aace italianchaptercourse 4 current approach to thyroid ... · roma, 7-10 novembre 2019 if131i...
TRANSCRIPT

Roma, 7-10 novembre 2019
AACE Italian Chapter Course 4Current approach to thyroid dysfunction
CURRENT MANAGEMENT OF GRAVES’ DISEASE
Jeffrey Garber (USA) & Massimo Salvatori 1. Real clinical practice (Andrea Frasoldati) 2. Natural history and long-term clinical consequences (Laszlo Hegedus, DK) 3. Efficacy and limits of treatment options: •• Medical treatment (Hossein Gharib, USA) •• Radioiodine treatment (Maurilio Deandrea) •• Surgery (Celestino Pio Lombardi) 4. THM (Andrea Frasoldati)
Roma, 7-10 novembre 2019
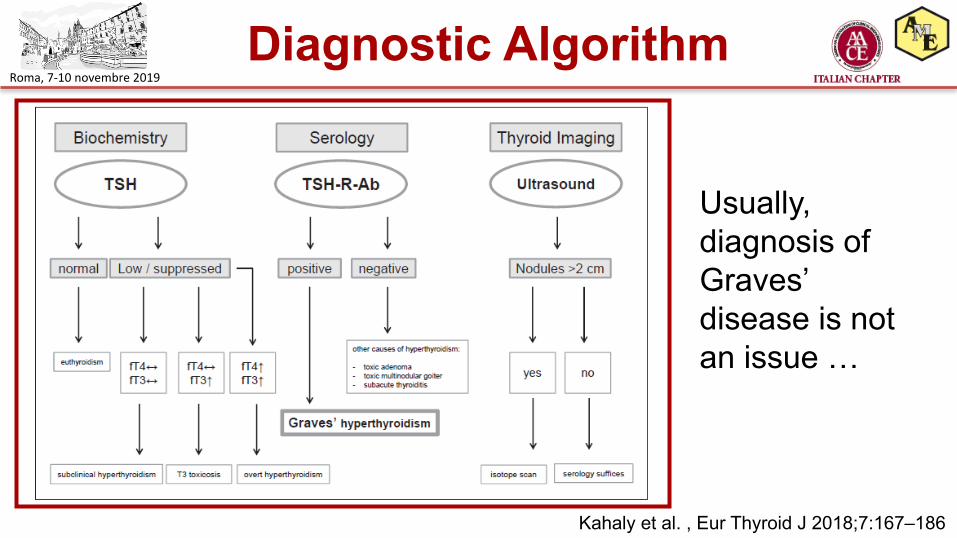
Diagnostic Algorithm
Kahaly et al. , Eur Thyroid J 2018;7:167–186
Usually, diagnosis of Graves’ disease is notan issue …
Roma, 7-10 novembre 2019
• Matteo, 16 year old volley ball player. Euthyroidism fully restored, but “thyroid inferno” on US and initial mild GO.
Case 1 - Matteo
Which treament?
•ATD•Surgery•131I
Roma, 7-10 novembre 2019
Case 2 - Sara
• Sara, 36 year old, hairdresser. Graves’ recurrence. Hyperthyroidism well controlled. She is planning a pregnancy
Which treament?
•ATD•Surgery•131I
Roma, 7-10 novembre 2019
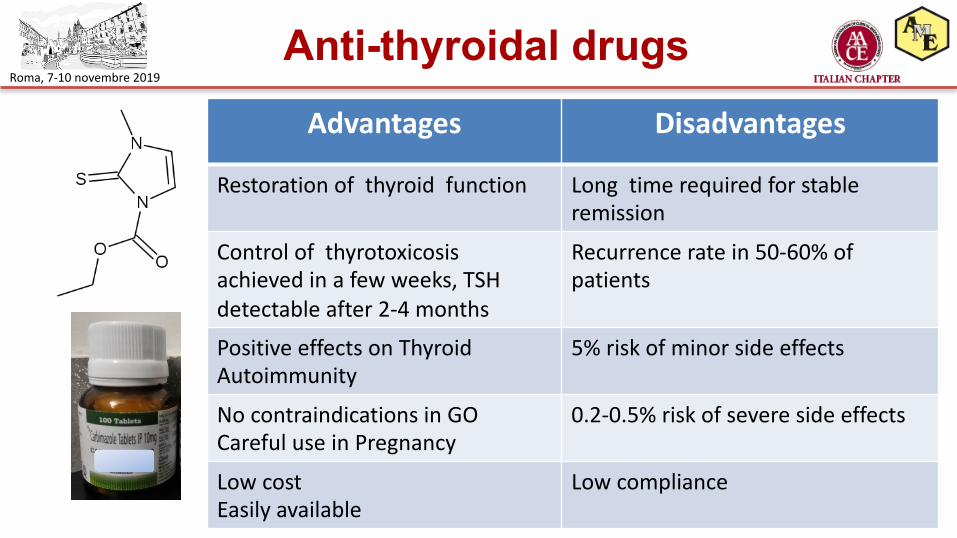
Anti-thyroidal drugsAdvantages Disadvantages
Restoration of thyroid function Long time required for stableremission
Control of thyrotoxicosisachieved in a few weeks, TSH detectable after 2-4 months
Recurrence rate in 50-60% ofpatients
Positive effects on ThyroidAutoimmunity
5% risk of minor side effects
No contraindications in GOCareful use in Pregnancy
0.2-0.5% risk of severe side effects
Low costEasily available
Low compliance
Roma, 7-10 novembre 2019
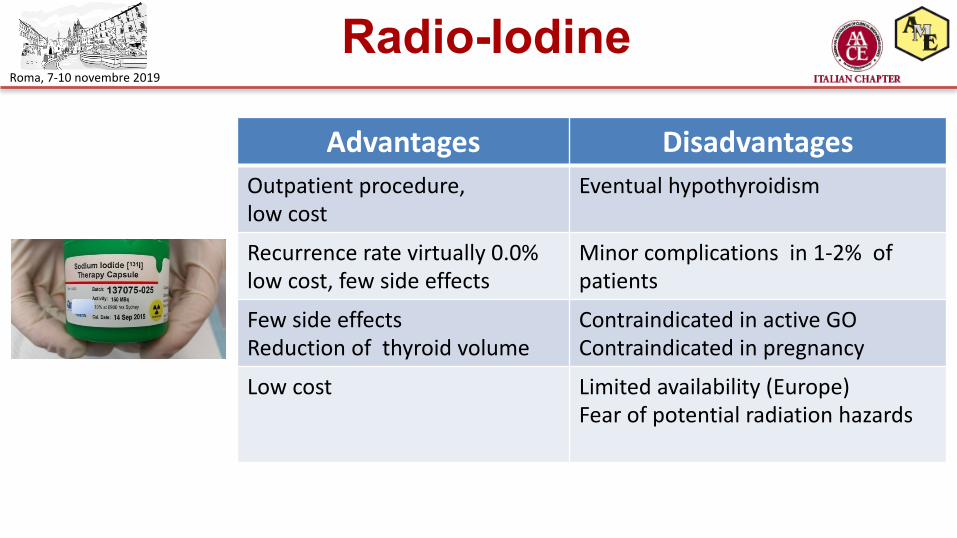
Radio-Iodine
Advantages DisadvantagesOutpatient procedure, low cost
Eventual hypothyroidism
Recurrence rate virtually 0.0% low cost, few side effects
Minor complications in 1-2% ofpatients
Few side effectsReduction of thyroid volume
Contraindicated in active GOContraindicated in pregnancy
Low cost Limited availability (Europe) Fear of potential radiation hazards
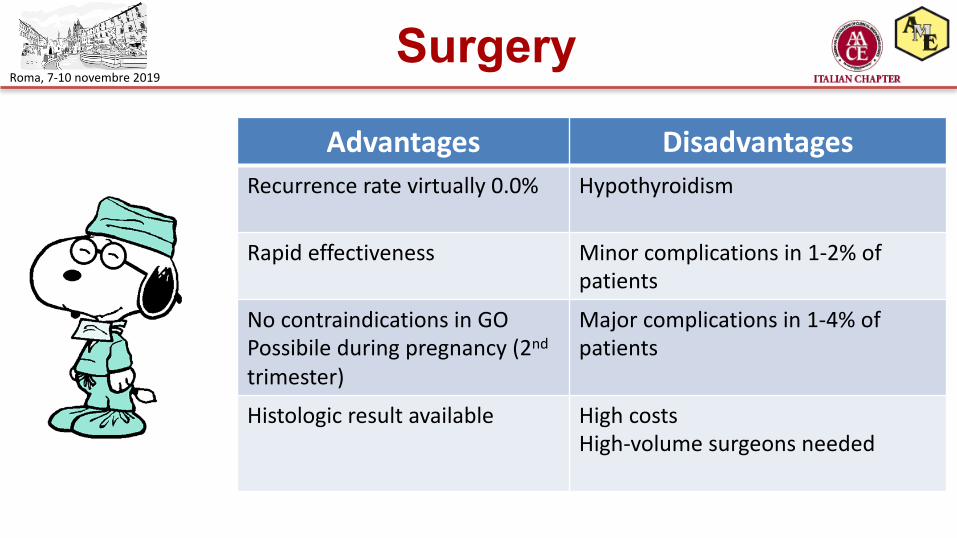
Roma, 7-10 novembre 2019Surgery
Advantages DisadvantagesRecurrence rate virtually 0.0% Hypothyroidism
Rapid effectiveness Minor complications in 1-2% of patients
No contraindications in GOPossibile during pregnancy (2nd
trimester)
Major complications in 1-4% ofpatients
Histologic result available High costsHigh-volume surgeons needed
Roma, 7-10 novembre 2019
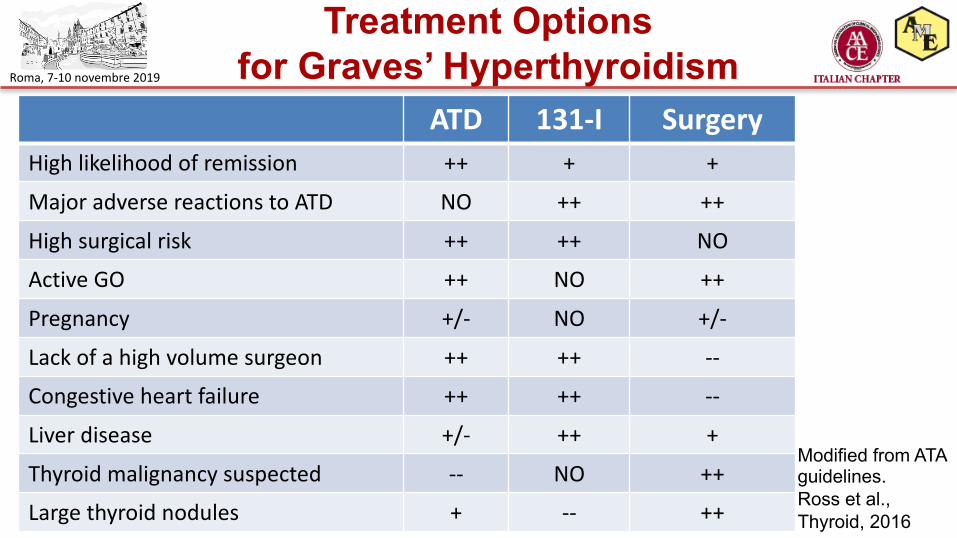
Treatment Optionsfor Graves’ Hyperthyroidism
ATD 131-I SurgeryHigh likelihood of remission ++ + +
Major adverse reactions to ATD NO ++ ++
High surgical risk ++ ++ NO
Active GO ++ NO ++
Pregnancy +/- NO +/-
Lack of a high volume surgeon ++ ++ --
Congestive heart failure ++ ++ --
Liver disease +/- ++ +
Thyroid malignancy suspected -- NO ++
Large thyroid nodules + -- ++
Modified from ATA guidelines. Ross et al., Thyroid, 2016

Roma, 7-10 novembre 2019
Management Algorithm
Kahaly et al. , Eur Thyroid J 2018;7:167–186
Roma, 7-10 novembre 2019
ATD as the first option
• Patients with newly diagnosed Graves’ hyperthyroidismshould be treated with ATD. RAI therapy or thyroidectomymay be considered in selected patients.
• MMI (CBZ) should be preferentially used in non-pregnantpatient. MMI is usually administered for 12–18 monthsthen discontinued if the TSH and TSH-R-Ab levels arenormal.
• Measurement of TSH-R-Ab levels prior to stopping ATDtherapy is recommended.
Adapted from Kahaly et al. , Eur Thyroid J 2018;7:167–186
Roma, 7-10 novembre 2019
Before startingantithyroid drugs
• If the chance of remission is low, Tx or RAI might be a betteroption.
• Factors associated with a low remission rate as suggested inmany but not all studies, are male sex, young age (<40 years),smoking, severe hyperthyroidism, highTBII, large goiter size,and the presence of GO.
• The predictive value of each of these risk factors is too low foraccurate assessment of the remission chance before startingATD in the individual patient …
Wiersinga et al. Endocrinol Metab 2019;34:29-38
Roma, 7-10 novembre 2019
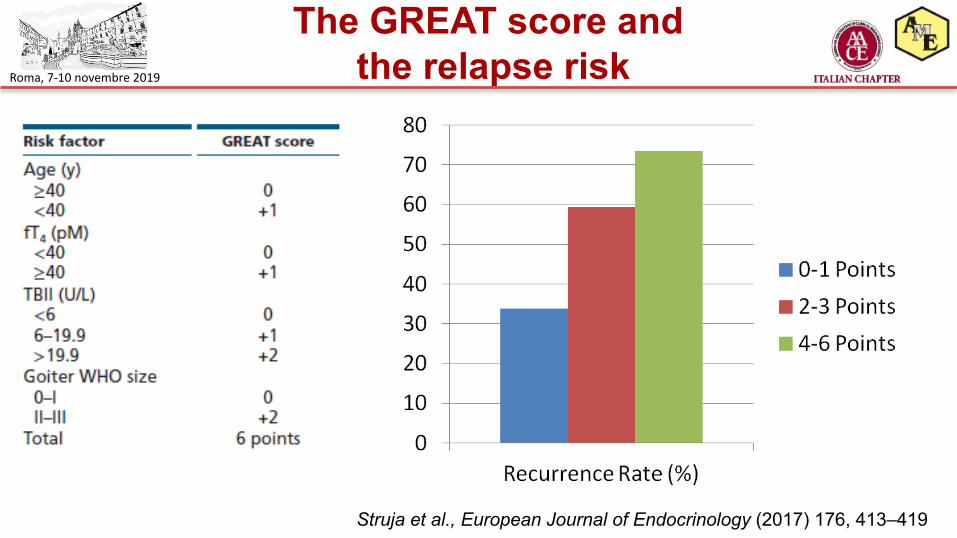
The GREAT score andthe relapse risk
Struja et al., European Journal of Endocrinology (2017) 176, 413–419

Roma, 7-10 novembre 2019If 131I is the chosen option …
• Often recommended for patients with side-effects to ATD or in case of disease recurrence.
• ATD should be stopped around 1 week before and after therapy.
• A fixed dose of RAI can usually be administered.• Patients should be informed that repeated doses may be
needed.• Conception should be postponed until at least 6 months
after RAI in both males and females.Adapted from Kahaly et al., Eur Thyroid J 2018;7:167–186
Roma, 7-10 novembre 2019
When surgery is selected …
• Total thyroidectomy is the procedure of choice, andshould be performed by a skilled “high-volume” surgeon.
• Euthyroidism should be restored by ATD prior to surgery.
• A solution containing potassium iodide can be given for 10 days prior to surgery.
Adapted from Kahaly et al. , Eur Thyroid J 2018;7:167–186
Roma, 7-10 novembre 2019
Implication for research• More long-term, high-quality randomized controlled clinical trials
comparing radioiodine with antithyroid medications for Graves diseaseare required. Data for children are lacking.
• Future trials should include all-cause mortality, health-related qualityof life, socioeconomic effects and information on bone mineral density,as well as data on co-medications to treat Graves’ ophthalmopathysuch as steroids.
• No long-term data exist on other antithyroid medications such aspropylthiouracil for the treatment of Graves’ disease.
Ma et al., Radioiodine therapy versus antithyroidmedications for Graves’ disease . Cochrane Database of Systematic Reviews 2016
Roma, 7-10 novembre 2019
THMs: the final cut
THANK YOU FOR YOUR ATTENTION!