acceptability and uptake of an electronic decision making
TRANSCRIPT
Acceptability and uptake of an electronic decision making tool to support
implementation of IMCI in PHC facilities in KwaZulu-Natal, South Africa.
Jensen C, McKerrow N, Wills G
9th SA AIDS Conference
12 June 2019

Background
Still too many preventable child deaths in SA (1)
� U5MR
� 2009: 56/1000 births → 2015: 37-44/1000 births
� SDG target: <25/1000 live births by 2030
� Causes
� Major: neonatal (1/3), diarrhoea, pneumonia, HIV, congenital, non-natural
� Underlying: malnutrition, HIV
� Modifiable factors
� 50% die outside health facilities
� Clinic: inadequate assessments/ identification: HIV, malnutrition
� Home: delayed recognition of signs/ care-seeking
IMCI is the WHO strategy to reduce child mortality
Poor implementation well described globally and in SA (2,3)
1. Third Triennial Report of the Committee on Morbidity and Mortality in Children under 5 years (CoMMiC): 2015-2017. 2. Gera et al. IMCI strategy for children under five. Cochrane Database of Systematic Reviews 2016.3. Horwood et al. An Evaluation of the Quality of IMCI Assessments among IMCI Trained Health Workers in SA. (2009)
Source: Bamford, McKerrow et al. Child mortality in South Africa: Fewer deaths, but better data are needed. S Afr Med J 2018;108:S25-S32.
IMCI implementation
Bottlenecks in South Africa (4)
� Suboptimal staff deployment after training
� Lack of functioning supervision systems
� Lack of user-friendly implementation tools
KwaZulu-Natal DoH responses
� Reduce staff rotation
� Strengthen supervision systems
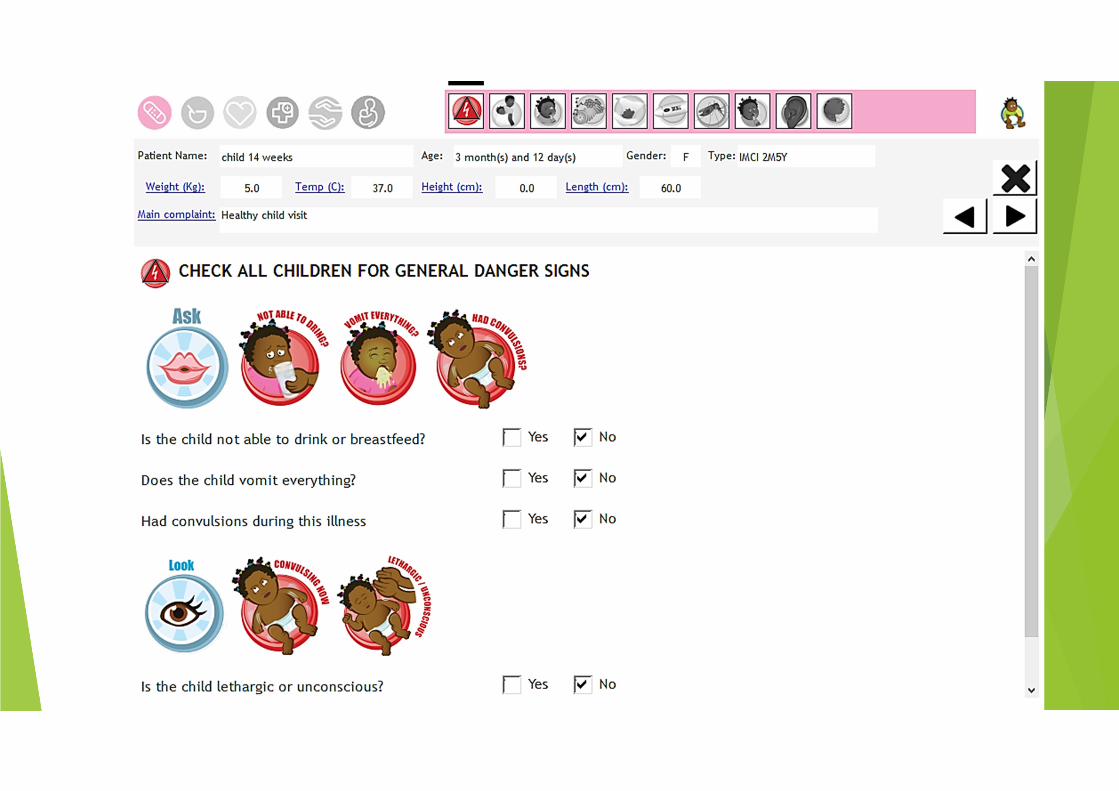
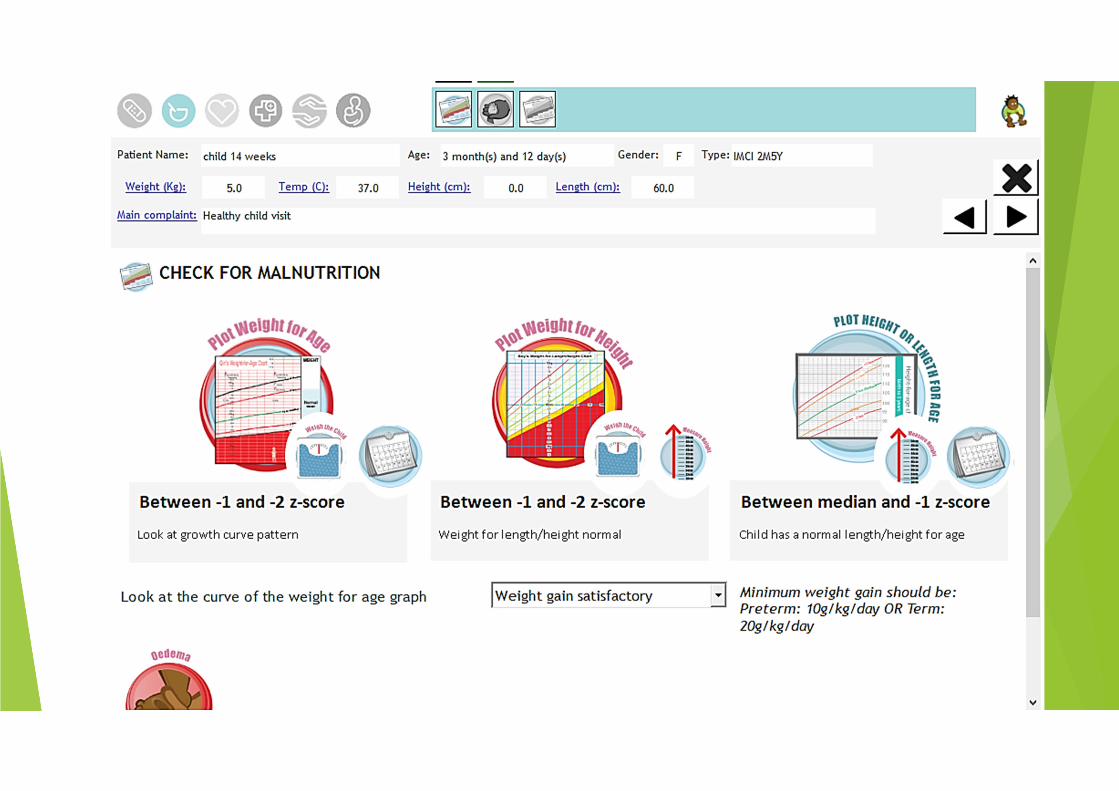
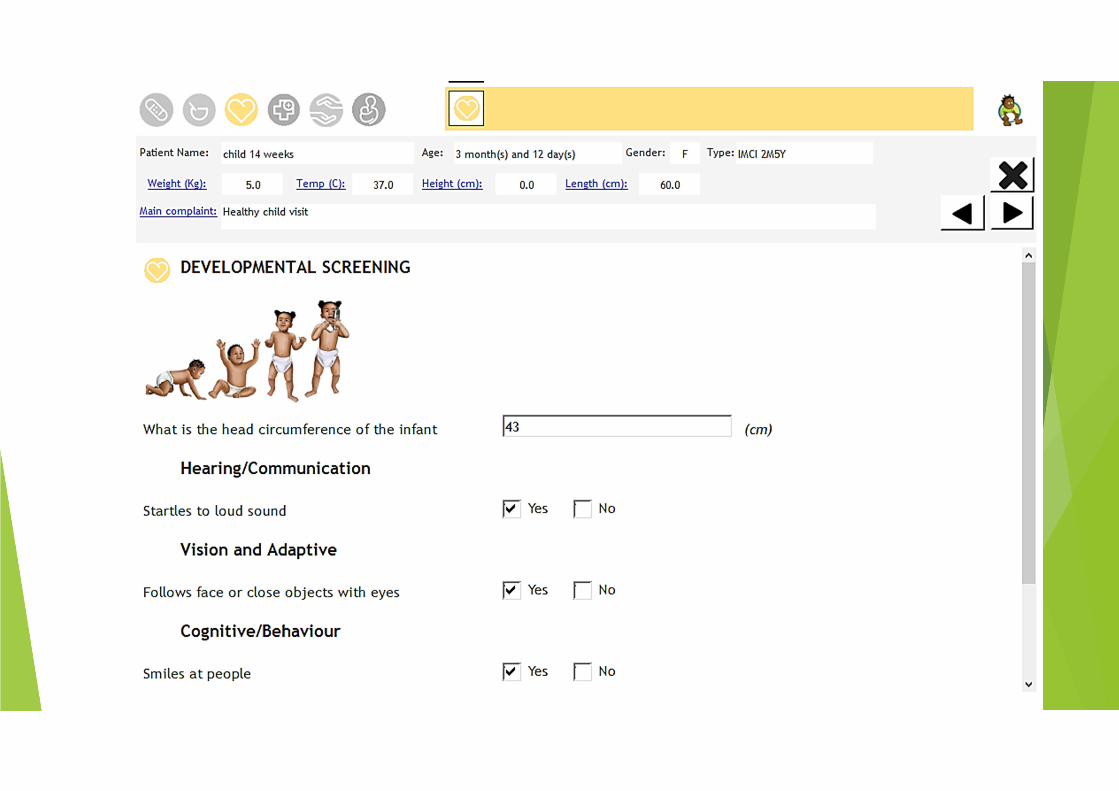
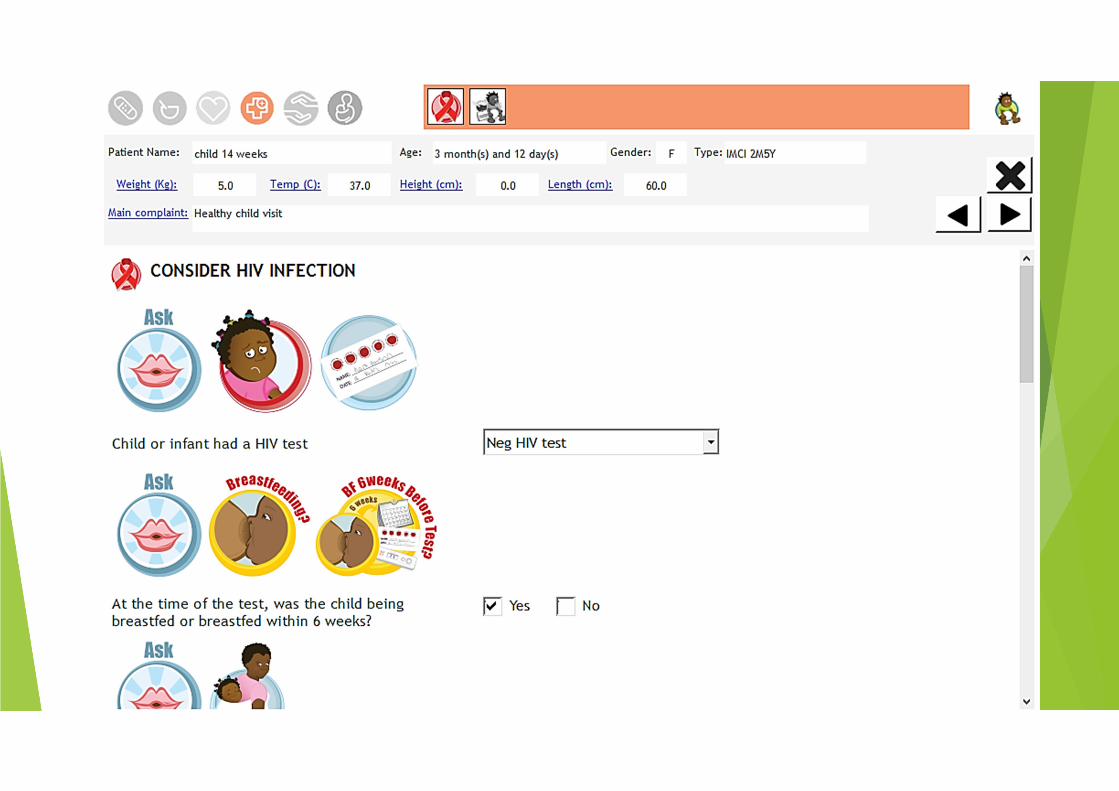
� User-friendly tools: IMCI colour checklists, electronic IMCI (eIMCI)
eIMCI software development
� Computer desktop tool – available hardware in DoH
� Health worker capacity: accessibility, decision support, automation
� Health systems: EMR, referral letters, data collection & reports
4. NDOH and UNICEF. Mid-Term Review of the Strategic Plan for MNCWH in SA 2012-2016.

Methodology
Data collection – uptake & acceptability
• eIMCI software: System use/ uptake.
• IMCI practitioners: Focus groups & questionnaires
• Operational Managers: In-depth interviews.
• Caregivers: Exit interviews.
Site selection and implementation
� 15 sites selected by uMgungundlovu District
� Baseline site assessments
� Training workshops (3d) in computer laboratory
� Implementation May – July 2018 (13 weeks)
� Support and mentorship:
� Weekly IT support calls
� Peer support cellphone texting group
� 2-3-weekly IT support visits
� Trouble shooting workshop after 3-4 weeks.
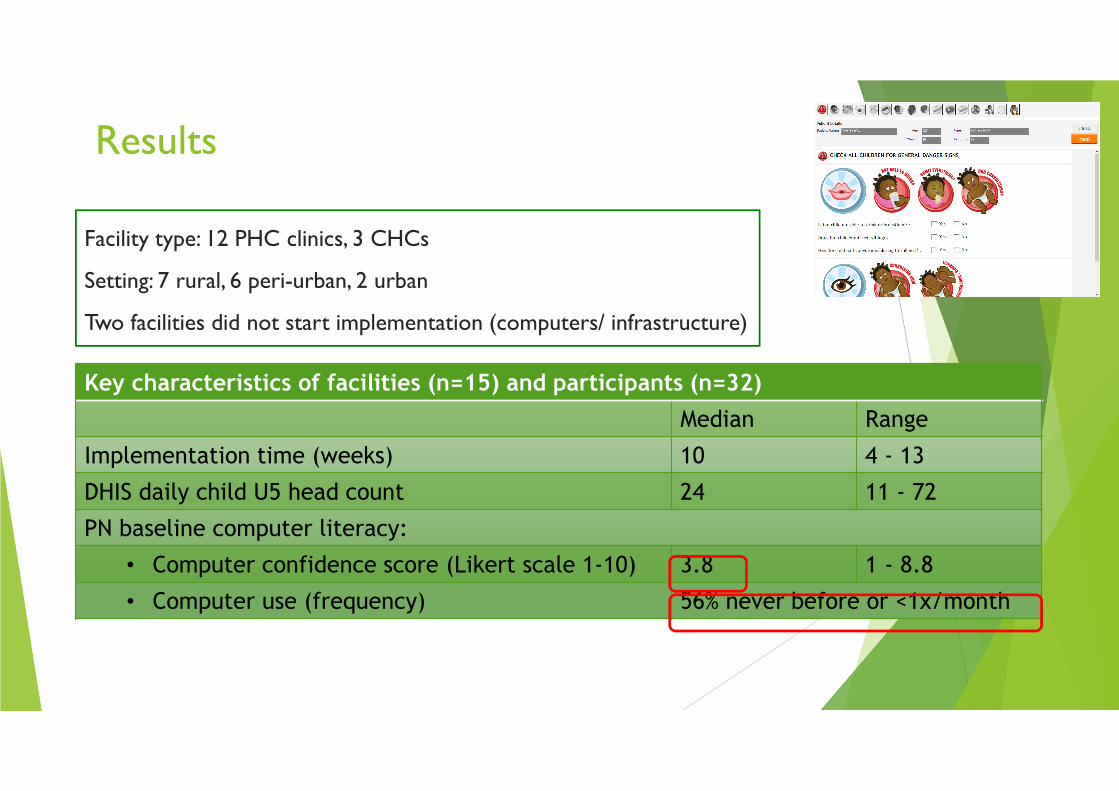
Results
Facility type: 12 PHC clinics, 3 CHCs
Setting: 7 rural, 6 peri-urban, 2 urban
Two facilities did not start implementation (computers/ infrastructure)
Key characteristics of facilities (n=15) and participants (n=32)
Median Range
Implementation time (weeks) 10 4 - 13
DHIS daily child U5 head count 24 11 - 72
PN baseline computer literacy:
• Computer confidence score (Likert scale 1-10) 3.8 1 - 8.8
• Computer use (frequency) 56% never before or <1x/month
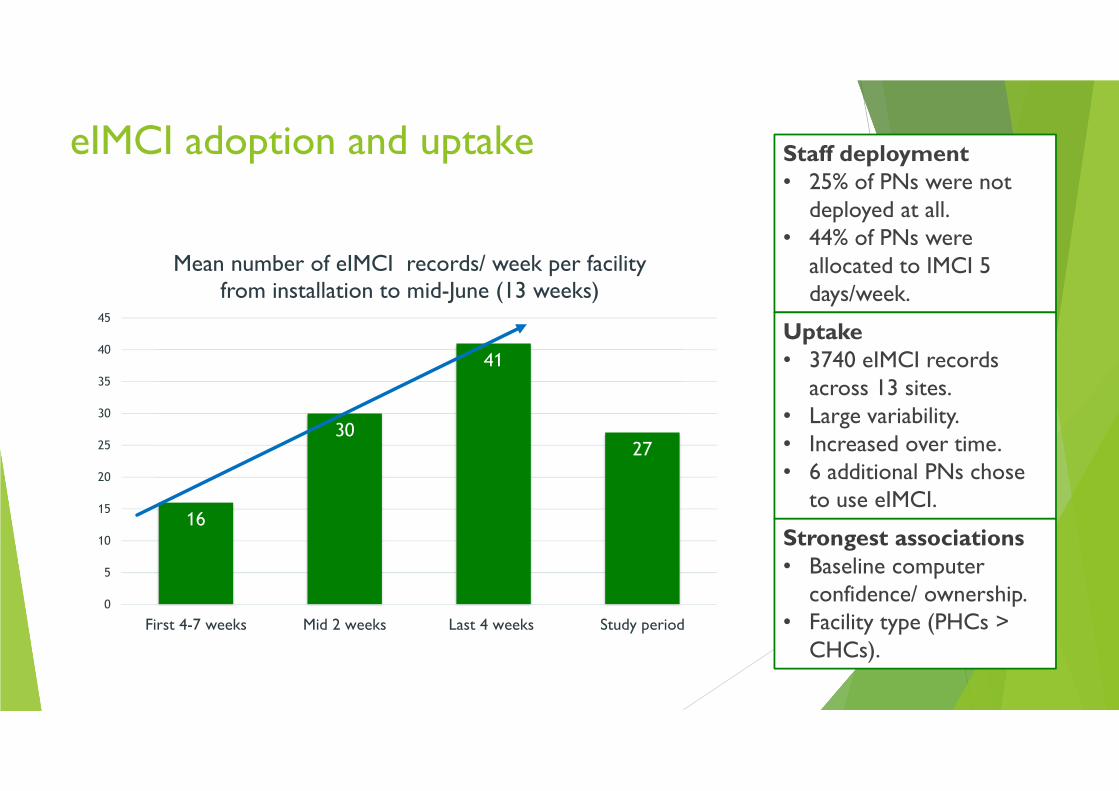
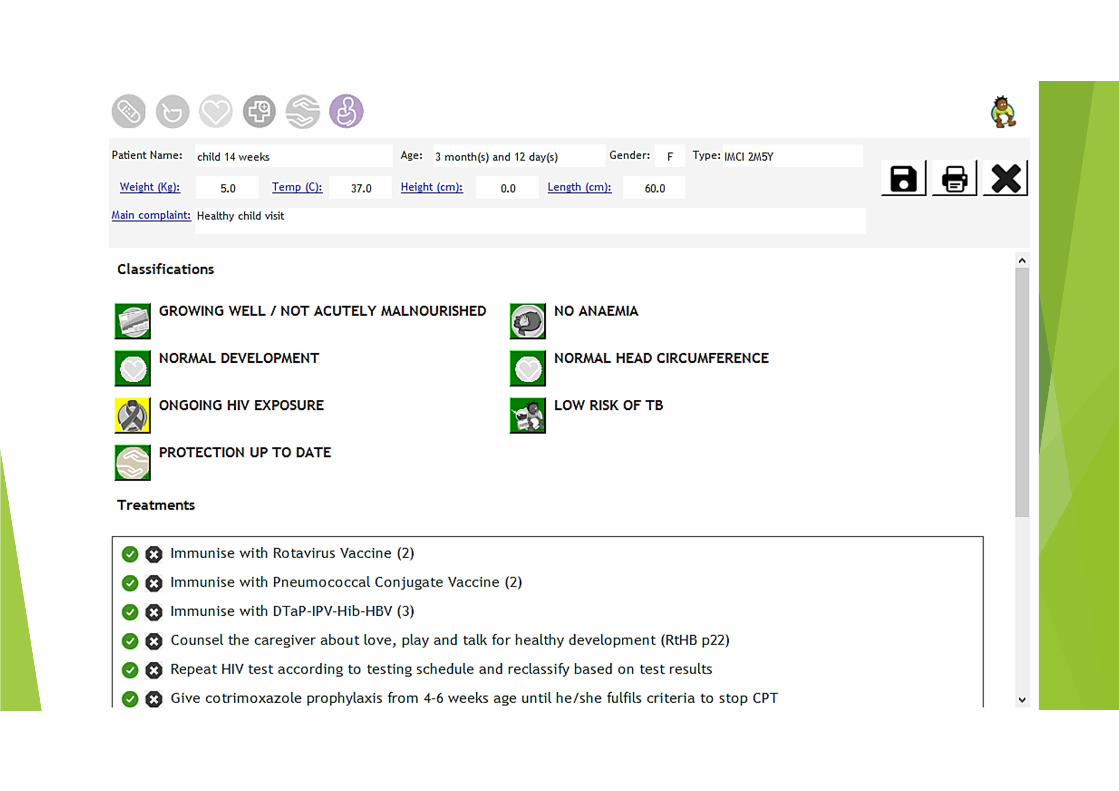
eIMCI adoption and uptake Staff deployment• 25% of PNs were not
deployed at all. • 44% of PNs were
allocated to IMCI 5 days/week.
16
30
41
27
0
5
10
15
20
25
30
35
40
45
First 4-7 weeks Mid 2 weeks Last 4 weeks Study period
Mean number of eIMCI records/ week per facility from installation to mid-June (13 weeks)
Uptake• 3740 eIMCI records
across 13 sites. • Large variability.• Increased over time. • 6 additional PNs chose
to use eIMCI.
Strongest associations• Baseline computer
confidence/ ownership. • Facility type (PHCs >
CHCs).

User acceptability
� Operational Managers
� High acceptance (benefits > disadvantages)
� Easy to accommodate & no additional resources required
� Mothers
� 76% reported marked difference in experience: comprehensiveness and efficiency
� IMCI practitioners
� High reported acceptance (benefits > disadvantages)
� Variability in uptake
� Significant improvement (p<0.05) in self-reported confidence and comprehensiveness of care
� Themes converged across 3 participant groups:
� Comprehensiveness/ holistic care
� Accuracy/ reduced errors/ HCW self-efficacy
� Efficiency/ reduced waiting times

Caregiver quotes
This visit was outstanding because I got help even for what I did not think of as a concern.
It saves time and I got a lot of information about my child's health.
The service is improved. There will now be a good history of a child in the computer as opposed to before when they only
relied on what the mother reports.
Before when they were using paper there were questions that were not asked, e.g. TB history at home and my (HIV) status as well as the child's status.

What now?
� Incremental KZN scale-up
� Funding secured for phase 2 roll-out and evaluation
� uMgungundlovu district
� Continue in 15 pilot clinics
� Add facilities with IT infrastructure (computers)
� Evaluate feasibility in real-life setting
� iLembe District
� Comparative evaluation (RCT) by UKZN: impact on quality of care
� 15 clinics eIMCI
� 15 control sites (paper-based)
� Strengthen tools and systems for supervision and monitoring
� If evaluations are favourable: roll out to remaining KZN districts

Thank you
Questions?
Contact:Dr Cecilie [email protected]: 071 892 5813
Special thanks to:• The ELMA foundation• Dr Neil McKerrow• Dr Deirdre Pansegrouw• Mr Shaun Krog • Dr Stephanie Thomas• Dr Gabrielle Wills

What happened since the pilot?
0
200
400
600
800
1000
1200
BruntvilleCHC
CaluzaClinic
CentralCity Clinic
GomaneClinic
ImpilwenhleClinic
InjabuloClinic
NdaleniClinic
RichmondClinic
SobantuClinic
SongonzimaClinic
TaylorsHalt Clinic
UMgungundlovu eIMCI uptake per pilot facility per quarter Q2 2018 - Q1 2019
Q2 2018 Q3 2018 Q4 2018 Q1 2019

Uptake & associations
Tobit regressionCoefficient Std. deviation Coefficient Std. deviation
PHC/ CHC facility (CHC = 0) 13.53** (3.32) 12.60** (2.77)IMCI practitioner characteristics:Reported case load per day -2.95 (1.32) -3.362* (1.95)Age -0.31* (1.83) -0.1 (0.48)Owns a PC (Does not own PC = 0) 15.29** (2.51)Confidence using a computer (scale 1-10) 3.302** (2.68)Qualification (PHC & short courses = 0)
Qualification: Basic nursing -9.29 (1.30) -13.26* (1.75)Qualification: Post basic/PHC 4.13 (0.53) 2.5 (0.38)
Qualification: Basic & short courses 8.38 (0.93) 9.719 (1.51)Constant 24.27* (1.79) 7.899 (0.49)Observations 32 32F statistics (p value) 9 (0.00) 10 (0.00)Notes: Significant at *p<0.1, **p<0.05, ***p<0.001. Standard errors are clustered as there are more than one IMCI
practitioner per facility. Coefficient: A 1-unit increase in the independent variable is associated with an X unit increase (+ve) or decrease (-ve) in the number of eIMCI
records per IMCI practitioner per week. As the sample size is small and the results sensitive, the magnitude of the coefficients must be
interpreted with caution.
Estimation of number of eIMCI records per IMCI practitioner divided by implementation weeks
Before After DifferenceP-value (one sided
t-test)
N (IMCI
pract.)
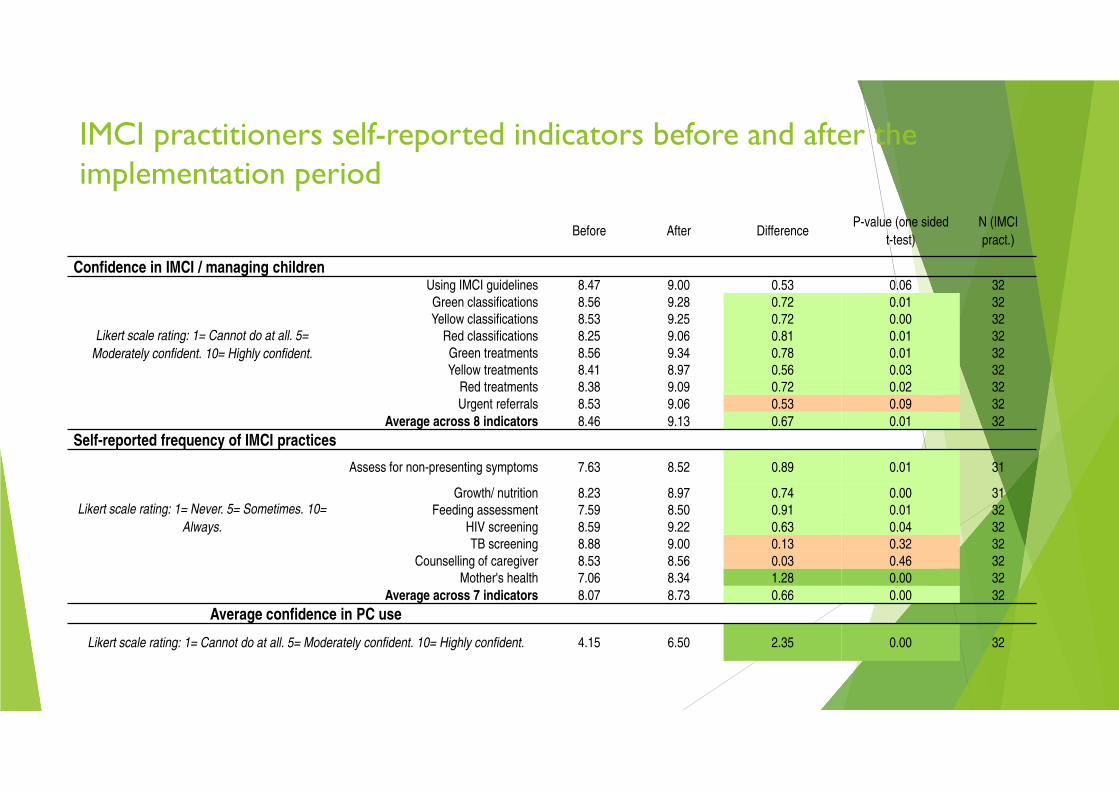
Confidence in IMCI / managing children
Likert scale rating: 1= Cannot do at all. 5=
Moderately confident. 10= Highly confident.
Using IMCI guidelines 8.47 9.00 0.53 0.06 32
Green classifications 8.56 9.28 0.72 0.01 32
Yellow classifications 8.53 9.25 0.72 0.00 32
Red classifications 8.25 9.06 0.81 0.01 32
Green treatments 8.56 9.34 0.78 0.01 32
Yellow treatments 8.41 8.97 0.56 0.03 32
Red treatments 8.38 9.09 0.72 0.02 32
Urgent referrals 8.53 9.06 0.53 0.09 32
Average across 8 indicators 8.46 9.13 0.67 0.01 32
Self-reported frequency of IMCI practices
Likert scale rating: 1= Never. 5= Sometimes. 10=
Always.
Assess for non-presenting symptoms 7.63 8.52 0.89 0.01 31
Growth/ nutrition 8.23 8.97 0.74 0.00 31
Feeding assessment 7.59 8.50 0.91 0.01 32
HIV screening 8.59 9.22 0.63 0.04 32
TB screening 8.88 9.00 0.13 0.32 32
Counselling of caregiver 8.53 8.56 0.03 0.46 32
Mother's health 7.06 8.34 1.28 0.00 32
Average across 7 indicators 8.07 8.73 0.66 0.00 32
Average confidence in PC use
Likert scale rating: 1= Cannot do at all. 5= Moderately confident. 10= Highly confident. 4.15 6.50 2.35 0.00 32
IMCI practitioners self-reported indicators before and after the implementation period
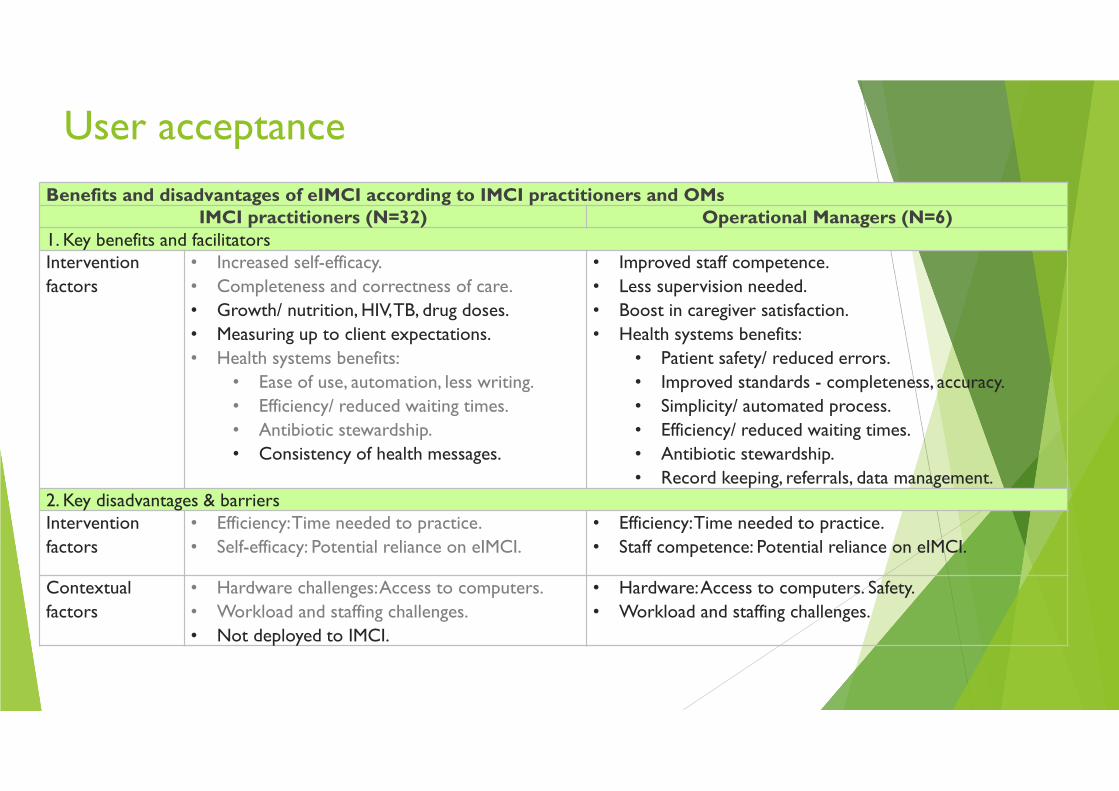
User acceptance
Benefits and disadvantages of eIMCI according to IMCI practitioners and OMs IMCI practitioners (N=32) Operational Managers (N=6)
1. Key benefits and facilitatorsIntervention
factors
• Increased self-efficacy.
• Completeness and correctness of care.
• Growth/ nutrition, HIV, TB, drug doses.
• Measuring up to client expectations.
• Health systems benefits:
• Ease of use, automation, less writing.
• Efficiency/ reduced waiting times.
• Antibiotic stewardship.
• Consistency of health messages.
• Improved staff competence.
• Less supervision needed.
• Boost in caregiver satisfaction.
• Health systems benefits:
• Patient safety/ reduced errors.
• Improved standards - completeness, accuracy.
• Simplicity/ automated process.
• Efficiency/ reduced waiting times.
• Antibiotic stewardship.
• Record keeping, referrals, data management.2. Key disadvantages & barriers Intervention
factors
• Efficiency: Time needed to practice.
• Self-efficacy: Potential reliance on eIMCI.
• Efficiency: Time needed to practice.
• Staff competence: Potential reliance on eIMCI.
Contextual
factors
• Hardware challenges:Access to computers.
• Workload and staffing challenges.
• Not deployed to IMCI.
• Hardware: Access to computers. Safety.
• Workload and staffing challenges.

Beneficiary acceptance
Key themes from caregiver interviews (N=30)
Theme number 1 2 3 4 5Occurrences per interview question Complete-
ness of care
Change in
service
Improved
communi-
cation
Improved
efficiency
Electronic
medical
recordsQuality of clinical care 22 2 11 2 0Quality of interpersonal interaction 8 3 28 0 0
Comparison with previous experiences 16 23 6 9 4Description of benefits with eIMCI 16 24 5 12 9Weighing benefit vs disadvantages of
eIMCI
12 14 14 8 9
Sum occurrences 74 66 55 31 22
Exit interviews with 30 mothers (6 sites) • 76% (23/30) reported: eIMCI consultation different from previous experiences • 100% (30/30) responded:
• No disadvantages of eIMCI • Computer not a barrier to communication • Would like the programme to continue