abdominal trauma - · pdf file“chemical peritonitis” which may not appear as a...
TRANSCRIPT

ABDOMINAL TRAUMA
Trauma Intensive Care Unit

Objectives
At the end of this presentation, the participants will be able to:
– Describe abdominal anatomy and functions of individual abdominal
organs
– Differentiate between blunt and penetrating trauma
– Discuss different diagnostic tools used in abdominal trauma
– Describe the management of organs injured by abdominal trauma
Abdominal Trauma
Abdominal trauma is an injury to the abdomen. It may be blunt or penetrating and may involve damage to the abdominal organs
• The abdomen is highly susceptible to injury because of it’s location and lack of boney protection
• The pediatric population are highly vulnerable because their solid organs are comparatively larger and they have less musculature and padding
• Injuries may go undiagnosed due to vast amounts of free space in abdominal cavity.
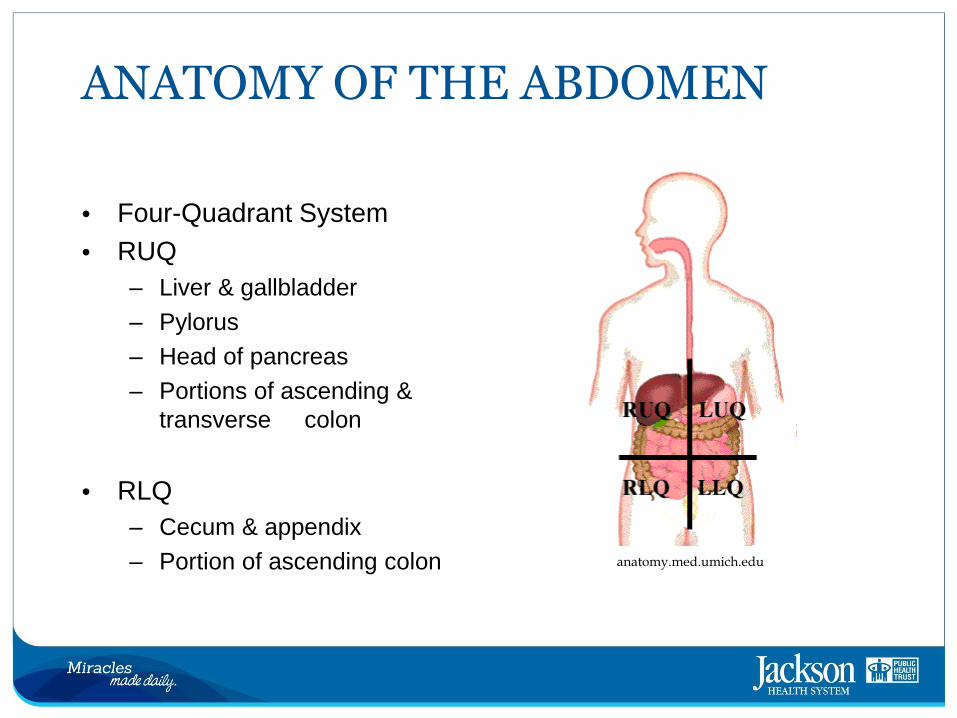
ANATOMY OF THE ABDOMEN
• Four-Quadrant System
• RUQ
– Liver & gallbladder
– Pylorus
– Head of pancreas
– Portions of ascending &
transverse colon
• RLQ
– Cecum & appendix
– Portion of ascending colon
anatomy.med.umich.edu

QUADRANTS (Continued)
• RLQ
– Bladder (if distended), Right ureter
• LUQ
– Stomach
– Spleen
– Body of pancreas
– Portions of transverse and descending colon
• LLQ
– Sigmoid colon, portion of descending colon
– Bladder (if distended), Left ureter


Peritoneal vs Retroperitoneal
• Abdominal Cavity
• Peritoneal
– Stomach
– Small intestines
– Liver
– Gallbladder
– Transverse & sigmoid
– Part of bladder

• Retroperitoneal
• Part of the duodenum
– Ascending colon
– Descending colon
– Kidneys
– Part of the bladder
– Pancreas
– Major vessels
becomehealthynow.com

Blunt Trauma to the Abdomen
• Blunt Trauma – Trauma that occurs without entry of the injuring agent into or through the skin
• Leading cause of intra-abdominal injury, with MVCs being first
• Common organs injured – spleen, liver, duodenum, pancreas & small bowel
• Mechanisms of Injury
– Compression
• Steering wheel in direct contact with the abdominal & chest wall
– Acceleration-deceleration forces
– Shearing forces
• During energy transfer, rupture of organs at attachment points or where
blood vessels enter the organ

SEAT BELT SIGN

Penetrating Trauma to the Abdomen
• Penetrating Trauma is when a foreign object enters the tissue
• Gunshot wounds, stab wounds and impalements
• GSWs produce a wide variety of wounds depending on bullet velocity
• Bullet has potential to ricochet off bony structures making the trajectory difficult to determine
• Tumbling increases amount of kinetic energy released
• Shotgun shells contain up to 200 small pellets, with each pellet being considered a missile
• GSWs responsible for almost 90% of mortality associated with penetrating trauma
• Most commonly injured organs include small bowel, colon, liver and abdominal vascular structures

PENETRATING ABDOMINAL TRAUMA

• Stab wounds – low velocity, low energy wounds
• Generally a low mortality rate (1-2%)
• Most commonly injured organs from stab wounds include the liver, small bowel, diaphragm and colon
– Many stab wounds do not even penetrate the peritoneum
• Injury can usually be predicted by the trajectory, type of weapon, length of the object & location
• Impalements – MVC, industrial accident, fall, assault or being hit
by a flying object
• Impaled object must be secured and left in place
• Must consider abdominal injury when penetrating chest trauma present

EPIDEMIOLOGY
• Blunt abdominal trauma = 66-75%
– MVC leading cause
• Seat belts can change the patterns of blunt trauma by increasing abdominal injuries from 18% to 40%
• Abdominal trauma associated with 8.5% mortality rate in pediatric population

EPIDEMIOLOGY (Continued)
• Penetrating
– 96%-98% of GSWs are associated with significant intraabdominal
injury
– 30%-40% of SWs are associated with significant intraabdominal
injury
– USA firearm deaths far exceeds all European countries
• Mortality
– 6%-10% of all patients with abdominal trauma die
• Polytrauma may skew this number
– ~ 50% of all OR deaths 1º due to abdominal trauma

PERTINENT HISTORY
• MVC
– Restrained or unrestrained
– Air bag deployment
– Patient’s position in vehicle
– Speed
– Type of collision (frontal, side, rear)
– Status of other passengers
• FALL
– Height

History (Continued)
• PENETRATING
– Time
– Type of weapon (knife, handgun, shotgun)
– Length of knife
– Number of stab wounds or number of shots fired

ASSESSMENT/EVALUATION
• Primary survey
– A – Airway maintenance with cervical spine control
– B – Breathing and Ventilation
– C – Circulation with hemorrhage control
– D – Disability: neurological status
– E – Exposure/environmental control
• Secondary survey
– Lab studies (Hct, WBCs, ABGs & Type and Cross

Physical Exam
• Manifestations of abdominal trauma may be subtle
• Abdomen may sequester large amounts of fluid without apparent distension
• Signs & symptoms associated with abdominal injury are:
– Blood loss
– Abdominal tenderness
– Specific pain patterns
– Absent bowel sounds

Blood Loss and Pain
• Injuries to organs or abdominal blood vessels may lead to extensive hemorrhage
• Spleen & liver are extremely vascular & serve as reservoirs for blood
• Pain, rigidity, guarding or spasms of the abdominal musculature are
classic signs of intra-abdominal pathology
• Sudden movement of irritated peritoneal membranes causes rebound
tenderness & guarding
• Irritation may be due to the presence of free blood or gastric contents
• Release of enzymes from a pancreatic or duodenal injury may lead to a
“chemical peritonitis” which may not appear as a sign & symptom until
several hours after injury
• Referred pain – Kehr’s sign

DIAGNOSTIC TOOLS
• CHEST X-RAY – may reveal lower rib fractures, causing associated injury to the liver or spleen
• ABDOMINAL X-RAY – can identify retroperitoneal free air, gross organ injury or foreign objects
• COMPUTED TOMOGRAPHY (CT)
– In the hemodynamically stable patient
– Source of bleeding can be identified
– ONLY imaging modality capable of evaluating the retroperitoneum
– Can determine the extent/grade of organ injury

Traumatic Splenic Rupture
emedicine.medscape.com

Focused Abdominal Sonography for Trauma (FAST)

FAST
• Rapid, bedside ultrasound examination
• Screen for significant hemoperitoneum or pericardial tamponade
• Directed solely at identifying the presence of free fluid; in trauma usually due to hemorrhage
• Decision making tool to help determine need for transfer to the OR, CT or angiography
• Timely diagnosis of potentially life-threatening hemorrhage

• 4 areas are viewed
– Perihepatic (RUQ)
– Perisplenic (LUQ)
– Pericardium
– Pelvis
• Ultrasound machine immediately available

FAST
cdemcurriculum.org

Positive FAST
cdemcurriculum.org

FAST Pros and Cons
• Pros
– Easily performed at the bedside
– Doesn’t require transfer of hemodynamically unstable patient
– Used concurrently with ongoing assessment
• Cons
– Can’t identify or grade retroperitoneal injuries
– Can’t identify injuries to the bowel or solid organs
– Can’t distinguish whether fluid is ascites or blood

Diagnostic Peritoneal Lavage (DPL)
• Also used to diagnose intraabdominal bleeding in abdominal trauma
• Appropriate tool when the source of blood loss is obscure
• Contraindications include:
• Advanced pregnancy
• Previous multiple abdominal surgeries
• Advanced cirrhosis
• Coagulopathy
• Can make diagnosis of small bowel injury

Technique of DPL
primary-surgery.org

Positive DPL
• Initial aspiration of blood
• (5 – 10 mL or greater)
• Presence of bile, bacteria,
• food particles or fecal
• material
• Presence of lavage fluid
• via Foley or chest tube
unboundedmedicine.com

Exploratory Laparotomy
• Midline incision made in order to examine abdominal organs
• Mandatory for:
– Evisceration of bowel or omentum
– Progressive abdominal distension with unexplained hypotension
– Ruptured diaphragm
– Free air on x-ray
• Indicated for:
– + FAST and hypotension
– + DPL
• Unstable patient (hemodynamically, coagulopathic, acidotic) – goal is damage control; further stabilization in ICU then return to OR at a later time


THERAPEUTIC INTERVENTIONS
• Assure ABCs
• Insert nasogastric/orogastric tube
• Insert Foley catheter – if no contraindications
• Prepare for surgical intervention – prophylactic IV antibiotics
• Consider extra peritoneal injuries

Specific Types of Injuries from Blunt Trauma

SPLEEN
• Most commonly traumatized solid organ in blunt trauma
• Dense organ, located on the left side of the abdomen
• Functions:
– Immune surveillance
– Extracts aged & defective blood
cells & platelets
– Removes debris, foreign matter,
bacteria, viruses & toxins – “blood
cleansing”
– Erythrocyte production in the fetus
– Stores blood platelets
• Rich blood supply (provided by splenic artery & vein)- can cause life threatening hemorrhage
buzzle.com
ispub.com

SYMPTOMS
• Profound bleeding
• Positive Kehr’s sign (pain radiating to L shoulder)
• Localized abdominal pain to the LUQ
• Palpation of mass in left flank area
• Saegesser’s sign (pain in the neck due to irritation of the phrenic nerve)
• Balance’s sign (dullness over left flank)

Diagnosis
• + FAST
• Presence of blood in DPL
• CT abdomen or exploratory laparotomy – definitive diagnosis

CT abdomen showing splenic laceration
emedicine.medscape.com

Intra-op view of splenic laceration
ispub.com

Grading of Splenic Lacerations & Treatment
• GRADE I
– Laceration/tear less than 1
cm deep
– Nonoperative if stable & not
bleeding
• GRADE II
– Laceration 1-3 cm without
vessel involved
– Non-operative if stable &
not bleeding
cdemcurriculum.org
Grading of Splenic Lacerations & Treatment (Continued)
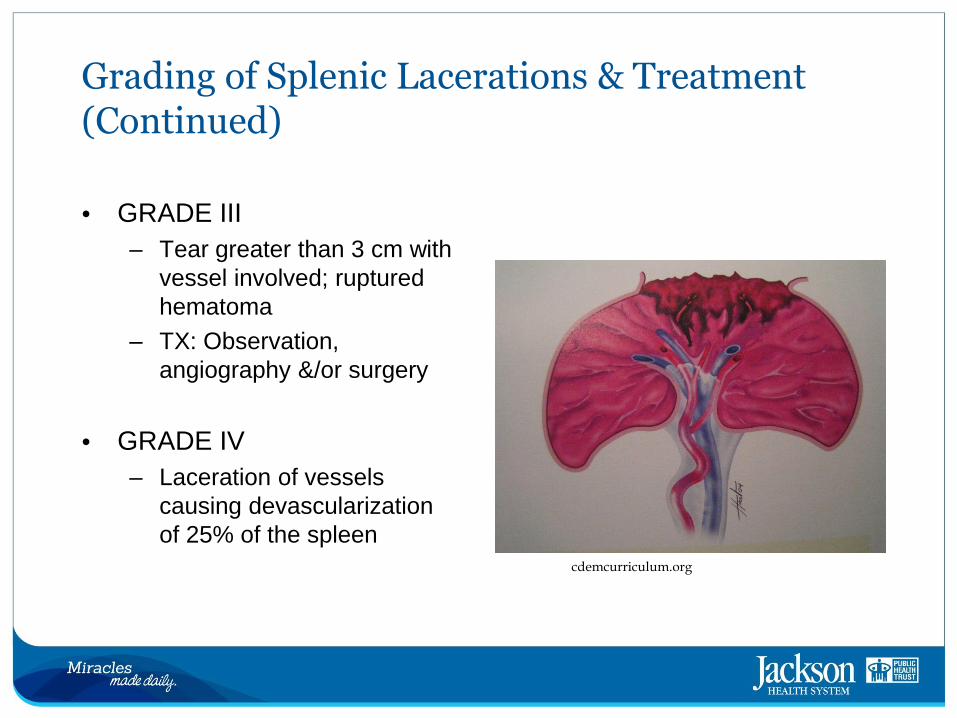
• GRADE III
– Tear greater than 3 cm with
vessel involved; ruptured
hematoma
– TX: Observation,
angiography &/or surgery
• GRADE IV
– Laceration of vessels
causing devascularization
of 25% of the spleen
cdemcurriculum.org

Grading of Splenic Lacerations & Treatment (Continued)
• GRADE V
– Shattered spleen
– Completely devascularized
– TX: Splenectomy
cdemcurriculum.org

Splenic Lacerations
buzzle.com

Classes of Shock
• Nonoperative management in those with isolated splenic injury mandates pt must be hemodynamically stable (Class I & II shock only)
• Class I
– < 15% total blood loss (of total blood volume)
– HR normal or minimally increased
– Normal B/P, mental status and respiratory rate
• Class II
– 15 – 30% blood loss (750 – 1500ml)
– HR > 100, B/P borderline
– Pt anxious
– Respiratory rate 20-30

Classes of Shock (continued)
• Class III
– 30 – 40% blood loss (1500 – 2000 ml)
– HR > 120
– SBP ↓ (80 mm Hg)
– RR 30-40
– Severe anxiety, confused
• Class IV
– > 40% blood loss (> 2000ml)
– HR > 140
– SBP ↓ (60 mm Hg)
– Lethargic to unconscious
– Anuric, Extremities cold, skin ashen to cyanotic

OTHER CONSIDERATIONS
• Effort is made to preserve splenic tissue due to important contributions to
immunocompetence
• Overwhelming postsplenectomy infection (OPSI) has been noted after removal
– Splenic macrophages which filter and phagocytose bacteria removed
– Rare but when does occur, most commonly found in the first 2 years after
splenectomy
– High mortality – more than half die
– Because of this risk, particularly from pneumococcal infection, these
patients should receive the pneumococcal vaccine before discharge & 2
years after
• Monitor for ongoing bleeding
• Other complications: abscess formation & thrombus formation (due to rebound
increases of thrombocytes)
• Should refrain from contact sports for a prescribed period of time
Delayed Splenic Rupture (DSR)
• Occurs through 2 mechanisms:
– Subtle splenic lesion undetected by conventional imagery
• Immediately after the trauma, the spleen may appear normal as the
hemorrhage is contained within the splenic parenchyma
– False negative CT
• Streak artifact due to ribs, air contrast interface within the stomach,
insufficient IV contrast or inadequately diluted oral contrast
• Crucial to consider DSR in instances of acute anemia or acute
abdominal pain in the presence of recent abdominal trauma, even if the initial CT is negative

LIVER INJURIES
• Most frequently injured organ due to size and location (from both blunt & penetrating)
• Mortality increases with:
– Presence of associated injuries
• Overall mortality rate for polytraumatized patients with liver injury = 10-
15%
– Delay in time from injury to treatment
– Presence of comorbid conditions
• Mortality due to hemorrhage (early) or sepsis (late)
• The friability of liver tissue, the extensive blood supply, and the blood storage capacity cause hepatic injury to result in profuse hemorrhage

LIVER INJURIES (continued)
• Bile production
• Conversion of excess glucose into glycogen for storage
• Regulates blood clotting (during gestation, liver forms blood in place of bone
marrow)
• Filters blood (bacteria, drugs, toxins)
• Conversion of ammonia to urea
McGraw-Hill Companies

LIVER INJURIES (continued)
• SIGNS
– Tenderness over right lower ribs or RUQ
– Dullness to percussion
– Signs of peritoneal irritation
– Increased abdominal girth
• DIAGNOSIS
– FAST/DPL
– CT SCAN (if hemodynamically stable)
– E-lap

Grading of Liver Hematomas & Lacerations

AVULSION

MANAGEMENT AND NURSING INTERVENTIONS
• Majority of Grade I to III managed nonoperatively (in hemodynamically stable)
– Monitor blood pressure, heart rate & urine output
– ACC & coagulation studies every 4 to 6 hours
– Monitor for increased abd distension, guarding to RUQ or increase
in pain
• Monitoring for an increase in peritoneal signs
– Assess neurological status
– Surgical intervention may be needed if there is evidence of
continued bleeding, sepsis or deterioration in liver function

• Larger injuries generally require surgical intervention to control bleeding and remove nonviable tissue
• If bleeding cannot be controlled in the OR, the abdomen may be packed with laparotomy pads
• Removal of pads & surgical repair performed 1 – 2 days later after hemostasis achieved
• ICU team:
• Monitor B/P, HR, urine output
• ACC, PT/PTT as ordered
• Transfuse needed blood products (PRBCs, FFP, Plts, cryo)
• Correct acidosis
• Warm patient
• Monitor amount & color of drainage from indwelling JPs
• Always be prepared to return patient to surgery

OPEN ABDOMEN DRESSING

Open Abdomen Without Dressing

COMPLICATIONS FOLLOWING LIVER INJURY/SURGERY
• Major complication = abscess formation
– Develops due to blood, bile, necrotic tissue or foreign material left
at site of injury
– Monitor for early signs of infection, including fever and increased
WBCs
– Can be drained by CT guided catheter placement
• Other complications:
• Sepsis and ARDS
• Postop hemorrhage
• Jaundice

PANCREATIC INJURY
• Injury from blunt trauma is relatively uncommon due to its protective placement in the posterior upper abdomen
• Represents 2% to 3% of all instances of significant abdominal trauma
• Most often caused by penetrating

ANATOMY & FUNCTION
• Retroperitoneal
• Endocrine – produces hormones (insulin, glucagon, etc)
• Exocrine -- secretes digestive enzymes (pancreatic amylase,
trypsin, etc)
becomehealthynow.com
DIAGNOSIS
• Difficult to diagnose as there are no immediate signs of injury
• Many patients have associated injuries which lead to + FAST/+
DPL → E-lap & diagnosis
• CT scan

NURSING INTERVENTIONS
• Monitor B/P, HR, urine output
– Can become hypovolemic due to hemorrhage
• Monitor serum electrolytes
– Pancreatitis can develop in these patients; particularly at risk for
hypocalcemia; Potassium, magnesium, sodium and chloride losses
should be considered due to vomiting or gastric suction
• Evaluate for acidosis/alkalosis
• Monitor for hypoglycemia/hyperglycemia
• Adequate pain control

COMPLICATIONS
• Minor injury – may suture and place drains
– Drains remain for 8 – 10 days or until patient tolerates feeding
without pain/vomiting
• Major injury – debridement and resection
• Complications:
– Hemorrhage
– Abscess formation (CT guided drainage)
– Pancreatic fistula (When controlled by drainage, close with time
and adequate nutrition)
– Pancreatitis

GASTRIC AND ESOPHAGEAL INJURIES
• Blunt injury to the stomach is rare
– May be more common in children due to the elasticity of the
anterior abdominal wall
• Cervical region of esophagus most commonly injured
• More commonly caused by penetrating trauma
• Stomach – most common sign is blood in the NG aspirate
• Look for tenderness & signs of peritonitis with free air on
abdominal x-ray
– Signs and symptoms related to the chemical irritation of nearby
tissues by highly acidic gastric contents

SMALL BOWEL INJURIES
• Blunt hollow injuries occur in
less than 1% of trauma patients
• Small bowel injuries often
related to shoulder harness
and lap belt devices; small intestine crushed between an
external force & vertebral
column
• Duodenal hematomas due to
handlebar
• Classic case of child falls off
bike and strikes abdomen on
end of handlebar

SMALL BOWEL
• Clinical signs & symptoms may develop slowly & be overshadowed by other injuries
• Peritoneal irritation manifested by abdominal wall muscle rigidity, spasm, involuntary guarding, rebound tenderness or pain
• Presence of Chance fracture (transverse fx of lower thoracic or lumbar vertebral body) raises index of suspicion
• + DPL will show presence of bile, feces or food fibers
• E-lap (explore full length of bowel)

MANAGEMENT
• Stomach – debridement of devitalized tissue and closure with sutures; partial gastrectomy may be indicated
• Small bowel – simple closure using sutures; more complex injuries managed with debridement or resection

POST-OP NURSING INTERVENTIONS
• Monitor closely for fluid volume deficit & electrolyte abnormalities
• If peritoneum contaminated, antibiotic administration and infection surveillance are recommended
• Monitor respiratory status with effective pain management and aggressive pulmonary toilet
• Nutritional support
COMPLICATIONS
• Breakdown of the anastomosis
• Peritonitis
• Bowel ischemia with necrosis
• Bowel obstruction
• Abscess formation
• Wound dehiscence

REFERENCES
• Bala, M., Avraham, I, Gideon, Z., Tal, H., Iryna, G., Yoav, M., Pikarsky, A., Amar, A., Shussman, N., Abu Gazala., M & Almogy,
G. (2008). Abdominal Trauma After Terrorist Bombing Attacks Exhibits a Unique Pattern of Injury. Annals of Surgery, 248(2), 303-
309.
• Civetta, J., Kirton, O., McKenney, M. and Shatz, D. (2000). Manual of Trauma and Emergency Surgery. 1st Ed. W.B. Saunders
Company
• Schnuriger, B., Inderbitzin, D., Schafer, M., Kickuth, R., Exadaktylos, A and Candinas, D. (2009). Concomitant Injuries are an
Important Determinant of Outcome of High-grade Blunt Hepatic Trauma. British Journal of Surgery, 96, 104-110.
• El-Osta, H. & Salyers, W. (2009). Delayed Splenic Rupture: Myth or Reality. Annals of Internal Medicine, 150(3), 224-225.
• Gamblin, T., Wall, C., Royer, G., Dalton, M & Ashley, D. (2005). Delayed Splenic Rupture: Case Reports and Review of the
Literature, The Journal of Trauma. 59(5), 1231-1234.
• Kinney, M., Dunbar, S., Brooks-Brunn, J., Molter, N., Vitello-Cicciu, J. (1998). AACN’s Clinical Reference for Critical Care
Nursing. 4th Ed. Mosby
• London, J., Parry, L., Galante, J. & Battistella, F. (2008). Safety of Early Mobilization of Patients With Blunt Solid Organ Injuries.
Archives of Surgery, 143(10), 972-976.
• McCray, V., Davis, J., Lemaster, D. & Parks, S. (2008). Observation For Nonoperative Management of the Spleen: How Long is
Long Enough? Journal of Trauma, 65(6), 1354-1358.
• Newland, A., Provan, D., & Myint, S. (2005). Preventing Severe Infection After Splenectomy. Retrieved March 5, 2009 from
http://www.bmj.com/cgi/content/full/331/7514/417
• Trauma Nursing Core Course. (2011). Emergency Nurses Association, 6th Ed.
• Sheehy, S., Blansfield, J., Danis, D. and Gervasini, A. (1999). Manual of Clinical Trauma Care: The First Hour. 3rd Ed. Mosby
• United States Marine Corp. (2008). Manage Shock Casualties FMST Student Manual. Retrieved March 5, 2009 from
http://www.operationalmedicine.org/TextbookFiles/FMST_20008/FMST_1401.htm
• Wiesley, B. (March 14, 2006). Abdominal Trauma.
• Retrieved on February 1, 2009 from www.aanet.org

Natasha Pollard, RN, BS
November 2013