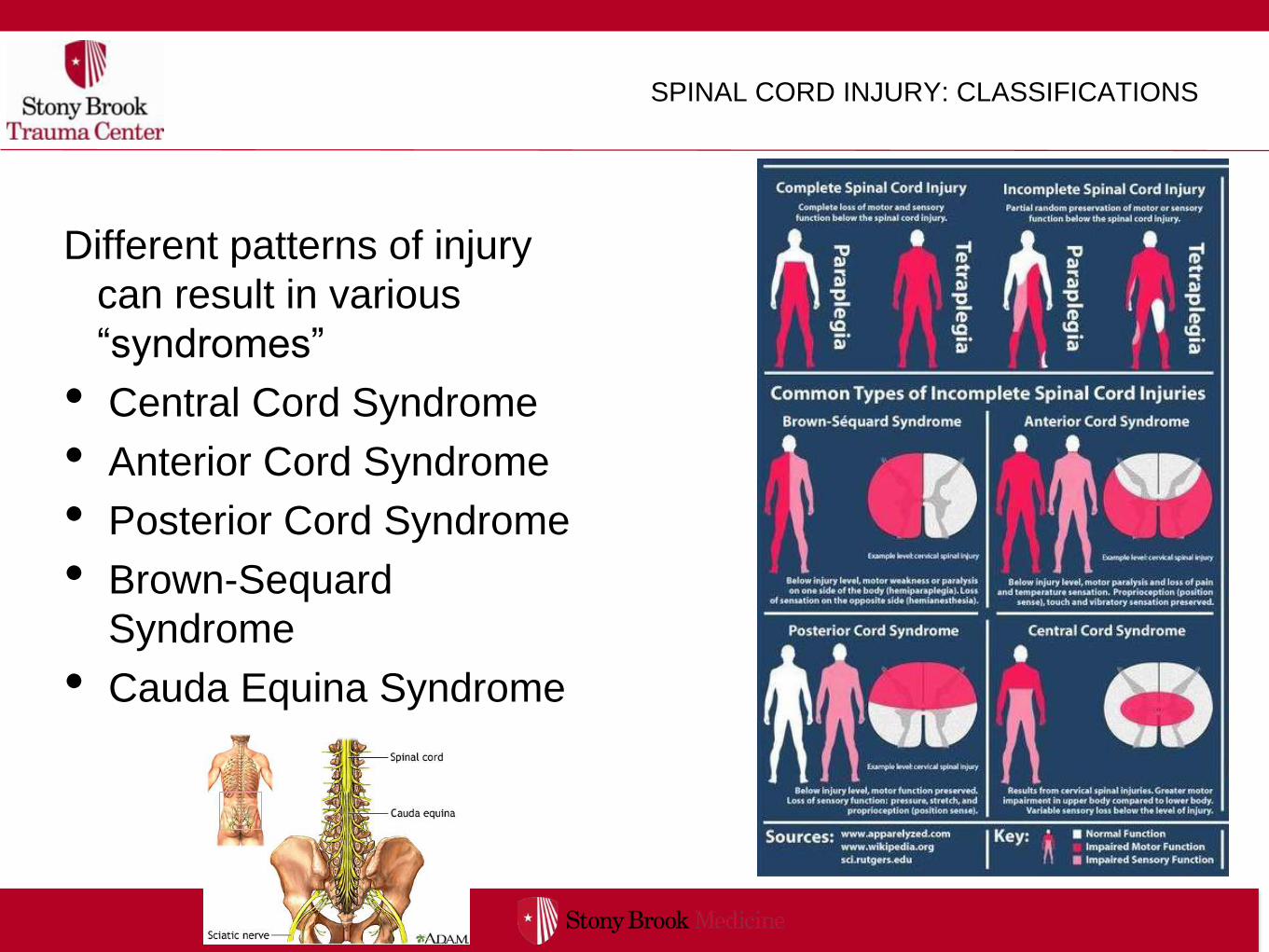
SPINAL CORD INJURY: CLASSIFICATIONS
Different patterns of injury
can result in various
“syndromes”
• Central Cord Syndrome
• Anterior Cord Syndrome
• Posterior Cord Syndrome
• Brown-Sequard
Syndrome
• Cauda Equina Syndrome

SPINAL CORD INJURY: CLASSIFICATION
Spinal injuries can also be described as:
• Fractures
• Fracture-dislocations
• Penetrating injury
• Spinal Cord Injury without Radiographic
Abnormalities (SCIWRA)

SPINAL CORD INJURY: EVALUATION
Signs and Symptoms:
• Pain
• Tingling, numbness and weakness in periphery
• Loss of sensation or paralysis below the level of
injury
• Respiratory distress
• Incontinence
• Priapism

SPINAL CORD INJURY: EVALUATION
Evaluation and care starts with the ABCs of trauma
• A=airway
- Need to establish an airway while maintaining c-
spine immobilization
- Place a definitive airway early if respiratory
compromise is suspected- typically with high
cervical injury (C3/4/5)

SPINAL CORD INJURY: EVALUATION
Evaluation and care starts with the ABCs of trauma
• B=breathing
- evaluate for any associated symptoms to
indicate underlying pulmonary trauma
- monitor for accessory muscle use to indicate
impending respiratory collapse
- use supplemental oxygen to prevent hypoxia

SPINAL CORD INJURY: EVALUATION
Evaluation and care starts with the ABCs of trauma
• C=circulation
- identify and control any bleeding from injuries
- Maintain a normal blood pressure to prevent
secondary spinal injury
- ? spinal shock- aggressive fluid resuscitation,
pressers may be required

SPINAL CORD INJURY: EVALUATION
Evaluation and care starts with the ABCs of trauma
• D=disability
- Check patient’s GCS status
- exam for equal and reactive pupils
- evaluate all 4 extremities for signs of weakness or
loss of sensation
- perform a rectal exam to evaluate for sphincter tone
- evaluate for priapism, bulbocavernosus reflex

SPINAL CORD INJURY: EVALUATION
Evaluation and care starts with the ABCs of trauma
• E=exposure
- remove all clothes to fully evaluate for injuries
- carefully log roll the pt to palpate the spine and paraspinal
regions
‣ identify all areas of pain with palpation
- patients with high spinal injuries may be vasodilated and
unable to regulate temperature
‣ Cover patients with warm blankets

SPINAL INJURY: EVALUATION
Adjuncts to primary survey
• Done after completion of ABCs
• Patient should be on continuous monitoring of vitals
• CXR and pelvic x-rays typically performed
• FAST exam- bedside ultrasound to evaluate for bleeding in
the abdomen as a source of hypotension
• Placement of Foley catheter, OGT
• Obtain a full medical history- important to ask about use of
anticoagulants!

SPINAL CORD INJURY: EVALUATION
Spinal Imaging
• X-rays- not done as first line, provided limited
information, can be difficult to obtain needed views
• CT scan- gold standard for defining bony injuries,
typically done as 1st line imaging as part of the
trauma “pan scan”
• MRI- useful to identify ligamentous injury or
contusions/compression of the spinal cord


SPINAL CORD INJURY: EVALUATION
Identify the level of spinal cord injury
• Make note of both sensory and motor
deficit levels
ANATOMY
Dermatome- area of
skin supplied by
a single spinal
nerve or cord
segment
Myotome- the
muscle/s
supplied by a
single spinal
nerve or cord
segment

SPINAL CORD INJURY: EVALUATION
Identify the level of spinal cord injury
• Make note of both sensory and motor
deficit levels

SPINAL CORD INJURY: EVALUATION
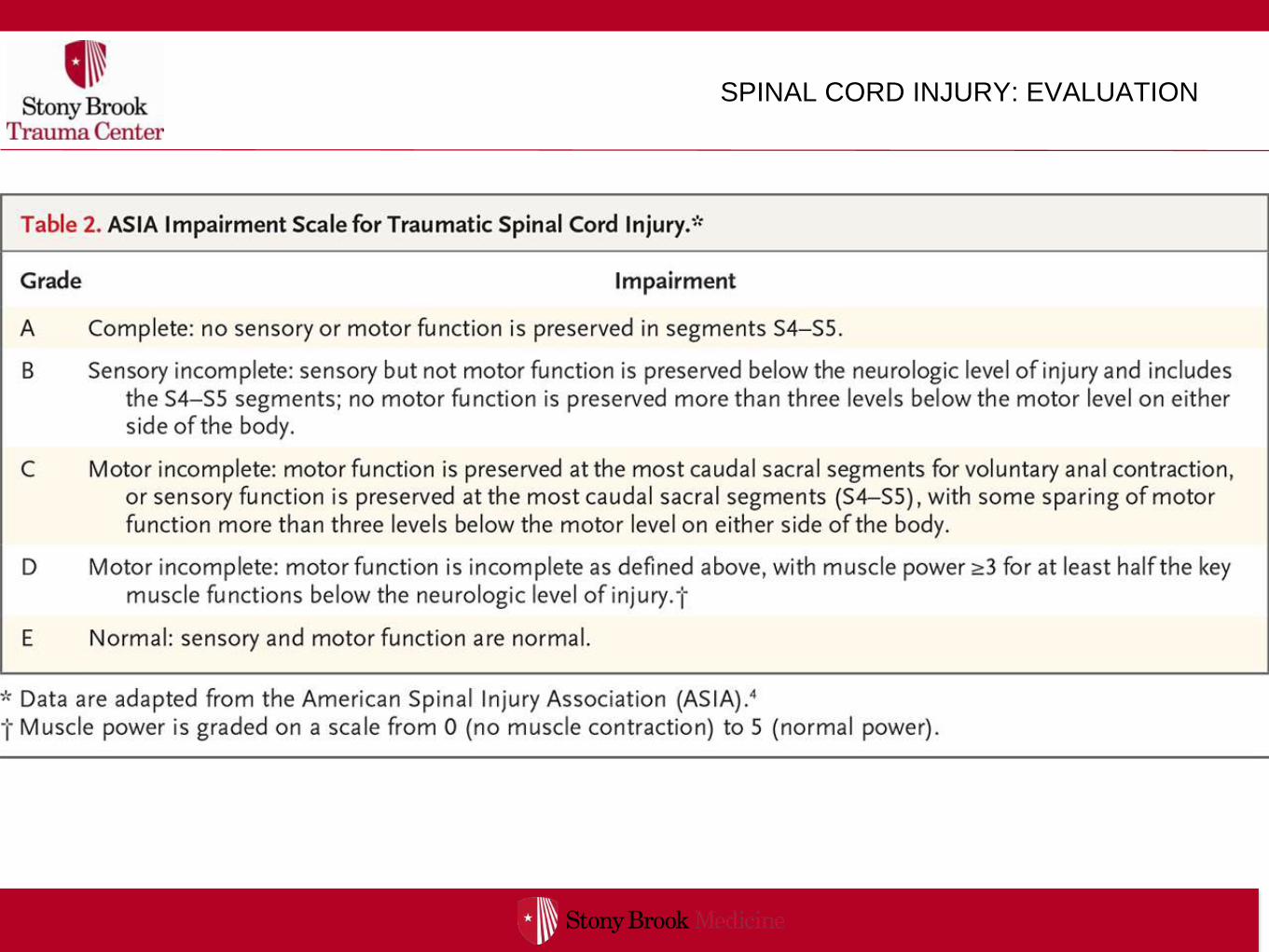
American Spinal Injury Association (ASIA)
Classification
• Allows for standardized classification of spinal cord
• Based on
• severity of neurological deficit- A=complete to
E=normal
• the neurological level- identify the most caudal
segment with normal function
SPINAL CORD INJURY: EVALUATION

SPINAL CORD INJURY: MANAGEMENT
Phases of injury
• Primary spinal cord injury- injury to spinal cord
directly related to fractures, dislocations,
compression, bleeding
• Secondary spinal injury- resulting from prolong
mechanical instability or subsequent episodes
of hypotension, hypoxia, infections

SPINAL CORD INJURY: MANAGEMENT
Management principles:
Stabilize the primary source of injury; prevent any
secondary injury from occurring
• Immobilization
• IV fluid resuscitation
• Medications
• Surgery

SPINAL CORD INJURY: MANAGEMENT
Strict immobilization
• 5% of patients with existing injury experience a worsening or
new onset of symptoms after arriving to the ED- poor
immobilization techniques
• use a cervical collar
• if a pt needs intubation must maintain inline cervical
stabilization
• These are potentially difficult intubations
• maintain patients flat and on bedrest until appropriate bracing
is in place if appropriate

SPINAL CORD INJURY: MANAGEMENT

SPINAL CORD INJURY: MANAGEMENT
IV fluid resuscitation
• maintain SBP > 90mm Hg
• Normal saline bolus
• If blood pressure is refractory to fluid
resuscitation consider neurogenic
shock

SPINAL CORD INJURY: MANAGEMENT
Hypovolemic Shock vs Neurogenic
SPINAL CORD INJURY: MANAGEMENT
Neurogenic Shock:
• Mechanism- impairment of descending sympathetic pathways
in the cervical or upper thorax (usually above T6)
- Leads to a loss of vascular sympathetic motor tone
‣ Results in peripheral vasodilation, pooling of blood and
hypotension
- Loss of sympathetic stimulus to the heart (injury above T1)
‣ Results in bradycardia and lack of reflexive tachycardia
response to hypotension

SPINAL CORD INJURY: MANAGEMENT
Neurogenic Shock vs Spinal shock

SPINAL CORD INJURY: MANAGEMENT
Spinal Shock:
• Mechanism- transient loss of voluntary and reflexive
neurologic function below the level of injury
- Spinal cord dysfunction maybe transient but can last
days to months
- flaccid paralysis, bowel and bladder incontinence,
priapism
- first reflexes to return are bulbocavernosus and babinski

SPINAL CORD INJURY: MANAGEMENT
Neurogenic Shock
• Management
- Hypotension:
‣ Bolus of crystalloid fluids- may require large amounts but beware of fluid overload and
pulmonary edema
‣ Vasopressors- typically a pure alpha-blocking agent such as phenylephrine
‣ Goal is to maintain end organ perfusion- warm extremities, MAP >65mm Hg, UO
>0.5cc/kr/hr
- Bradycardia: treatment only needed if persistent hypotension
‣ Atropine given for acute therapy
‣ Pacemaker can be needed rarely in refractory cases
‣ Avoid over-zealous vagal stimulation such as NT suctioning, ETT manipulation, carotid
massage

SPINAL CORD INJURY: MANAGEMENT
Medical therapy:
• Corticosteroids- Aimed at reducing the extent of secondary spinal damage
- Most trials have used high dose methylprednisolone
‣ to be given within 8 hrs from time of injury
‣ bolus first given followed by IV infusion for 24-48hrs
- Insufficient evidence to routinely recommend
‣ Early studies (NASCIS I&II) showed no increased complications or mortality, however larger
and later studies have raised significant concerns related to sepsis and mortality
‣ In 2013, based upon the available evidence, the American Association of Neurological
Surgeons and Congress of Neurological Surgeons stated that the use of glucocorticoids in
acute spinal cord injury is not recommended
‣ Position statements from the Canadian Association of Emergency Physicians, endorsed by the
American Academy of Emergency Medicine, concur that treatment with glucocorticoids is a
treatment option and not a treatment standard.

SPINAL CORD INJURY: MANAGEMENT
Management of co-morbidities of the injury
• Respiratory compromise- Pulmonary complications, including respiratory
failure, pulmonary edema, pneumonia, and pulmonary embolism, are the most
frequent category of complications after injury
- early intubation and ventilator support as needed
- Tracheostomy is performed within 7-10 days unless extubation is imminent
• Venous thrombosis- Deep venous thrombosis (DVT) is a common complication
of spinal injury, occurring in 50 to 100 percent of untreated patients, with the
greatest incidence between 72 hours and 14 days
- All spinal cord injury patients should receive DVT prophylaxis as soon as
possible
- Early consideration for placement of an IVC Filter if pt is quadriplegic

SPINAL CORD INJURY: MANAGEMENT
Management of co-morbidities of the injury
• Pain control. After spinal injuries, patients usually require pain relief.
• Pressure sores. Pressure sores are most common on the buttocks and heels and
can develop quickly (within hours) in immobilized patients.
- Backboards should be used only to transport patients with potentially unstable
spinal injury and discontinued as soon as possible.
- After spinal stabilization, the patient should be turned side to side (log-rolled)
every two to three hours to avoid pressure sores.
- Check for pressure sores under cervical collars
• Urinary catheterization. Typically an indwelling urinary catheter is used to avoid
bladder distention.
- Three or four days after injury, intermittent catheterization should be
substituted, as this reduces the incidence of bladder infections

SPINAL CORD INJURY: MANAGEMENT
Management of co-morbidities of the injury
• Gastrointestinal stress ulceration. Patients with spinal injury, particularly those that affect the
cervical cord, are at high risk for stress ulceration. Prophylaxis with proton pump inhibitors is
recommended upon admission for four weeks
• Paralytic ileus. Bowel motility may be silent for a few days to weeks after injury. Patients
should be monitored for bowel sounds and bowel emptying, and should not ingest food or
liquid until motility is restored
• Temperature control. Patients with a cervical spinal cord injury may lack vasomotor control
and cannot sweat below the lesion. Their temperature may vary with the environment and
need to be maintained.
• Functional recovery. Occupational and physiotherapy should be started as soon as
possible. Psychological counseling is also best offered to patients and relatives as early as
possible.
• Nutrition- nutritional support should be provided early after injury- ideally within the first
24hrs if patient is stable
- Enteral or PO feeding is the prefer route.

SPINAL CORD INJURY: MANAGEMENT
Surgical Fixation
• Cervical Traction
- Gardner-Wells tongs
‣ Provides temporary stability of the cervical spine
‣ Contraindicated in unstable hyperextension injuries
‣ Weight depends on the level (usually 5lb/level, start with 3lb/level, do
not exceed 10lb/level)
‣ Cervical collar can be removed while patient is in traction
‣ Pin care: clean q shift with appropriate solution, then apply povidone-
iodine ointment
‣ Take XRays at regular intervals and after every move from bed

SPINAL CORD INJURY: MANAGEMENT

SPINAL CORD INJURY: MANAGEMENT

SPINAL CORD INJURY: MANAGEMENT

SPINAL CORD INJURY:MANAGEMENT

SPINAL CORD INJURY : CONCLUSIONS
Take Home Messages:
• Over 1/2 of spinal cord injuries occur in the cervical spine
• C-spine immobilization is critically early in patients with
suspected injury to prevent further damage
• Consider early intubation and ventilation for patients with
evidence of high cervical injuries before they show signs of
respiratory distress
• The principles of ATLS “ABCs” still apply to fully evaluate
the patient and treat any associated injuries

SPINAL CORD INJURY: CONCLUSIONS
Take Home Messages:
• Neurogenic shock is a triad of hypotension, bradycardia,
and peripheral vasodilation
• In trauma patients, neurogenic shock is a diagnosis of
exclusion
• Avoid over-zealous fluid resuscitation- consider
vasopressors if blood pressure is refractory to treatment
• Early consultation with a spinal specialist for surgical
fixation

Questions?
Thank you!