act iikanser.org/saglik/upload/malign_pdf2/gastrointestinal...tegafur- urasil .sorafenib...
TRANSCRIPT

ASCO 2012
Non-Kolorektal Dr Sezer Sağlam
İstanbul Bilim Üniversitesi Medikal Onkoloji

The optimum time to assess
complete clinical response (CR)
following chemoradiation (CRT) using mitomycin C (MMC) or
Cisplatin (CisP) with or without Maintenance CisP/5FU in
squamous cell carcinoma of the anus: Results of ACT II
Dr Rob Glynne-Jones on behalf of the NCRI ACT II Trial Management Group and Investigators
ASCO, Chicago, June 2012. Abstract ID: 4004 Cancer Research UK grant number: C444/A628
ISRCTN number: 26715889
Sponsor Funder

Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled
trial.JAMA 2008 Ajani J Mitomycin-( 341), who received fluorouracil (1000 mg/m2 on days
1-4 and 29-32) plus mitomycin (10 mg/m2 on days 1 and 29)
Radiotherapy (45-59 Gy) Cisplatin (n = 341), who received fluorouracil (1000 mg/m2 on days 1-4, 29-32, 57-60, and 85-88) plus cisplatin (75 mg/m2 on
days 1, 29, 57, and 85) radiotherapy (45-59 Gy; start day = day 57).
644 patients. median follow-up for all patients was 2.51 years. 55 years, 69% 27% had a tumor diameter greater than 5 cm,
and 26% had clinically positive nodes.
Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled
trial.JAMA 2008 Ajani J
1998-2005 The 5-year DFS was 60% in the mitomycin-based group and 54% (P = .17). The 5-year OS rate was 75% in the mitomycin-based group and 70% in the cisplatin-based group (P = .10). The 5-year local-regional recurrence and distant metastasis rates were 25% (and 15%), for mitomycin-based treatment and 33% and 19%, respectively, for cisplatin-based treatment. The cumulative rate of colostomy was significantly better for mitomycin-based than cisplatin-based treatment (10% vs 19%; P = .02). Severe hematologic toxicity was worse with mitomycin-based treatment (P < .001) Conclusion:In this population of patients with anal canal carcinoma, cisplatin-based therapy failed to improve disease-free-survival compared with mitomycin-based therapy, but cisplatin-based therapy resulted in a significantly worse colostomy rate
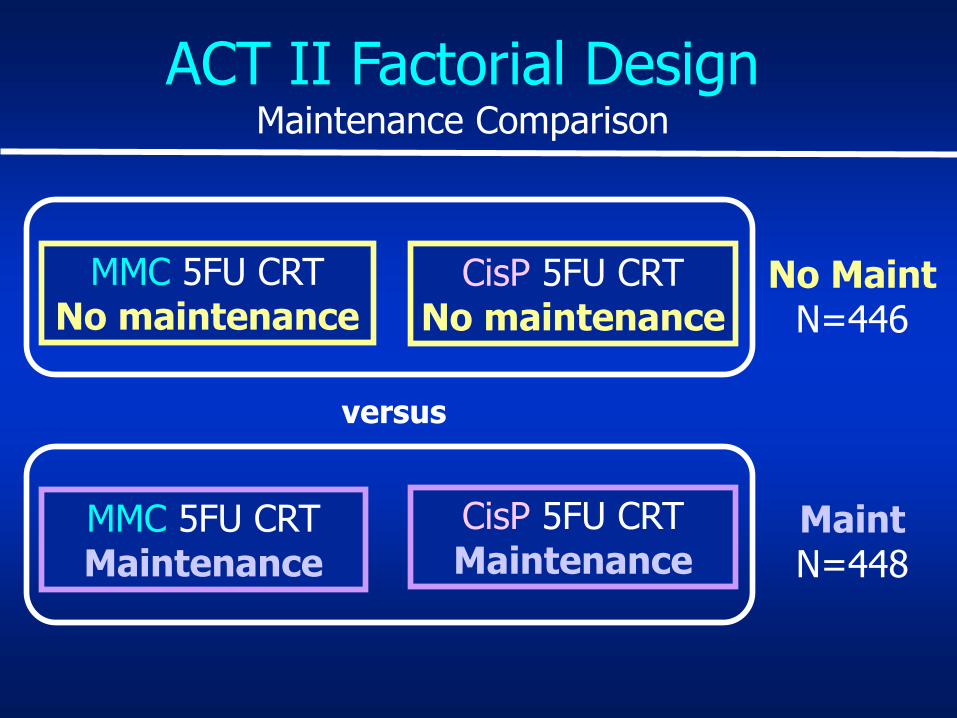
MMC 5FU CRT No maintenance
CisP 5FU CRT No maintenance
MMC 5FU CRT Maintenance
CisP 5FU CRT Maintenance
No Maint N=446
Maint N=448
versus
ACT II Factorial Design Maintenance Comparison

Chemoradiation Regimens
1 2 3 4 5 RT week
5FU
MMC
1 2 3 4 5 RT week
5FU
CisP
1000mg/m2 d1-4 & 29-32 24 hour continuous iv infusion
12mg/m2 d1 only iv bolus, max single dose 20 mg
60mg/m2 d1 & 29 iv infusion
1000mg/m2 d1-4 & 29-32 24 hour continuous iv infusion
6
6

Timing of CR Assessment (691 pts with data at all 3 time-points)
Wk Pts with CR
CR rate%
MMC CisP
Absolute risk difference
HR (95% CI) (CR vs not CR) PFS OS
11 426 65.2 58.1
7.1%
p=0.05 Ajani’yi
destek…
p=0.02 p=0.046
18 526 75.4 76.9 1.5%
p=0.64
0.52
p<0.001
0.48
p<0.001
26 584 84.1 85.0
0.9%
p=0.74
p<0.001
p<0.001
ACT II – Conclusions
• Excellent CR rate at 6 months - 83% v 84%
• 60% of pts not in CR at 11 weeks achieved CR at 26
weeks.
• Bundan sonra 26 haftada yanıt değerlendirmesi Öneriyor
• YANIT değerlendirmesi Rektum ile benzerlik gösteriyor diyebiliriz..
A Randomized Controlled Phase II Study of the Prophylactic Effect of Urea-Based Cream on the Hand-Foot Skin Reaction
Associated with Sorafenib in Advanced Hepatocellular Carcinoma
Zhenggang Ren1,et al (China) *
Hand-foot skin reaction (HFSR) is one of the most common adverse events associated with Sorafenib (SOR), with the incidence ranging from
21% to 93%.1

A Randomized Controlled Phase II Study of the Prophylactic Effect of Urea-Based Cream on the Hand-Foot
Skin Reaction Associated with Sorafenib in Advanced Hepatocellular Carcinoma
• We sought to investigate the prophylactic effect of urea-based creams on the incidence of HFSR associated with SOR treatment of patients with advanced HCC.
• Objective
– To investigate the prophylactic effect of an urea-based cream on HFSR associated with SOR;
Primary endpoint:
Incidence of all grade HSFR within 12 weeks of starting SOR treatment.

Study Rationale and Objective • Rationale
– Mild hyperkeratosis is an early sign of HFSR, and sometimes the only manifestation of sorafenib-related HFSR;
– Urea is useful for the treatment of hyperkeratotic conditions and has been recommended for treatment of multitargeted kinase inhibitor-related HFSRLacouture et al., Oncologist 2008
.Kapesitabine,
Tegafur- urasil .Sorafenib Vinorelbine, vinkristin, vinblastine liposomal Doksorubisin Merkaptopürin Florodeoksiüridin Hidroksiüre Siklofosfamid
1 Lacouture et al., The Oncologist 2008; 13:1001-1011
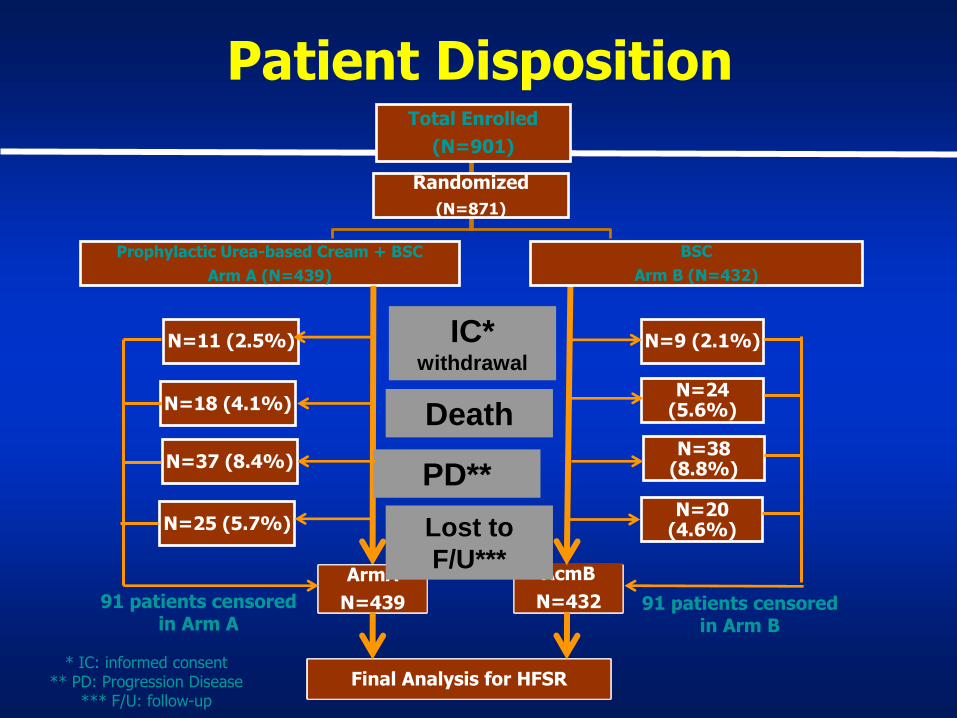
Total Enrolled
(N=901)
Prophylactic Urea-based Cream + BSC
Arm A (N=439)
N=11 (2.5%)
N=18 (4.1%)
N=37 (8.4%)
N=25 (5.7%)
Randomized
(N=871)
N=9 (2.1%)
N=24 (5.6%)
N=38 (8.8%)
N=20 (4.6%)
ArmA
N=439
AcmB
N=432
Final Analysis for HFSR
IC* withdrawal
Death
PD**
Lost to
F/U***
BSC
Arm B (N=432)
* IC: informed consent ** PD: Progression Disease
*** F/U: follow-up
Patient Disposition
91 patients censored in Arm A
91 patients censored in Arm B
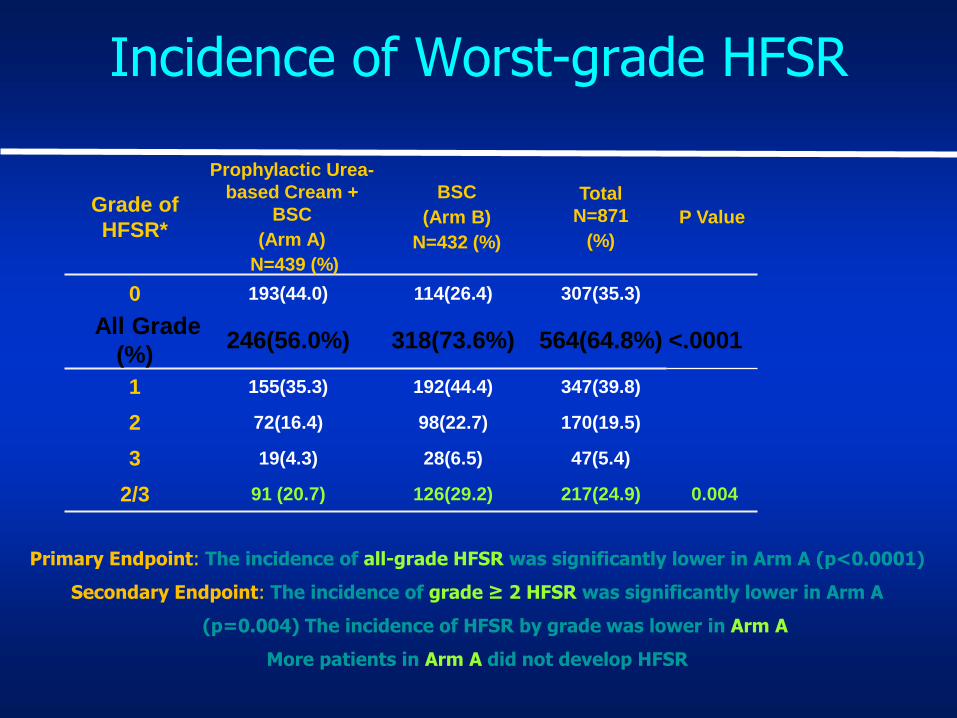
Incidence of Worst-grade HFSR
Grade of
HFSR*
Prophylactic Urea-
based Cream +
BSC
(Arm A)
N=439 (%)
BSC
(Arm B)
N=432 (%)
Total
N=871
(%)
P Value
0 193(44.0) 114(26.4) 307(35.3)
All Grade
(%) 246(56.0%) 318(73.6%) 564(64.8%) <.0001
1 155(35.3) 192(44.4) 347(39.8)
2 72(16.4) 98(22.7) 170(19.5)
3 19(4.3) 28(6.5) 47(5.4)
2/3 91 (20.7) 126(29.2) 217(24.9) 0.004
Primary Endpoint: The incidence of all-grade HFSR was significantly lower in Arm A (p<0.0001)
Secondary Endpoint: The incidence of grade ≥ 2 HFSR was significantly lower in Arm A
(p=0.004) The incidence of HFSR by grade was lower in Arm A
More patients in Arm A did not develop HFSR
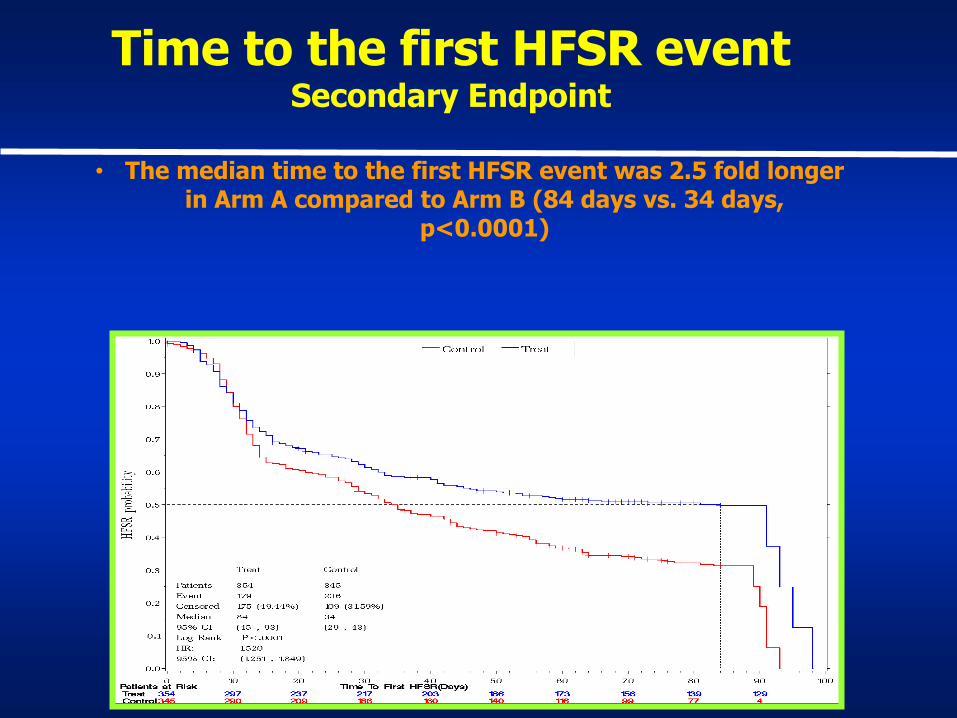
Time to the first HFSR event Secondary Endpoint
• The median time to the first HFSR event was 2.5 fold longer in Arm A compared to Arm B (84 days vs. 34 days,
p<0.0001)
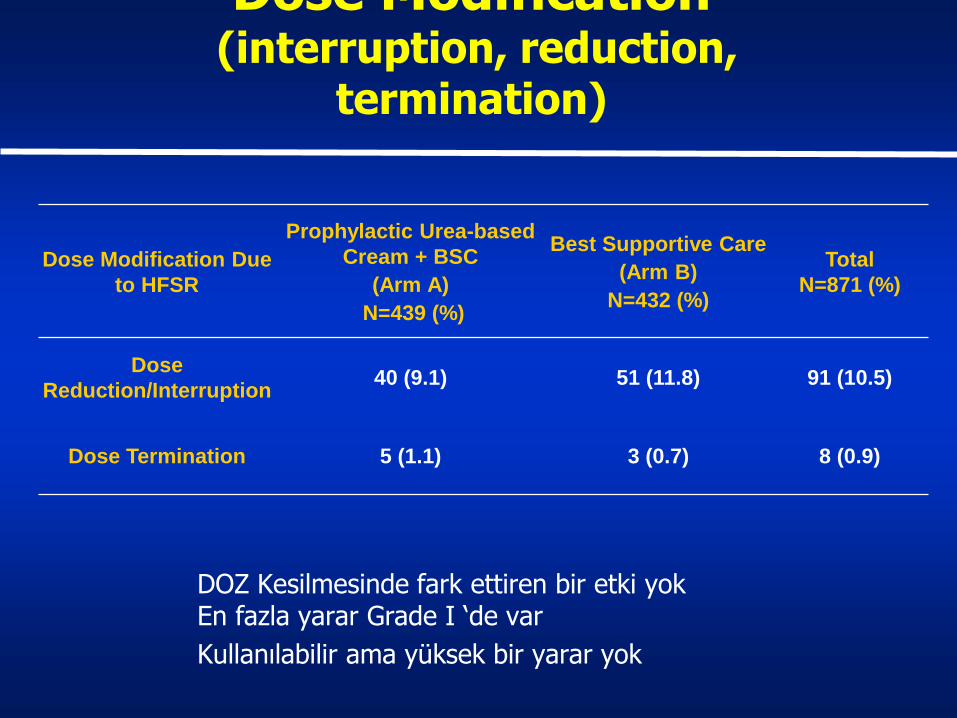
Dose Modification (interruption, reduction,
termination)
Dose Modification Due
to HFSR
Prophylactic Urea-based
Cream + BSC
(Arm A)
N=439 (%)
Best Supportive Care
(Arm B)
N=432 (%)
Total
N=871 (%)
Dose
Reduction/Interruption 40 (9.1) 51 (11.8) 91 (10.5)
Dose Termination 5 (1.1) 3 (0.7) 8 (0.9)
DOZ Kesilmesinde fark ettiren bir etki yok En fazla yarar Grade I ‘de var
Kullanılabilir ama yüksek bir yarar yok
Sınırlamalar
• Körleme bir çalışma değil
• Placebolo bir ürün yaratılabilirdi fakat ileridede yarar beklenecek bir ürün gibi gözükmüyor.
• Gözlem süresi az deniyor(14 hafta) ama klinisyen olarak yeterli diye düşünüyorum
• Krem olmayan kontrol yok….
• İlacın çalışma mekanızması önlemeye yönelik değil

PHASE II-III RANDOMISED TRIAL OF DEFINITIVE CHEMORADIOTHERAPY WITH FOLFOX OR CISPLATIN
AND FLUOROURACIL IN ESOPHAGEAL CANCER
PRODIGE 5 - ACCORD 17 trial: final results
T. Conroy, MP. Galais, JL. Raoul, O. Bouché, S. Gourgou,
JY. Douillard, PL. Etienne, V. Boige, I. Martel-Lafay, P. Michel,
C. Llacer-Moscardo, J. Bérille, L. Bedenne, A. Adenis; UNICANCER-GI/PRODIGE Group
Centre Alexis Vautrin, Nancy; Centre François Baclesse, Caen; Centre Eugène Marquis, Rennes and Institut Paoli-Calmettes, Marseille; Centre Hospitalier R. Debré, Reims; Centre Val d’Aurelle, Montpellier; Institut de Cancérologie de l’Ouest, Nantes; Clinique Armoricaine, Saint Brieuc;
Institut Gustave Roussy, Villejuif; Centre Léon Bérard, Lyon; Centre Hospitalier Universitaire, Rouen; UNICANCER R&D, Paris; Centre Hospitalier Universitaire, Dijon; Centre Oscar Lambret,
Lille; FRANCE

Prodige 5 - ACCORD 17 trial design
Stratification :
• Adenocarcinoma(?) vs squamous-cell vs adenosquamous • pretreatment weight loss < 10% vs ≥ 10% • performance status: 0 vs 1 vs 2 • center
Unresectable esophageal
cancer
R A N D O M I Z E
50 Gy/5 weeks + Folfox, 3 cycles
50 Gy/5 weeks + 5FU/cisplatin, 2
cy.
Folfox, 3
cycles
5FU/cisplatin,
2 cycles
Main Inclusion Criteria
• Patients unfit for surgery or locally advanced esophageal carcinoma (disease status: any T, N0 or N1, M0 or M1a)
• Histologically proven adenocarcinoma, squamous-cell or adenosquamous carcinoma of the esophagus
• ( uyumlu değil adenokarsinomda Wagner 2006 analizi üçlü kemoterapi daha uygun)
• No prior treatment for esophageal cancer
Birincil Sonlanım
Secondary:
*complete response rate
*toxicity (NCI-CTC version 3.0 grading)
*time to treatment failure
*overall survival
*quality of life (EORTC QLQ-C30 v 3.0 and QLQ-OES18)
Primary: progression-free survival

Statistical considerations
• Hypothesis:
– Study designed to have 90% power to detect an increase of 20% in 3 year-PFS
– (Çok gerçekçi değil ve 2 siklus versus 3 siklus şeklinde olmuş)
• Sample size:
– 266 hasta 144 event olarak hesaplanmış.
– 2004-2011 yılları arasında

Yorum
• Cisplatin ve Oxaliplatinde fark beklemiyoruz
• Yanıt oranlarını değiştirecek sadece EGFR gen amplifikasyonu nun en çok olduğu ikinci tümör grubu olan bu grupta fark olur …
• Sadece faz II cetuximabile sonuçlar iyi
• Daha rahat bir kemoterapi olabilir bu açıdan önemli….
A randomised multi-centre trial of epirubicin, oxaliplatin, and capecitabine plus
panitumumab in advanced oesophagogastric cancer (REAL3)
Dr T Waddell MBChB, MRCP
On behalf of the REAL-3 trial collaborators
T. Waddell, I. Chau, Y. Barbachano, D. Gonzalez-de-Castro, A. Wotherspoon, C. Saffery, G. Middleton, J. Wadsley, D. Ferry,
W. Mansoor, T. Crosby, F. Coxon, D. Smith, J. Waters, T. Iveson, S. Falk, S. Slater, A. Okines, D. Cunningham
Rationale for REAL3 Trial
• OG cancers 2nd commonest cause of cancer death worldwide (>1.1 million deaths/yr)1
• REAL2 trial2:
–EOC vs ECF (median OS 11.2mo vs 9.9mo, p=0.020; HR 0.80, 95% CI 0.66-0.97)
• EGFR pathway: AMPLİFİKASYON YOK ve FİSH NEGATİF !!!!!!
–Variable rates of over-expression in OG cancer (30-90%)
–Association with poor prognosis3,4
–Potential therapeutic target
–EGFR positivity / HER-2 status / KRAS mutation status not required for study entry
1. GLOBOCAN 2008 2. Cunningham et al, NEJM 2008
3. Yonemura et al, Oncology 1989 4. Kim et al, BJC 2009
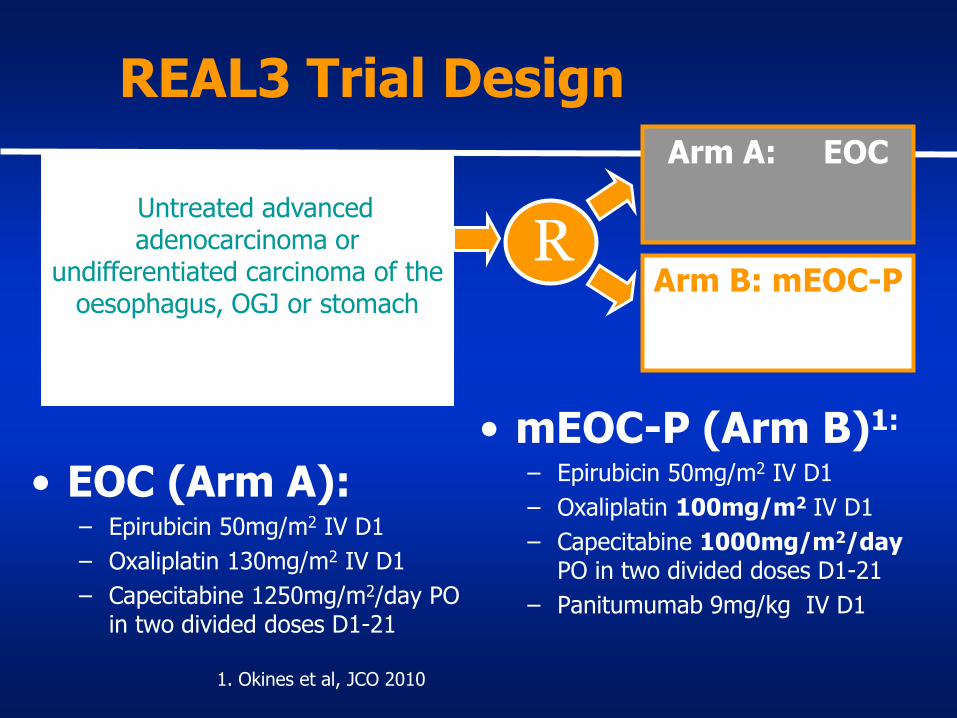
REAL3 Trial Design
Arm A: EOC
Arm B: mEOC-P R
Untreated advanced aUntreated advanced adenocarcinoma or
undifferentiated carcinoma of the oesophagus, OGJ or stomach
denocarcinoma or undiff the oesophagus, OGJ or stomach
• EOC (Arm A): – Epirubicin 50mg/m2 IV D1
– Oxaliplatin 130mg/m2 IV D1
– Capecitabine 1250mg/m2/day PO in two divided doses D1-21
• mEOC-P (Arm B)1:
– Epirubicin 50mg/m2 IV D1
– Oxaliplatin 100mg/m2 IV D1
– Capecitabine 1000mg/m2/day PO in two divided doses D1-21
– Panitumumab 9mg/kg IV D1
1. Okines et al, JCO 2010

Birincil Sonlanım
• Primary endpoint: overall survival – Aimed for 10% improvement in 1-year survival
rate (45% 55%)
– Hazard ratio 0.749
– 509 events, 90% power, 2-sided alpha 0.05
– Planned n=730
OS farkı dışında onay alma şansı yok
Çalışma Kapatılmış
• Inferior OS outcome in mEOC-P arm – HR 1.53, p=0.006
– Based on 169 events (EOC:68, mEOC-P:101)
• Phase III Trial closed (n=553, 76% total)
• All patients crossed over to EOC
• Data for patients still on treatment censored at time of trial closure
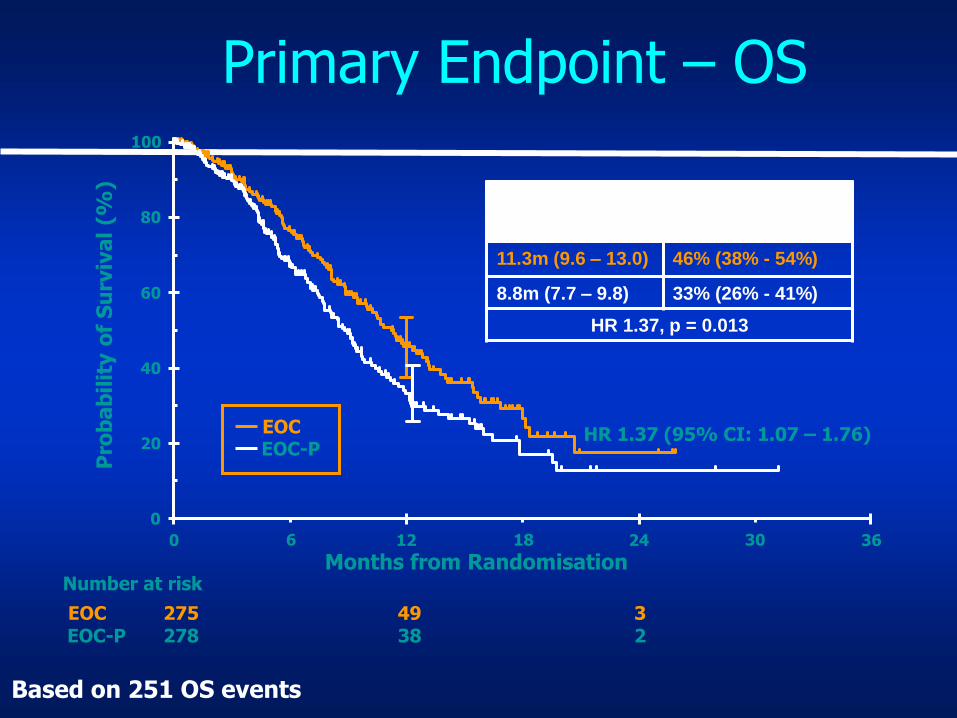
Primary Endpoint – OS
3 49 275 EOC 2 38 278 EOC-P
Number at risk
0
20
40
60
80
100
0 12 24 36
Months from Randomisation
Pro
ba
bil
ity o
f S
urv
iva
l (%
)
EOC EOC-P
% alive at 1 year
(95% CI)
11.3m (9.6 – 13.0) 46% (38% - 54%)
8.8m (7.7 – 9.8) 33% (26% - 41%)
HR 1.37, p = 0.013
HR 1.37 (95% CI: 1.07 – 1.76)
6 18 30
Based on 251 OS events
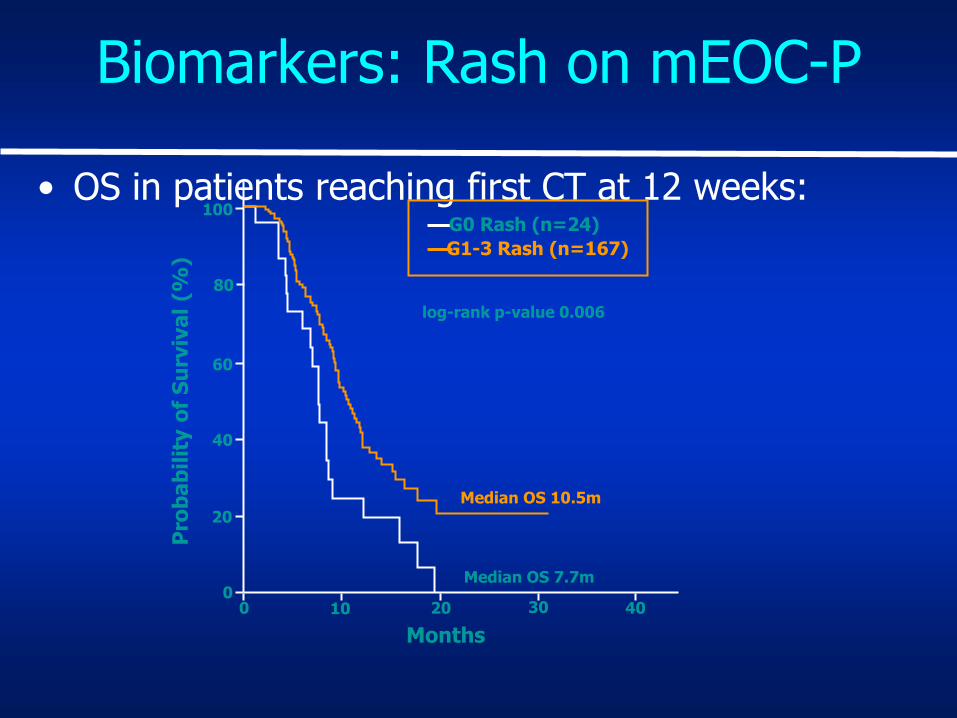
• OS in patients reaching first CT at 12 weeks:
Biomarkers: Rash on mEOC-P
20
40
60
80
100
0 0 10 20 40 30
G0 Rash (n=24)
G1-3 Rash (n=167)
Pro
ba
bil
ity o
f S
urv
iva
l (%
)
Months
Median OS 10.5m
Median OS 7.7m
log-rank p-value 0.006
Conclusions 2
• Crystal Çalışmasındaki BAŞARI YOK
• Mide diğerleri gibi seyretmiyor!

Bajetta Emilio ITACA-S Mide Adjuvan Folfiri+TXT Cisp versus DeGramount
• Adjuvant Mide Çalışması
• 4 siklus folfiri 3 siklus TC
• En az D1 diseksiyon olacak pN+ veya pT2-3-4
• RT yok
• DFS primary end point(?)
• 1106 hasta randomize edilmiş
• D2 %72 fakat 25 lenf üstü 56% yani az
• 76% tamamlamış 86%FUFA
• Nötropeni kusma diare fazla
• 48 ay takip DS 41 ay eşit 52% 5 yıl Osurvival
• KULLANMAYIN diyor

Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal poorly differentiated neuroendocrine carcinoma: The NORDIC NEC study
Aggressive tumors with Ki-67.20%
GI-NEC patients diagnosed during 2000-2009 at 12 Nordic university hospitals.305 patients Palliative chemotherapy was given to 252 patients, median survival was 11 months
• Response rate to 1st-line chemotherapy was 31%, 33% had stable disease. Ki-67,55% was
• by ROC analyses the best cut-off value concerning correlation to response rate.
Response rate to platinum-based chemotherapy was lower in patients with Ki-67,55% (14% vs.44%, p,0.001). Response
rate for 84 patients given 2nd-line chemotherapy was 18%, whereas 33% achieved SD. The most important negative prognostic factors for survival were poor performance status, primary colorectal tumors, and
elevated baseline platelets or lactate dehydrogenase (LDH) levels. Patients with Ki-67,55% had longer median survival (15 months) than patients with Ki-67.55% (10 months) (p,0.001). Survival and response rates did not differ between the different platinum chemotherapy schedules (cisplatin-based vs. carboplatinbased)
or morphology subtypes. 53 patients received best supportive care only with a median survival of 1
month. Conclusions: This is, to our knowledge, the largest study reporting patient and tumor characteristics,
treatment and survival in advanced GI-NEC. Performance status, location of primary tumor and blood levels
of platelets and LDH were the strongest prognostic factors for survival. Patients with Ki-67,55% had
significantly longer survival than patients with higher Ki-67,