academic detailing improving patient safety through informed medication prescribing and disposal...
Post on 19-Dec-2015
214 views
TRANSCRIPT
Academic Detailing
Improving Patient Safety Through Informed Medication Prescribing and Disposal Practices
Portland ME
October 2007
Michael Allen MD
Dalhousie University Continuing Medical Education
3
Outline
• Definition
• Evidence - general
• Evidence - specific
• Dalhousie program
• Canadian academic detailing
• US academic detailing
4
Academic Detailing
• One-on-one educational intervention provided to physicians in their office by a trained health care professional
• Evidence-based
• Information for clinical decisions
6
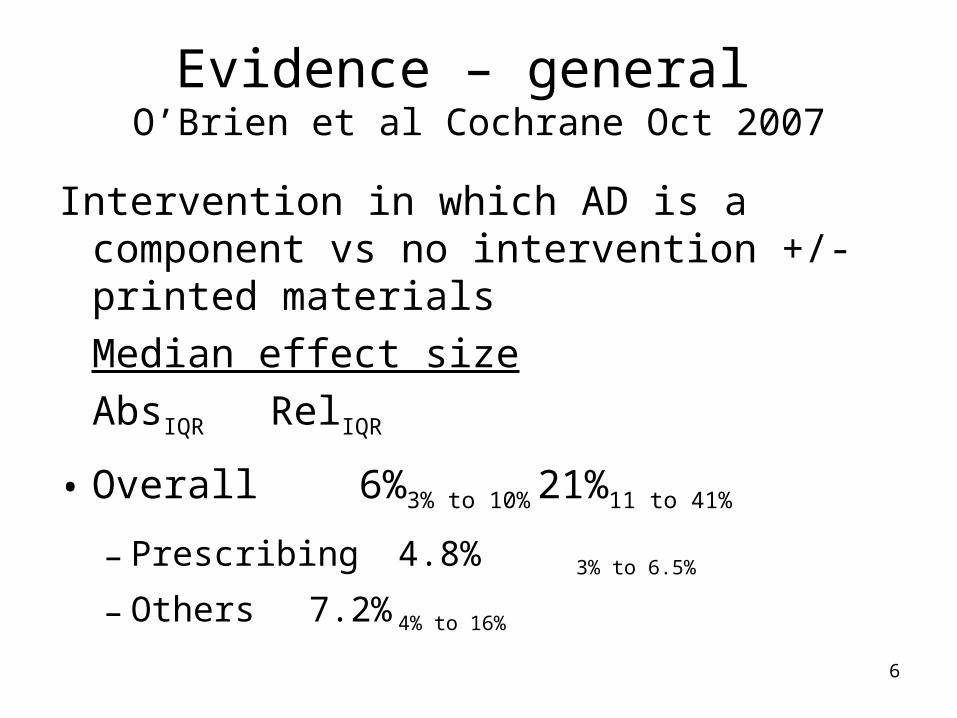
Evidence – general O’Brien et al Cochrane Oct 2007
Intervention in which AD is a component vs no intervention +/- printed materials
Median effect size
AbsIQR RelIQR
• Overall 6%3% to 10% 21%11 to 41%
– Prescribing 4.8% 3% to 6.5%
– Others 7.2% 4% to 16%
7
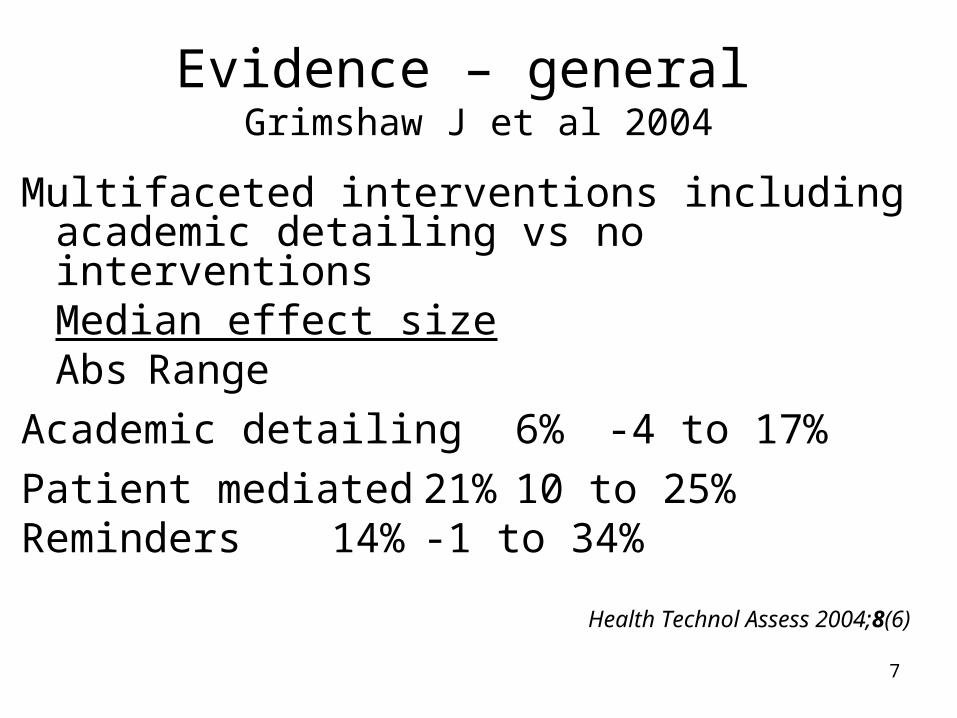
Evidence – general Grimshaw J et al 2004
Multifaceted interventions including academic detailing vs no interventions
Median effect sizeAbs Range
Academic detailing 6% -4 to 17%
Patient mediated21% 10 to 25%Reminders 14% -1 to 34%
Health Technol Assess 2004;8(6)
8
Evidence – specificBenzodiazepines Zwar, Aus Fam Physician, 2000
• 20 minute visit to 79 GP-registrars re gradual withdrawal of benzos for anxiety or insomnia if indicated
• Management guidelines – gradual withdrawal • Patient education aids re relaxation • Prescribing evaluated by 3 practice-activity
surveys of 110 consecutive patients at 6 mos intervals
• Both groups decreased prescribing – no diff• Need to involve patients, family, nursing staff
9
Evidence – specificBenzodiazepines de Burgh Aus J Pub Health 1995
• ~142 FPs in New South Wales in control and intervention groups
• Baseline survey of 110 consecutive patients• 20 minute academic detailing visit
– Indications for benzos– Patient education material for sleep– Approach to management of long-term users– Asked to review 5 patients on long-term benzos with
review card– Follow-up phone call to assess docs reaction
• Survey 110 consecutive patients 5 months later
10
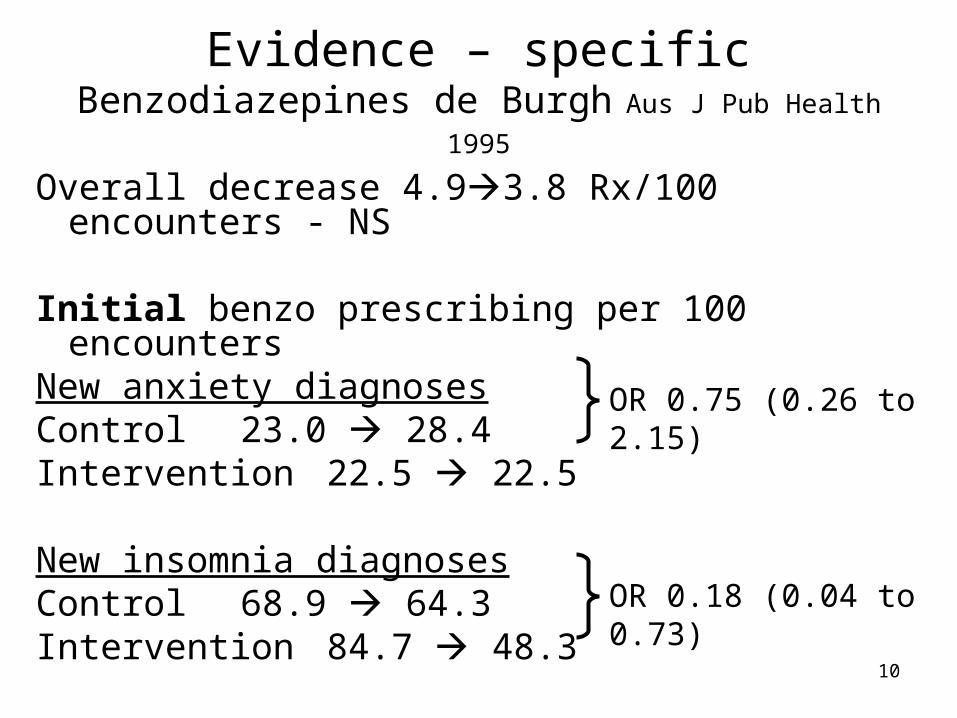
Evidence – specificBenzodiazepines de Burgh Aus J Pub Health 1995
Overall decrease 4.93.8 Rx/100 encounters - NS
Initial benzo prescribing per 100 encountersNew anxiety diagnosesControl 23.0 28.4Intervention 22.5 22.5
New insomnia diagnosesControl 68.9 64.3Intervention 84.7 48.3
OR 0.75 (0.26 to 2.15)
OR 0.18 (0.04 to 0.73)
11
Evidence – specificBenzodiazepines Berings Euro J Clin Pharmacol 1994
• FPs – 3 groups – N~43 each group– Written material + academic detailing– Written material– Control – no information
• Written material similar to drug ads– Rational and short-term use of benzos– Limited long-term benefit of benzos– Cognitive and emotional side effects of benzos– Importance of habituation and dependence
12
Evidence – specificBenzodiazepines Berings Euro J Clin Pharmacol 1994
• Data collected by surveys before and 4 weeks after interventions
• 85% repeat users, 15% new prescriptions
• # packs of benzos per 100 patient contacts– Written material + AD 14.1 10.8 ↓24%– Written material 13.0 11.2 ↓14%– Control 14.7 14.2 ↓3%
ANOVA F=4.7, df 2 P<0.05
13
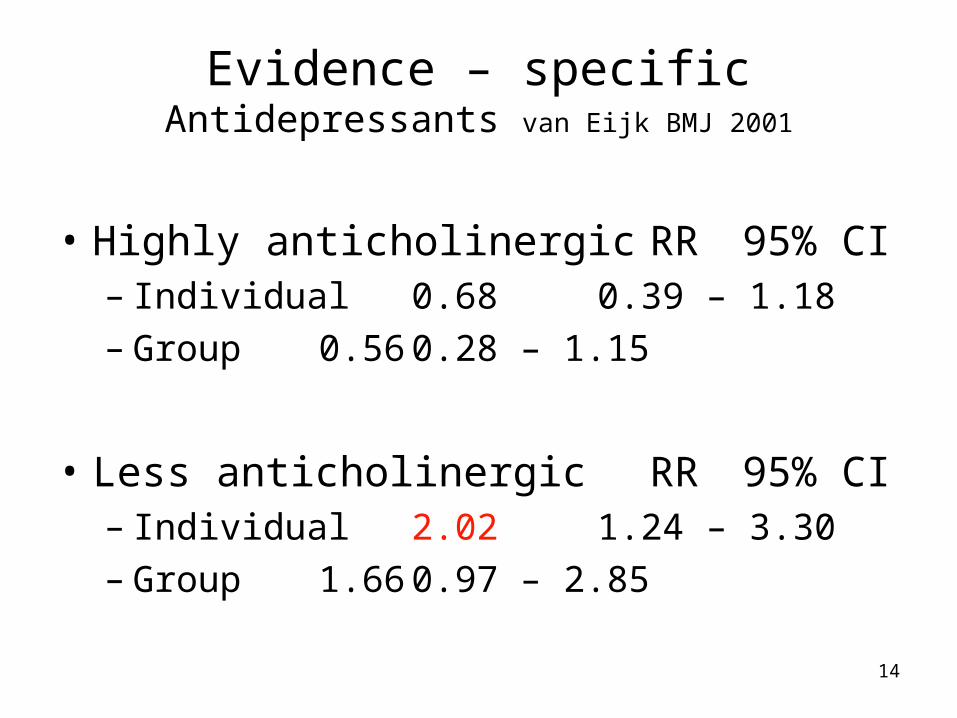
Evidence – specificAntidepressants van Eijk BMJ 2001
• Individual vs group vs control ~ 40 docs 14 pharms per group
• 2 visits 4 mos apart– Content then prescribing profile
• Data collected from pharmacy reimbursement databases
14
Evidence – specificAntidepressants van Eijk BMJ 2001
• Highly anticholinergic RR 95% CI – Individual 0.68 0.39 – 1.18– Group 0.56 0.28 –
1.15
• Less anticholinergic RR 95% CI – Individual 2.02 1.24 – 3.30– Group 1.66 0.97 –
2.85
15
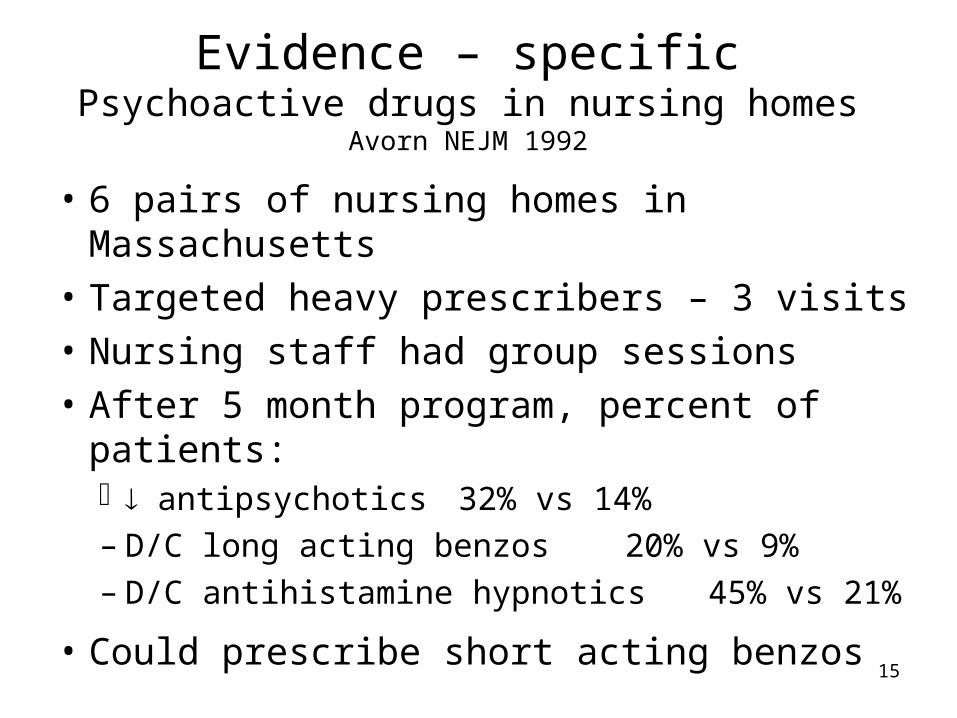
Evidence – specificPsychoactive drugs in nursing homes Avorn NEJM 1992
• 6 pairs of nursing homes in Massachusetts
• Targeted heavy prescribers – 3 visits
• Nursing staff had group sessions
• After 5 month program, percent of patients: antipsychotics 32% vs 14%– D/C long acting benzos 20% vs 9%– D/C antihistamine hypnotics 45% vs 21%
• Could prescribe short acting benzos
16
Suggestions
• Changing psychotrophic prescribing complex and difficult.
• May be easier to affect new prescribing
• Insomnia may be easier than anxiety
• May need to involve more than MDs
• Academic detailing may not be enough
• Review these and other papers
18
Dalhousie Academic Detailing Service
• Started fall 2001
– 3 academic detailers
• 2 pharmacists, 1 nurse
• Advisory committee
– 4 family physicians
– Content expert
19
Dalhousie Academic Detailing Service
• Each topic see ~ 350 FPs +
–Nurse practitioners
–Medical students/residents
–Nurses
–Pharmacists
20
Dalhousie Academic Detailing Service
• Handout
– 30-40 page booklet
– Summary statements
– Double-sided laminate
22
Canadian Academic Detailing Collaboration (CADC)
• British Columbia (est. 1993)– BC Community Drug Utilization Program– 50-60 general practitioners in North/West Vancouver– www.cdup.org
• Alberta (est. 2001, then 2006)– Academic Detailing – Calgary Health Region – 150 urban physicians– www.calgaryhealthregion.ca
• Saskatchewan (est. 1997)– RxFiles Academic Detailing Program– 400 physicians and other HCPs in SK– www.rxfiles.ca
• Manitoba (est. 2003)– Prescription Information Services of Manitoba– 70 general practitioners– www.prisminfo.org
• Nova Scotia (est. 2001)– Dalhousie Academic Detailing Services– 350 physicians and other HCPs in Nova Scotia– http://cme.medicine.dal.ca/ADS.htm
23
25
1. Outcomes evaluation – BC
2. Use of technology in ADing – BC
3. Canadian/international experience with ADing
4. Evaluate printed educational materials – AB
5. Time and motion study – SK
6. Needs assessment – MB
7. Physicians’ perceptions of ADing – NS
Research
26
Physician education beyond ADing
• Grand Rounds– U of SK internal med, neurology, geriatrics– Dalhousie - cardiology, respirology, geriatrics
• Anti-infective and antihypertensive courses in SK and at national Family Medicine Forum
• Conference presentations
• PowerPoint slides and printed materials
• Collaboration with the CMA
27
Educating other health professionals
• Medical students• Residents • Pharmacy students:
– PharmD, MSc Undergrad
– Applying EBM to drug decisions
• Pharmacists• Nurses• Nurse practitioners• Psychologists• Physiotherapists• Diabetes educators
Students Other HCPs
29
Guidelines development & review
• Hypertension – Review Panel (Toronto-MUMs)
– Canadian Consensus input
• Health Quality Council – SK– Post-MI drugs
• Acute coronary syndrome• STEMI• COMPUS Expert Review Committee
NS
30
Commentaries/publications
• RxFiles Drug Comparison Chart Book – 6th edition (current CMA best-seller)– All SK physicians, pharmacies & 3000+
nationally
• Measuring prescribing improvements– Basic & Clinical Pharmacology &
Toxicology 2006; 98, 243-52.
31
Commentaries/publications
• Coxibs– CMAJ 2005;173:83
• Statin guidelines– Can J Cardiol 2007– AFP 2006;73:973-4
33
34
Academic Detailing in USA
• Kentucky– Frank May [email protected]
• Pennsylvania – Independent Drug Information Service– Michelle Spetman [email protected]
• Vermont– Charles Maclean
[email protected]– http://www.med.uvm.edu/ahec/TB1+BL.asp?SiteAreaID=290