acl rehab - nj orthopedic surgeons: princeton, … · acl rehab objectives - determine the...
TRANSCRIPT

ACL REHAB
Jessica Spivey, MPT,CKTP
UOA
DISCLOSURE
I have no relevant financial or nonfinancial relationship(s) within the topics described, reviewed, evaluated or compared in this presentation.
www.UOANJ.com

ACL Rehab
OBJECTIVES
- Determine the significance of prehabiliation
- Identify benchmarks in a postoperative ACL protocol
- Determine phase appropriate goals during ACLR rehabilitation program
- Identify proper Progression Criteria for activity advancement
- Identify factors limiting neuromuscular control after ACL injury
www.UOANJ.com

QUESTIONS ???
1. Do patients have better results if they participate in formal therapy prior to ACLR?
2. Is it acceptable to progress a patient based on protocol timelines ?
3. Does a patient need to achieve all the goals of the preceding phase prior to being progressed to the next phase during ACLR rehab?
4. What is best approach to regaining quadriceps strength after ACLR?
www.UOANJ.com

PREHAB
Prehabilitation has been defined as “the process of enhancing functional capacity of the individual to enable them to withstand the stressor of inactivity.”(1)
www.UOANJ.com

PREHAB
• Preoperative quadriceps strength :predictor of the functional outcome knee joint after ACLR (7)
• Loss of 50% of quadriceps strength in the first 14 weeks after ACL injury of ACLR
• Biomechanical changes: decreased extensor torque at knee, increased extensor torque at hip(3,4,5,6)
• Good preoperative strength (>90% ) results in higher postoperative strength at 1,3 months when compared to poor quad strength(<75%) group (2)
www.UOANJ.com

PREHAB
• Strength Training • A pre-rehabilitation strategy of progressive muscle
strengthening prior to ACLR: – Improved knee function – Improved quadriceps peak torque at 30 degrees of flexion – Improved total work (8)
• 4-6 pre-rehabilitation program followed by a 4 month minimum program after ACLR : – Improvement in the shuttle run, side step and carioca – Minimal deficit between injured and uninjured leg at 6
months post-op.(9)
www.UOANJ.com
Prehab
• Proprioception and NM training • ACL rupture: impaired proprioception increase latency of hamstring contraction
– ongoing instability in the ACL deficient knee – predisposing to DJD
• Preoperative management of proprioception leads to significantly better outcomes than those undergoing the traditional exercise regime (11)
• Prehab focus: – somatosensory input from the weight distribution of the foot – afferent information coming from the lower extremity to enhance joint proprioception and muscle response
• Perturbation training program versus strength training(3-4 wks.) – Poor dynamic knee stability prior to initiation – perturbation group had better symmetrical quadriceps strength (97% of the injured leg) and gait (13) – Improve NM feedback, decrease antagonistic muscle activity
• The perturbation technique yields a 92% success rate compared to the standard group that had a 50% success rate( no episodes of “giving way”) at 6 months post-op. (12)
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals
QUESTIONS??
Is it acceptable to progress patients based on protocol timelines ?
Does a patient need to achieve all the goals of the preceding phase prior to advancing to the next
during ACLR rehab?
www.UOANJ.com
ACL REHAB PROTOCOL /Physical Therapy Goals
• Pre-op goals – minimal pain, swelling and inflammatory response – full ROM and NM control
• Crutch training and independence in postsurgical exercises
• Understanding the rehab program and process : – increases self efficacy during rehabilitation – stimulates early recovery of knee function – decreases expected postsurgical pain – creates realistic view about the rehabilitation process(14-
20)
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals
PHASE 1 (week 1) Most important goals:
– controlling pain, swelling and inflammation – recovery of ROM and NM control
• Aggressive control of pain, swelling and inflammation: – prevents quadriceps inhibition – maintains full extension – makes immediate weight bearing possible (14,18,20,21)
• Immediate recovery of passive and active ROM – reduces pain – stimulates the homeostasis of cartilage – prevents patellofemoral problems, alterations in gait pattern, quadriceps atrophy and arthrofibrosis.
• Multi-directional mobilizations of patella • Prevent patellar immobility (leading to decreased ROM and quadriceps inhibition) (22,23)
• Regaining muscle control without endangering the graft – isometric – closed chained (0-60 is safe range) – open chain ( 90-40 is safe range) without additional weight. ** Theses exercises should include muscle setting exercises, SLR, heel slides, mini squats (0-30 flexion)body weight shifting/acceptance(14-25)
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals PHASE 2 (week 2-9)
Goals
• Walk without crutches (day 4-10)
• Normalize gait – Walking on a treadmill week 3
– Jogging in a straight line week 8
• Full ROM (maintain full extension) – 120 degrees flexion from week 2
– Attain and maintain good patellar mobility
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals (Phase 2 Cont’d)
Interventions • Cryotherapy • Flexion can be increased gradually • Full extension and patellar mobility will be maintained. • Isotonic strength training ( in a safe range, CC 0-60,OC 90-40) aimed at endurance:
– increases quadriceps strength significantly – has no negative effect on anterior knee pain and knee laxity (25)
• Quadriceps strength and hamstring strength can be increased by isometric isotonic and isokinetic exercises without endangering the graft (25)
• Inadequate extension can be treated aggressively to prevent postsurgical complications like arthrofibrosis
• Phase appropriate exercises:
– walking on a treadmill, cycling on an ergometer and swimming from week 3, – stair stepping week4 – and jogging a straight line , outdoor cycling from week 8 (25)
• Neuromuscular training: – static stability – dynamic stability.
• vestibular and somatosensory system for balance, – increase surface instability /decrease visual input.
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals (Phase 2 Cont’d)
Special Considerations
• **In phase 2 the strength of the graft is not optimal(15,17,18,19,23)
• Predisposing factors for quadriceps weakness after 6 months – Quadriceps atrophy – Persistent quad lag with SLR – Incomplete extension – Gait impairments (26)
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals Phase 3 (Week 9-16)
Goals
• Decrease pain and swelling
• Obtain and maintain full ROM
• Increase Muscle Strength
• Regain Neuromuscular control
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals Phase 3 (Week 9-16)
Special Considerations • NM control
– functional dynamic balance training – plyometric exercises
• Increase knee stability with CC and OC exercises (14,16,18,20,24,25) – Tensile strength of the graft is rising
• Endurance training to resistance training – Determined by pain and swelling – CC ad OC exercises for the ideal bases for sport specific
function training in phase 4 ( 19-25)
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals Phase 3 (Week 9-16)
Special Considerations
• Functional movement patterns: – improve the interactions between stabilizing structures of the kinetic chain (27)
• Plyometric exercises:
– preparation for agility training (ph 4) – improve the concentric contraction power of the muscle(28) – allows for quicker changes in direction
• Stimulate coordination and control ( afferent and efferent information processing)
– variation in visible input – surface stability, – speed of exercise performance – complexity of the test – resistance – single legged and two legged performance (25)
• Specific exercises for phase 3 should include normalization of running ( gradually increasing duration and
speed to decrease NM adaption and recovery time) from week 9 to progress to jogging outdoors week 13 ( 6,24,41)
www.UOANJ.com
ACL REHAB PROTOCOL /Physical Therapy Goals Phase 4 (Week 16-22)
GOALS
• Maximizing endurance of ACLR leg
• Maximizing strength of the knee stabilizers
• Optimize NM control
• Regaining agility
www.UOANJ.com

ACL REHAB PROTOCOL /Physical Therapy Goals Phase 4 (Week 16-22)
Intervention • Plyometric exercises
– Optimizing NM control
• Sports specific agility training
– with variations in running, turning , and cutting maneuvers,
– acceleration and decelerations,
**Improves arthrokinetic reflexes so that new trauma during competition can be prevented (21,27,29)
www.UOANJ.com
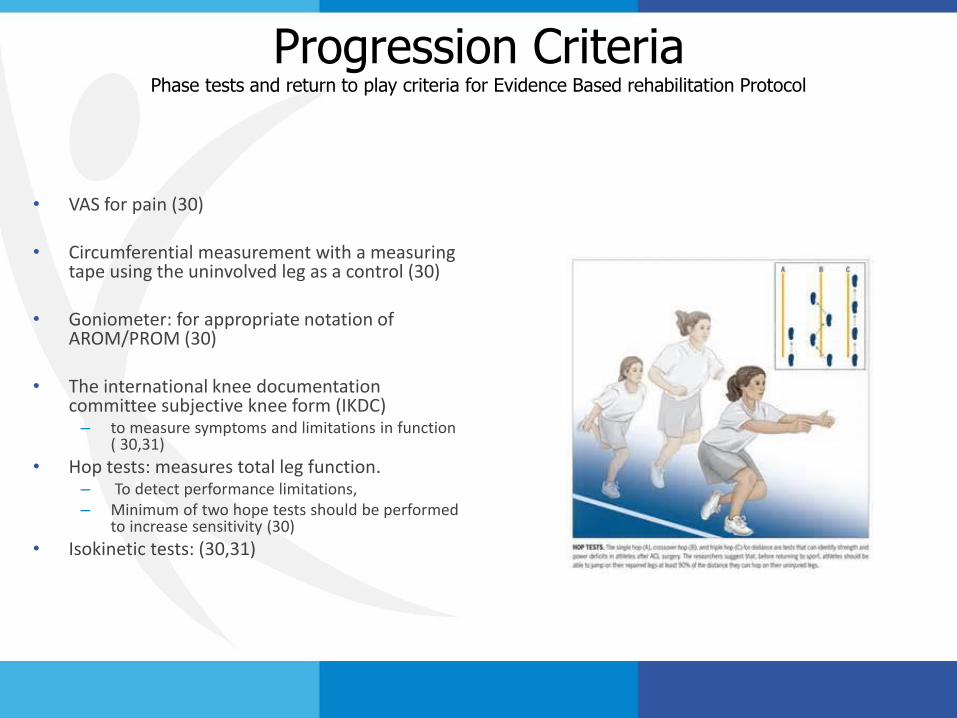
Progression Criteria Phase tests and return to play criteria for Evidence Based rehabilitation Protocol
• VAS for pain (30) • Circumferential measurement with a measuring
tape using the uninvolved leg as a control (30) • Goniometer: for appropriate notation of
AROM/PROM (30) • The international knee documentation
committee subjective knee form (IKDC) – to measure symptoms and limitations in function
( 30,31)
• Hop tests: measures total leg function. – To detect performance limitations, – Minimum of two hope tests should be performed
to increase sensitivity (30)
• Isokinetic tests: (30,31)

Progression Criteria Phase tests and return to play criteria for Evidence Based rehabilitation Protocol
Rehab Goals: (phase appropriate) - Subjective, objective, and as per physician protocol timeline Return to sports: -full ROM - hop tests - hamstring/quadriceps strength are 85% compared to the contralateral side - difference in HS/quad strength ratio is less than 15% compared to the contralateral side -patient tolerates sports specific activities ( no increase in pain or swelling) (6,11,24,41,44,51)
www.UOANJ.com

Special Considerations
Quadriceps strength
– Open Kinetic Chain versus Closed Kinetic Chain
– NMES versus Isotonic
• Eccentric, concentric
www.UOANJ.com
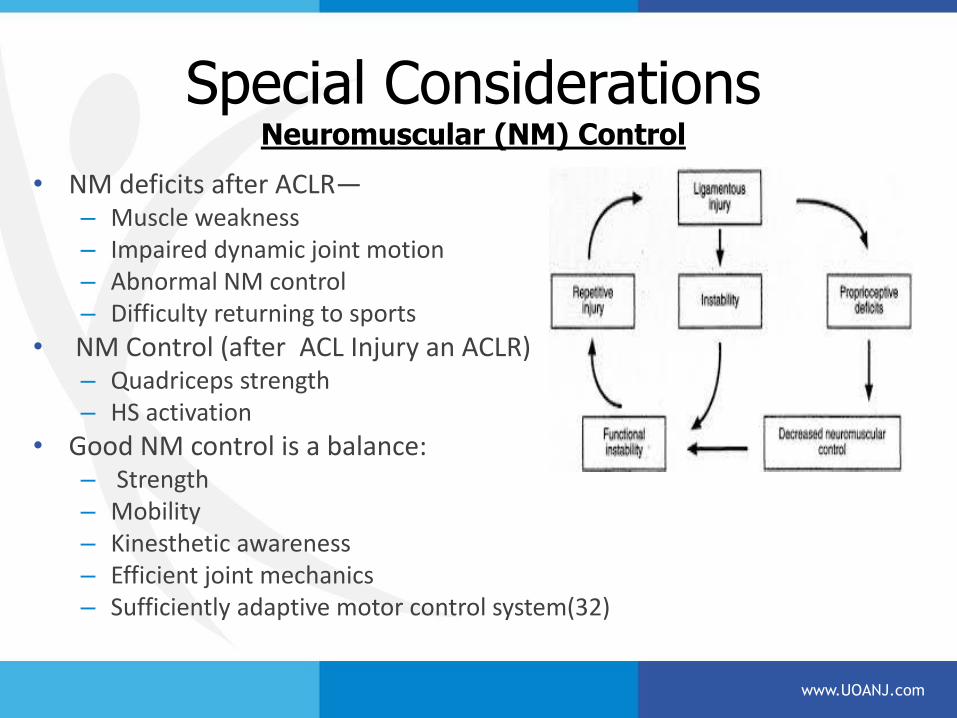
Special Considerations Neuromuscular (NM) Control
• NM deficits after ACLR— – Muscle weakness – Impaired dynamic joint motion – Abnormal NM control – Difficulty returning to sports
• NM Control (after ACL Injury an ACLR) – Quadriceps strength – HS activation
• Good NM control is a balance: – Strength – Mobility – Kinesthetic awareness – Efficient joint mechanics – Sufficiently adaptive motor control system(32)
www.UOANJ.com

SUMMARY
• Based on the literature :
- Prehab is important and effective in addressing possible post-op challenges.
- Proper progression should be based upon subjective information, objective information and protocol timelines.
- Evidence based criteria for advancement should be utilized to maximize results .
- Recruitment of quadriceps should be focused on endurance and transition to power.
- Strength training should progress to include NM control and timing.
www.UOANJ.com

REFERENCES
1.M.M Ditmyer, R.Topp, and Pifer, “Prehabilitation in preparation for orthopedic surgery,” Orthopedic Nursing, vol.21,no.5,pp43-52,2002.
2. I.Eitzen,I.Holm,and M.A.Risberg, “Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction,”British Journal of Sports Medicine vol.43no.5,pp.371-376,2009.
3. T. P. Andriacchi and D. Birac, “Functional testing in the anterior cruciate ligament-deficient knee,” Clinical Orthopaedics and Related Research, no. 288, pp. 40–47, 1993.
4. M. Berchuck, T. P. Andriacchi, B. R. Bach, and B. Reider, “Gait adaptations by patients who have a deficient anterior cruciate ligament,” Journal of Bone and Joint Surgery—Series A, vol. 72, no. 6, pp. 871–877, 1990.
5. P. Devita, P. B. Hunter, and W. A. Skelly, “Effects of a functional knee brace on the biomechanics of running,” Medicine and Science in Sports and Exercise, vol. 24, no. 7, pp. 797–806, 1992.
6. J. M. Timoney, W. S. Inman, P. M. Quesada et al., “Return of normal gait patterns after anterior cruciate ligament reconstruction,” The American Journal of Sports Medicine, vol. 21, no. 6, pp. 887–889, 1993.
7. I. Eitzen, I. Holm, and M. A. Risberg, “Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction,” British Journal of Sports Medicine, vol. 43, no. 5, pp. 371–376, 2009.
8. I. Eitzen, H. Moksnes, L. Snyder-Mackler, and M. A. Risberg, “A progressive 5-week exercise therapy program leads to significant improvement in knee function early after anterior cruciate ligament injury,” Journal of Orthopaedic and Sports Physical Therapy, vol. 40, no. 11, pp. 705–721, 2010.
9. S. L. Keays, J. Bullock-Saxton, and A. C. Keays, “Strength and function before and after anterior cruciate ligament reconstruction,” Clinical Orthopaedics and Related Research, no. 373, pp. 174–183, 2000.
10. R. L. Barrack, H. B. Skinner, and S. L. Buckley, “Proprioception in the anterior cruciate deficient knee,” The American Journal of Sports Medicine, vol. 17, no. 1, pp. 1–6, 1989.

REFERENCES 11. D. J. Beard, C. A. F. Dodd, H. R. Trindle, and A. H. R. W. Simpson, “Proprioception enhancement for anterior cruciate ligament deficiency. A prospective randomised trial of two physiotherapy regimes,” Journal of Bone and Joint Surgery— Series B, vol. 76, no. 4, pp. 654–659, 1994.
12. G. K. Fitzgerald, M. J. Axe, and L. Snyder-Mackler, “Proposed practice guidelines for nonoperative anterior cruciate ligament rehabilitation of physically active individuals,” Journal of Orthopaedic and Sports Physical Therapy, vol. 30, no. 4, pp. 194–203, 2000.
13. E. Hartigan, M. J. Axe, and L. Snyder-Mackler, “Perturbation training prior to ACL reconstruction improves gait asymmetries in non-copers,” Journal of Orthopaedic Research, vol. 27, no. 6, pp. 724–729, 2009.
14. Allum R (2003) Aspects of current management, complications of arthroscopic reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 85-B:12–16
15. 3. Beynnon B, Johnson R, Abate J, Fleming B, Nichols C (2005) Treatment of anterior cruciate ligament injuries, Part I. Am J Sports Med 33:1579–1602
16. 8. DeHaven K, Cosgarea A, Sebastianelli W (2003) Arthrofibrosis of the knee following ligament surgery. Instr Course Lect 52:369–381
17. Mc Carty L, Bach B (2005) Rehabilitation after patellar tendon autograft anterior cruciate ligament reconstruction. Tech Orthop 20:439–451
18. Shelbourne K, Patel D (1999) Treatment of limited motion after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthosc 7:85–92
19. Wilk K, Reinold M, Hooks T (2003) Recent advances in the rehabilitation of isolated and combined anterior cruciate ligament injuries. Orthop Clin North Am 34:107–137
20. Maddison R, Prapavessis H, Clatworthy M (2006) Modelling and rehabilitation following anterior cruciate ligament reconstruction. Ann Behav Med 31:89–98
21. Cascio B, Culp L, Cosgarea A (2004) Return to play after anterior cruciate ligament reconstruction. Clin Sports Med 23:395–408
22. Gale T, Richmond J (2006) Bone patellar tendon bone anterior cruciate ligament reconstruction. Tech Knee Surg 5:72–79
23. Potter N (2006) Complications and treatment during rehabilitation after anterior cruciate ligament reconstruction. Oper Tech Sports Med 14:50–58

REFERENCES
24. Risberg M, Lewek M, Snyder-Mackler L (2004) A systematic review of evidence for anterior cruciate ligament rehabilitation, how much and what type. Phys Ther Sport 5:125–145
25.Shaarani S.R., Moyna N ,Moran R, O’Byrne J.M(2012) Prehabilitation:The Void in Managemet of Anterior Cruciate Ligament Injuries-A Clinical Review.ISRN Rehabilitation 2012:2-6
26. Potter N (2006) Complications and treatment during rehabilitation after anterior cruciate ligament reconstruction. Oper Tech Sports Med 14:50–58
27. . Wilk K, Reinold M, Hooks T (2003) Recent advances in the rehabilitation of isolated and combined anterior cruciate ligament injuries. Orthop Clin North Am 34:107–137 52. Wu G, Ng G, Mak A (2001) Effects of knee bracing on the sensorimotor function of subjects with anterior cruciate ligament reconstruction. Am J Sports Med 29:641–645 1144 Knee Surg Sports Traumatol Arthros
28. . Risberg M, Mork M, Jenssen H, Holm I (2001) Design and implementation of a neuromuscular training program following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 31:620–631
29. Rebel M (2000) Koordinatives training nach VKB-operationen. Sportverletz Sportschaden 14:12–19
30. Shaw T, Chipchase L, Williams M (2004) A users guide to outcome measurement following reconstruction. Phys Ther Sport 5:57–67
31.Keating J, Matyas T (1996) The influence of subject and test design on dynamometric measurements of extremity muscles. Phys Ther 76:866–889
32.Di Stasi S, Meyer G, Hewett T (2013) Neuromuscular Training to Target Deficits Associated With Second Anterior Cruciate Ligament Injury. . J Orthop Sports Phys Ther 43:776-851
www.UOANJ.com