accelerating performance under risk-based contracts · page 2 acceerang performance under riskbased...
TRANSCRIPT

On the vanguard of thought. The future of healthcare requires nothing less.
W H I T E P A P E R
Accelerating Performance Under Risk-Based Contracts
Authors: Melissa McCain, Maureen Ward and Kaitlyn Faris

Accelerating Performance Under Risk-Based Contracts
Health systems are increasingly engaging in contractual arrangements in which they are responsible for the financial risk of a specific, targeted population. Often organizations do so without a full understanding of the competencies necessary to achieve the performance objectives; as a result, they do not execute on critical clinical and operational capabilities necessary for success. Many health systems turn to primary care as a solution to manage populations and contracts; while work in primary care offers some solutions, there are many more operational capabilities that are required in a risk environment such as analytics, network management, utilization management, and other care and service capabilities. Implementing new capabilities that integrate with and inform the existing care model without fundamentally changing it will accelerate an organization’s ability to succeed under risk contracts.
Current State and Key Challenges It is common for organizations to move along the continuum of risk-taking with the assumption that performance management mastered in pay-for-performance and shared savings contracts is simply leveraged into upside and downside risk contracts. This is an erroneous assumption. Each type of contract relies on different parts of the health system and different work:
P4P and Shared Savings
Upside Risk
Downside Risk
Financial Accountability
Shared between provider and payor
Shared between provider and payor Provider
Domain Impacting Performance Primary care
Primary, specialty and inpatient
services
All care services and network resources
Required Work
Care gaps and quality outcomes; care coordination
Population cohorts; quality outcomes;
transition and referral
management; costs of diagnosis-based
systems of care
Upside risk work, plus: care
management; clinical pathyways; provider performance; referral
management; utilization
management
Page 1
Applying an untested upside performance management system to a population in a downside risk contract is misguided.
Exhibit 1

Page 2
Accelerating Performance Under Risk-Based Contracts
Applying an untested upside performance management system to a population in a downside risk contract is misguided. Performance requirements, operational approaches and performance management activities must be differentiated by each contract’s specific requirements and aligned accordingly with the necessary interventions. This effort often results in multiple care models and multiple clinical interventions that can create confusion at the front lines of patient care.
Required Pivots When Preparing for Downside Risk ContractsThere are two distinct shifts in thinking – or pivots – that provider organizations must make to successfully execute on risk-based contracts. Providers must 1) behave like a clinically integrated network (CIN); and 2) leverage health plan capabilities.
Pivot 1- Behaving like a CIN: The network must actively manage itself to drive specific clinical outcomes, patient engagement and care that is planned, purposeful and coordinated for specific patient cohorts. This requires more than just an organizational structure with dedicated committees and appointed physician leaders; it requires a behavioral and cultural shift such that all providers and administrators agree to specific objectives, targets, behaviors and processes that consistently execute and perform against those targets. For example, an effective CIN will precisely define clinical, operating and medical expense targets, define specific action plans to achieve performance and relentlessly monitor and improve performance.
Pivot 2- Leveraging health plan capabilities: Provider organizations must build strong analytic and actuarial platforms to enable detailed patient cohorting to drive the development and implementation of targeted interventions. The cohorts should be created around psychographic and patient characteristics in addition to health risks. The provider entity must have a strong understanding of the various drivers of medical expense trends at the patient cohort level to inform strategies and tactics to improve health and reduce expense. Finally, it must institute utilization management (UM) programs that are intentional, multi-faceted and closely linked to network performance management. The UM programs should inform other population management capabilities, including navigation and referral management.
Page 2

Page 3
Accelerating Performance Under Risk-Based Contracts
An organization can begin to understand its progress against these two pivots by asking a series of related questions, including:
How can we use populations management data to develop network capacity and composition requirements?
How can we optimize referral management to ensure that patients are directed to the right provider and care, which includes steerage to preferred access points and prioritized providers?
How are we advancing our performance management and reporting approach to support contract performance?
How can we develop financial models that inform and identify utilization management opportunities and savings with minimal impact to current revenue?
How will we ensure that investments are focused on the contracted populations?
Is there clarity and agreement on the pace of and return on investment in populations and contract management?
Near-Term Solution through the Creation of a Shared Services OverlayFor most organizations participating in at-risk contracts, there is insufficient knowledge on what exactly needs to change related to performance management. Resource and intervention investments are more broadly applied than necessary, often as justification for the investment; this dilutes the ability to discern where true scale opportunities exist and must be leveraged. Organizations must align investments and optimize existing resources with the number of lives in at-risk contracts, until a tipping point is created that facilitates the shift to sustainable new care models for a broader set of patients. The investment balance is critical to cost effectiveness when operating in both a risk-based and fee-for-service environment.
In the near term, provider organizations engaging in risk-based contracting should invest in an “overlay” of shared services capabilities to establish the operational and clinical requirements for risk-based contracting. The overlay wraps around the existing clinical infrastructure and minimizes unnecessary disruption. The goal of the overlay is to improve patient health outcomes and reduce medical expense in at-risk contracts by efficiently leveraging organizational resources.

Page 4
Accelerating Performance Under Risk-Based Contracts
The Shared Services Overlay Drives Three Key Processes: Assign, Know and PredictThe overlay ensures that three critical process steps happen with all contracted patients, as illustrated in Exhibit 2. All patients are empaneled to a care team; the care team understands the patient’s health status and needs; and the health system actively works to manage utilization of resources.
Purpose
ExampleIndicativeMetrics
Create a reliable, well-defined process to empanel patients as the basis for care team and patient engagement, care delivery and performance measurement
Operate with a clear understanding of the panel’s health status and quality of life
Use patient segmentation and leverage standard clinical protocols, interventions and optimized care model processes to forecast utilization and associated care resources
z 90% of patients are accurately assigned to a provider using the PCP assignment algorithm
z 100% of providers in the PCP field meet the policy definition of PCP
z The PCP field is validated with providers twice/year
z Intervention utilization at 90% or higher
z 100% of patients requiring a plan of care have one that is referenceable in the patient record
z 80% of pharmacy, social work, mental health and community health services are delivered as a substitute to provider visits
z Care teams review panel performance metrics and execute improvement activities on a quarterly basis
z 90% of patients have completed onboarding process
z 100% of new patients have completed a first appointment
z Out of network utilization as a percentage of total utilization
z Actual intervention visit utilization as a percentage of all intervention referrals
z Percentage referrals to preferred sites of care
z Percentage of specialist to specialist referrals for a specific at-risk population cohort
z High performing providers as a percentage of all providers
AssignPatients
Know YourPanel
PredictUtilization
Exhibit 2
Page 5
Accelerating Performance Under Risk-Based Contracts
Network ModelThe right size & composition
z Enrollment & attributions
z Onboarding z Navigation
z Interventions z Product care
coordination z Pharmacy &
psychosocial services
z Referral management
z Network capacity & composition
z Network performance
Population Health AnalyticsInsights into cohort care requirements
Utilization ManagementOptimized use of resources
z Population segmentation z Payor data integration z Performance reporting
z Utilization trend tracking
z Practice change recommendations
Service ModelPatient engagement & steerage
Care ModelAppropriate patient care & services
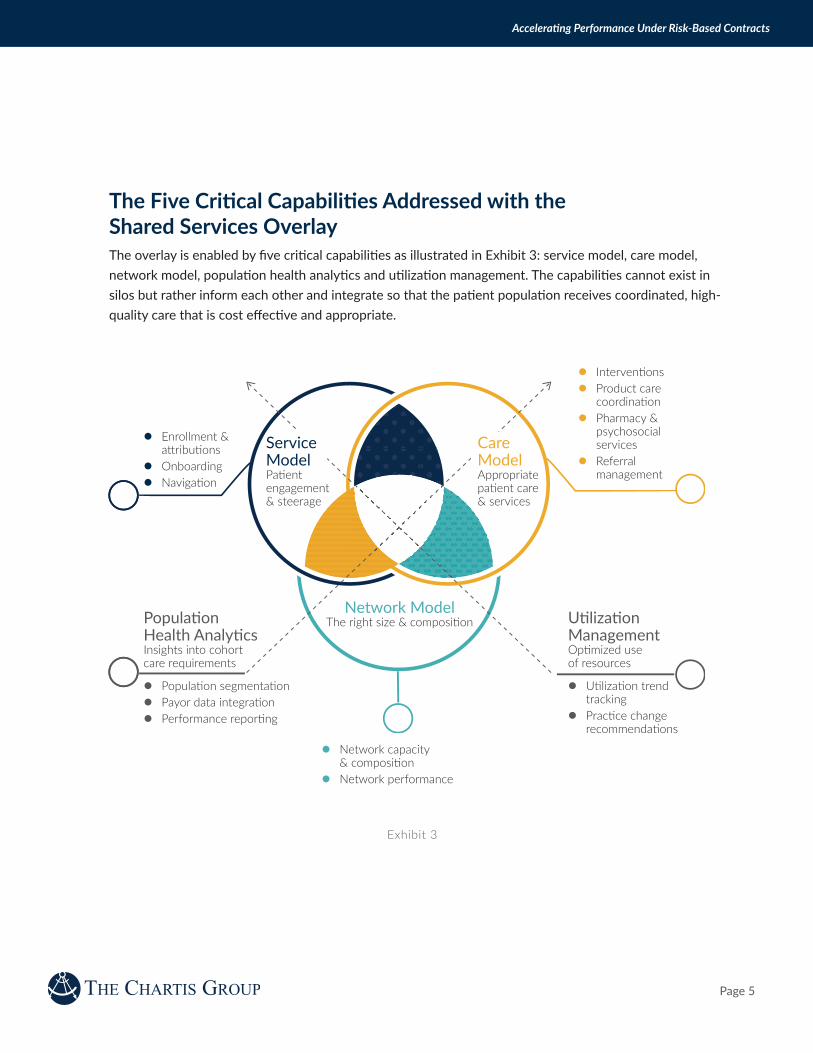
The Five Critical Capabilities Addressed with the Shared Services OverlayThe overlay is enabled by five critical capabilities as illustrated in Exhibit 3: service model, care model, network model, population health analytics and utilization management. The capabilities cannot exist in silos but rather inform each other and integrate so that the patient population receives coordinated, high-quality care that is cost effective and appropriate.
Exhibit 3

Page 6
Accelerating Performance Under Risk-Based Contracts
Service Model
Enrollment and Attribution. Enrollment and attribution should be a provider-driven function and not left to the payor. It requires an agreed-upon and broadly understood methodology for attributing patients to provider panels based on patient preference and activity. A governance mechanism should be established to inform when changes to attribution may occur, validate attribution changes and ensure patients are not dropped without valid reason or without re-attribution.
Onboarding. Onboarding is often the patient’s first interaction with the provider system when new coverage is achieved, and leaves a lasting impression. The first objective of onboarding is to orient patients to the network, including providers, services available and access points and locations. A vital function is to link patients to primary care providers if the patient is new to the network. Onboarding also evaluates whether a patient has immediate care needs due to concerning utilization patterns (e.g. frequent ED visits or hospitalizations) or for continuity of care (e.g. on warfarin).
Navigation. Navigation services provide patients with a single (clinical or non-clinical) point of contact for network questions, services available, access points and locations, appointment scheduling, benefits questions and occasionally claims and billing. This is a comprehensive patient engagement function that must be service-oriented and customer-friendly. It can also serve as a triage and steerage mechanism to guide patients to preferred access points and prioritized providers.
The service model overlay includes a suite of consumer engagement capabilities
that develop trust between the provider organization and the patient. The service model serves as the front door to the network and guides the patient through the health system. It also is responsive to the patient’s clinical
and non-clinical questions and needs.
1

Page 7
Accelerating Performance Under Risk-Based Contracts
2
Care Model
Interventions. The care model defines interventions for patient segments, identified
by population health analytic segmentation and micro-segmentation. Interventions are actions
taken to improve a patient’s health status or mitigate health risk; they are developed based on the needs and
health profile of the population under management and are then prioritized based on the most critical needs of the patient. Interventions should have a measurable and observable impact on medical expense and health risk factors.
Product Care Coordination. Product care coordinators assess the needs of the contracted population to ensure patients are engaged and gain access to the appropriate interventions. They confirm that the interventions are prioritized according to the patient’s needs. Further, product care coordinators work closely with primary care teams to ensure that providers are aware of the services that may benefit the patients in their panel.
Pharmacy and Psychosocial Services. Patients in risk-based contracts will likely benefit from low-cost pharmacy and psychosocial services to improve health and manage utilization, including but not limited to clinical pharmacy, behavioral health, social work and community health. Patients are identified for specific services based on identification algorithms, and assessment and screening tools.
Referral Management. Referral management leverages information from population health and utilization management analytics and identifies preferred sites of care and specialists based on cost, quality and providers’ adherence to standards of care. Referral management then feeds the consumer-facing navigation capability to steer patients to the most appropriate sites of care. Referral management may also influence practice standards as it relates to primary care to specialist and specialist to specialist referral patterns.
The care model overlay wraps around the primary care team to
coordinate care and provide patients with access to the resources they need
from specialty care, pharmacy, social work, behavioral health and community health. The overlay ensures that patients under risk-based contracts receive the services they need
without requiring an overhaul of the foundational primary care model.

Page 8
Accelerating Performance Under Risk-Based Contracts
3
Network Model
Network Capacity and Composition. Population segmentation informs network
requirements, providing insights for intentional design and use of network resources by understanding the
clinical and resource needs of the contracted population. Network management ensures that there are sufficient high-
performing clinicians by specialty to deliver appropriate care to the population cohorts under contract. The function also calibrates
and aligns network resources with the lives under contract by geography and other criteria that become market drivers, for example, consumer preferences on access.
Network Performance. Network performance is an important competency that uses practice insights to drive network management. For example, network referral management guidelines are informed by specialist cohort performance, and more specifically, individual specialty provider performance. Care is directed to high performing providers who thereby receive a higher proportion of referrals to sustain network performance while providers who have opportunities to improve their performance learn to optimize their practices. Network capacity is ultimately determined and optimized by performance standards set by high performing provider cohorts and providers.
The network model includes administrative functions to manage
the network and payor products including network capacity and composition, as well as performance. With population segmentation, network capabilities and capacity are no
longer a guessing game of resources required for risk-based contracts.

Page 9
Accelerating Performance Under Risk-Based Contracts
Population Health Analytics & Performance Reporting
Effective population health analytics create insights into population-based care requirements by identifying patient cohorts that have generated or are expected to generate high medical spend and may benefit from targeted interventions to improve health. The population health analytics overlay should focus on the segmentation and micro-segmentation of priority patient cohorts that are tailored to specific interventions.
Population Segmentation. Population health analytic insights inform what programs will be most beneficial to the population under management and identify trends that are contributing to higher than expected medical expense (see utilization management for additional detail). Risk stratification methodologies serve several purposes including driving insight into the actuarial risk of a population, identifying care needs and driving insight into the relative risk of panels for risk adjustment.
Payor Data Integration. Payor data integration includes requesting, receiving and integrating data from the product’s payor into the analytical tools at the provider organization, including eligibility files, demographic information and prior claims data including any out of network utilization. Integrating payor data with clinical data from the provider’s electronic medical records provides robust insights into the health and utilization of the population, which can in turn feed the population health analytics and utilization management programs.
Performance Reporting. Performance reporting aligns the network components and is the intentional foundation that drives the network and its resources to behave as a clinically integrated unit. While network scorecards and dashboards track overall success against target metrics, performance expectations can be communicated and tested through nested reports based on drill down capabilities, to track the actual performance at various levels, including product, facility, specific provider and panel levels. Performance reporting at the provider and panel levels provides important insights into opportunities to improve results. Used by the care teams, these reports identify patients on the provider’s panel that have gaps to target outcomes and/or opportunities to shift utilization. High performing provider practices can be identified, and best practices codified and leveraged into practices that require improvement, driving success in the aggregate.

Page 10
Accelerating Performance Under Risk-Based Contracts
Utilization Management
A utilization management (UM) program monitors the utilization and the drivers of utilization (practice standards, clinical variation, etc.) of the population under management with the goal of maximizing appropriate care, reducing unnecessary care and predicting resource consumption. UM also identifies admissions, procedural, specialist, primary care and pharmaceutical-driven utilization and trends.
Utilization Trend Tracking. UM programs may include, but are not limited to, the evaluation of medical necessity and appropriateness; population utilization rates and quality indicators; and clinicians’ utilization trends and standards of care relative to other network clinicians, predetermined standards of care and regional and national benchmarks. The program may also monitor out-of-network utilization and coordinate transfers to in-network facilities, as needed.
Practice Change Recommendations. Ideally the UM program is a single, centralized resource to the network. Network analysts study and evaluate network utilization, and in partnership with clinical consultants, identify opportunities that shift utilization and positively influence outcomes. They can model the financial impact of applying the UM lens through specific population segmentation. The same consultative team recommends UM policy changes that are necessary to facilitate and govern the desired practice changes which influence utilization and utilization management.
5
The overlay of shared services capabilities can be built in the near term to address the operational and clinical requirements for value-based payor contracting without changing the entire care delivery system. The goal of the overlay on current clinical operations and management is to optimize the outcomes of patients in at-risk contracts while simultaneously optimizing organizational resources. The overlay is the mechanism that provides insight into that tipping point and positions the organization for successful execution in the value-based landscape.

Page 11
Accelerating Performance Under Risk-Based Contracts
About the Authors
Melissa [email protected]
Melissa McCain is a Director of The Chartis Group and is a leader in the firm’s Performance practice. Ms. McCain has over 22 years of advisory services and health system leadership experience. She has spent the last several years as an advisor to executive leadership on the development and successful execution of operational strategy to support organizational economic and mission sustainability. She directs consulting engagements in the areas of clinical transformation, operational performance improvement and value-based clinical program planning.
Maureen WardAssociate [email protected]
Maureen Ward is an Associate Principal with The Chartis Group. She has over 20 years of leadership experience in the healthcare industry, with a focus on population health and care management in both provider and payor settings. Drawing on her deep expertise in clinical operations and change management, Ms. Ward helps organizations develop and operationalize new clinical programs and supporting functions and capabilities to improve performance under traditional and innovative value-based care models.
Kaitlyn [email protected]
Kaitlyn Faris is a Director of New Products at Aspire Health, a provider of in-home palliative care services headquartered in Nashville, TN. In her role, Kaitlyn is focused on developing strategic partnerships and expanding Aspire’s product offerings. At the time of writing, Kaitlyn was an Engagement Manager at The Chartis Group.

© 2018 The Chartis Group, LLC. All rights reserved. This content draws on the research and experience of Chartis consultants and other sources. It is for general information purposes only and should not be used as a substitute for consultation with professional advisors.
Atlanta | Boston | Chicago | Minneapolis | New York | San Francisco
About The Chartis Group
The Chartis Group® (Chartis) provides comprehensive advisory services and analytics to the healthcare industry. With an unparalleled depth of expertise in strategic planning, performance excellence, informatics and technology, and health analytics, Chartis helps leading academic medical centers, integrated delivery networks, children’s hospitals and healthcare service organizations achieve transformative results. Chartis has offices in Atlanta, Boston, Chicago, New York, Minneapolis and San Francisco. For more information, visit www.chartis.com.