abc of general surgery in children acute abdominal pain in
TRANSCRIPT
ABC of General Surgery in Children
ACUTE ABDOMINAL PAIN IN CHILDREN
Mark Davenport
Principles of diagnosis
-*.....Ah with acute abdominal pain can be a disconcerting experiencefor most doctors, and there is often little in the way of aids or
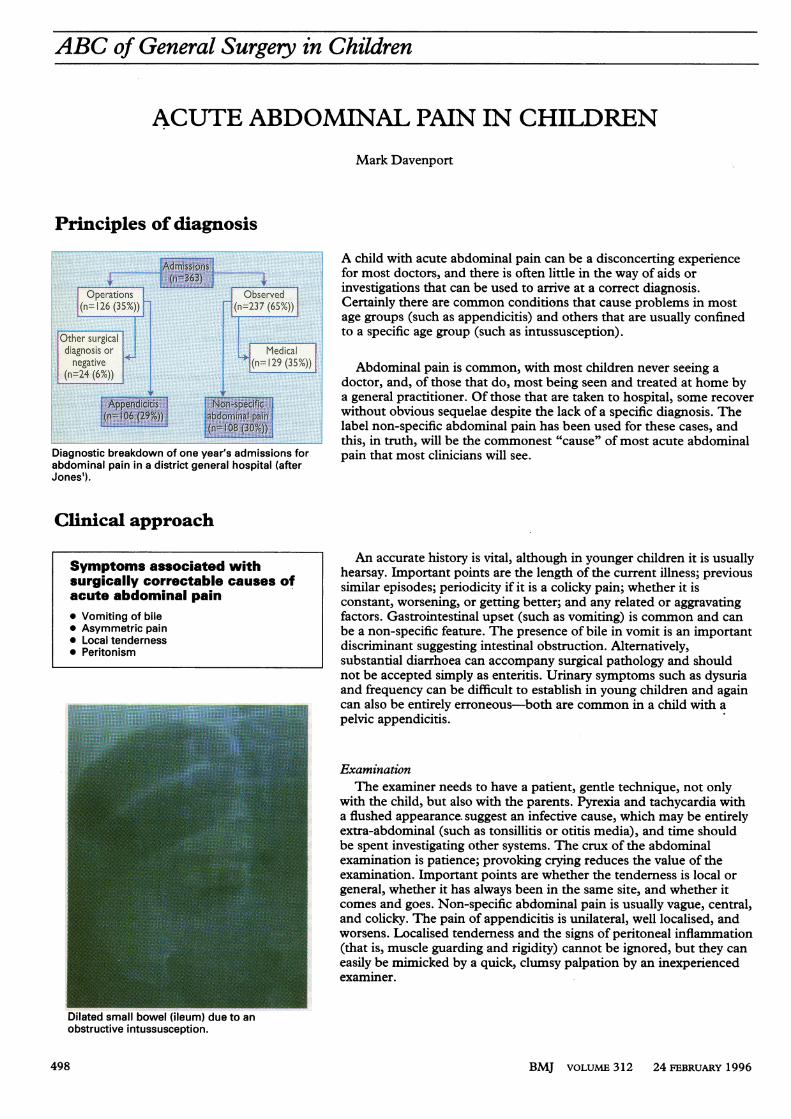
Operation Observed ~~investigations that can be used to arrive at a correct diagnosis.m(n=126 (35X)) 7 : (n=237 (65%)) m Certainly there are common conditions that cause problems in most
age groups (such as appendicitis) and others that are usually confined~~~~~~~toa specific age group (such as intussusception).
doctor, and, of those that do, most being seen and treated at home bya general practitioner. Of those that are taken to hospital, some recoverwithout obvious sequelae despite the lack of a specific diagnosis. Thelabel non-specific abdominal pain has been used for these cases, andthis, in truth, will be the commonest "cause" of most acute abdominal
Diagnostic breakdown of one year's admissions for pain that most clinicians will see.abdominal pain in a district general hospital (afterJones').
Clinical approach
Symptomsassociatedwith An accurate history is vital, although in younger children it is usuallySymptoms associated with | hearsay. Important points are the length of the current illness; previoussurgically correctable causes of similar episodes; periodicity if it is a colicky pain; whether it isacute abdominal pain constant, worsening, or getting better; and any related or aggravating* Vomiting of bile factors. Gastrointestinal upset (such as vomiting) is common and can* Asymmetric pain be a non-specific feature. The presence of bile in vomit is an important* Local tenderness discriminant suggesting intestinal obstruction. Alternatively,______Peritonism ____________________ substantial diarrhoea can accompany surgical pathology and should
not be accepted simply as enteritis. Urinary symptoms such as dysuriaand frequency can be difficult to establish in young children and againcan also be entirely erroneous-both are common in a child with a
......... ! pelvic appendicitis.
ExaminationThe examiner needs to have a patient, gentle technique, not only
with the child, but also with the parents. Pyrexia and tachycardia witha flushed appearance. suggest an infective cause, which may be entirelyextra-abdominal (such as tonsillitis or otitis media), and time shouldbe spent investigating other systems. The crux of the abdominalexamination is patience; provoking crying reduces the value of theexamination. Important points are whether the tenderness is local orgeneral, whether it has always been in the same site, and whether itcomes and goes. Non-specific abdominal pain is usually vague, central,and colicky. The pain of appendicitis is unilateral, well localised, andworsens. Localised tenderness and the signs of peritoneal inflammation(that is, muscle guarding and rigidity) cannot be ignored, but they caneasily be mimicked by a quick, clumsy palpation by an inexperiencedexaminer.
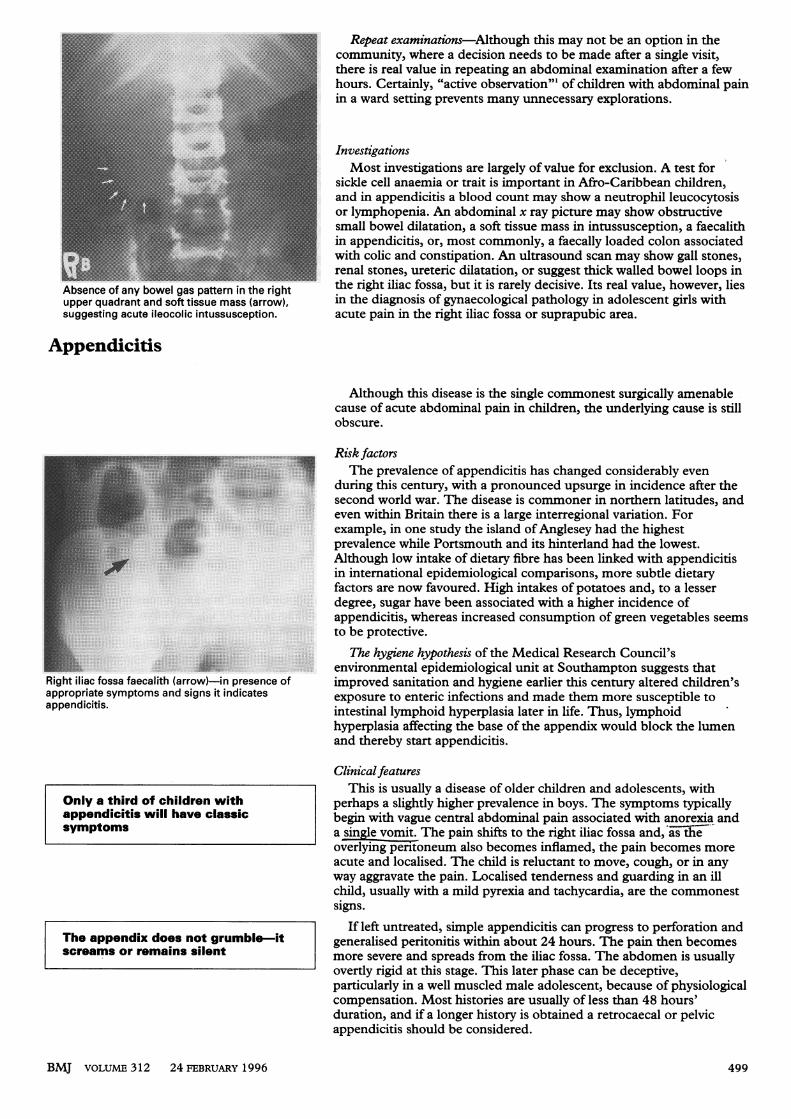
Dilated small bowel (ileum) cobstructive intussusception.
BMJ voLUME 312 24 FEBRUARY 1996498
-- :. ......Repeat examinations-Although this may not be an option in the
communty, where a decision needs to be made after a single visit,
_ lg;0=:; i d _ ~~~~hours. Certainly, "activeobsrain'o children with abdominal pain
_ | | _ ; : - ~~~~~in
~~ l w _i ><- i - _ ~~Investigations
I C ........ ..:_ ....Most..........--.sicke
_1M11 l '. -- :: ..............................~~~~~~~~~~~................ N:l..............__.and
- 1 _: ~~~~~~~~orlymphopenia. An. abdominal x ray picture may show obstructive
theresmall bel edilatation, mass in tussusception, afaecalith
hourenal stones, ureteric dilatation,aorue thick walled bowel loops in
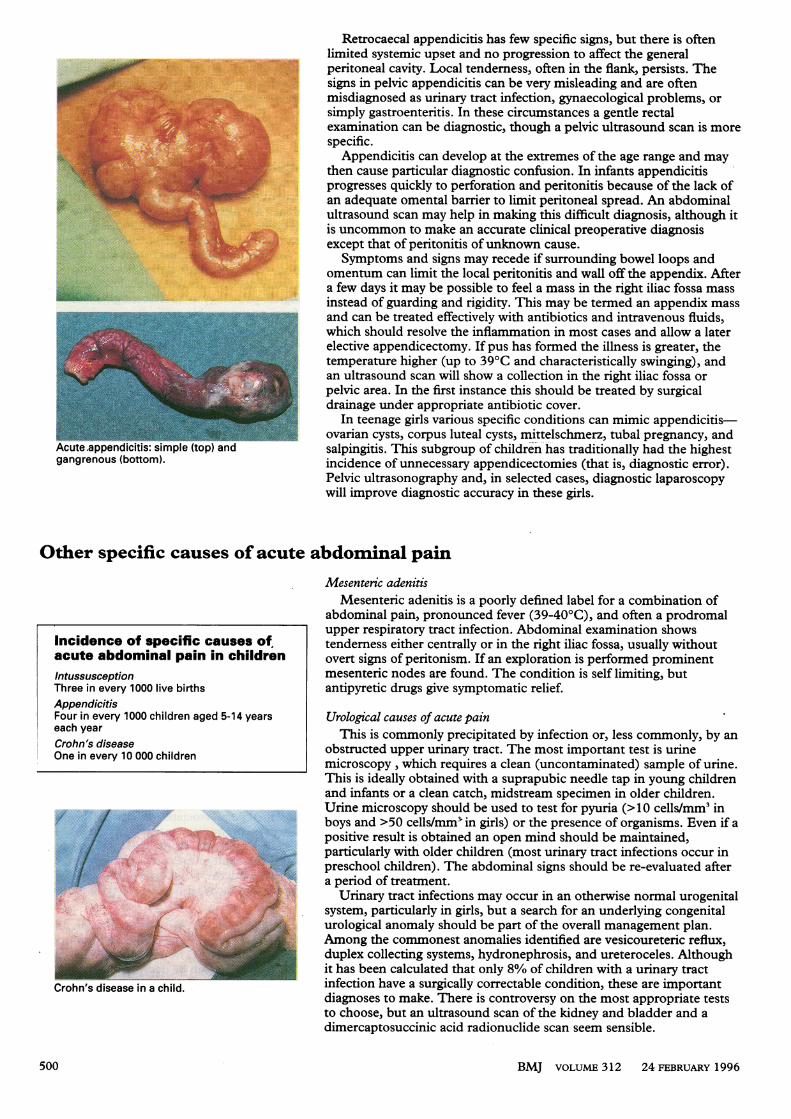
Absence of any bowel gas pattern in the righ the right iliac fossa, but it iS rarely decisive. Its real value, however, lies
upper quadrant and soft tissue mass (arrow), in the diagnosis of gynaecological pathology in adolescent girls with
suggesting acute ileocolic intussusception. acute pain in the right iliac fossa or suprapubic area.
Appendicitis
Although this disease is the single commonest surgically amenable
cause of acute abdominal pain in children, the underlying cause is still
obscure.
Risk factors
_ W ~~~~~~~~~~~Theprevalence of appendicitis has changed considerably even
_ -X5~~~~~~~~~during
__ _ E X ~~~~~~~~secondworld war. The disease is commoner in northern latitudes, and
_ ; rX~~~~~~~~~evenS ;~~~~~~~~~~example,
....... in_prevalence while Portsmouth and its hinterland had the lowest.
_ r; -3g_FF ~~~~~~~Although low intake of dietary fibre has been linked with appendicitis
In international epidemiological comparisons, more subtle dietary
t factors are now favoured. High intakes of potatoes and, to a lessersickldegree, sugar have been associated with a higher incidence of
appendictis, whereas increased consumption of green vegetables seems
to be protective.i appendiciti,Thehygiene hypothesis ofmthe Medical Research Council's
renvironmental epidemiological unit at Southampton suggests that
Right iliac fossa faecalith (arrow) in presence of improved sanitation and hygiene earlier this century altered children's
appropriate symptoms and signs it indicates exposure to enteric infections and made them more susceptible to
appendicitis. intestinal lymphoid hyperplasia later in life. Thus, lymphoid
hyperplasia affecting the base of the appendix would block the lumen
and thereby start appendicitis.
Only a third of children withappendicitis will have classicsymptoms
ClinicalfeaturesThis is usually a disease of older children and adolescents, with
perhaps a slightly higher prevalence in boys. The symptoms typicallybegin with vague central abdominal pain associated with anorexia anda single vomit. The pain shifts to the right iliac fossa and, asthieoverlying peritoneum also becomes inflamed, the pain becomes moreacute and localised. The child is reluctant to move, cough, or in anyway aggravate the pain. Localised tenderness and guarding in an illchild, usually with a mild pyrexia and tachycardia, are the commonestsigns.
If left untreated, simple appendicitis can progress to perforation andgeneralised peritonitis within about 24 hours. The pain then becomesmore severe and spreads from the iliac fossa. The abdomen is usuallyovertly rigid at this stage. This later phase can be deceptive,particularly in a well muscled male adolescent, because of physiologicalcompensation. Most histories are usually of less than 48 hours'duration, and if a longer history is obtained a retrocaecal or pelvicappendicitis should be considered.
BMJ VOLUME 312 24 FEBRUARY 1996
The appendix does not grumble-itscreams or remains silent
499
Retrocaecal appendicitis has few specific signs, but there is oftenlimited systemic upset and no progression to affect the generalperitoneal cavity. Local tenderness, often in the flank, persists. The
E ,,''.'signsin pelvic appendicitis can be very misleading and are oftenmisdiagnosed as urinary tract infection, gynaecological problems, orSimply gastroenteritis. In these circumstances a gentle rectalexamination can be diagnostic, though a pelvic ultrasound scan is morespecific.
Appendicitis can develop at the extremes of the age range and maythen cause particular diagnostic confusion. In infants appendicitisprogresses quickly to perforation and peritonitis because of the lack ofan adequate omental barrier to limit peritoneal spread. An abdominalultrasound scan may help in making this difficult diagnosis, although itis uncommon to make an accurate clinical preoperative diagnosisexcept that of peritonitis of unknown cause.Symptoms and signs may recede if surrounding bowel loops and
omentum can limit the local peritonitis and wall off the appendix. Aftera few days it may be possible to feel a mass in the right iliac fossa massinstead of guarding and rigidity. This may be termed an appendix massand can be treated effectively with antibiotics and intravenous fluids,which should resolve the inflammation in most cases and allow a laterelective appendicectomy. If pus has formed the illness is greater, thetemperature higher (up to 39°C and characteristically swinging), andan ultrasound scan will show a collection in the right iliac fossa orpelvic area. In the first instance this should be treated by surgicaldrainage under appropriate antibiotic cover.
In teenage girls various specific conditions can mimic appendicitis-ovarian cysts, corpus luteal cysts, mittelschmerz, tubal pregnancy, and
Acute-appendicitis: simple (top) and salpingitis. This subgroup of children has traditionally had the highestgangrenous (bottom). incidence of unnecessary appendicectomies (that is, diagnostic error).
Pelvic ultrasonography and, in selected cases, diagnostic laparoscopywill improve diagnostic accuracy in these girls.
Other specific causes of acute abdominal painMesenteric adenitis
Incidence of specific causes ofacute abdominal pain in childrenIntussusceptionThree in every 1000 live birthsAppendicitisFour in every 1000 children aged 5-14 yearseach yearCrohn's diseaseOne in every 10 000 children
Crohn's disease in a child.
Mesenteric adenitis is a poorly defined label for a combination ofabdominal pain, pronounced fever (39-40°C), and often a prodromalupper respiratory tract infection. Abdominal examination showstendemess either centrally or in the right iliac fossa, usually withoutovert signs of peritonism. If an exploration is performed prominentmesenteric nodes are found. The condition is self limiting, butantipyretic drugs give symptomatic relief.
Urological causes of acute painThis is commonly precipitated by infection or, less commonly, by an
obstructed upper urinary tract. The most important test is urinemicroscopy, which requires a clean (uncontaminated) sample of urine.This is ideally obtained with a suprapubic needle tap in young childrenand infants or a clean catch, midstream specimen in older children.Urine microscopy should be used to test for pyuria (> 10 cells/mm' inboys and >50 cells/mm' in girls) or the presence of organisms. Even if apositive result is obtained an open mind should be maintained,particularly with older children (most urinary tract infections occur inpreschool children). The abdominal signs should be re-evaluated aftera period of treatment.
Urinary tract infections may occur in an otherwise normal urogenitalsystem, particularly in girls, but a search for an underlying congenitalurological anomaly should be part of the overall management plan.Among the commonest anomalies identified are vesicoureteric reflux,duplex collecting systems, hydronephrosis, and ureteroceles. Althoughit has been calculated that only 8% of children with a urinary tractinfection have a surgically correctable condition, these are importantdiagnoses to make. There is controversy on the most appropriate teststo choose, but an ultrasound scan of the kidney and bladder and adimercaptosuccinic acid radionuclide scan seem sensible.
BMJ VOLUME 312 24FEBRUARY 1996500

Causes of acute abdominal pain in childrenCommon causes* Appenticitis * Non-specific abdominal painUncommon causesMeckel's diverticulitis, mesenteric adenitis, Crohn's disease, sickle cellcrisis, gall stones, pancreatitis, tonsillitis, otitis media, acute hapatitis, acuteporphyria, intestinal bands, malrotation, ureteric calculi, urinary tractinfection, pneumonia, peptic ulcer disease, psychogenic, Henoch-Schonleinpurpura, intussusception, yersinia infection, obstructed inguinal hernia,torsion of testicle, omental infarction, renal vein thrombosis, acutehydronephrosis, primary peritonitis, salpingitis, ovarian cyst, ectopic tubalpregnancy, pyelonephritis, trauma, infective gastroenteritis, foodpoisoning, child abuse, attention seeking behaviour, intestinal volvulus,choledochal cyst, cholangitis, foreign body, adhesions and small bowelobstruction, pica, ketoacidosis
1 Jones PF. Active observation in management of acute abdominal pain in childhood. BMJ 1976;ii:551-3.
Professor Lewis Spitz, Institute of Child Health, London, provided the pictures of faecalith,gangrenous appendicitis, and Crohn's disease.
Renal and ureteric calculi, though rare, area potent cause of acute abdominal pain, withmost being associated with chronic urinaryinfection. Children with neurogenic bladders(for instance, those with spina bifida) areprone to develop this problem.
Upper abdominalpainAcute upper abdominal pain is much less
common in children than in adults, but if itoccurs in older children, and particularly if itis recurrent, thought should be given to gallstones (especially in children with chronichaemolysis, such as sickle cell anaemia),peptic ulcers, and pancreatitis (oftenassociated with a choledochal cyst).
The ABC ofPaediatric Surgery is edited by MarkDavenport, consultant paediatric surgeon, department ofpaediatric surgery, King's College Hospital, London.
Department ofPaediatrics,Chinese University ofHongKong, 6/F Clinical SciencesBuilding, Prince ofWalesHospital, Shatin, HongKongA Mok, medical officerE A S Nelson, lecturer inpaediatrics
Correspondence to:Dr Nelson.
BMJ 1996;312:501-4
Children on hunger strike: child abuse or legitimate protest?
A Mok, E A S Nelson
The issue of children on hunger strike (voluntarytotal fasting) has not been reported before. TheWorld Medical Association Declaration of Tokyo1975 and the Declaration of Malta 1991 (revised1992) provide clinicians with guidelines for themanagement of adult patients on hunger strike1 2 butdo not mention children. We report the managementof 14 Vietnamese children, aged 1 to 12 years, whotook part in a hunger strike at a refugee detentioncentre in Hong Kong.
The influx of Vietnamese boat people to Hong Kongand other South East Asian countries began in the1970s. Initially all were deemed to be political refugeeswho would be resettled in a third country. This policywas then revised and over 20 000 refugees werereclassified as "economic migrants" for repatriation toVietnam. Some returned under a voluntary repatri-ation programme, but most resisted. Earlier attemptsat forced repatriation were opposed by the UnitedStates Administration. A resumption of forcedrepatriation, together with a possible reversal ofUnited States policy, was reported in the local media inSeptember 1994.3 This resulted in the north section ofthe High Island Detention Centre (population 1500)embarking on a hunger strike. Everyone in thissection, including children, fasted or were fasted, forup to five days. Only water was taken orally. Breastfeeding was allowed, although mothers were expectedto fast.
The hunger strikeSixty seven hunger strikers made 93 attendances to
the camp sick bay during this period. Fifty seven of theattendees were children under the age of 15 years(fig 1). Attendees were assessed, given treatment forminor complaints, and offered food and oral re-hydration fluid. Parents were advised of their respon-sibility to feed their children and of the clinicalconsequences ofwithholding food.
Fourteen children were transferred from the campsick bay to the Prince of Wales Hospital. No parentsobjected. The youngest "hunger striker" was less than
98 Sick bay (n=57)
M Hospital (n= 14)| __
6-
U-..5
45
02
2 3 4 5 6 7 8 9 10 11 12 13 14Age (years)
Age distribution ofchildren on hunger strike
2 years old (fig 1). All children had some degree ofketonuria and two were hypoglycaemic. Normal warddiet was offered and no child refused food.
In the absence of guidelines or previous experience,we considered that total fasting of the children was aform of child abuse and we did not discharge' thechildren until we were satisfied that they would be fednormally. Fortunately after five days, before majorlogistical problems developed, the hunger strikestopped.
Parents were interviewed when their children weredischarged. On direct questioning no parents admittedsecretly feeding their children and some indicated thatthere had been coercion. The reasons they gave as towhy they let their child fast included regretting it butthinking it was right; that it had been their child's owndecision to fast; or that they had been forced by theleaders to fast their child. Some older children claimedthat they had begun the hunger strike voluntarilybecause their parents and everyone else were fasting,and they believed that such action might have pre-vented them from being sent back to Vietnam. Parentswere informed that we considered this an unacceptableform of political protest, and we emphasised thepotential adverse effects on their children's health.
DiscussionA hunger striker is defined as a "mentally competent
person who has indicated that he has decided to refuse
BMJ voLuME 312 24 FEBRUARY 1996 501