acid - base physiology definitions acid - can donate a hydrogen ion base – can accept a hydrogen...
TRANSCRIPT

ACID - BASE PHYSIOLOGYACID - BASE PHYSIOLOGYDEFINITIONSDEFINITIONS
• ACID - can donate a hydrogen ion• BASE – can accept a hydrogen ion• STRONG ACID – completely or almost completely
dissociates into a hydrogen ion and its conjugate base in aqueous solution
• WEAK ACID – only slightly dissociated in aqueous solution
• Strong acids usually have weak conjugate bases; weak acids usually have strong conjugate bases
• BUFFER – mixture of substances in aqueous solution. Usually a weak acid and its conjugate base, that can resist changes in hydrogen ion concentration when strong acids or bases are added.
• ACID - can donate a hydrogen ion• BASE – can accept a hydrogen ion• STRONG ACID – completely or almost completely
dissociates into a hydrogen ion and its conjugate base in aqueous solution
• WEAK ACID – only slightly dissociated in aqueous solution
• Strong acids usually have weak conjugate bases; weak acids usually have strong conjugate bases
• BUFFER – mixture of substances in aqueous solution. Usually a weak acid and its conjugate base, that can resist changes in hydrogen ion concentration when strong acids or bases are added.
ACID - BASE PHYSIOLOGYACID - BASE PHYSIOLOGYDEFINITIONSDEFINITIONS
pH - negative log of hydrogen ion concentrationpH - negative log of hydrogen ion concentrationpH - negative log of hydrogen ion concentrationpH - negative log of hydrogen ion concentration
ACIDOSIS - pH < 7.35ACIDOSIS - pH < 7.35
ALKALOSIS - pH > 7.45ALKALOSIS - pH > 7.45
ACIDOSIS - pH < 7.35ACIDOSIS - pH < 7.35
ALKALOSIS - pH > 7.45ALKALOSIS - pH > 7.45



• ISOHYDRIC PRINCIPLE – All buffer pairs in a homogeneous solution are in equilibrium with the same hydrogen ion concentration
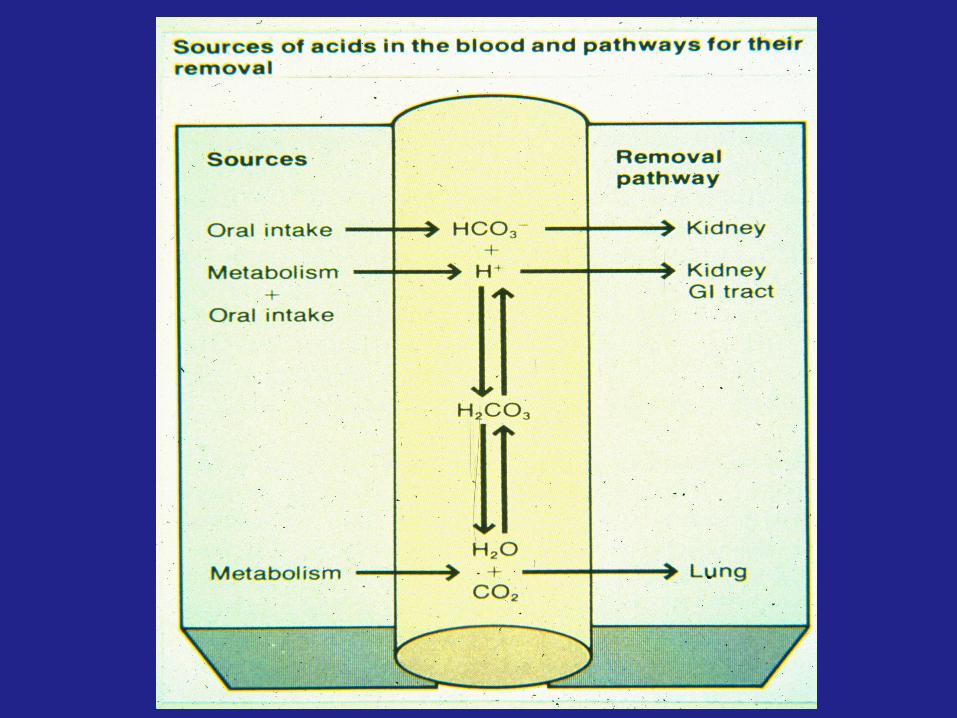
• BICARBONATE• PHOSPHATE• BLOOD PROTEINS – especially hemoglobin• INTERSTITIAL FLUID – mainly bicarbonate, some
phosphate• BONES – mainly phosphate in hydroxyapatite• INTRACELLULAR BUFFERS – intracellular proteins and
organic phosphates
• ISOHYDRIC PRINCIPLE – All buffer pairs in a homogeneous solution are in equilibrium with the same hydrogen ion concentration
• BICARBONATE• PHOSPHATE• BLOOD PROTEINS – especially hemoglobin• INTERSTITIAL FLUID – mainly bicarbonate, some
phosphate• BONES – mainly phosphate in hydroxyapatite• INTRACELLULAR BUFFERS – intracellular proteins and
organic phosphates
ACID - BASE PHYSIOLOGYACID - BASE PHYSIOLOGYBUFFERS OF THE BODYBUFFERS OF THE BODY
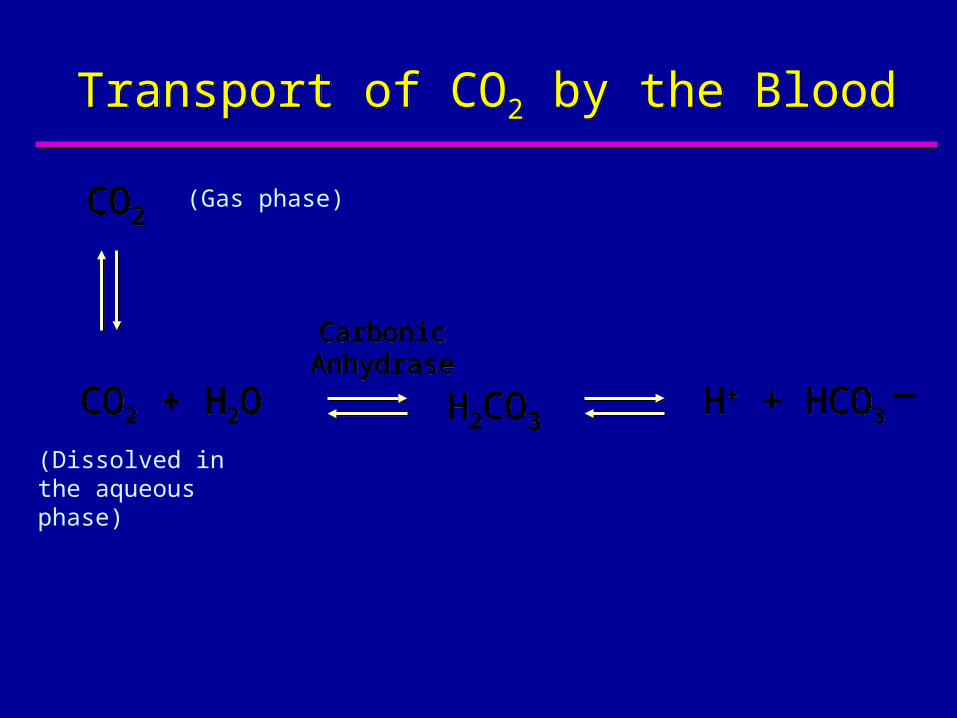
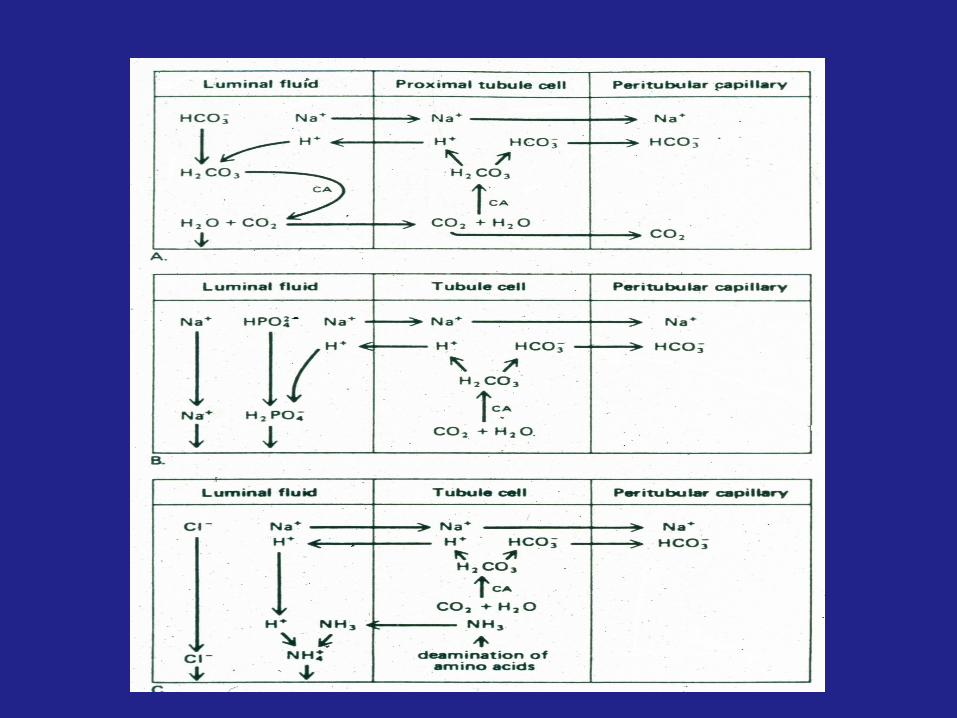
CO2 + H2OCO2 + H2O H2CO3H2CO3H+ + HCO3H+ + HCO3
CarbonicAnhydraseCarbonic
Anhydrase _
Transport of CO2 by the BloodTransport of CO2 by the Blood
CO2CO2(Gas phase)
(Dissolved in the aqueous phase)

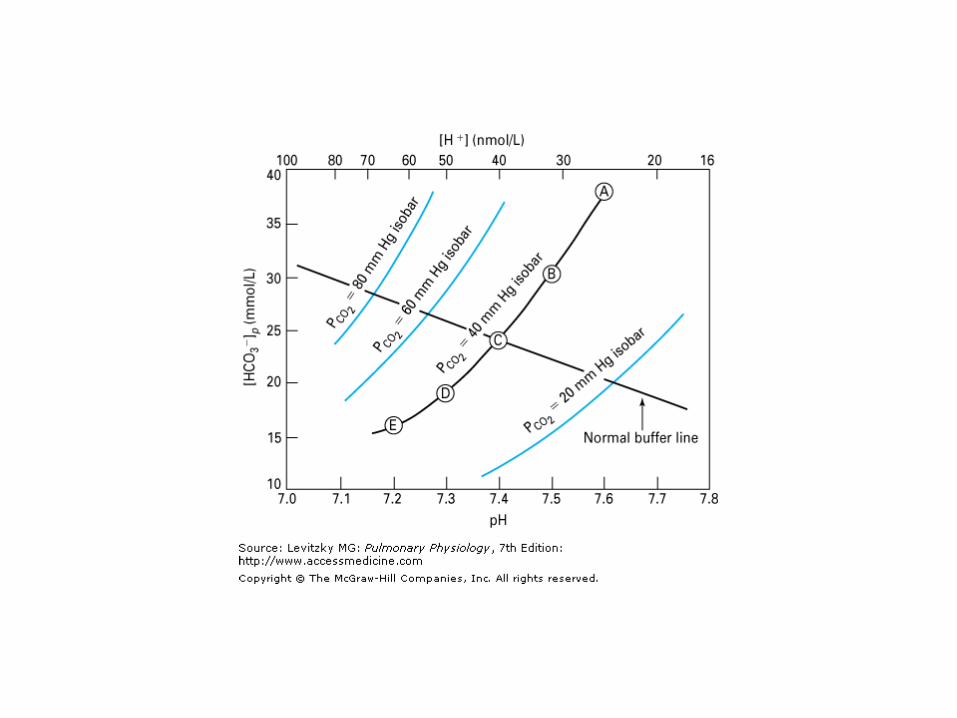
Taking Logarithms
Since pH is negative logarithm

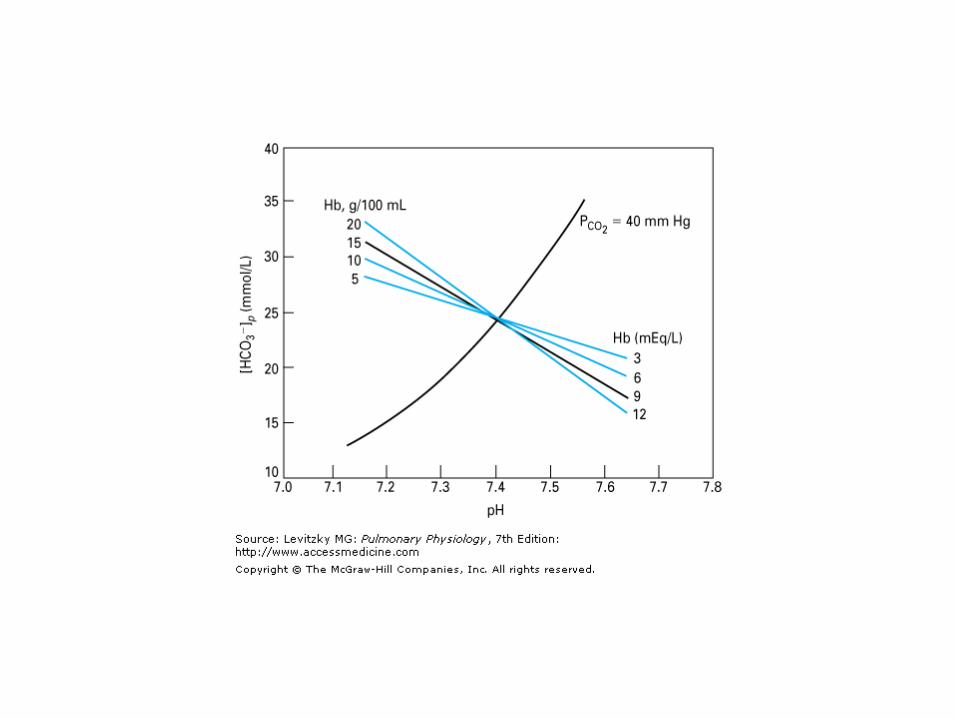
Henderson – Hasselbalch Equation
pH = pK´ + log [HCO-
3] p
0.03 x Pco2

[HC
O3
- ]p
, m
mol/ lit
er
[HC
O3
- ]p
, m
mol/ lit
er
15
20
25
30
35
40
pHpH7.0 7.1 7.2 7.3 7.4 7.5 7.6 7.7 7.8
HCO3-
Pco2
HCO3-
Pco2
Respiratory acidosis
DD
AA
GG
EE
FF
CC
II
HH
BB
Uncompensated respiratory acidosis
Uncompensated respiratory acidosis
Metabolic alkalosis and respiratory acidosis
Metabolic alkalosis and respiratory acidosis
Compensated
Common Causes of Respiratory AcidosisCommon Causes of Respiratory Acidosis Depression of Respiratory Control Centers
Anesthetics Sedatives Opiates Brain injury or disease Severe hypercapnia, hypoxia
Neuromuscular disorders Spinal cord injury Phrenic nerve injury Poliomyelitis Botulism, tetanus Myasthenia gravis Administration of curare-like drugs Diseases affecting the respiratory muscles
Pulmonary diseases Acute asthma Pulmonary vascular disease
Depression of Respiratory Control Centers Anesthetics Sedatives Opiates Brain injury or disease Severe hypercapnia, hypoxia
Neuromuscular disorders Spinal cord injury Phrenic nerve injury Poliomyelitis Botulism, tetanus Myasthenia gravis Administration of curare-like drugs Diseases affecting the respiratory muscles
Pulmonary diseases Acute asthma Pulmonary vascular disease

Common Causes of Respiratory AcidosisCommon Causes of Respiratory Acidosis
Chest wall restriction Kyphoscoliosis Extreme obesity
Lung restriction Pulmonary fibrosis Sarcoidosis Pneumothorax
Pulmonary parenchymal diseases Pneumonia Pulmonary edema
Airway obstruction Chronic obstructive pulmonary
disease Upper airway obstruction
Chest wall restriction Kyphoscoliosis Extreme obesity
Lung restriction Pulmonary fibrosis Sarcoidosis Pneumothorax
Pulmonary parenchymal diseases Pneumonia Pulmonary edema
Airway obstruction Chronic obstructive pulmonary
disease Upper airway obstruction

[HC
O3
- ]p
, m
mol/ lit
er
[HC
O3
- ]p
, m
mol/ lit
er
15
20
25
30
35
40
pHpH7.0 7.1 7.2 7.3 7.4 7.5 7.6 7.7 7.8
HCO3-
Pco2
HCO3-
Pco2
Respiratory alkalosis
DD
AA
GG
EE
FF
CC
II
HH
BB
Uncompensated respiratory alkalosis
Uncompensated respiratory alkalosis
Metabolic acidosis and respiratory alkalosisMetabolic acidosis and respiratory alkalosis
Compensated

Common Causes of Respiratory AlkalosisCommon Causes of Respiratory Alkalosis Central Nervous System
Anxiety Hyperventilation Inflammation (encephalitis, meningitis) Cerebrovascular disease Tumors
Drugs or hormones Salicylates Progesterone
Pulmonary diseases Acute asthma Pulmonary vascular disease (pulmonary
embolism)
Central Nervous System Anxiety Hyperventilation Inflammation (encephalitis, meningitis) Cerebrovascular disease Tumors
Drugs or hormones Salicylates Progesterone
Pulmonary diseases Acute asthma Pulmonary vascular disease (pulmonary
embolism)
Common Causes of Respiratory AlkalosisCommon Causes of Respiratory Alkalosis
Bacteremias, fever Overventilation with mechanical
ventilators Hypoxia,high altitude
Bacteremias, fever Overventilation with mechanical
ventilators Hypoxia,high altitude

[HC
O3
- ]p
, m
mol/ lit
er
[HC
O3
- ]p
, m
mol/ lit
er
15
20
25
30
35
40
pHpH7.0 7.1 7.2 7.3 7.4 7.5 7.6 7.7 7.8
DD
AA
GG
EE
FF
CC
BB
HCO3-
Pco2
HCO3-
Pco2
Metabolic acidosis
II
HH
Metabolic acidosisMetabolic acidosis
Metabolic acidosis and respiratory alkalosisMetabolic acidosis and respiratory alkalosis
Uncompensatedmetabolic acidosisUncompensatedmetabolic acidosis
Compensated

Common Causes of Metabolic AcidosisCommon Causes of Metabolic Acidosis
Ingested drugs or toxic substances Methanol Alcohol Salicylates Ammonium Chloride Ethylene glycol
Loss of bicarbonate ions Diarrhea Pancreatic Fistulas Renal dysfunction
Inability to excrete hydrogen ions Renal dysfunction
Ingested drugs or toxic substances Methanol Alcohol Salicylates Ammonium Chloride Ethylene glycol
Loss of bicarbonate ions Diarrhea Pancreatic Fistulas Renal dysfunction
Inability to excrete hydrogen ions Renal dysfunction
Common Causes of Metabolic AcidosisCommon Causes of Metabolic Acidosis
Lactic acidosis Hypoxemia Anemia, carbon monoxide Shock (hypovolemic,cardiogenic,
septic, etc.) Severe exercise Acute respiratory distress syndrome
(ARDS) Ketoacidosis
Diabetes mellitus Alcoholism Starvation
Lactic acidosis Hypoxemia Anemia, carbon monoxide Shock (hypovolemic,cardiogenic,
septic, etc.) Severe exercise Acute respiratory distress syndrome
(ARDS) Ketoacidosis
Diabetes mellitus Alcoholism Starvation
[HC
O3
- ]p
, m
mol/ lit
er
[HC
O3
- ]p
, m
mol/ lit
er
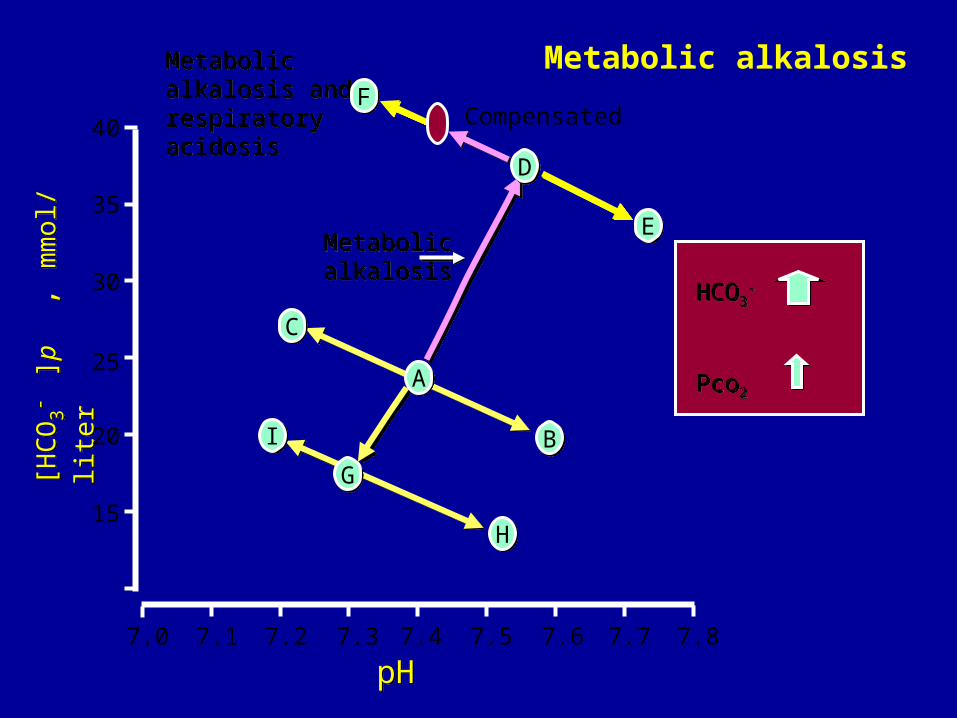
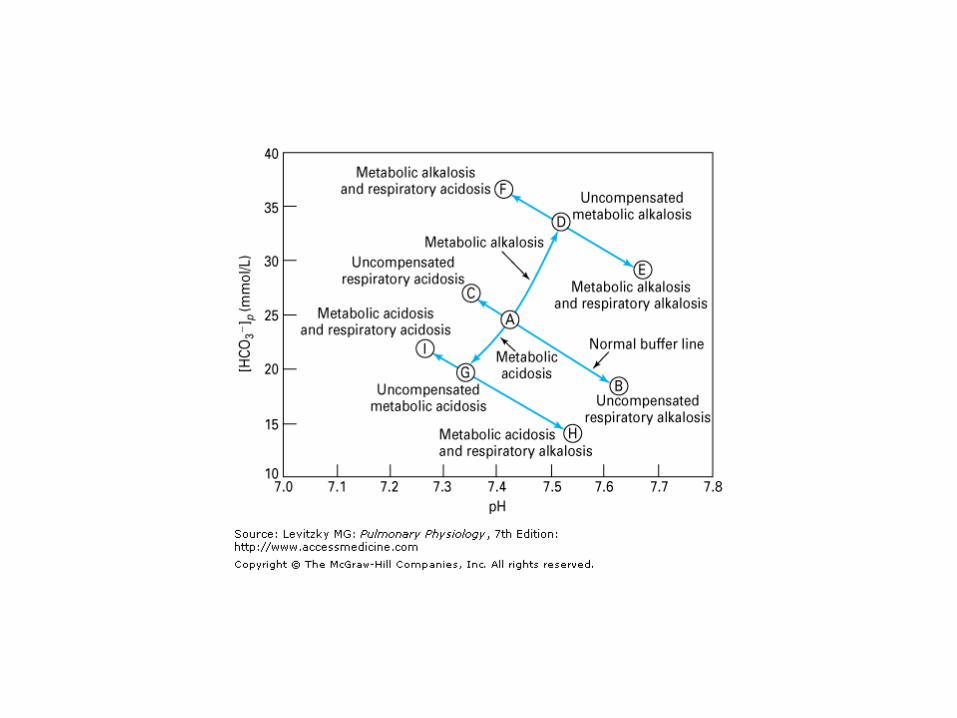
Metabolic alkalosis and respiratory acidosis
Metabolic alkalosis and respiratory acidosis
15
20
25
30
35
40
pHpH
Metabolic alkalosisMetabolic alkalosis
7.0 7.1 7.2 7.3 7.4 7.5 7.6 7.7 7.8
DD
AA
GG
EE
FF
CC
II
HH
BB
HCO3-
Pco2
HCO3-
Pco2
Metabolic alkalosis
Compensated
Common Causes of Metabolic AlkalosisCommon Causes of Metabolic Alkalosis
Loss of hydrogen ions Vomiting Gastric fistulas Diuretic therapy Treatment with or overproduction of
mineralocorticoids Ingestion or administration of excess
bicarbonate Intravenous bicarbonate Ingestion of bicarbonate or other bases
(e.g. antacids)
Loss of hydrogen ions Vomiting Gastric fistulas Diuretic therapy Treatment with or overproduction of
mineralocorticoids Ingestion or administration of excess
bicarbonate Intravenous bicarbonate Ingestion of bicarbonate or other bases
(e.g. antacids)

ACID - BASE PHYSIOLOGYACID - BASE PHYSIOLOGYDEFINITIONSDEFINITIONS
BASE EXCESS OR DEFICIT = mEq of acid or base needed to titrate 1 liter of blood to a pH of 7.4 at 37ºC if the Pco2 were 40 torr
BASE EXCESS OR DEFICIT = mEq of acid or base needed to titrate 1 liter of blood to a pH of 7.4 at 37ºC if the Pco2 were 40 torr
ANION GAP = [Na+] - ([Cl-] + [HCO3-])
Normally 12 ± 4 mEq / L
ANION GAP = [Na+] - ([Cl-] + [HCO3-])
Normally 12 ± 4 mEq / L
If the anion gap is greater than 16 mEq / L :Lactic acidosis, ketoacidosis or organic
anionsRenal retention of sulfate, phosphate, or
urateDecreased [K+], [Ca++], and/ or [Mg++]
If the anion gap is greater than 16 mEq / L :Lactic acidosis, ketoacidosis or organic
anionsRenal retention of sulfate, phosphate, or
urateDecreased [K+], [Ca++], and/ or [Mg++]

Acid- Base DisturbancesAcid- Base Disturbances
Uncompensated respiratory acidosisUncompensated respiratory acidosis
Uncompensated respiratory alkalosisUncompensated respiratory alkalosis
Uncompensated metabolic acidosisUncompensated metabolic acidosis
Uncompensated metabolic alkalosisUncompensated metabolic alkalosis
Partially compensated respiratory acidosisPartially compensated respiratory acidosis
Partially compensated respiratory alkalosisPartially compensated respiratory alkalosis
Partially compensated metabolic acidosisPartially compensated metabolic acidosis
Partially compensated metabolic alkalosisPartially compensated metabolic alkalosis
Respiratory and metabolic acidosisRespiratory and metabolic acidosis
Respiratory and metabolic alkalosis Respiratory and metabolic alkalosis
pHpH Pco2Pco2 HCO3HCO3
__

A Classification of the Causes of HypoxiaA Classification of the Causes of HypoxiaIncreased
FIo2
helpful?Classification PAo2
Pao2 Cao2 Cvo2Pvo2
Hypoxic hypoxia
Low alveolar Po2
Diffusion impairment
Right to left shunts
V/Q mismatch
Anemic hypoxia
CO poisoning
Hypoperfusion hypoxia
Histotoxic hypoxia
Low
Norm
Norm
Norm
Norm
Norm
Norm
Norm
Low
Low
Low
Low
Norm
Norm
Norm
Norm
Low
Low
Low
Low
Low
Low
Norm
Norm
Low
Low
Low
Low
Low
Low
Low
High
Low
Low
Low
Low
Low
Low
Low
High
Yes
Yes
No
Yes
No
Possibly
No
No