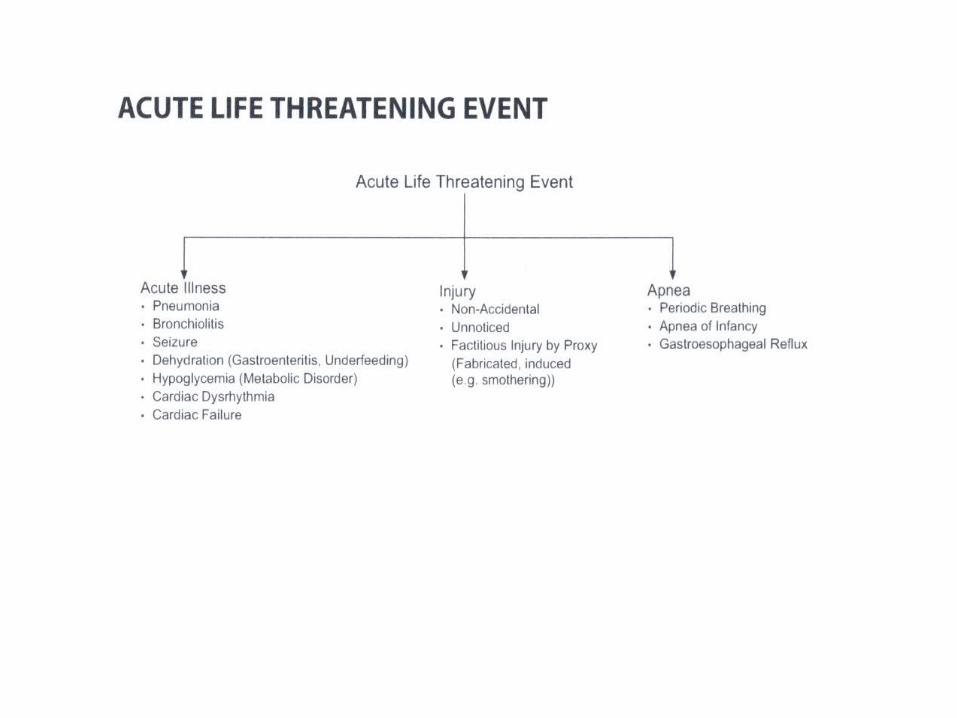
acute life threatening event
DESCRIPTION
ACUTE LIFE THREATENING EVENT. SUDDEN UNEXEPECTED DEATH IN INFANCY. - PowerPoint PPT PresentationTRANSCRIPT

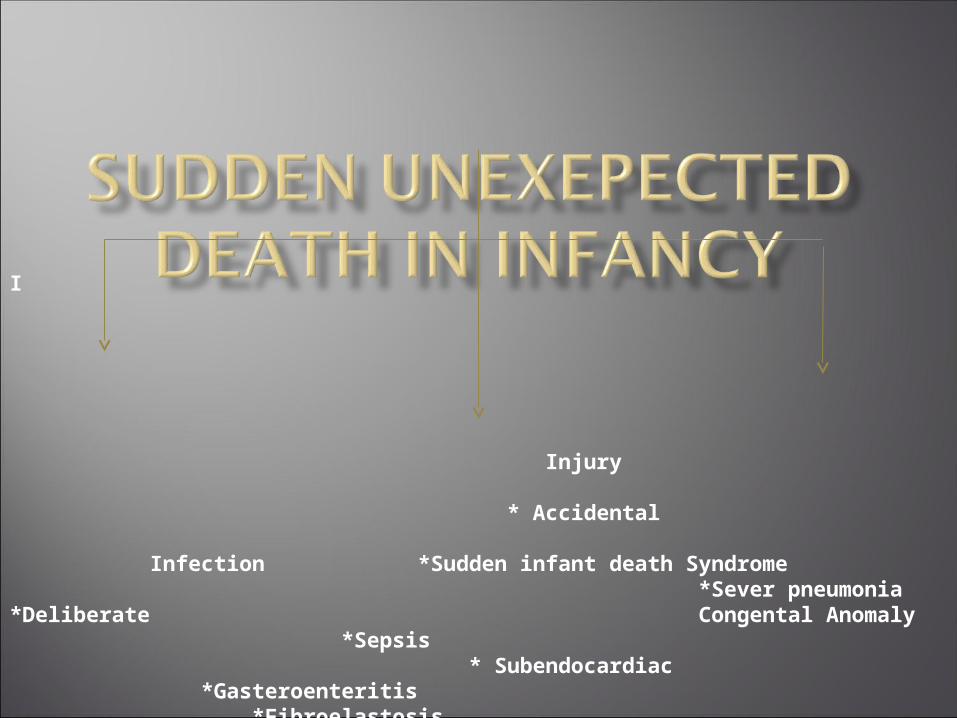
I Injury * Accidental Infection *Sudden infant death Syndrome *Sever pneumonia *Deliberate Congental Anomaly *Sepsis * Subendocardiac *Gasteroenteritis *Fibroelastosis *Long QT Syndrome *Cardiac Anomaly *Pulmonary Anomaly
*Neurological Anomaly
FT baby 6days old, producte of home vaginal delivary with PROM>24hr ,he had fever&vomting,poor sucking laste 3days.O/E ;Lethargic,febrile(38C) NN reflex weak

Pathways of ascending or intrapartum infection
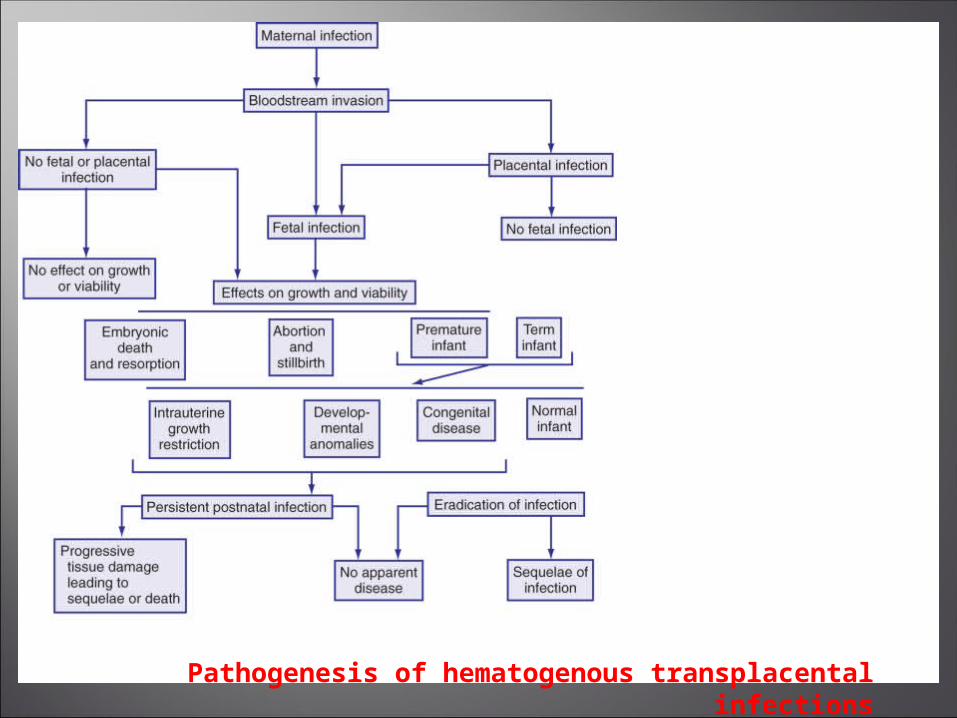
Pathogenesis of hematogenous transplacental infections

It is the systemic inflammtory responesto an infection process.
The most commen cause;
GBS , E-Coli ,L-monocytogenusOther causes are ;(non-bactrial)Viral , protozal , fungal
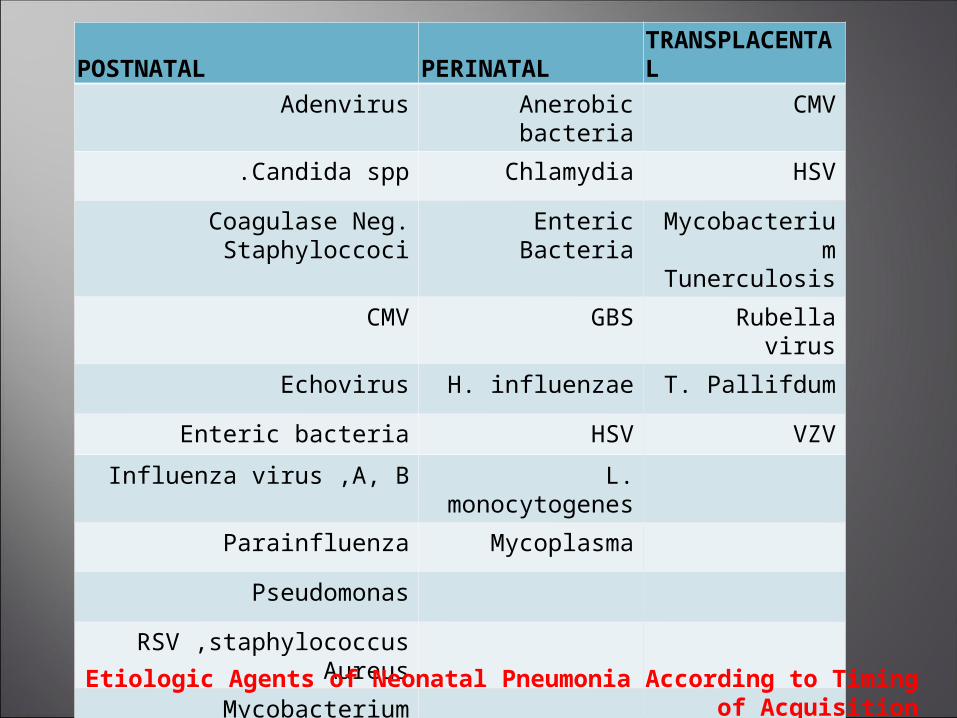
TRANSPLACENTALPERINATALPOSTNATAL
CMVAnerobic bacteria
Adenvirus
HSVChlamydiaCandida spp.
Mycobacterium Tunerculosis
Enteric BacteriaCoagulase Neg. Staphyloccoci
Rubella virusGBSCMV
T. PallifdumH. influenzaeEchovirus
VZVHSVEnteric bacteria
L. monocytogenes
Influenza virus ,A, B
MycoplasmaParainfluenza
Pseudomonas
RSV ,staphylococcus Aureus
Mycobacterium Tuberculosis
Etiologic Agents of Neonatal Pneumonia According to Timing of Acquisition

BACTERIAEARLY ONSETLATE ONSET, MATERNAL ORIGIN
LATE ONSET, NOSOCOMIAL
LATE ONSET, COMMUNITYGRAM POSITIVE
Clostridia+ +
Enterococci+ ++ Group B streptococcus++++++Listeria monocytogenes
++
Other streptococci++ +Staphylococcus aureus+ +++Staphylococcus, coagulase negative
+ +++
Streptococcus pneumoniae
+ ++
Viridans streptococcus+ ++ GRAM NEGATIVE
Bacteroides+ + Campylobacter+ Citrobacter ++Enterobacter + Escherichia coli+++ +++Haemophilus influenzae+ +Klebsiella + Neisseria gonorrhoeae+ Neisseria meningitidis+ + Proteus + Pseudomonas + Salmonella + +Serratia +
OTHERS
Treponema pallidum++ Mycobacterium tuberculosis
+
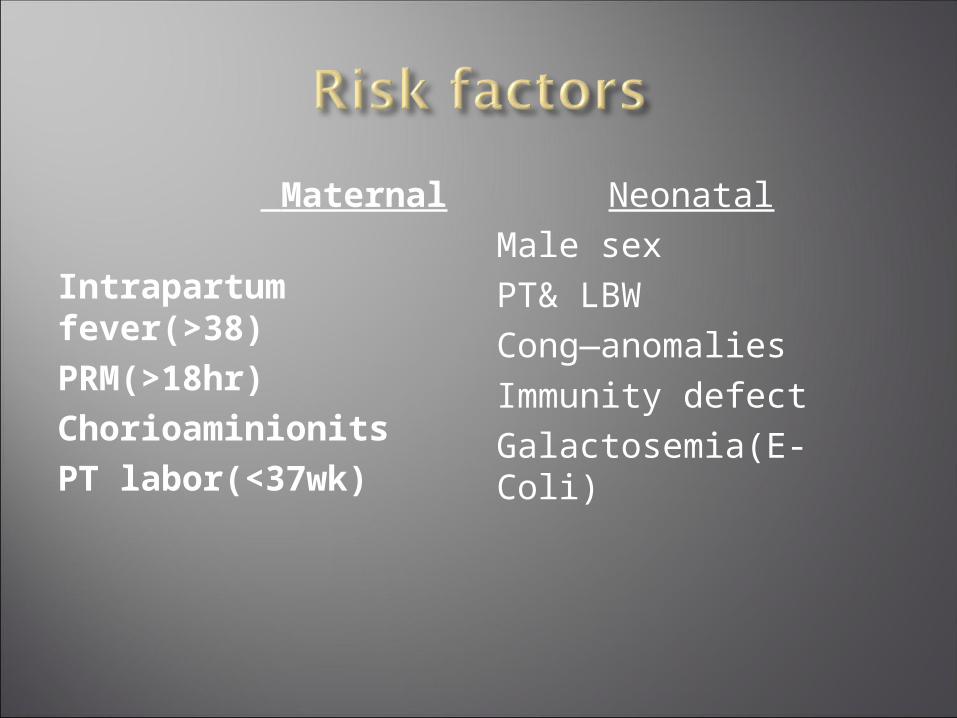
Maternal
Intrapartum fever(>38)PRM(>18hr)ChorioaminionitsPT labor(<37wk)
NeonatalMale sexPT& LBWCong—anomaliesImmunity defectGalactosemia(E-Coli)

General;Fever.temperature instabilityPoor feedingGIT;
Diarreh,VomitingAbd-distentionRespiratory;Apnea,RDSRenal;oliguria
CNS;Irritability,lethargy,seizers High pitch cry,hypotonia,Full fontanel,CVS;
Pallor,mottling,HR) (hypotention,Hematology; Jaundies, pallor,petechia,purpuraBleeding
sepsis workup;
*Culture; Blood—CSF—Urine*CBC; WBC(<5000), ANC<1750, I : T>0,2
*CRP*G.stain;CSF,Urine;Infected side
*Chest Xry
Once the pathogen has been identified & antibiotic sensitivities determined, the most appropriate drug or drugs should be selected.
For most gram-negative enteric bacteria, Ampicillin & an Aminoglycoside or a 3rd-generation cephalosporin (cefotaxime or ceftazidime) should be used .
Enterococci should be treated with both a penicillin (Ampicillin or piperacillin) & an aminoglycoside because the synergy of both drugs is needed. Ampicillin alone is adequate for L. monocytogenes,
and penicillin suffices for GBS .
Clindamycin or metronidazole is appropriate for anaerobic infections
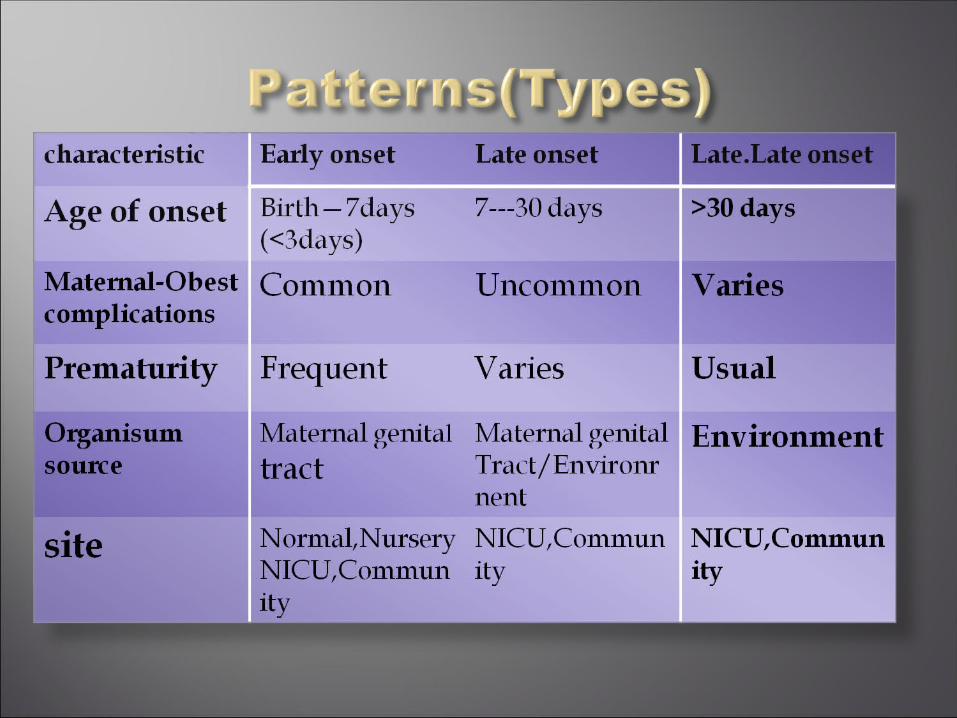
Is determined by pattern of disease and the organisms that are common for the age of
infant&
the flora of the nursery.
Duration of Rx;
meningits(14—21days)Pneumonia(7—10)
CVS;
CHD.myocaditis,PPHNGIT;
Necrotizing enterocolitisspontanousGITperfora-tionHematology;
Nnpurpuric fulminansSever anemiaImmune mediated neutropenia&thromboc-ytopenia
Respiratory;
RDS,lung hypoplasiaTEOF,aspiratin pneumonia,
Metabolic;
HypoglysemiaGalactosemiaCNS;
HIE.Infant botulismICH
The risk factors for death or for moderate or severdisability include;
*Duration of seizeres >72hrs*Coma
*Necessity for the use of inotropic agents*Lukopenia

MANIFESTATIONPATHOGEN
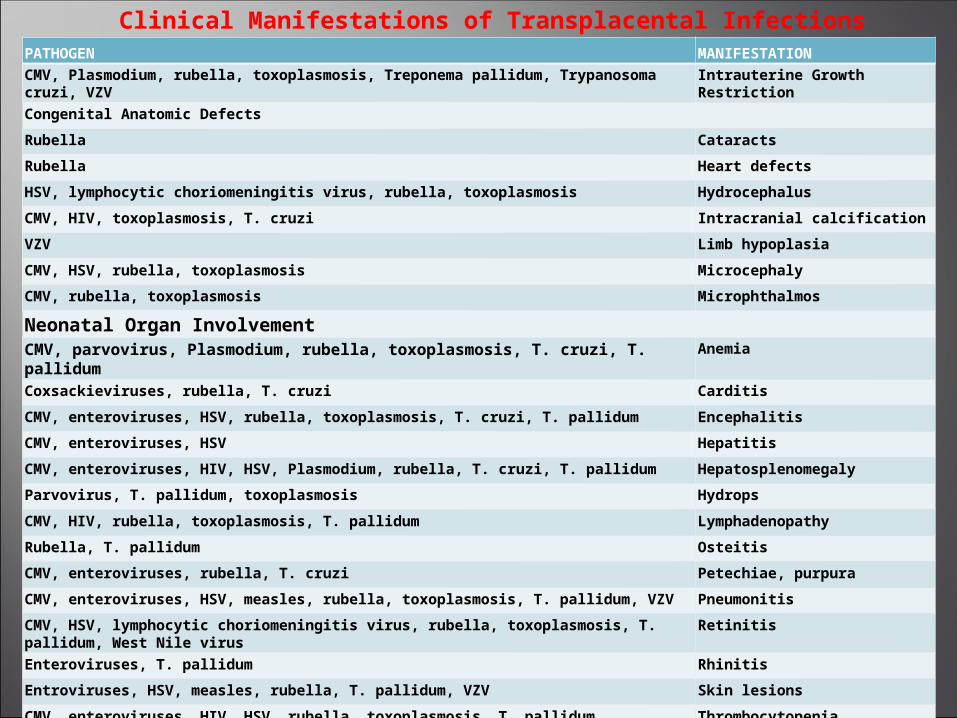
Intrauterine Growth Restriction
CMV, Plasmodium, rubella, toxoplasmosis, Treponema pallidum, Trypanosoma cruzi, VZV
Congenital Anatomic Defects
CataractsRubella
Heart defectsRubella
HydrocephalusHSV, lymphocytic choriomeningitis virus, rubella, toxoplasmosis
Intracranial calcificationCMV, HIV, toxoplasmosis, T. cruzi
Limb hypoplasiaVZV
MicrocephalyCMV, HSV, rubella, toxoplasmosis
MicrophthalmosCMV, rubella, toxoplasmosis
Neonatal Organ InvolvementAnemiaCMV, parvovirus, Plasmodium, rubella, toxoplasmosis, T. cruzi, T.
pallidumCarditisCoxsackieviruses, rubella, T. cruzi
EncephalitisCMV, enteroviruses, HSV, rubella, toxoplasmosis, T. cruzi, T. pallidum
HepatitisCMV, enteroviruses, HSV
HepatosplenomegalyCMV, enteroviruses, HIV, HSV, Plasmodium, rubella, T. cruzi, T. pallidum
HydropsParvovirus, T. pallidum, toxoplasmosis
LymphadenopathyCMV, HIV, rubella, toxoplasmosis, T. pallidum
OsteitisRubella, T. pallidum
Petechiae, purpuraCMV, enteroviruses, rubella, T. cruzi
PneumonitisCMV, enteroviruses, HSV, measles, rubella, toxoplasmosis, T. pallidum, VZV
RetinitisCMV, HSV, lymphocytic choriomeningitis virus, rubella, toxoplasmosis, T. pallidum, West Nile virus
RhinitisEnteroviruses, T. pallidum
Skin lesionsEntroviruses, HSV, measles, rubella, T. pallidum, VZV
ThrombocytopeniaCMV, enteroviruses, HIV, HSV, rubella, toxoplasmosis, T. pallidum
Clinical Manifestations of Transplacental Infections
Aggressive management of suspected maternal chorioamnionitis with antibiotic therapy during labor,along with rapid delivaryof the infant,reduces the risk of early Nnsepsis.
Intrapartum chemoprophylaxsis reduced the vertical transmission of GBS .

That is unexpected by history and unexplained by a thorough postmortem examination ,which includes a complete autopsy,investigation of the scene of death, and review of medical history .

Maternal;
Smoking,DrugsNutritional deficiencyDecreased age,educationSingle marital statusIGR,increas parityLow socioeconomic status
Infant;Age(2-4mo),PT,MalePron sleep positionGrowth failureRecent(febrile) illnessSoft bedding

Objectives ;
*Definition Factors ;
Risk * Mternal &neonatal
* Types & clinical manifestation l
Diagnosis *
Treatment *Prognosis *
Prevention * * DD