achalasia 05 2015 - home | gastroenterology und … · • degeneration of ganglion cells in the...
TRANSCRIPT

ACHALASIA 05 2015 ACG 2013

Titel der Präsentation / Name Referent/-in 2
Gastroenterologie
• 1674 Sir Thomas Willis, mechanical dilatation with
whalebone
• 1929 “does not relax” “Achalasia” Sir Arthur Hurst
• Primary motor disorder of the esophagus characterized by
insufficient (incomplete or absent) lower esophageal
sphincter relaxation and loss of esophageal peristalsis
Definition ?

Titel der Präsentation / Name Referent/-in 3
Gastroenterologie
Pathophysiology ?
Park und Vaezi, 2005
Titel der Präsentation / Name Referent/-in 4
Gastroenterologie
• Autoimmune, viral immune, or neurodegenerative etiology
• Degeneration of ganglion cells in the myenteric plexus of the esophageal body
and the LES by inflammatory process
• Loss of inhibitory neurotransmitters nitrous oxide and vasoactive intestinal
peptide and consequently imbalance between the excitatory and inhibitory
neurons
unopposed cholinergic activity
incomplete relaxation of the LES and aperistalsis due to loss of latency
gradient along the esophageal body
Pathophysiology

Titel der Präsentation / Name Referent/-in 5
Gastroenterologie

Titel der Präsentation / Name Referent/-in 6
Gastroenterologie

Titel der Präsentation / Name Referent/-in 7
Gastroenterologie
• Equally in men and women
• Incidence of 1 in 100,000 individuals annually
• Prevalence of 10 in 100,000
• Peak incidence occurs between 30 and 60 years of age
Vaezi et al, 1999
Francis DL et al, 2010
Epidemiology?

Titel der Präsentation / Name Referent/-in 8
Gastroenterologie
• Dysphagia to solids and liquids 90 %
• Regurgitation (of undigested food) 76–91 %
• Chest pain 25-64 %
• Weight loss 35-91 %
• Heart burn 18-52 %
• Aspiration 38 %
• Long vs short duration of symptoms
• “unresponsive to an adequate trial of proton pump inhibitor
(PPI) therapy”
–Compliance, Changing PPI, trial bid dosing
Symptoms/classic presentation?

Titel der Präsentation / Name Referent/-in 9
Gastroenterologie
Score?
Titel der Präsentation / Name Referent/-in 10
Gastroenterologie
• Pseudoachalasia from tumors (not only gastroscopy, also CT)
• Secondary achalasia
–Fundoplicatio, gastric banding
• Chagas disease (Trypanozoma cruzi)
• Esophagitis with or without stenosis/Schatzki
• Motility disorders (primary Achalasie, Jackhammer
esophagus, diffuse esophageal spasms)
• Neuromuscular diseases eg Apoplex (Oropharyngeal),
AML, Myasthenia gravis
• EOE
• Amyloidose, Kollagenosen, Sklerodermie
• ……
Differentialdiagnosis of Dysphagia

Titel der Präsentation / Name Referent/-in 11
Gastroenterologie
• Gastroscopy
• Contrast studies
• Manometry
Diagnosis

Titel der Präsentation / Name Referent/-in 12
Gastroenterologie
Gastroscopy

Titel der Präsentation / Name Referent/-in 13
Gastroenterologie
• Ruling out a mechanical obstruction or pseudoachalasia
• Bx EOE…
• Red flags:
–Short duration of symptoms, Age, Weight loss
• Strong resistance at the EGJ suspect of
pseudoachalasia further imaging (CT)
• EUS? Ziegler et al, 1990
Mittal et al, 2003
Gastroscopy

Titel der Präsentation / Name Referent/-in 14
Gastroenterologie
• Barium column height 1 and 5 min = “ timed barium
esophagram ” (TBE)
De Oliveira et al, 1997
• Nondiagnostic in up to one-third of patients, but no false
positive Ott et all, 1987
• TBS recommended in those with equivocal motility testing
• Objective assessment of esophageal emptying after
therapy!
Esophagogram/Contrast studies

Titel der Präsentation / Name Referent/-in 15
Gastroenterologie
• Dilation of the esophagus
• “ bird beak”
• Aperistalsis
• Poor emptying of barium
• Late- or end-stage achalasia
changes (tortuosity,
angulation, megaesophagus)
Esophagogramm/TBS

Titel der Präsentation / Name Referent/-in 16
Gastroenterologie
• Gold standard
• Normal findings in gastroscopy and esophagramm should
prompt manometry
Esophageal Manometry

Titel der Präsentation / Name Referent/-in 17
Gastroenterologie
Figure 1: Esophageal conventional manometry using 4-5 pressure sensors located in the lower
esophageal sphincter (LES) high pressure zone (HPZ) and esophageal body 5, 10, 15 and 20cm
above the LES.

Titel der Präsentation / Name Referent/-in 18
Gastroenterologie
Figure 2: Esophageal high-resolution manometry. Esophageal pressure data is collected from
sensors placed with 1-1.5cm from each other (a). In pressure topography the pharyngeal
contraction, upper esophageal sphincter relaxation (normal 300-500 msec), proximal esophageal
peristalsis, transition zone (TZ), distal esophageal peristalsis and lower esophageal sphincter
(LES) relaxation (normal 6-10 sec) can be quantified for each swallow (b).

Titel der Präsentation / Name Referent/-in 19
Gastroenterologie
Diagnostik

Titel der Präsentation / Name Referent/-in 20
Gastroenterologie
• HRM criteria:
– Impaired EGJ relaxation (Mean 4 s IRP >/= 10 mmHg over
test swallows)
–Aperistalsis
–Sensitivity of 98 % and a specificity of 96 % (Pandolfino et al)
• Increased basal LES pressure is not requiered
Katz et al, 1986
Esophageal Manometry
Titel der Präsentation / Name Referent/-in 21
Gastroenterologie
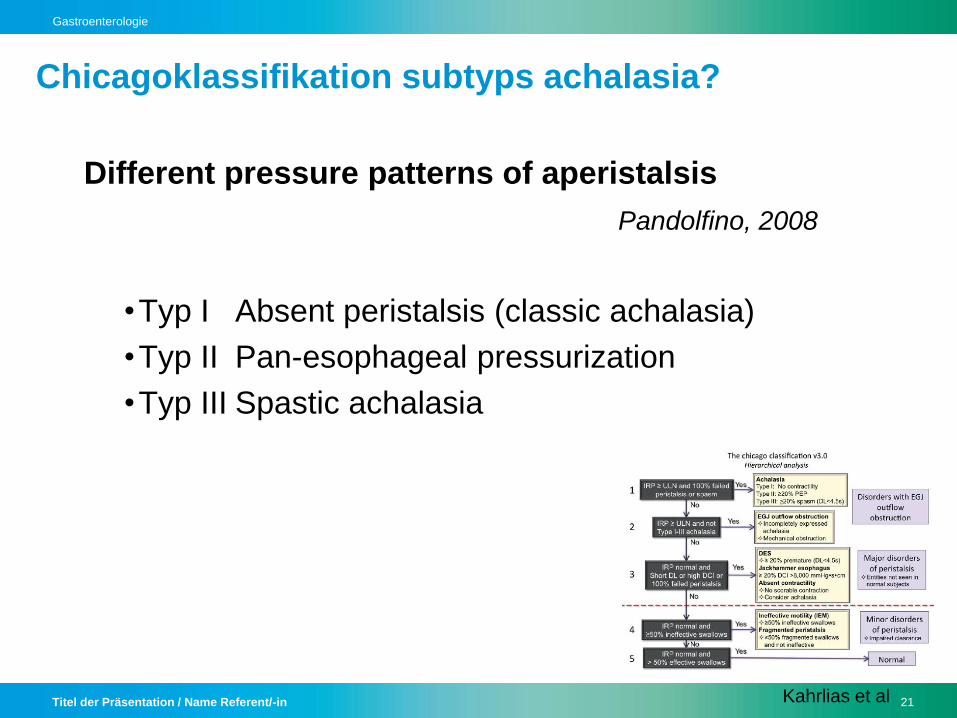
Different pressure patterns of aperistalsis
Pandolfino, 2008
•Typ I Absent peristalsis (classic achalasia)
•Typ II Pan-esophageal pressurization
•Typ III Spastic achalasia
Chicagoklassifikation subtyps achalasia?
Kahrlias et al

Titel der Präsentation / Name Referent/-in 22
Gastroenterologie
type I classic achalasia –
impaired EGJ relaxation and absent esophageal peristalsis

Titel der Präsentation / Name Referent/-in 23
Gastroenterologie
type II with pressurization -
impaired EGJ relaxation and
non-peristaltic pressure changes exceeding 30mmHg

Titel der Präsentation / Name Referent/-in 24
Gastroenterologie
type III with spasms –
more than 20% spastic contractions in the distal esophagus
with impaired EGJ relaxation

Titel der Präsentation / Name Referent/-in 25
Gastroenterologie
Clinically relevant!
•Typ I Absent peristalsis (classic achalasia)
•Typ II Pan-esophageal pressurization
best outcome (100 % by Heller myotomy and 91 %
with PD
•Typ III Spastic achalasia
poorest overall response (29 %)
Pandolfino JE, Kwiatek MA, Nealis TJ, Bulsiewicz W, Post J,
Kahrilas PJ.Achalasia: it’s not all one disease., Gastroenterology
2008; 135: 1526–33
Chicagoklassifikation subtyps achalasia -
Why?

Titel der Präsentation / Name Referent/-in 26
Gastroenterologie
• Pharmacologic therapy
–Nitrates, Ca-channel blockers
–BoTox
• Endoscopic treatment
–Pneumatic dilatation
–Temporary Stents
–POEM
• Surgical options
–Myotomie (open vs. laparoscopicaly) ± Fundoplicatio (Dor
vs. „floppy Nissen“)
–Esophagectomy
Treatment

Titel der Präsentation / Name Referent/-in 27
Gastroenterologie
Treatment •Chronic non curable disease, often recurrence
•The choice of initial therapy should be guided by patients age, gender,
preference, and local institutional expertise

Titel der Präsentation / Name Referent/-in 28
Gastroenterologie
• Least effective, noninvasive
• Side effects (headache, hypotension, pedal edema)
• Not complete relief of symptoms
–Phosphodiesterase-5-inhibitor, sildenafil also effective ia
Bartolotti et al, 2000
• Ca-Channel blockers
• Sublingual Isosorbide dinitrate
Pharmacologic therapy

Titel der Präsentation / Name Referent/-in 29
Gastroenterologie
Ca-channel blockers
• Decrease LES pressure by 13 – 49 %
• Improve symptoms by 0 – 75 %
–Nifedipine time to maximum effect after ingestion of 20 – 45
min, duration from 30 to 120 min
–10 – 30 mg sublingually 30– 45 min before meals
Pharmacologic therapy

Titel der Präsentation / Name Referent/-in 30
Gastroenterologie
Sublingual isosorbide dinitrate
• symptomatic improvement ranging from 53 to 87 %
–Time to maximum reduction in LES pressure (3 –27 min)
duration 30 – 90 min
–5 mg 10 – 15 min before meals
Indication only if Patient cannot or refuse to undergo more
definitive therapies (PD or surgical myotomy)
+
those who have failed botulinum toxin injections
Pharmacologic therapy
Titel der Präsentation / Name Referent/-in 31
Gastroenterologie
• 12 month success rate 35 -41 %, after 1 month > 75 %
• 50 % relaps in 6- 24 months Pasricha et al, 1995
Vaezi, 1999; Annese et al, 2000
• 100 units botox just above the squamocolumnar junction in
at least 4 quadrants (diluted in preservative-free saline and
injected in 0.5 – 1 ml aliquots)
• Complications:
–25% chest pain, rare mediastinitis, allergy to egg protein
• Repeated injections…eventually higher rate of surgical
complications in subsequent myotomy Smith , 2006
Pharmacologic therapy II:
BoTox

Titel der Präsentation / Name Referent/-in 32
Gastroenterologie
Endoscopic treatment Pneumatic dilatation
Treatment

Titel der Präsentation / Name Referent/-in 33
Gastroenterologie
PD
• Rigiflex (polyethylene ballons)
• Ballon 3–3.5-4 cm
• Pressure 5-10-20 PSI
• Distention time 6-15 sec–5 min
• Sessions 1 – 5
• Ballon distention more important
(no waist) than distention time
–8-15 psi, held 15-60 s

Titel der Präsentation / Name Referent/-in 34
Gastroenterologie
• Esophageal perforation overall median rate of 1.9 %
(range 0 – 16 % )
Campos, 2009; Eckardt, 1997
Must be candidates for surgical intervention
• GERD may occur after PD in 15 – 35 %
• Recurrence of dysphagia should exclude GERD-related
distal esophageal stricture as a potential contributing
complication PPI
PD Complications

Titel der Präsentation / Name Referent/-in 35
Gastroenterologie
• Success rate of
–Single PD ~ 62 % at 6 months and 28 % at 6 years
–Serial dilation ~ 90 % at 6 months and 44 % at 6 years
Vela, 2006
Graded dilatator approach...50-93 % response
– Initial dilation 3-cm balloon
–Followed by symptomatic and objective assessment in 4 – 6
weeks next size dilator
• After treatment a third relapses over 4 – 6 years follow-up
PD

Titel der Präsentation / Name Referent/-in 36
Gastroenterologie
Favorable clinical response to PD:
• Postdilation LES pressure < 10 mmHg
• Chicago classification (pattern of contraction)
–Best effect for all treatments in typ II
• Age > 40/45 years
• Female
• No dilatation
Boeckxstaens 2011, Pandolfino 2008
Farhoomand, 2004; Eckardt, 1992; Pratap, 2011
Predictors of outcome PD

Titel der Präsentation / Name Referent/-in 37
Gastroenterologie
POEM peroral esophageal myotomy
–Cut the muscle over a minimum length of 6 cm into the
esophagus and 2 cm below the squamocolumnar junction
onto the cardia
–Overall, the success rate in prospective cohorts > 90%
Inoue, 2010; von Renteln, 2012; Swanstrom, 2011
–Since no long term + comparison with standards only within
trials
Endoscopic perspectives
Inoue 2010
Titel der Präsentation / Name Referent/-in 38
Gastroenterologie
Endoscopic treatment
• Pneumatic dilatation
• PEG
• POEM
• Temporary Stents
–30 mm stents success rate of 83 % at 10 years
Li, 2010
Cai, 2013
Treatment

Titel der Präsentation / Name Referent/-in 39
Gastroenterologie
• Surgical options
–Myotomie (open vs. Laparoscopicaly, thoracoscopic) ±
Fundoplicatio (Dor vs. „floppy Nissen“, Toupet)
–Esophagectomy
Treatment

Titel der Präsentation / Name Referent/-in 40
Gastroenterologie
Modified Heller myotomy
• Myotomie extending at least 6 cm above
Gastroesophageal Junction and 1.5 cm
Over stomach + 180° Fundoplication
Of Dor
• Symptome improvement in
• 77-100 %, decreases with follow up
period Campos, 2009
• Complications?
–GERD!
Treatment

Titel der Präsentation / Name Referent/-in 41
Gastroenterologie
Modified Heller myotomy
• GERD but with antireflux procedure possible postoperative
dysphagia?
–GERD without fundoplicatio 29-31 %
–GERD with added fundoplicatio 9-14 %
Campos, 2009, Torquati , 2006
• Anterior Dor vs posterior Toupet vs floppy Nissen
Treatment

Titel der Präsentation / Name Referent/-in 42
Gastroenterologie
Endstage achalasia: megaesophagus, sigmoid esophagus
• PD less effective
• Two recent studies documented symptomatic improvement
after myotomy in 72 - 92 % Sweet, 2008; Mineo, 2004
• Unresponsive esophageal resection with gastric or
colonic interposition (greater morbidity/mortality (0-5.4 %)
good candidates for surgery) response in 80 %
• Dysphagia requiring dilation may occur in up to 50 % of
patients after esophagectomy
Duranceau, 2012
Options in endstage achalasia?

Titel der Präsentation / Name Referent/-in 43
Gastroenterologie
• PD vs Botox 70 vs 32 % after 12 months, no differences
after 1 months Vaezi, 1999; Leyden, 2006
• PD vs Heller
–Boeckxstaens only prospective randomized multicentre 3
series of 3 sets of dilatation! No significant differences: 92 vs
87 %
–Systematic review 2006 by Campos found after 12 months
and 36 months First PD vs Heller: 68 vs 89 % and 56 vs 89
%, not graded PD!
• PD more cost-effective
Comparative effectiveness

Titel der Präsentation / Name Referent/-in 44
Gastroenterologie
• After 5-7 years 1/3 needs retreatment after Heller and PD
• Those who failed with the first intervention have a worse
outcome
• Botox, PD, re-do myotomy, esophagectomy
Treatment in case of recurrence

Titel der Präsentation / Name Referent/-in 45
Gastroenterologie
• Assessment of symptoms and esophageal emptying by
barium esophagogram
Aim avoid developement of endstage achalasia
Short-term and lifelong follow-up (recurrence,
megaesophagus, carcinoma), 1-3 months
Postintervention LES pressure 10 mmHg higher remission,
but controversy… Eckardt, 1992
More aggressive follow-up in those with abnormal barium
height at 5 min TBS Vaezi, 1999
Early recurrence(no response) vs. Late recurrence (after
iniial response)
Follow-up I + II ?

Titel der Präsentation / Name Referent/-in 46
Gastroenterologie
Megaesophagus (Diameter > 6 cm)
• Sigmoidesophagus
• Of treatet patients 15 % develop megaesophagus
Of those 5 % need esophagektomy
No data for aggressive treatment, even with post treatment
LES > 10 mmHg, TBS height 5 min abnormal
Endstage disease

Titel der Präsentation / Name Referent/-in 47
Gastroenterologie
• Surveillance endoscopy is not recommended
• Risk of esophageal squamous cell carcinoma 10-50 times
increased in achalasia: incidence rate 1 cancer per 300
patient years (+ adenocarcinoma)
Leeuwenburgh, 2010; Dunaway, 2001
• Overall number of cancers remains low
• Many experts favor endoscopic surveillance after 10 - 15
years, interval of every 3 years Eckardt, 2010
Follow-up II

Titel der Präsentation / Name Referent/-in 48
Gastroenterologie