absent pulmonary valve
TRANSCRIPT

ABSENT PULMONARY VALVE
SYNDROME
Dr.Sherif Sabet
PSCC

Absent Pulmonary Valve Syndrome is Fascinating
and unique variety of structural heart disease!
Moss and Adams’

PATHOLOGY
Tetralogy of Fallot with an absent pulmonary valve
occurs in approximately 2% of patients with TOF.
The pulmonary valve leaflets are either completely
absent or have an uneven rim of rudimentary valve tissue
present
Rudimentary pulmonary valve is typically both stenotic
and regurgitant with aneurysmally dilated pulmonary
arteries, and a large malaligned outlet ventricular septal
defect (VSD)

The massive pulmonary artery aneurysm
develops during fetal life.
It compresses the developing trachea and
bronchi throughout fetal life.

Airway obstruction and respiratory distress during
infancy.
Pulmonary complications (e.g.,atelectasis,
pneumonia), rather than the intracardiac defect, are the
usual causes of death.

Clinical Manifestations
Mild cyanosis
Signs of CHF may develop after the
newborn period
Respiratory symptoms

To-and-fro murmur (with “sawing-wood”
sound) at the upper and mid-left sternal
Borders
The S2 is loud and single

The ECG shows RAD and RVH
Chest radiography images reveal a
noticeably dilated main PA and hilar Pas
Echocardiography
CT or MRI scan

MANAGEMENT
After the pulmonary symptoms appear,
neither surgical nor medical management
has good results.
Symptomatic neonates should have
corrective surgery on an urgent basis. Even
asymptomatic children should have elective
surgery in the first 3 to 6 month of life.

Complete primary repair is the procedure of
choice. VSD is closed through right
ventriculotomy
(across the pulmonary annulus).
Alternatively, a valved conduit may be used to
restore competence of the pulmonary valve,
and the aneurysmal PAs are plicated


REAL CTA CASES
Absent Pulmonary Valve Syndrome

EPARTERIAL HYPARTERIAL

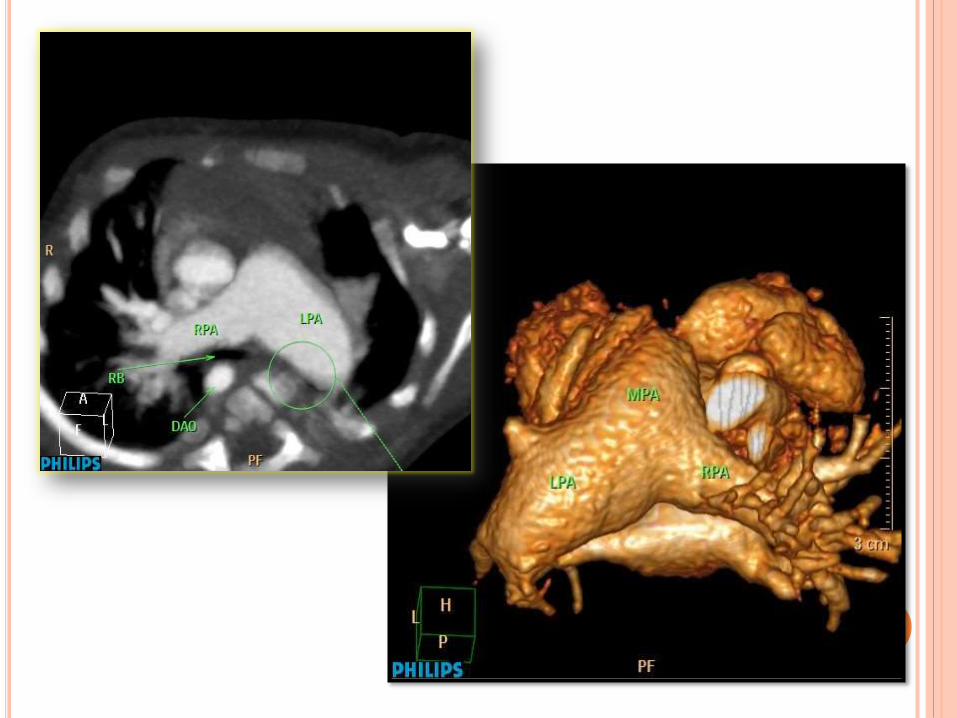
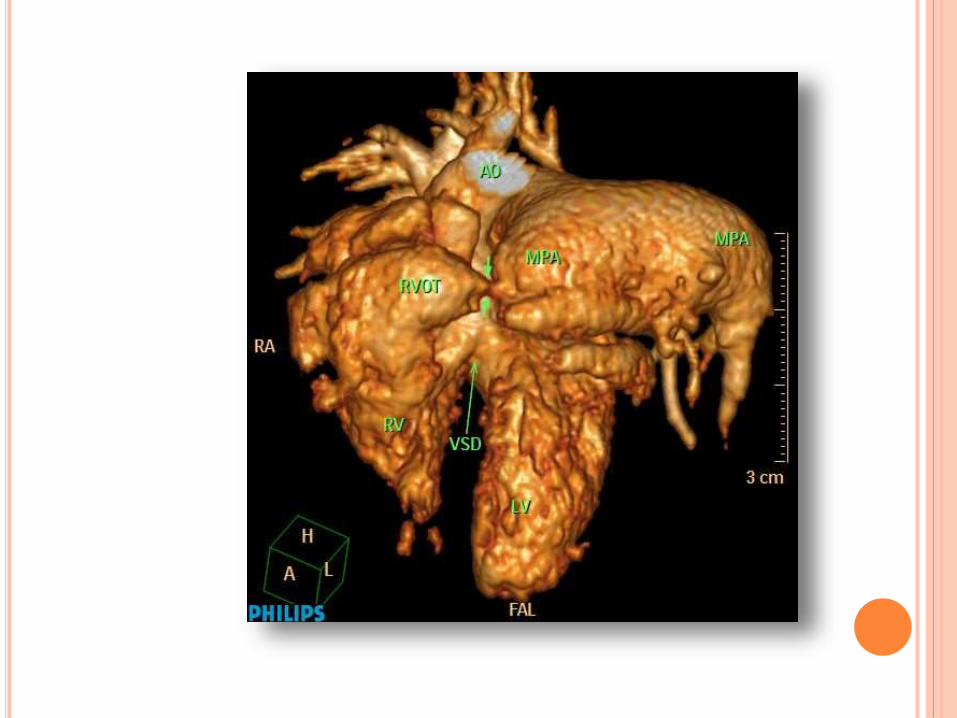
CASE #1
13 MONTH-OLD BOY
S/P TOF REPAIR


Huge RPA
Huge MPA
Severe PS
Aneurysmal RVOT


Posterior

CASE #2
8 MONTH-OLD GIRL




Case 3
35 Days girl




Home Message:
Absent Pulmonary Valve Syndrome
Pulmonary valve is both stenotic and regurgitant.
The massively dilated pulmonary arteries compresses
the trachea from the fetal life
Should be corrected soon after diagnosis.

Thank You
Dr.Sherif Sabet