acls ce -part i of iii -ecg strip interpretation w case scenarios supplemental
TRANSCRIPT
ACLS CE Part I of III
ECG STRIP INTERPRETATION
Prepared and presented by
Marc Imhotep Cray, M.D.
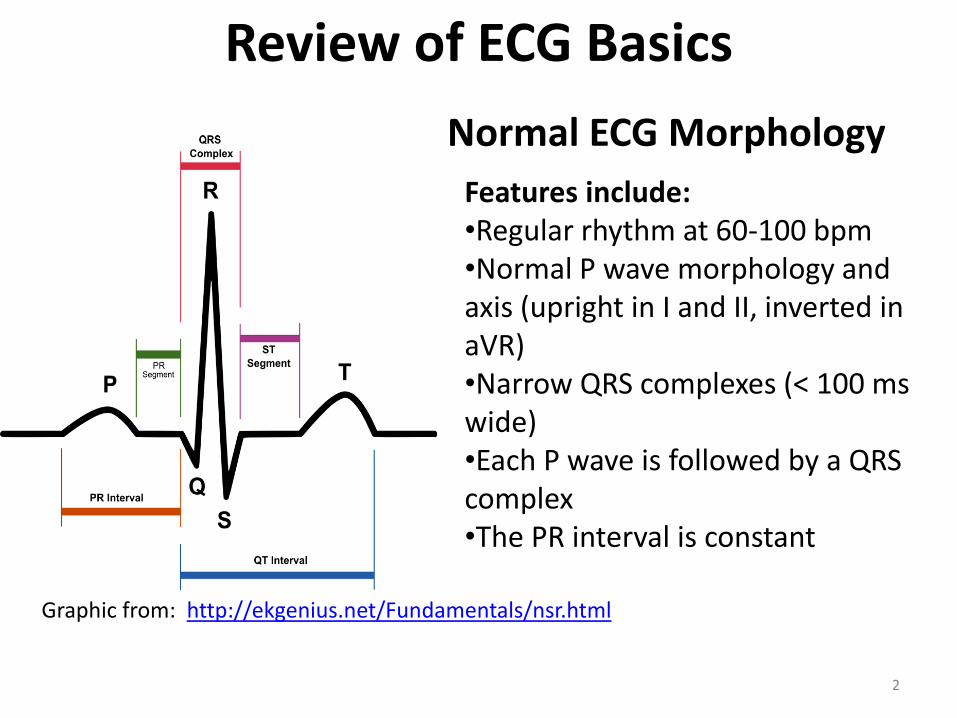
Graphic from: http://ekgenius.net/Fundamentals/nsr.html
Features include: •Regular rhythm at 60-100 bpm •Normal P wave morphology and axis (upright in I and II, inverted in aVR) •Narrow QRS complexes (< 100 ms wide) •Each P wave is followed by a QRS complex •The PR interval is constant
2
Review of ECG Basics
Normal ECG Morphology
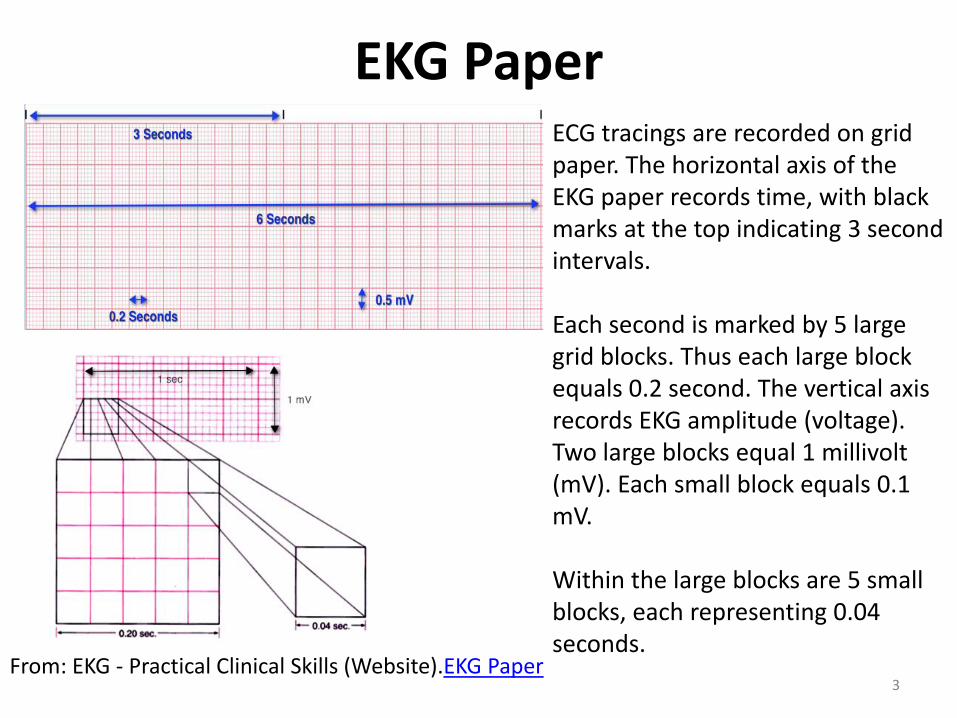
EKG Paper
3 From: EKG - Practical Clinical Skills (Website).EKG Paper
ECG tracings are recorded on grid paper. The horizontal axis of the EKG paper records time, with black marks at the top indicating 3 second intervals. Each second is marked by 5 large grid blocks. Thus each large block equals 0.2 second. The vertical axis records EKG amplitude (voltage). Two large blocks equal 1 millivolt (mV). Each small block equals 0.1 mV. Within the large blocks are 5 small blocks, each representing 0.04 seconds.
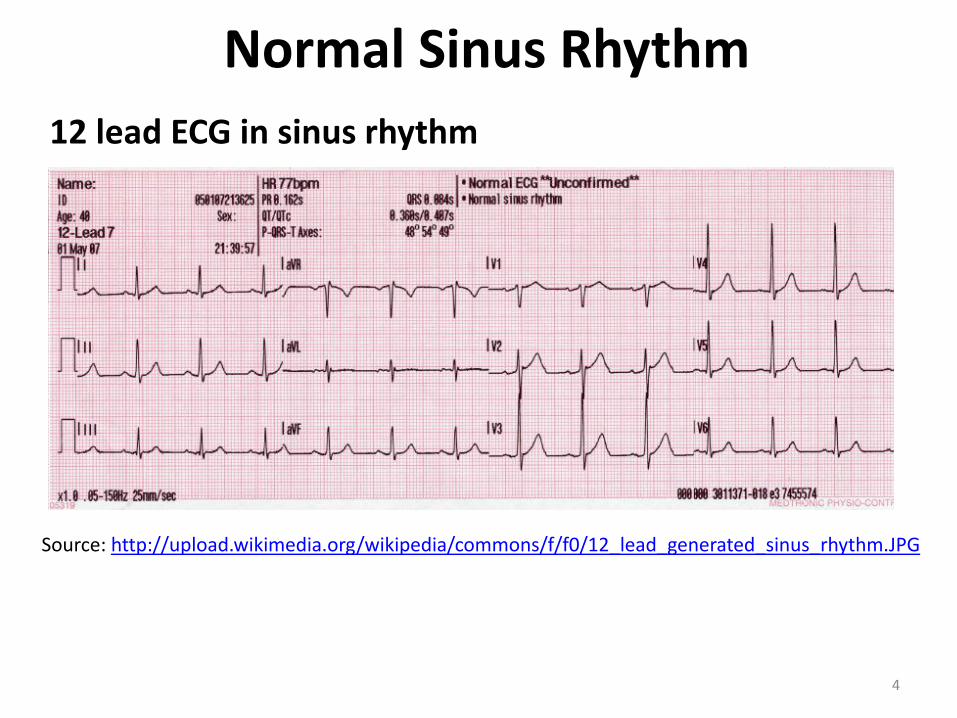
Normal Sinus Rhythm
12 lead ECG in sinus rhythm
Source: http://upload.wikimedia.org/wikipedia/commons/f/f0/12_lead_generated_sinus_rhythm.JPG
4
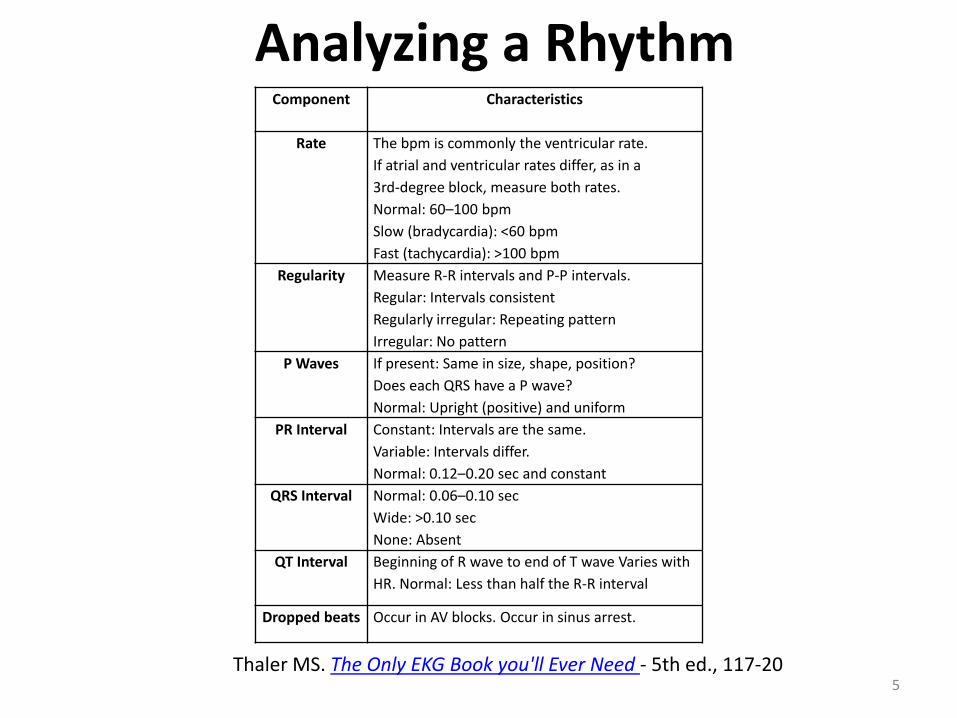
Analyzing a Rhythm
5
Component Characteristics
Rate The bpm is commonly the ventricular rate.
If atrial and ventricular rates differ, as in a
3rd-degree block, measure both rates.
Normal: 60–100 bpm
Slow (bradycardia): <60 bpm
Fast (tachycardia): >100 bpm
Regularity Measure R-R intervals and P-P intervals.
Regular: Intervals consistent
Regularly irregular: Repeating pattern
Irregular: No pattern
P Waves If present: Same in size, shape, position?
Does each QRS have a P wave?
Normal: Upright (positive) and uniform
PR Interval Constant: Intervals are the same.
Variable: Intervals differ.
Normal: 0.12–0.20 sec and constant
QRS Interval Normal: 0.06–0.10 sec
Wide: >0.10 sec
None: Absent
QT Interval Beginning of R wave to end of T wave Varies with
HR. Normal: Less than half the R-R interval
Dropped beats Occur in AV blocks. Occur in sinus arrest.
Thaler MS. The Only EKG Book you'll Ever Need - 5th ed., 117-20

Basic Rhythm Analysis
• Rate – too fast or too slow?
• Rhythm – regular or irregular?
• Is there a normal looking QRS? Is it wide or narrow?
• Are P waves present?
• What is the relationship of the P waves to the QRS complex?
6
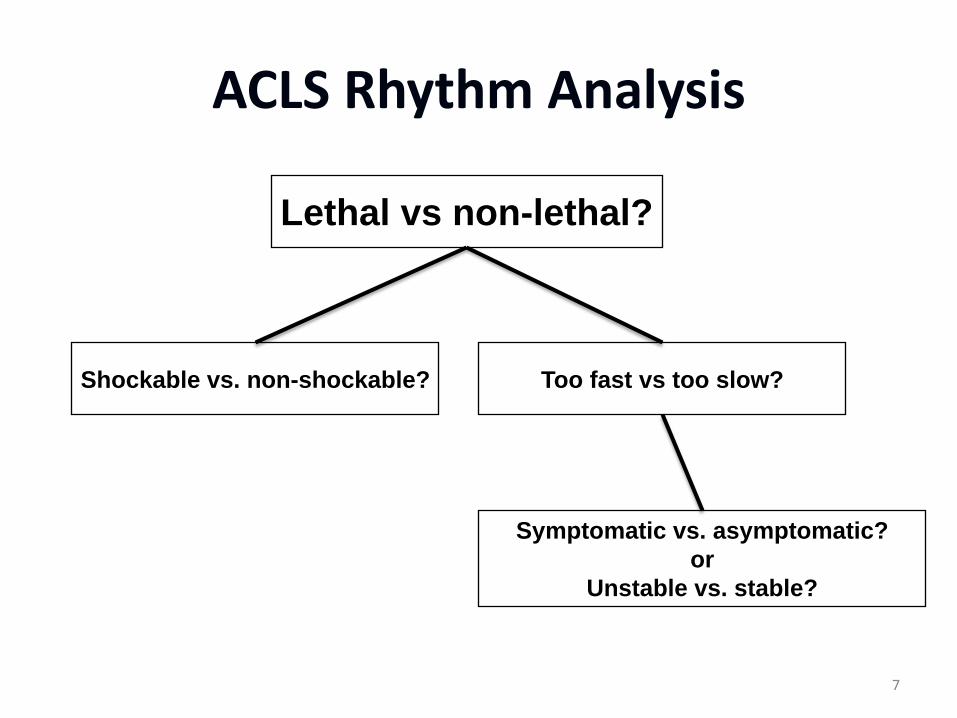
ACLS Rhythm Analysis
Lethal vs non-lethal?
Shockable vs. non-shockable? Too fast vs too slow?
Symptomatic vs. asymptomatic?
or
Unstable vs. stable?
7
Hemodynamically Significant Rhythm =Symptomatic or Unstable
8
•Clinically, most important parameter to assess in any patient with a cardiac dysrhythmia is rhythm hemodynamically "significant"
•This holds true regardless of whether rhythm in question is slow or fast
•A rhythm is "hemodynamically" significant IF it produces signs or symptoms of concern as a direct result of the rate
N.B. Is the Patient Stable? How to Assess:

Signs and Symptoms of Concern (“Think hypoperfusion of heart-brains-kidneys”)
9
•Signs of Concern --include hypotension (i.e., systolic BP ≤80-90 mm Hg); shock; heart failure/pulmonary edema; and/or acute infarction •Symptoms of Concern -- include chest pain; shortness of breath; and/or impaired mental status
Hemodynamic stability VT or SVT
10
•The definition of hemodynamic stability is equally applicable for supraventricular tachyarrhythmias (SVT) as it is for ventricular tachycardia (VT)
•patient with tachycardia who is symptomatic (i.e., hypotensive; short of breath; confused) is in need of immediate synchronized cardioversion — regardless of whether rhythm is VT or SVT
•In contrast – a trial of medical therapy is justified IF the patient is stable!
See SVT and Tachycardia Notes.pdf
TO SUMMARIZE “Symptomatic = unstable”
• Any abnormal rhythm that produces signs or symptoms of hypoperfusion – Chest Pain/ischemic EKG changes
– Shortness of Breath
– Decreased level of consciousness
– Syncope/pre-syncope
– Hypotension
– Shock - decreased Urine output, cool extremities, etc.
– Pulmonary Congestion/CHF
11
Treat the patient not the monitor!!!!!!
“Sometimes you just have to be there"
12
For example
• despite a systolic BP of 75 mm Hg-we would not
necessarily cardiovert a patient with tachycardia who was
otherwise tolerating the rhythm well (i.e., without chest
pain, dyspnea, or confusion).
•Some patients may remain stable for hours (or even
days) despite being in sustained VT
Again Treat the patient not the monitor!!!!
Lethal Rhythms
• Shockable (Defibrillation)
–Ventricular fibrillation
–Pulseless ventricular tachycardia
• Non-shockable
–Asystole
–Pulseless electrical activity (PEA)
13
Non-Lethal Rhythms
• Too fast (tachycardias)
– Sinus
– Supraventricular (including a-fib/flutter)
– Ventricular
• Too slow (bradycardias)
– Sinus
– Heart block (1°, 2°, 3° AV block)
14
N.B. May have the potential to become lethal rhythms if not treated appropriately
The following outlined ECG strips will be reviewed OUTLINE: • SINUS RHYTHMS SINUS RHYTHM SINUS BRADYCARDIA SINUS ARREST SINUS TACHYCARDIA • ATRIAL RHYTHMS SUPRAVENTRICULAR TACHYCARDIA ATRIAL FIBRILLATION ATRIAL FLUTTER • VENTRICULAR RHYTHM VENTRICULAR TACHYCARDIA VENTRICULAR FIBRILLATION • ATRIOVENTRICULAR BLOCKS FIRST DEGREE HEART BLOCK SECOND DEGREE HEART BLOCK TYPE 1 SECOND DEGREE HEART BLOCK TYPE 2 THIRD DEGREE HEART BLOCK
For full rationale see respective disorders at http://emedicine.medscape.com/cardiology
15
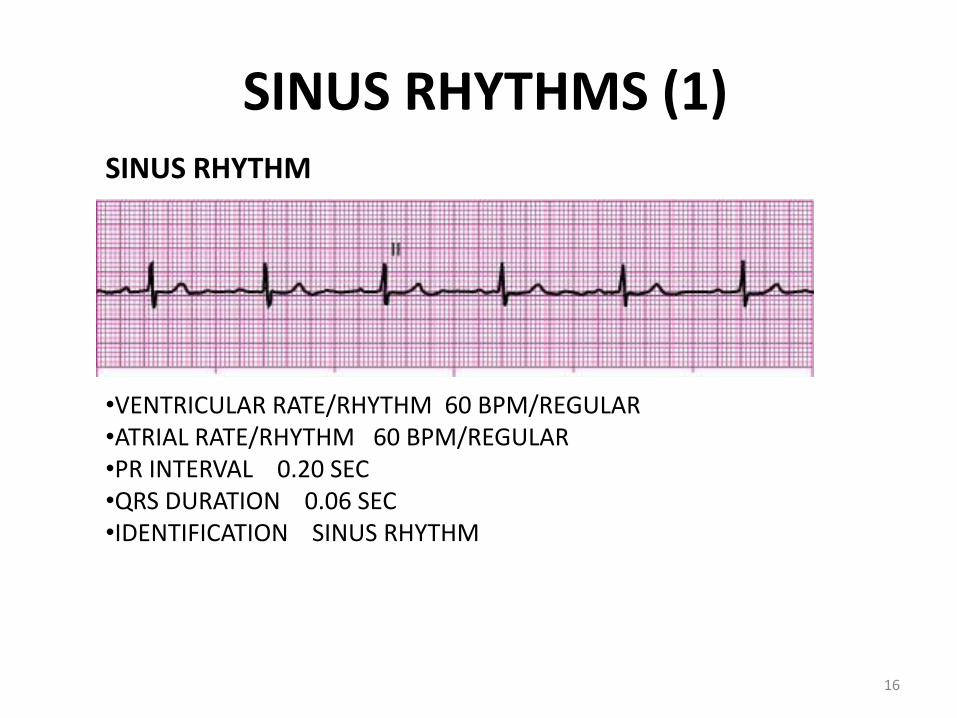
SINUS RHYTHMS (1) SINUS RHYTHM
•VENTRICULAR RATE/RHYTHM 60 BPM/REGULAR •ATRIAL RATE/RHYTHM 60 BPM/REGULAR •PR INTERVAL 0.20 SEC •QRS DURATION 0.06 SEC •IDENTIFICATION SINUS RHYTHM
16
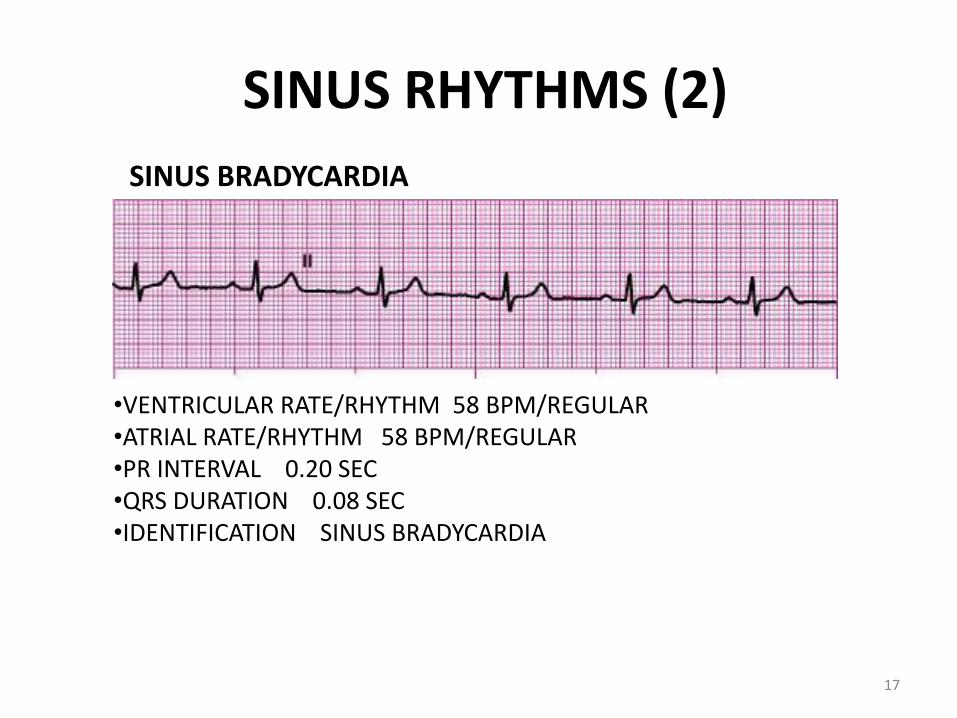
SINUS RHYTHMS (2)
SINUS BRADYCARDIA
•VENTRICULAR RATE/RHYTHM 58 BPM/REGULAR •ATRIAL RATE/RHYTHM 58 BPM/REGULAR •PR INTERVAL 0.20 SEC •QRS DURATION 0.08 SEC •IDENTIFICATION SINUS BRADYCARDIA
17
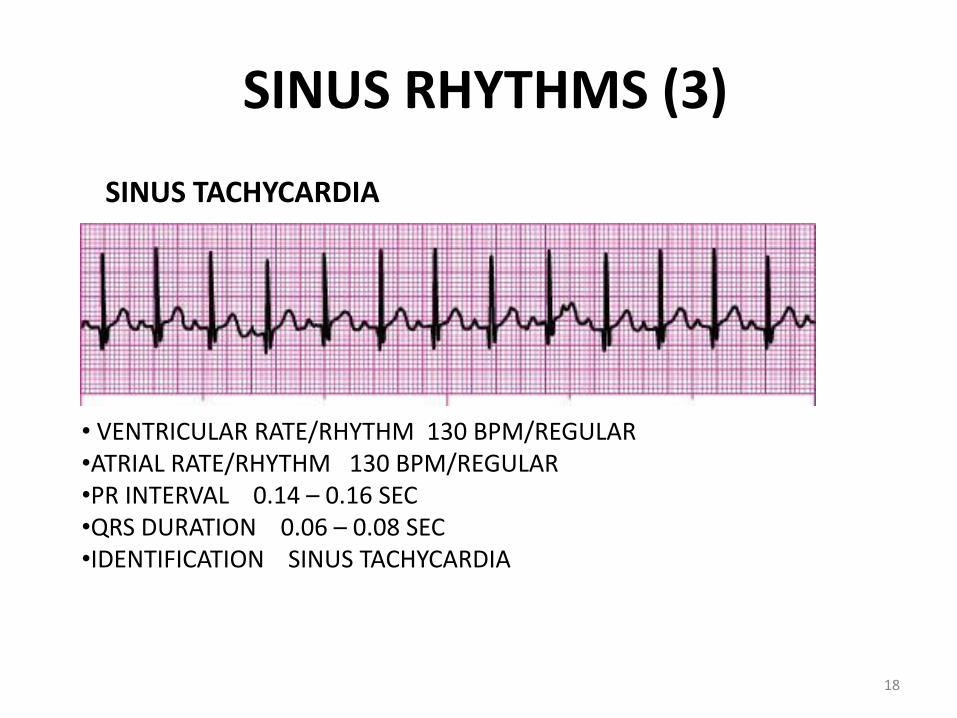
SINUS RHYTHMS (3)
SINUS TACHYCARDIA
• VENTRICULAR RATE/RHYTHM 130 BPM/REGULAR •ATRIAL RATE/RHYTHM 130 BPM/REGULAR •PR INTERVAL 0.14 – 0.16 SEC •QRS DURATION 0.06 – 0.08 SEC •IDENTIFICATION SINUS TACHYCARDIA
18
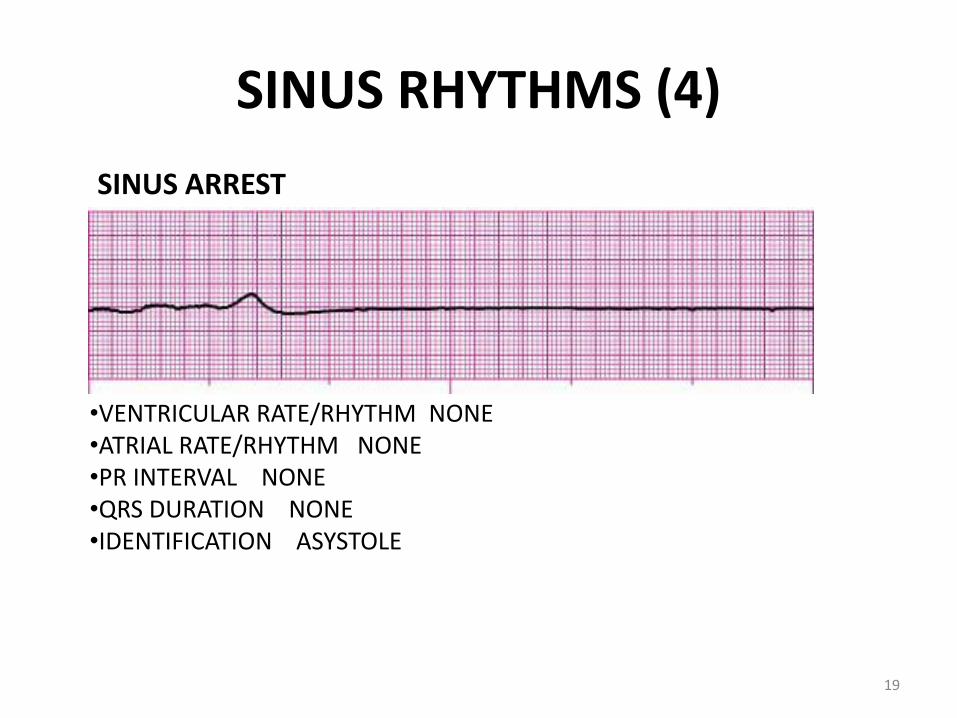
SINUS RHYTHMS (4)
SINUS ARREST
•VENTRICULAR RATE/RHYTHM NONE •ATRIAL RATE/RHYTHM NONE •PR INTERVAL NONE •QRS DURATION NONE •IDENTIFICATION ASYSTOLE
19
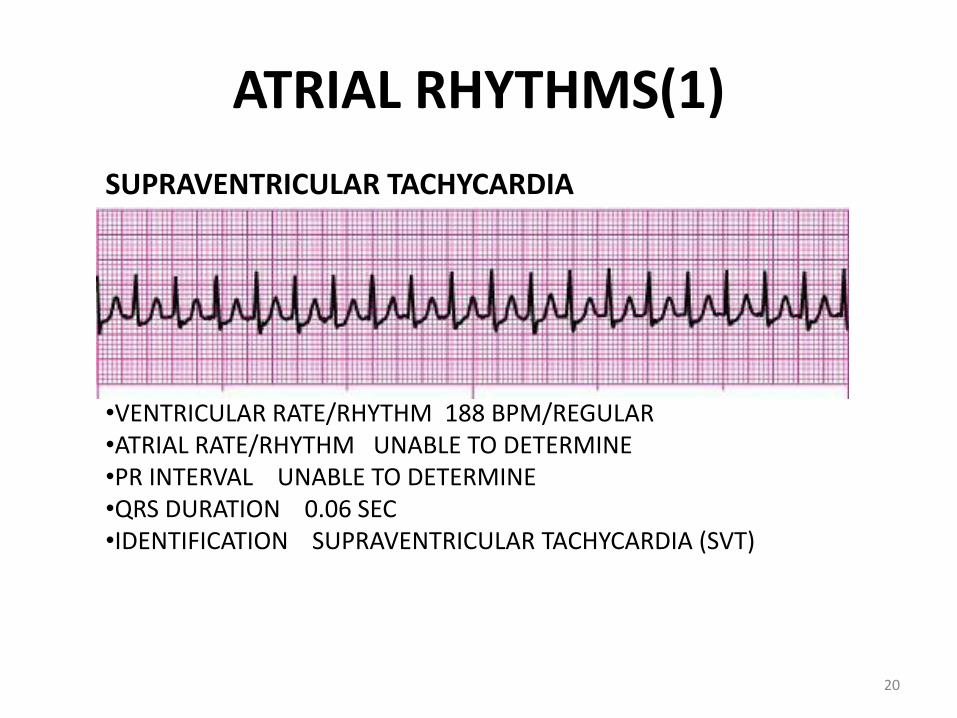
ATRIAL RHYTHMS(1)
SUPRAVENTRICULAR TACHYCARDIA
•VENTRICULAR RATE/RHYTHM 188 BPM/REGULAR •ATRIAL RATE/RHYTHM UNABLE TO DETERMINE •PR INTERVAL UNABLE TO DETERMINE •QRS DURATION 0.06 SEC •IDENTIFICATION SUPRAVENTRICULAR TACHYCARDIA (SVT)
20
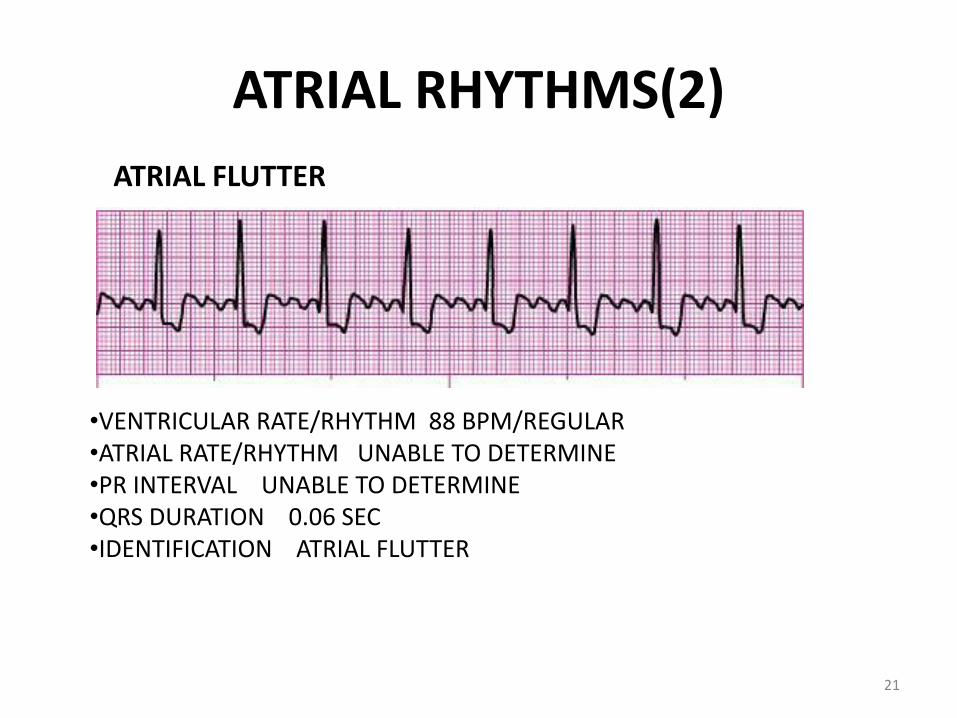
ATRIAL RHYTHMS(2)
ATRIAL FLUTTER
•VENTRICULAR RATE/RHYTHM 88 BPM/REGULAR •ATRIAL RATE/RHYTHM UNABLE TO DETERMINE •PR INTERVAL UNABLE TO DETERMINE •QRS DURATION 0.06 SEC •IDENTIFICATION ATRIAL FLUTTER
21
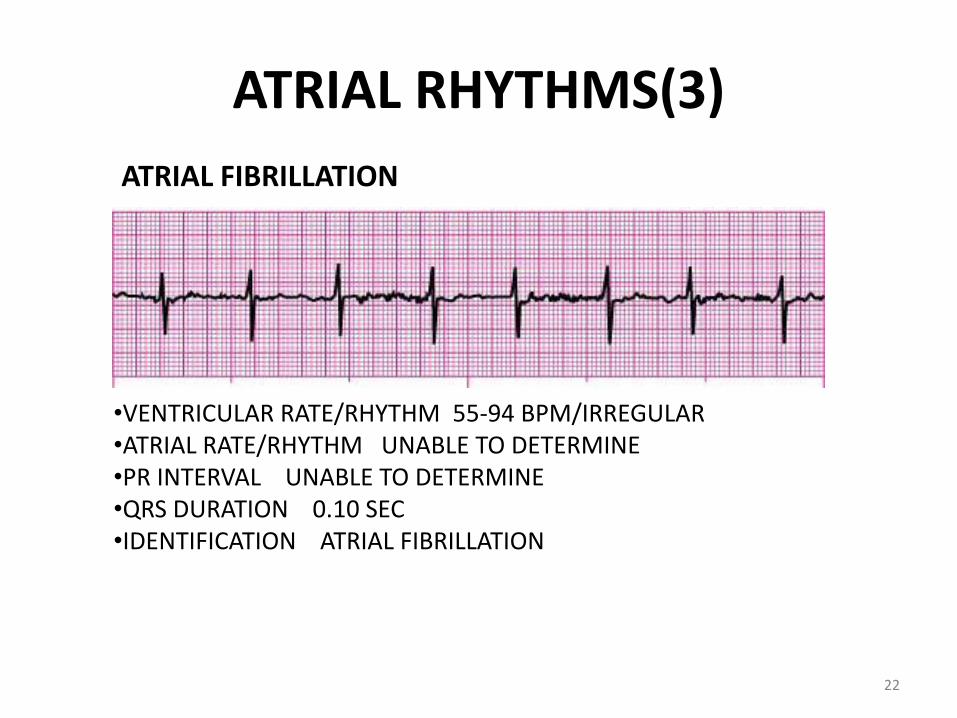
ATRIAL RHYTHMS(3)
ATRIAL FIBRILLATION
•VENTRICULAR RATE/RHYTHM 55-94 BPM/IRREGULAR •ATRIAL RATE/RHYTHM UNABLE TO DETERMINE •PR INTERVAL UNABLE TO DETERMINE •QRS DURATION 0.10 SEC •IDENTIFICATION ATRIAL FIBRILLATION
22
VENTRICULAR RHYTHMS(1)
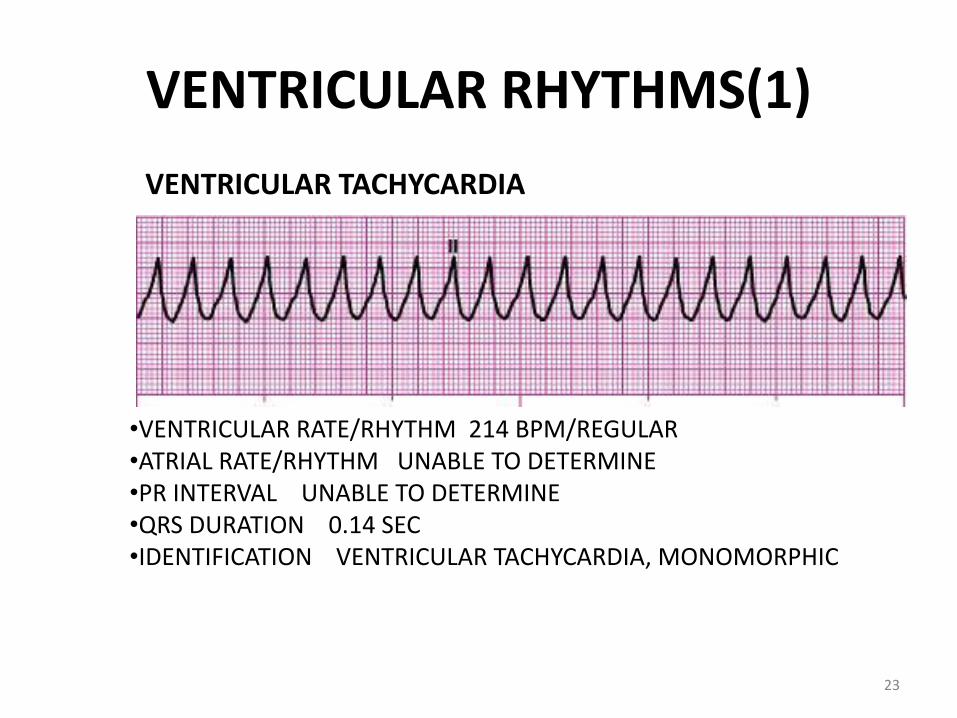
VENTRICULAR TACHYCARDIA
•VENTRICULAR RATE/RHYTHM 214 BPM/REGULAR •ATRIAL RATE/RHYTHM UNABLE TO DETERMINE •PR INTERVAL UNABLE TO DETERMINE •QRS DURATION 0.14 SEC •IDENTIFICATION VENTRICULAR TACHYCARDIA, MONOMORPHIC
23
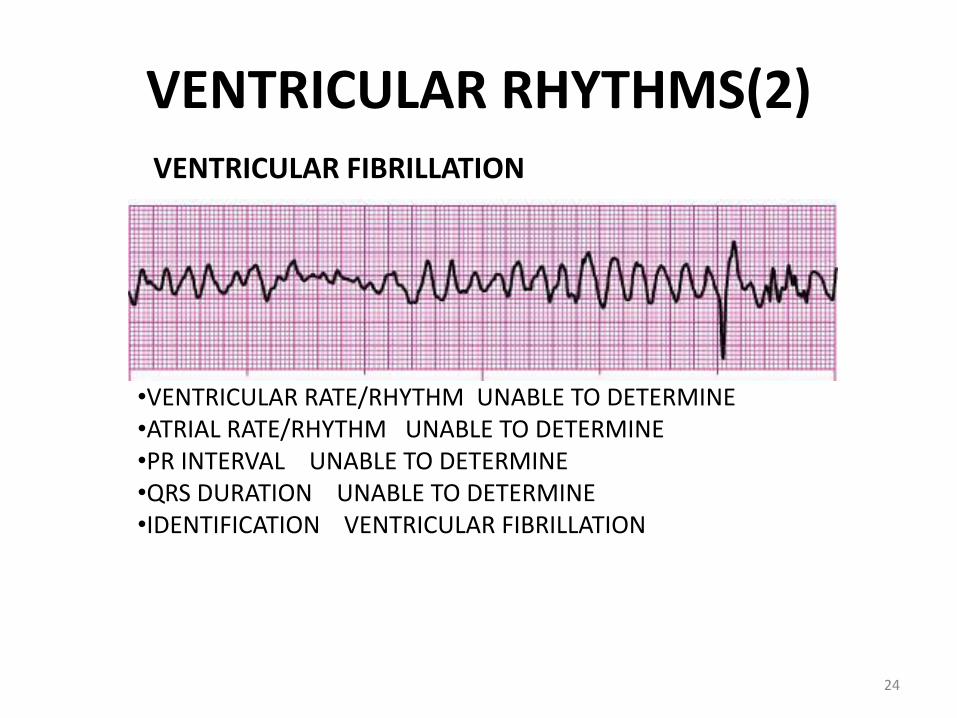
VENTRICULAR RHYTHMS(2) VENTRICULAR FIBRILLATION
•VENTRICULAR RATE/RHYTHM UNABLE TO DETERMINE •ATRIAL RATE/RHYTHM UNABLE TO DETERMINE •PR INTERVAL UNABLE TO DETERMINE •QRS DURATION UNABLE TO DETERMINE •IDENTIFICATION VENTRICULAR FIBRILLATION
24
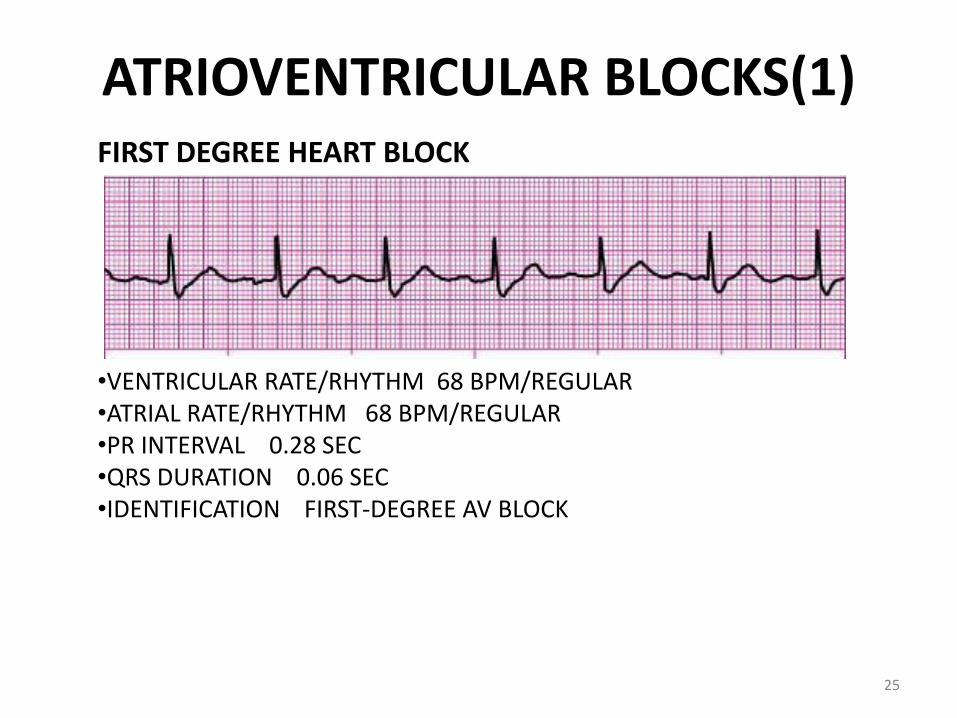
ATRIOVENTRICULAR BLOCKS(1) FIRST DEGREE HEART BLOCK
•VENTRICULAR RATE/RHYTHM 68 BPM/REGULAR •ATRIAL RATE/RHYTHM 68 BPM/REGULAR •PR INTERVAL 0.28 SEC •QRS DURATION 0.06 SEC •IDENTIFICATION FIRST-DEGREE AV BLOCK
25
ATRIOVENTRICULAR BLOCKS(2)
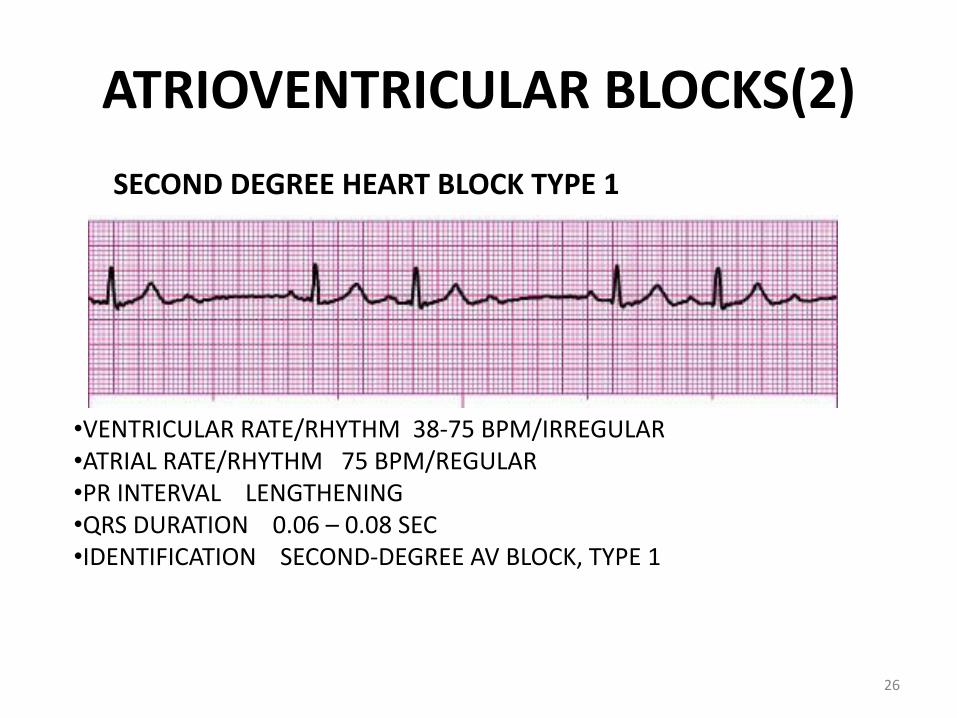
SECOND DEGREE HEART BLOCK TYPE 1
•VENTRICULAR RATE/RHYTHM 38-75 BPM/IRREGULAR •ATRIAL RATE/RHYTHM 75 BPM/REGULAR •PR INTERVAL LENGTHENING •QRS DURATION 0.06 – 0.08 SEC •IDENTIFICATION SECOND-DEGREE AV BLOCK, TYPE 1
26
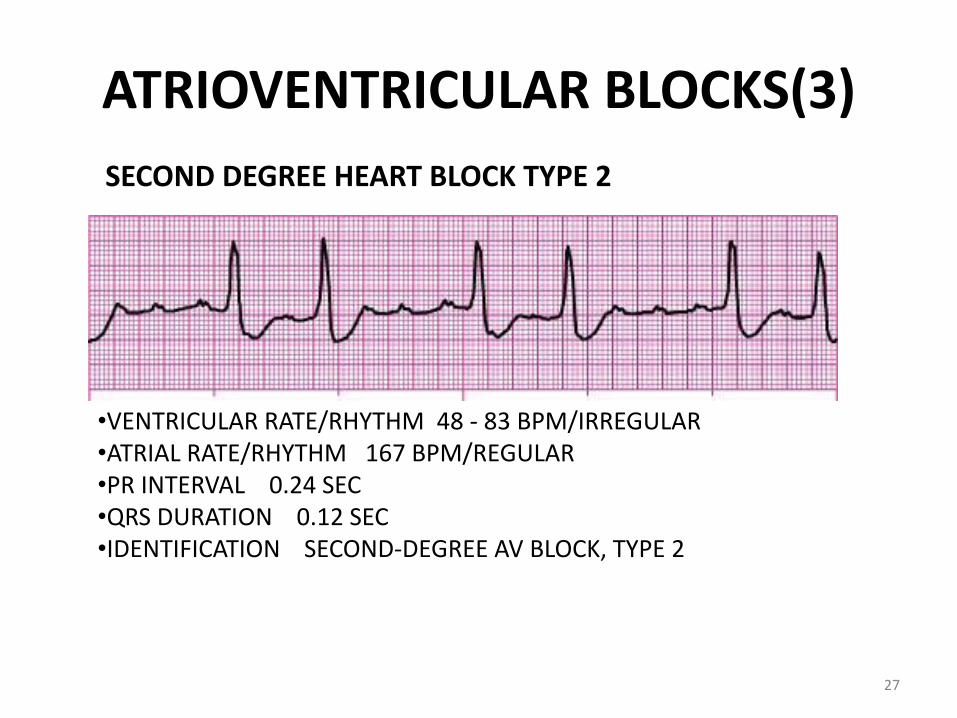
ATRIOVENTRICULAR BLOCKS(3)
SECOND DEGREE HEART BLOCK TYPE 2
•VENTRICULAR RATE/RHYTHM 48 - 83 BPM/IRREGULAR •ATRIAL RATE/RHYTHM 167 BPM/REGULAR •PR INTERVAL 0.24 SEC •QRS DURATION 0.12 SEC •IDENTIFICATION SECOND-DEGREE AV BLOCK, TYPE 2
27
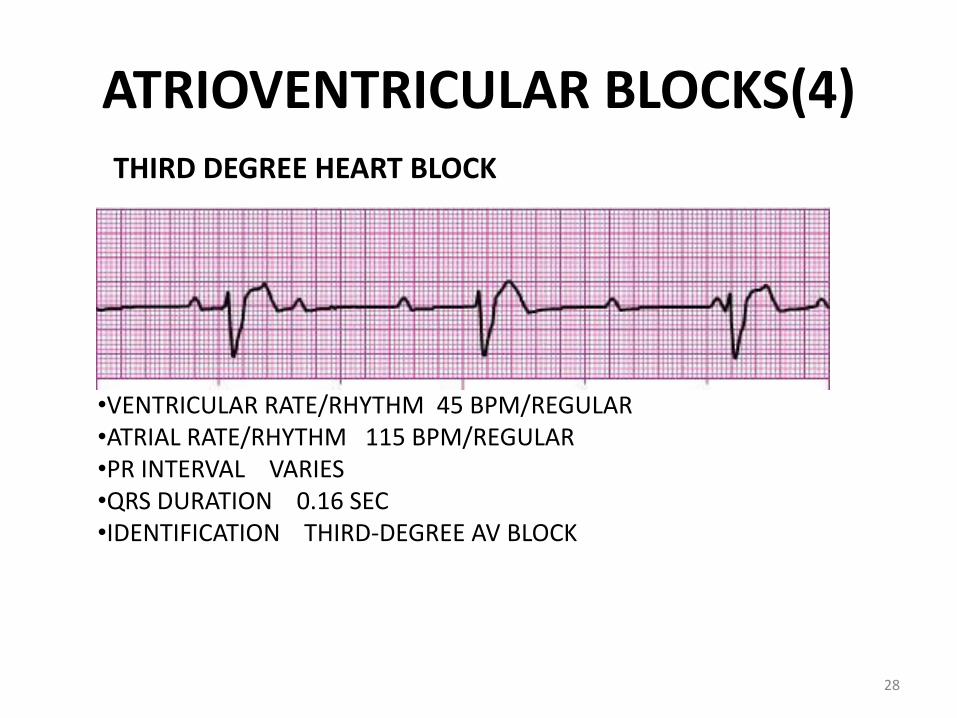
ATRIOVENTRICULAR BLOCKS(4) THIRD DEGREE HEART BLOCK
•VENTRICULAR RATE/RHYTHM 45 BPM/REGULAR •ATRIAL RATE/RHYTHM 115 BPM/REGULAR •PR INTERVAL VARIES •QRS DURATION 0.16 SEC •IDENTIFICATION THIRD-DEGREE AV BLOCK
28
Name the rhythm & its management …
ACLS Case Scenarios Supplement to Part I- ECG STRIP INTERPRETATION
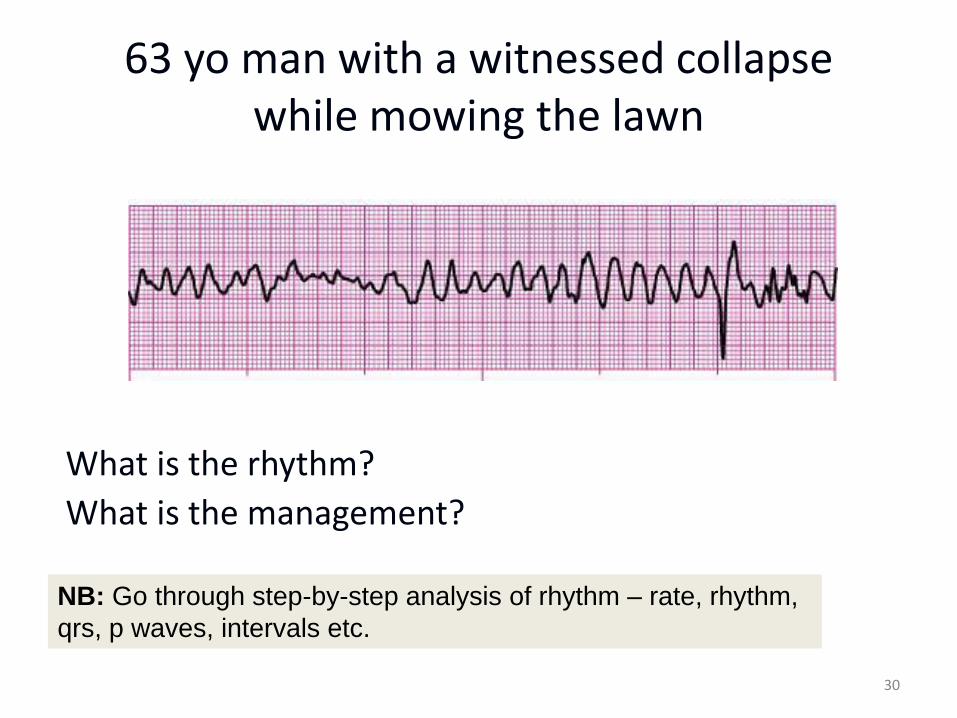
63 yo man with a witnessed collapse while mowing the lawn
What is the rhythm?
What is the management?
30
NB: Go through step-by-step analysis of rhythm – rate, rhythm,
qrs, p waves, intervals etc.
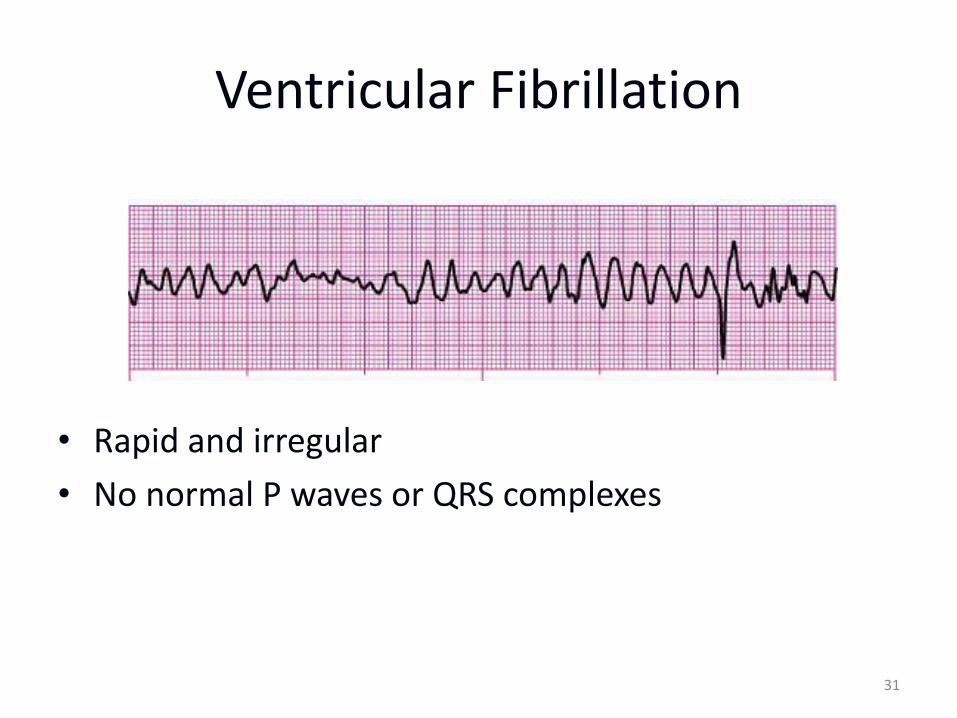
Ventricular Fibrillation
• Rapid and irregular
• No normal P waves or QRS complexes
31
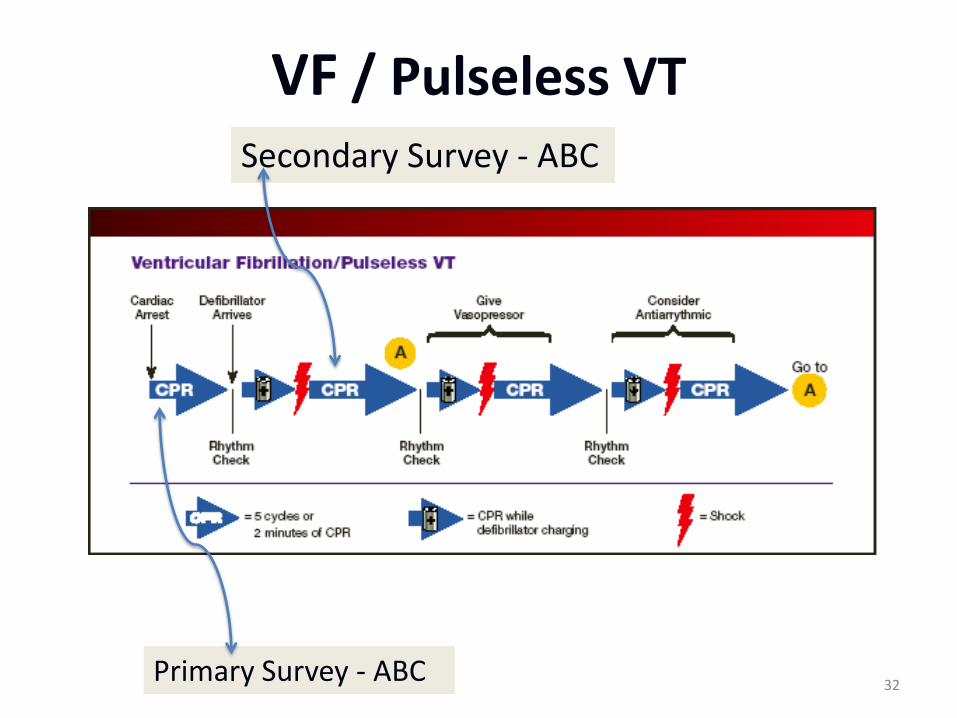
VF / Pulseless VT
Primary Survey - ABC
Secondary Survey - ABC
32
ACLS Algorithm • Primary Survey
• Shock – 360 J
• Secondary Survey
• Vasopressor - Epi or Vasopressin IV
• Shock 360J
• Antiarrhythmic – Amiodarone, Lidocaine or Magnesium Sulfate IV
• Shock 360J
33
NB: Don’t forget CPR in between shocks – don’t stop CPR for anything
except to assess patient (no longer than 10 seconds) or shock resume CPR
*immediately* after the shock for 5 cycles *without* checking a rhythm until
after 5 cycles of 30/2 CPR
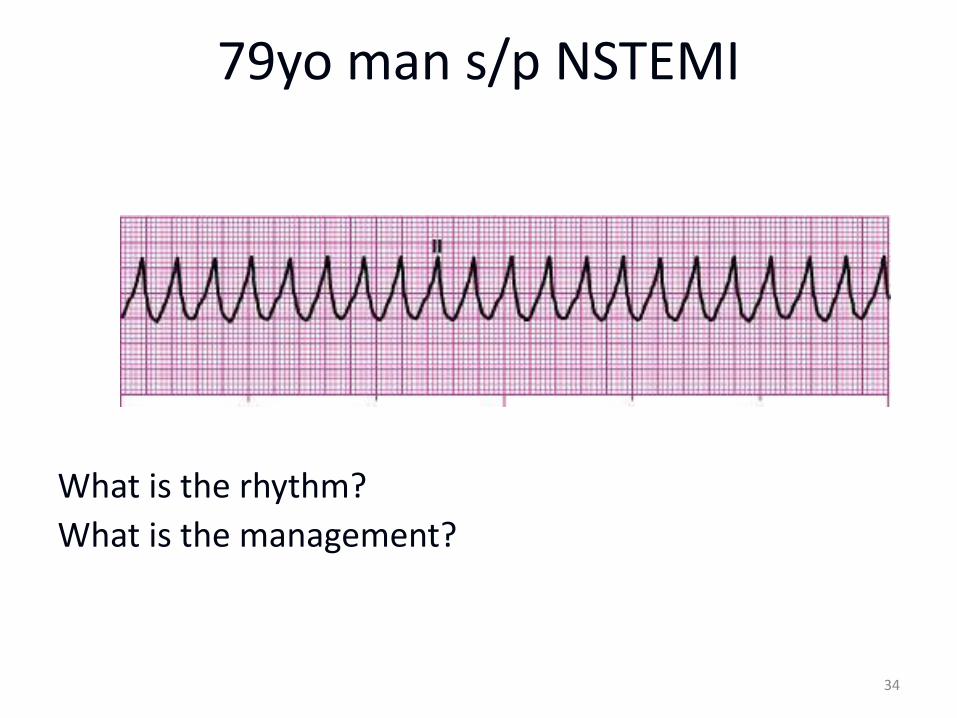
79yo man s/p NSTEMI
What is the rhythm?
What is the management?
34
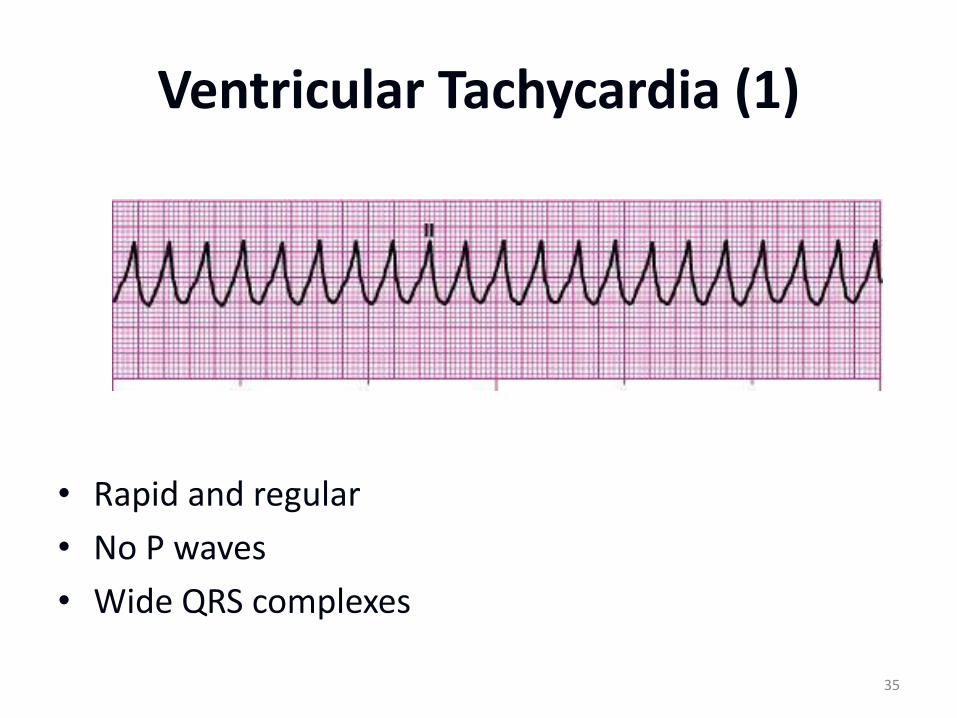
Ventricular Tachycardia (1)
• Rapid and regular
• No P waves
• Wide QRS complexes
35
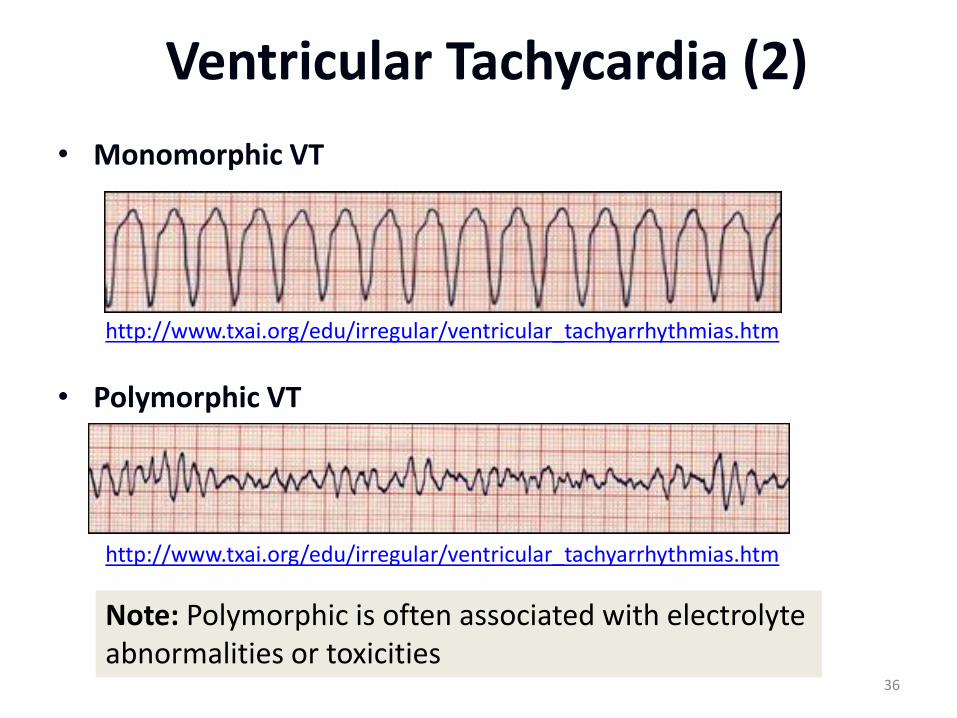
Ventricular Tachycardia (2)
• Monomorphic VT
• Polymorphic VT
36
Note: Polymorphic is often associated with electrolyte abnormalities or toxicities
http://www.txai.org/edu/irregular/ventricular_tachyarrhythmias.htm
http://www.txai.org/edu/irregular/ventricular_tachyarrhythmias.htm
Ventricular Tachycardia (3)
• Assume any wide complex tachycardia is VT until proven otherwise – SVT with aberrant conduction may also have wide
QRS complexes
• Attempt to establish the diagnosis – Ischemia risk and VT go together
37
Treatment of VT (1)
• If pulseless - follow VF algorithm
• If stable try anti-arrhythmics
– Amiodarone
– Lidocaine
– Procainamide?
• If patient has a pulse, but is unstable or not responding to meds - shock
38
Treatment of VT (2)
• Anti-arrhythmics are also pro-arrhythmic
• One antiarrhythmic may help, more than one may harm
• Anti-arrhythmics can impair an already impaired heart
• Electrical cardioversion should be the second intervention of choice
39
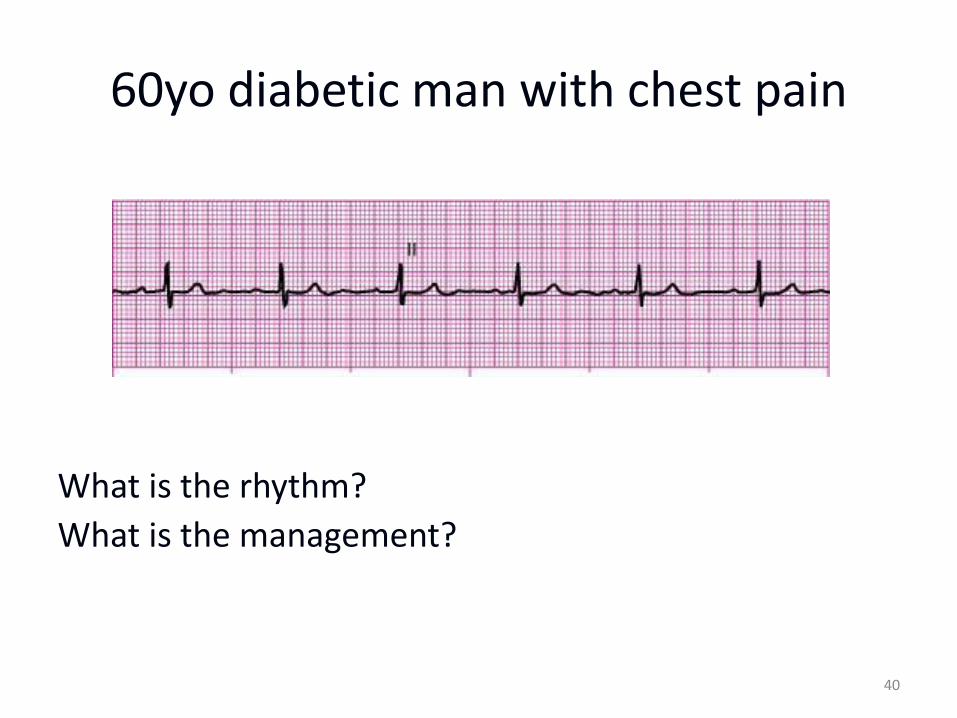
60yo diabetic man with chest pain
What is the rhythm?
What is the management?
40

Normal Sinus Rhythm
• Regular rate and rhythm
• Normal P waves and QRS
• Evaluate for cause of chest pain and monitor for change in rhythm
41
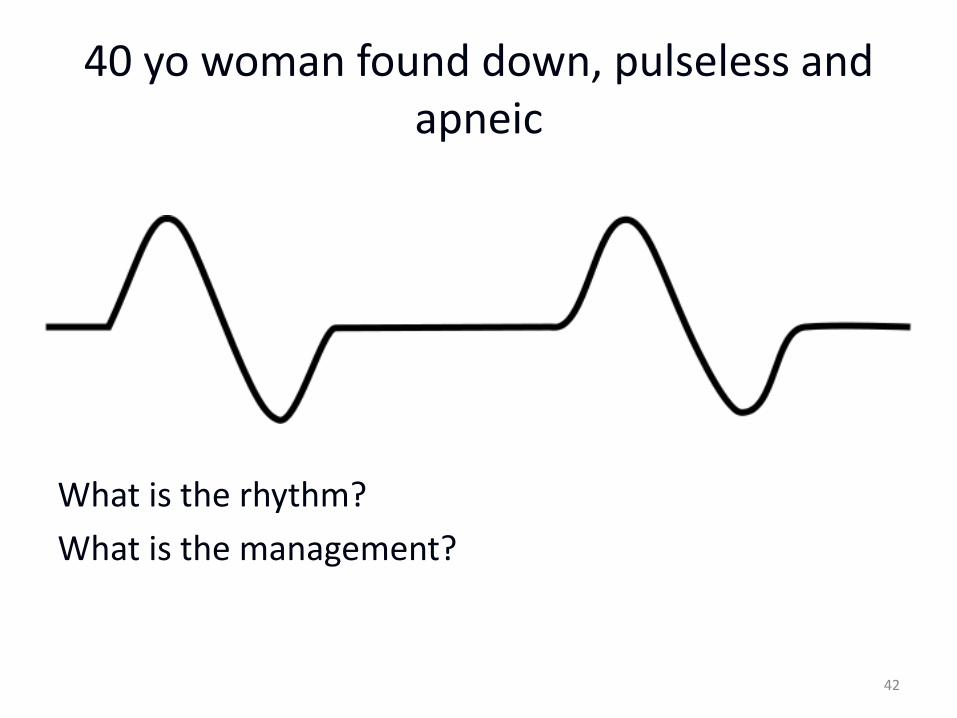
40 yo woman found down, pulseless and apneic
What is the rhythm?
What is the management?
42
Pulseless Electrical Activity (PEA)
• Any organized (or semi-organized) electrical activity in a patient without a detectable pulse
• Non-perfusing
• Treat the patient NOT the monitor
• Find and treat the cause!!!!!
43
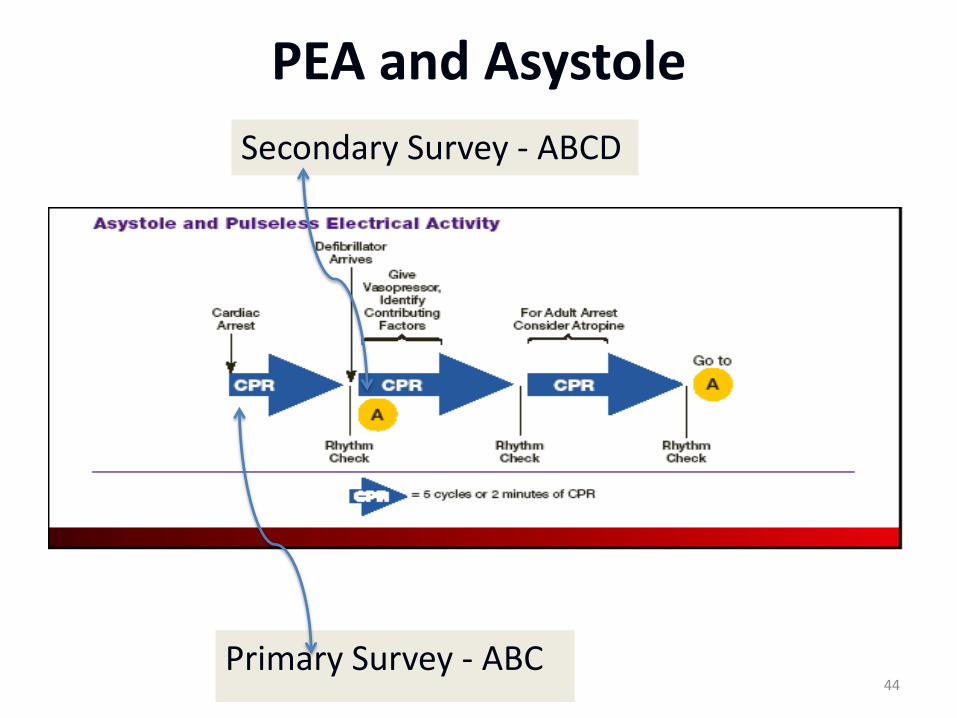
PEA and Asystole
Secondary Survey - ABCD
Primary Survey - ABC 44

PEA
Atropine 1 mg IVP
if PEA is slow
Epinephrine 1 mg IVP
repeat every 3-5 minutes
Search for and Treat Causes
Secondary Survey
Primary Survey
45
Find and Treat the Cause
• Remember Non-shockable rhythms include:
–Asystole
–Pulseless electrical activity (PEA)
– The most effective treatment is to find and fix the underlying problem
46
Causes of PEA?
• #1 cause of PEA in adults is hypovolemia
• #1 cause in children is hypoxia/respiratory arrest
• Other causes? The H’s and T’s (Next Slide)
47
The H’s and T’s
• Hypovolemia
• Hypoxia
• Hydrogen ion (acidosis)
• Hyper-/hypokalemia
• Hypothermia
• Hypoglycemia (rare)
• Toxins
• Tamponade
• Tension pneumothorax
• Thrombosis (coronary or pulmonary)
• Trauma
48
N.B. There are now actually 6 H’s – hypoglycemia added on AHA
guidelines BUT only a few anecdotal reports of actually causing PEA
and usually in association with underlying chronic cardiac dysfunction
(severe heart failure)
Treat the H’s and T’s
• Hypovolemia – Volume – IVF, PRBC’s
• Hypoxia – Oxygenate/Ventilate
• Hydrogen ion (acidosis) – Sodium bicarbonate – Hyperventilation
• Hyper-/hypokalemia – Sodium bicarbonate – Insulin/glucose – Calcium
• Hypothermia – Warm -- invasive
• Hypoglycemia – Dextrose
• Toxins – Check levels – Charcoal – Antidotes
• Tamponade – pericardiocentesis
• Tension pneumothorax – Needle decompression – Tube thoracostomy
• Thrombosis (coronary or pulmonary) – Thrombolytics – OR/cath lab
• Trauma 49
Busy slide – the point is to TREAT whatever the problem is
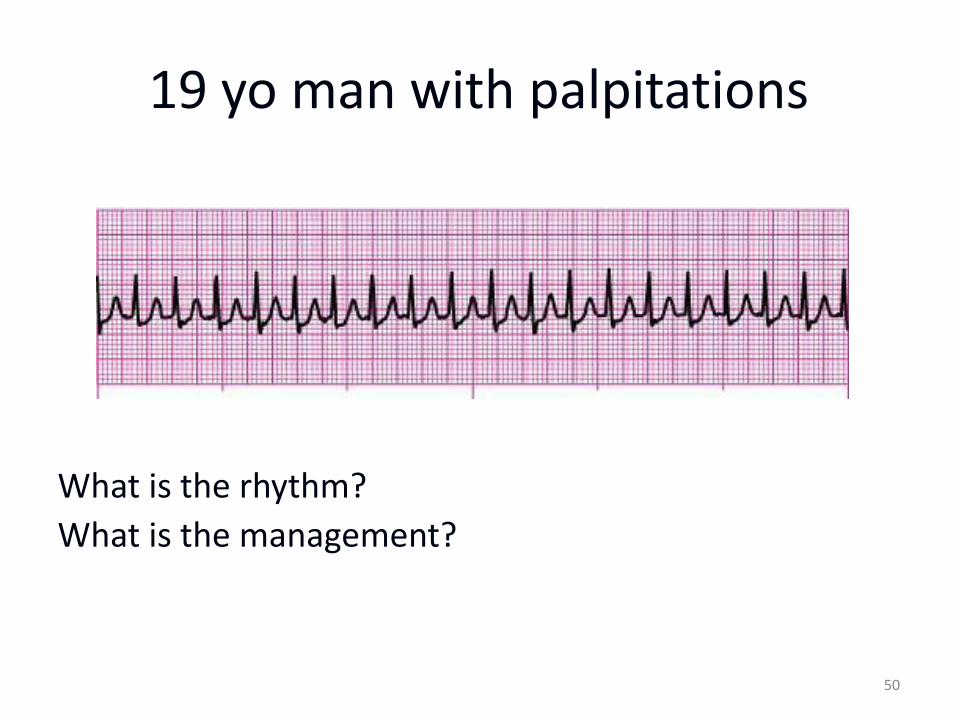
19 yo man with palpitations
What is the rhythm?
What is the management?
50

Supraventricular Tachycardia
• Rapid (usually 150-250 bpm) and regular
• P waves cannot be positively identified
• QRS narrow
51
Note: P waves either merge with preceding T waves or are buried in QRS complexes so the differentiation between atrial and junctional tachycardia is impossible. P waves buried in T wave or QRS or not present – can’t differentiate supraventricular from junctional – most are supraventricular
Treatment of Stable SVT (1) • Consider vagal maneuvers
– Carotid sinus massage
– Valsalva
– Eyeball massage
– Ice water to face
– Digital rectal exam
• Adenosine
– 6 mg, 12 mg, 12 mg
52
NB: Carotid massage - Turn head, Locate maximal impulse of carotid artery. Massage up and down massage for 5-10 seconds. One side at a time. Do not do in someone you suspect carotid disease
Treatment of Unstable SVT (2)
• Electrical Cardioversion
• Cardioversion is not defibrillation
• Use defibrillator in “sync” mode
– prevents delivering energy in the wrong part of the cardiac cycle (R on T phenomenon)
53
NB: Heart is not fibrillating
Electrical Cardioversion (1)
• Energy level – somewhat controversial
• 100 J→200J→300J→360J
• Atrial flutter may convert with lower energy
– 50J
• For polymorphic VT – start with 200J
54
Electrical Cardioversion (2)
• Be prepared
– Patient on monitor, IV, Oxygen
– Suction ready and working
– Airway supplies ready
• Pre-medicate whenever possible
– Conscious sedation
– Electrical shocks are painful!
55
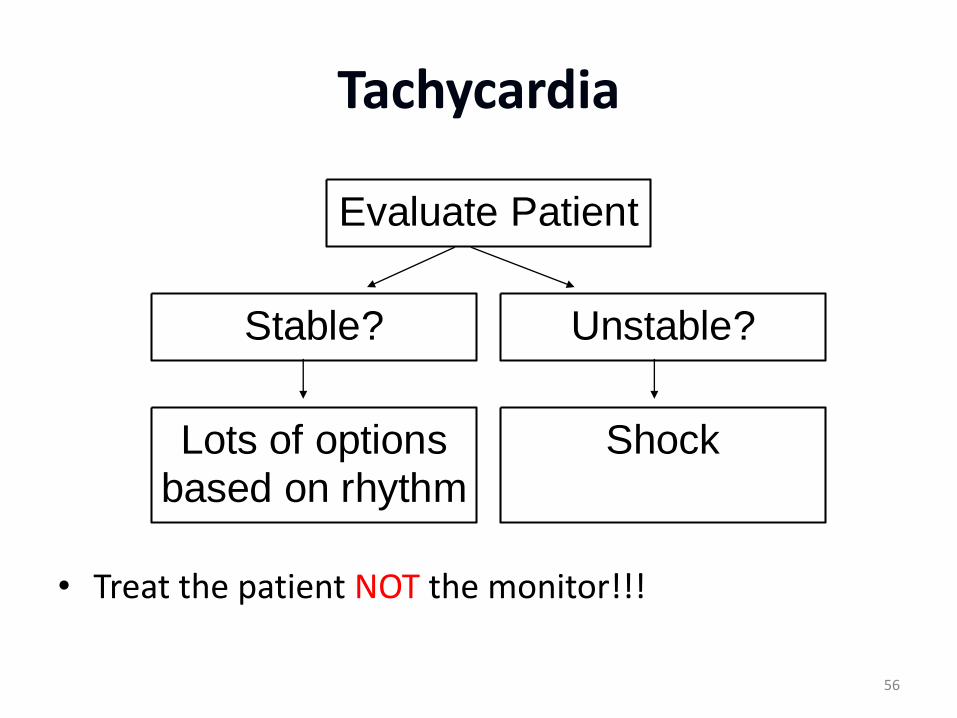
Tachycardia
Lots of optionsbased on rhythm
Stable?
Shock
Unstable?
Evaluate Patient
• Treat the patient NOT the monitor!!!
56
Stable Tachycardias
• Narrow complex?
– Regular rhythm
• Sinus tachycardia
• SVT
• AV nodal reentry
– Irregular rhythm
• Atrial fibrillation
• Atrial flutter
• Wide complex?
– Uncertain rhythm – assume VT
– Narrow complex tachycardia with aberrancy
– Ventricular tachycardia
• Monomorphic or polymorphic
57
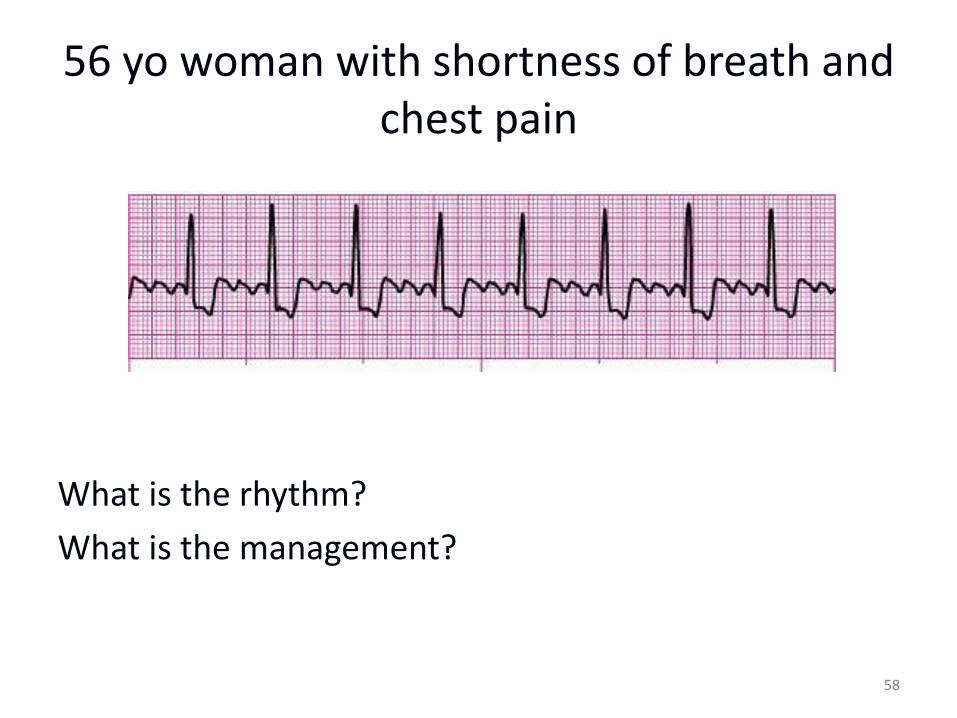
56 yo woman with shortness of breath and chest pain
What is the rhythm?
What is the management?
58
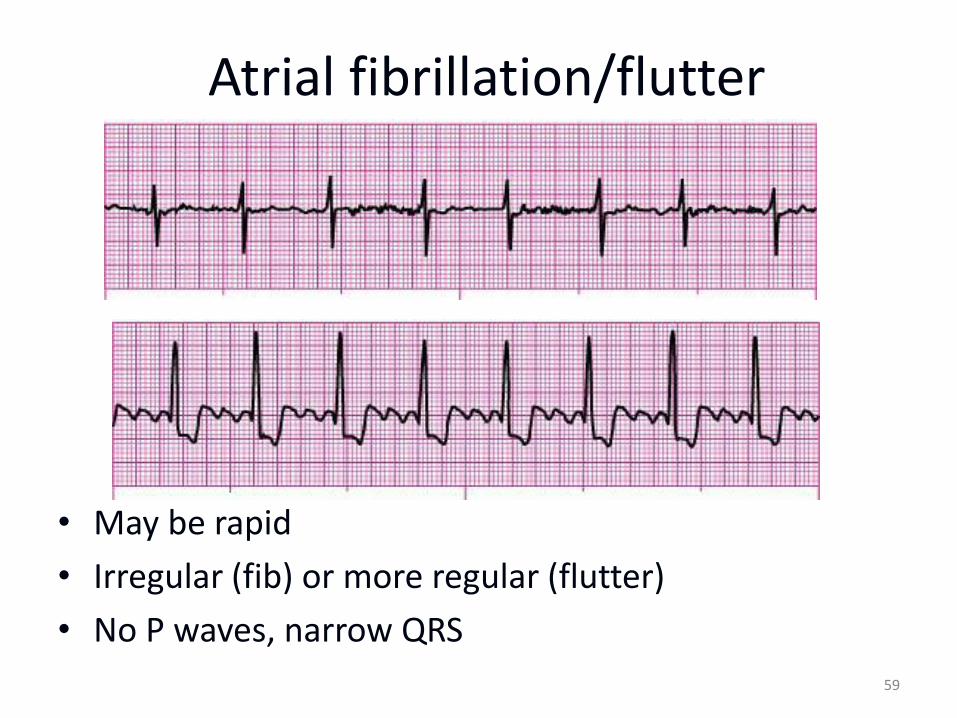
Atrial fibrillation/flutter
• May be rapid
• Irregular (fib) or more regular (flutter)
• No P waves, narrow QRS
59
Atrial fibrillation/flutter • Treatment based on patient’s clinical picture
– Unstable = Immediate electrical cardioversion
– Stable
• Control the rate
– Diltiazem
– Esmolol (not if EF < 40%)
– Digoxin
• Provide anticoagulation
• Treat the patient NOT the monitor!!!
60
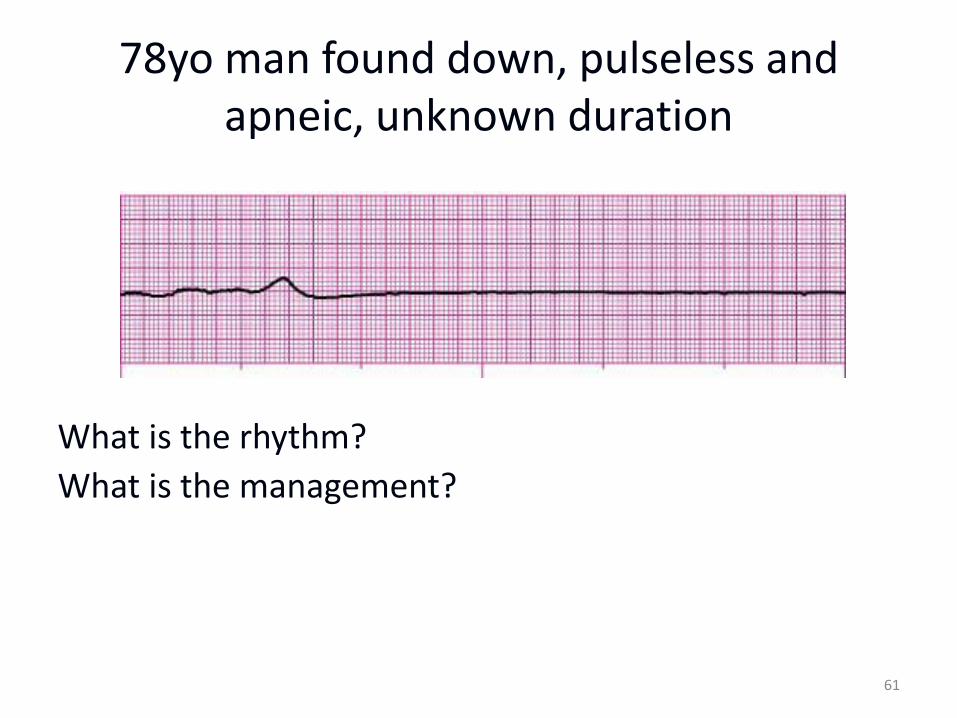
78yo man found down, pulseless and apneic, unknown duration
What is the rhythm?
What is the management?
61
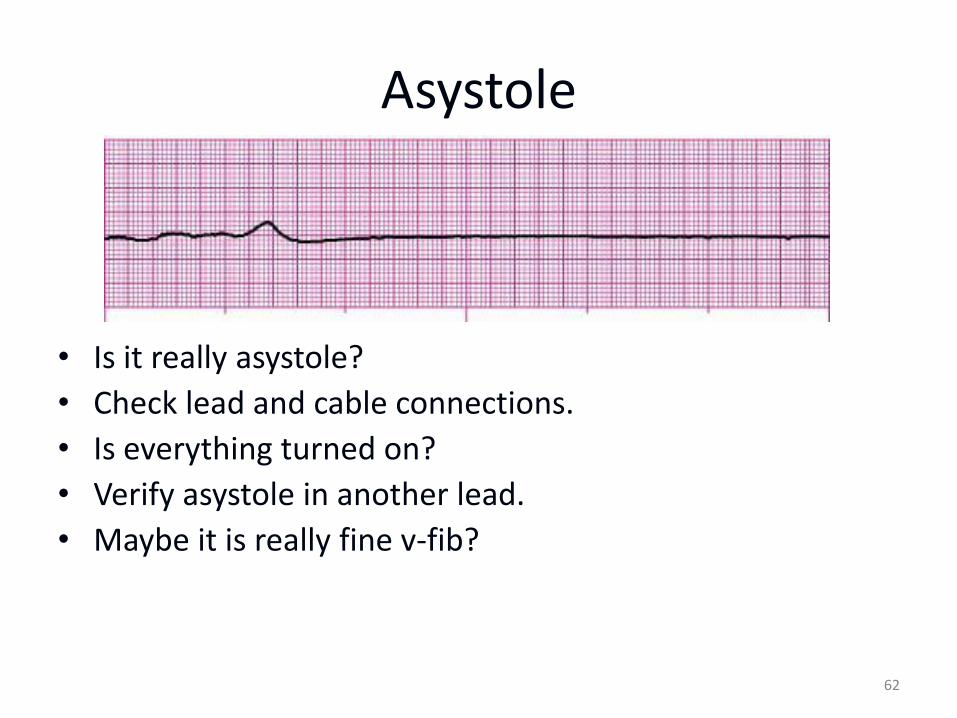
Asystole
• Is it really asystole?
• Check lead and cable connections.
• Is everything turned on?
• Verify asystole in another lead.
• Maybe it is really fine v-fib?
62
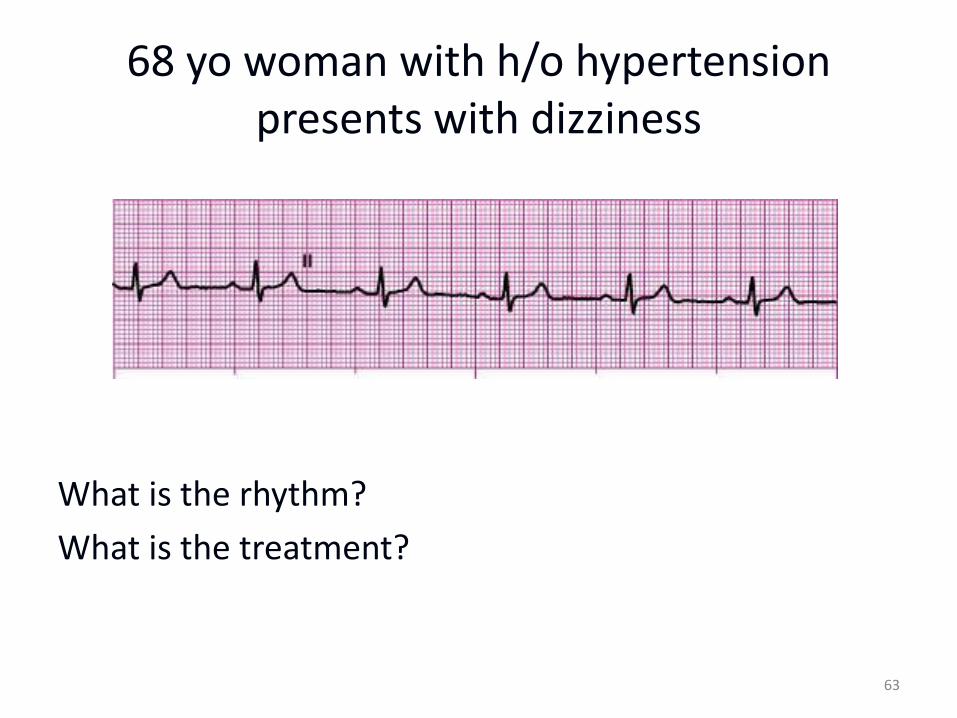
68 yo woman with h/o hypertension presents with dizziness
What is the rhythm?
What is the treatment?
63
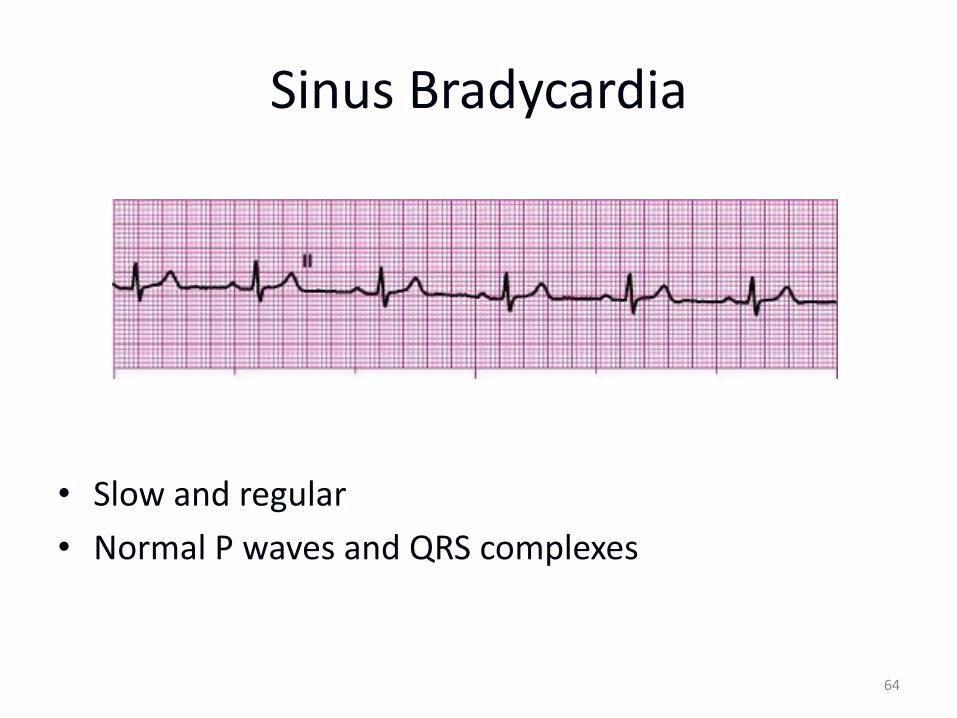
Sinus Bradycardia
• Slow and regular
• Normal P waves and QRS complexes
64
Bradycardias (1)
• Many possible causes
– Enhanced parasympathetic tone
– Increased ICP.
– Hypothyroidism
– Hypothermia
– Hyperkalemia
– Hypoglycemia
– Drug therapy
65
Bradycardias (2)
• Treat only symptomatic bradycardias
– Ask if the bradycardia causing the symptoms
• Recognize the red flag bradycardias
– Second degree type II block
– Third degree block
66
Transcutaneous pacing (1)
• Class I for all symptomatic bradycardias
• Always appropriate
• Doesn’t always work
• Technique – Attach pacer pads
– Set a rate to 80 bpm
– Turn up the juice (amps) until you get capture
• Painful – may need sedation / analgesia
67
Transvenous Pacing (2)
• Invasive
• Time-consuming to establish
• Skilled procedure
• Better long-term than transcutaneous
• May have better capture than transcutaneous pacing
68
Bradycardia Treatment
• Medications
–Vagolytic
• Atropine
–Adrenergic
• Epinephrine
• Dopamine
69
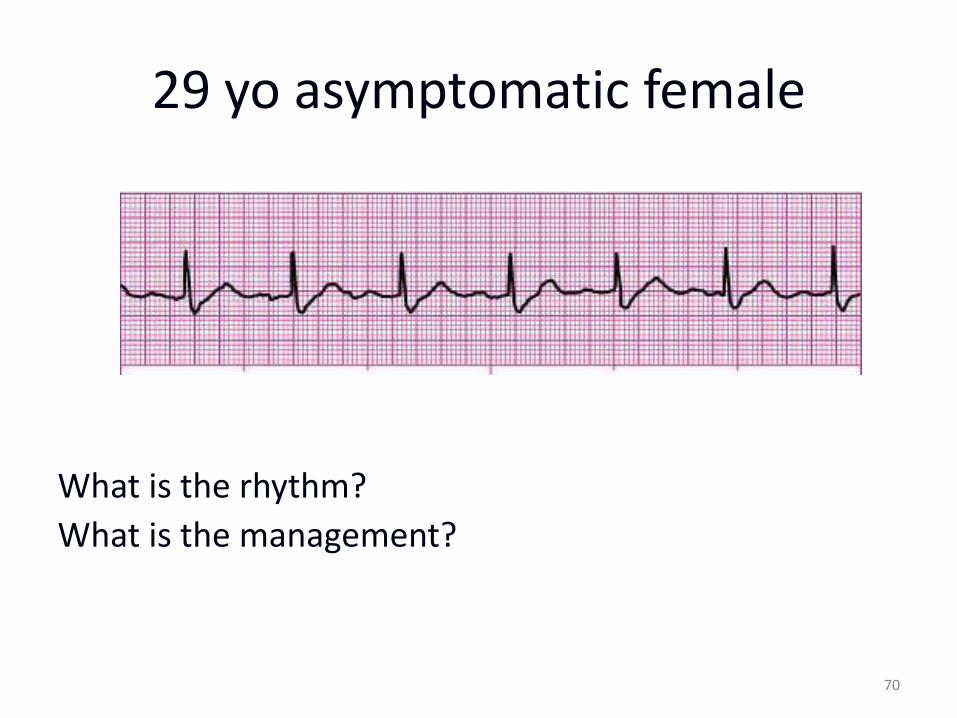
29 yo asymptomatic female
What is the rhythm?
What is the management?
70
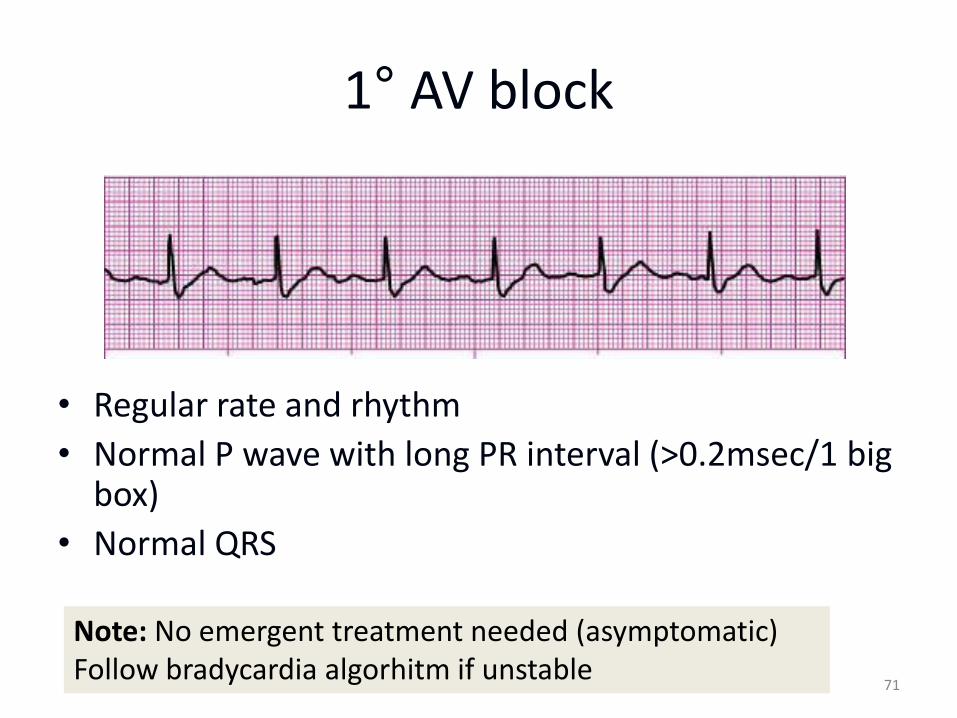
1° AV block
• Regular rate and rhythm
• Normal P wave with long PR interval (>0.2msec/1 big box)
• Normal QRS
71
Note: No emergent treatment needed (asymptomatic) Follow bradycardia algorhitm if unstable
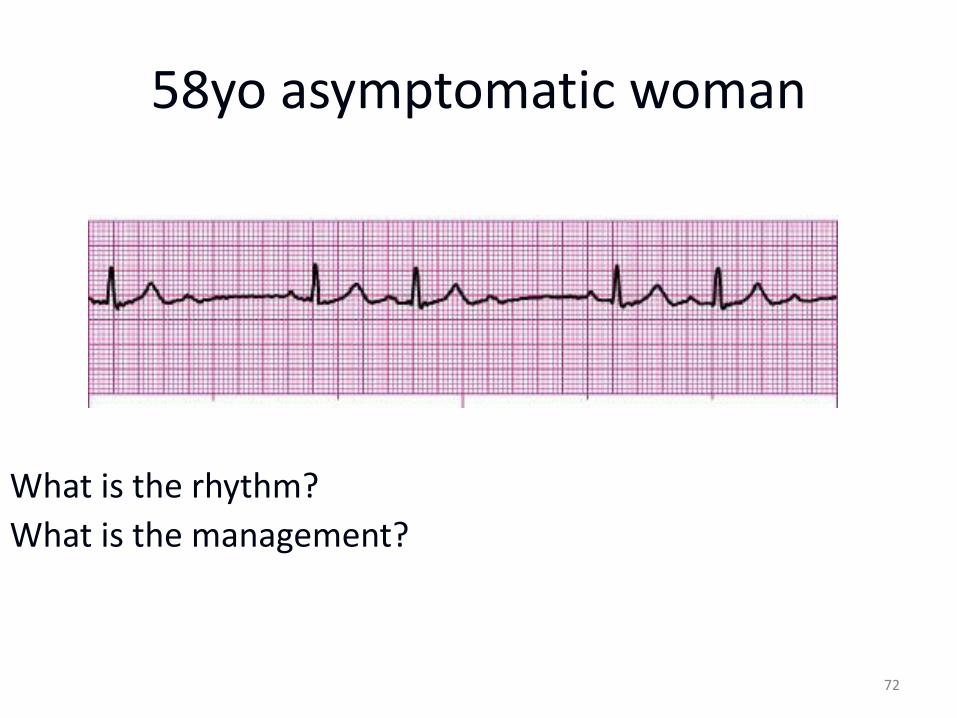
58yo asymptomatic woman
72
What is the rhythm?
What is the management?
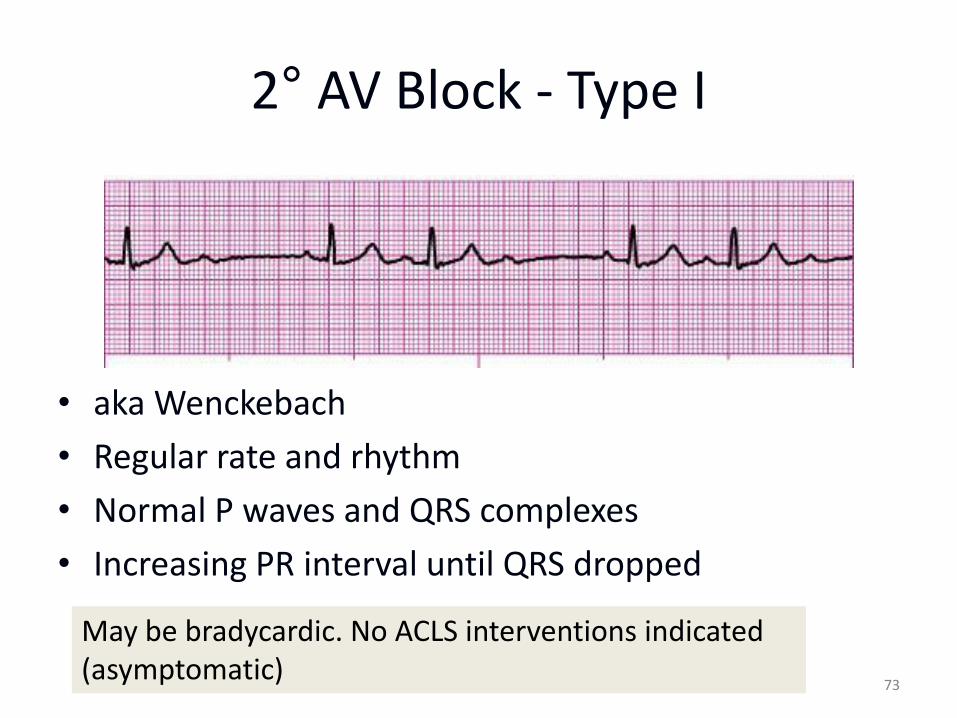
2° AV Block - Type I
• aka Wenckebach
• Regular rate and rhythm
• Normal P waves and QRS complexes
• Increasing PR interval until QRS dropped
73
May be bradycardic. No ACLS interventions indicated (asymptomatic)
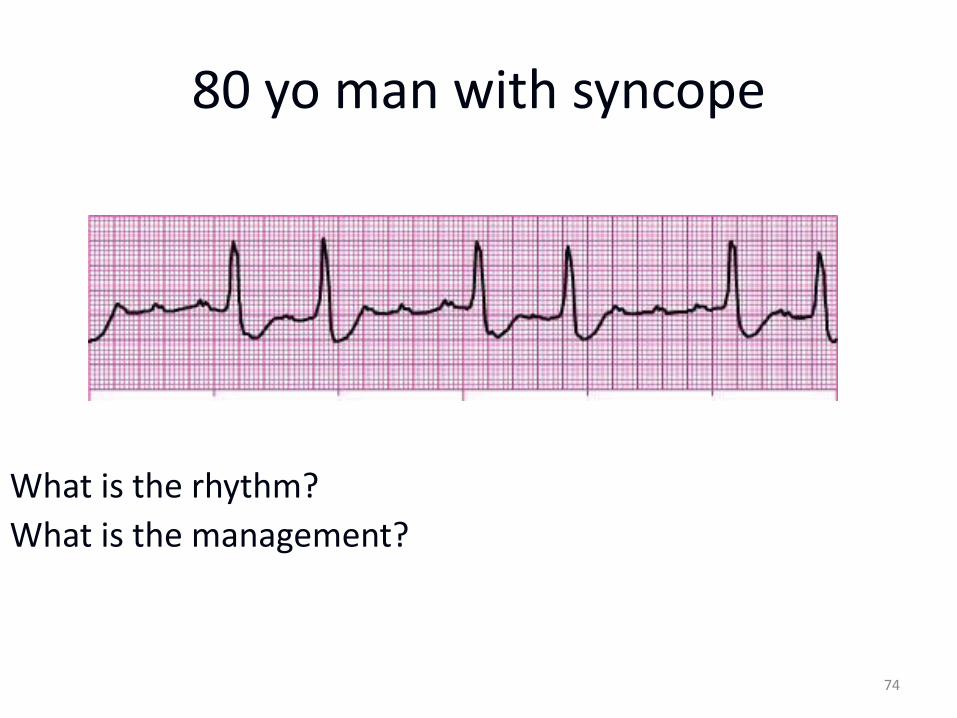
80 yo man with syncope
74
What is the rhythm?
What is the management?
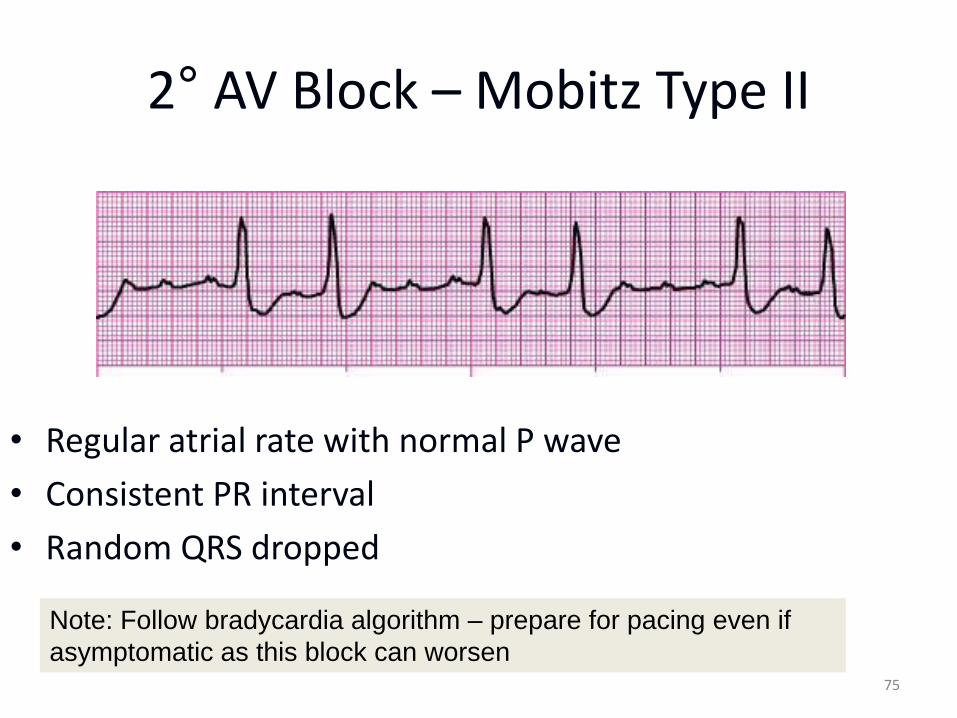
2° AV Block – Mobitz Type II
75
• Regular atrial rate with normal P wave
• Consistent PR interval
• Random QRS dropped
Note: Follow bradycardia algorithm – prepare for pacing even if
asymptomatic as this block can worsen
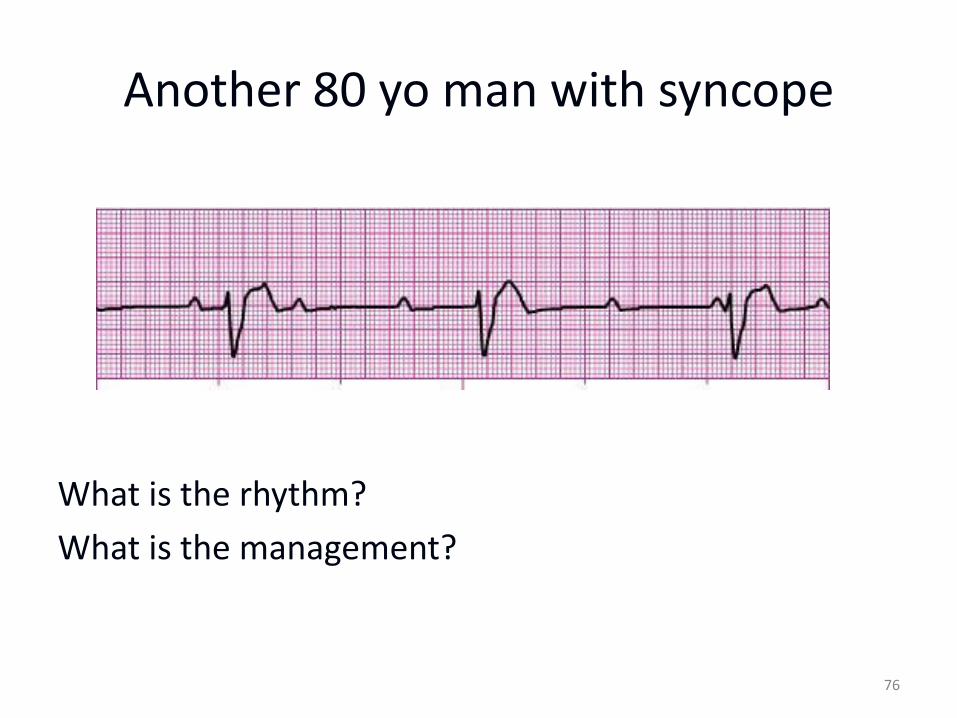
Another 80 yo man with syncope
What is the rhythm?
What is the management?
76
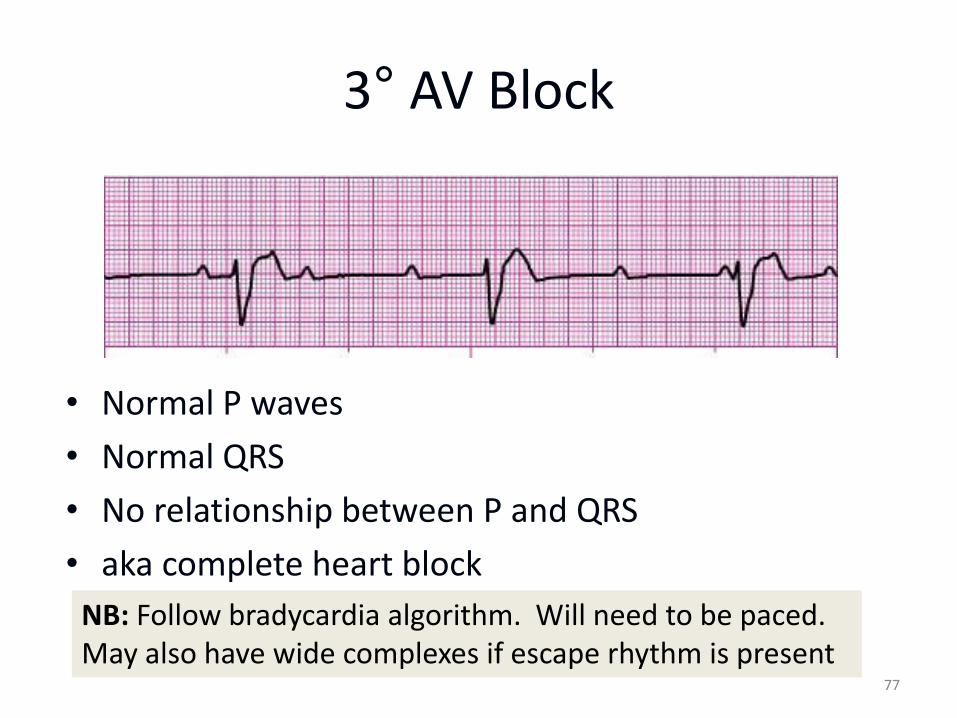
3° AV Block
• Normal P waves
• Normal QRS
• No relationship between P and QRS
• aka complete heart block
77
NB: Follow bradycardia algorithm. Will need to be paced. May also have wide complexes if escape rhythm is present
Know When To Stop
• With return of spontaneous circulation
• No ROSC during or after 20 minutes of resuscitative efforts
– Possible exceptions include near-drowning, severe hypothermia, known reversible cause, some overdoses
• DNR orders presented
• Obvious signs of irreversible death
78
N.B. For out-of-hospital providers also include transfer of care, danger to providers, etc
Take Home Points
• Assess and manage at every step before moving on to the next step
• Rapid defibrillation is the ONLY effective treatment for VF/VT
• Search for and treat the cause
• Treat the patient not the monitor
• Reassess frequently
• Minimize interruptions to chest compressions
79
80
End of ACLS CE Part I THANK YOU FOR YOUR ATTENTION
To follow: Part II ACLS in Acute Coronary Syndromes / Cardiac Arrest •Importance of CPR / BLS in most current (2010) AHA ACLS •Relationship of the chain of survival to successful resuscitation of the cardiac arrest patient •Discuss the interventions required to ensure good outcomes with Return of Spontaneous Circulation (ROSC) Part III •Defibrillation and ACLS Drug Therapy
Reference resources and further study: ACLS Study Guide - ECG STRIP INTERPRETATION.pdf ACLS Rhythms for the ACLS Algorithms.pdf http://acls-algorithms.com/ Website, including Megacode simulator