a time for change: what is the future for successful ... · national center for chronic disease...
TRANSCRIPT
10/4/11
1
National Center for Chronic Disease Prevention and Health Promotion
Division of Cancer Prevention and Control
T’Ronda Joseph, MPA, MCHES Public Health Advisor, Program Services Branch
Division of Cancer Prevention and Control National Center for Chronic Disease Prevention & Health
Promotion Centers for Disease Control and Prevention
A Time for Change: What is the Future for
Successful Chronic Disease Prevention?
Presentation Outline
CDC
Public Health Priorities
THEMES

10/4/11
2
CDC 24/7 Saving lives. Protecting people and
communities. Saving money.
• CDC works 24/7 to save lives, protect people and communities from health threats, and save money by prevention
• CDC puts science and prevention into action to make the healthy choice the easy choice
• CDC helps people live longer, healthier, more productive lives with lower health care costs

10/4/11
3
CDC Strategic Directions
• Excellence in surveillance, epidemiology, and laboratory services
• Strengthen support for state, tribal, local, and territorial public health
• Increase global health impact
• Use expertise to advance policies that promote health
• Better prevention of illness, injury, disability, and death
Obesity, Nutrition, Physical Activity and Food Safety
Healthcare- Associated Infections
HIV
Motor Vehicle Injuries
Tobacco
Teen and Unintended Pregnancy
Better prevent illness, injury, disability, and death
Winnable Battles – 6 key areas where public health can have a substantial impact

10/4/11
4
Providers have an important part to play in winnable battles
Tobacco prevention
Question patients about use; offer/refer counseling and cessation; advocate for tobacco control
Nutrition, physical activity, obesity, and food safety
Screen patients for obesity, diabetes, high blood pressure, cholesterol and offer/refer counseling, interventions
Healthcare-associated infections
Implement and track prevention guidelines
Motor vehicle injury prevention
Alcohol brief intervention; seat belt use counseling
Teen pregnancy prevention
Offer/refer counseling and family planning services
HIV prevention Implement routine HIV testing (ages 13-64); prevention with positives; partner services
On ABCS, U.S. gets an F
Aspirin People at increased risk of heart disease who take aspirin
33%
Blood pressure People with hypertension with blood pressure controlled
46%
Cholesterol Peoplewith high cholesterol with hyperlipidemia controlled
33%
Smoking People trying to quit smoking who get help
20%
Despite spending $1 out of every $6 on healthcare

10/4/11
5
What Public Health Can Do q Help win these public health battles
§ Priority issues at the local, state, and federal levels
§ Known, effective, scalable interventions § Potential for large impact on health
q Collective and focused efforts § Identify optimal strategies at all levels, across all
sectors § Rally resources and partnerships § Communicate about successes and challenges
along the way § Accelerate efforts to make measureable impact
on health
www.cdc.gov/winnablebattles
10/4/11
6
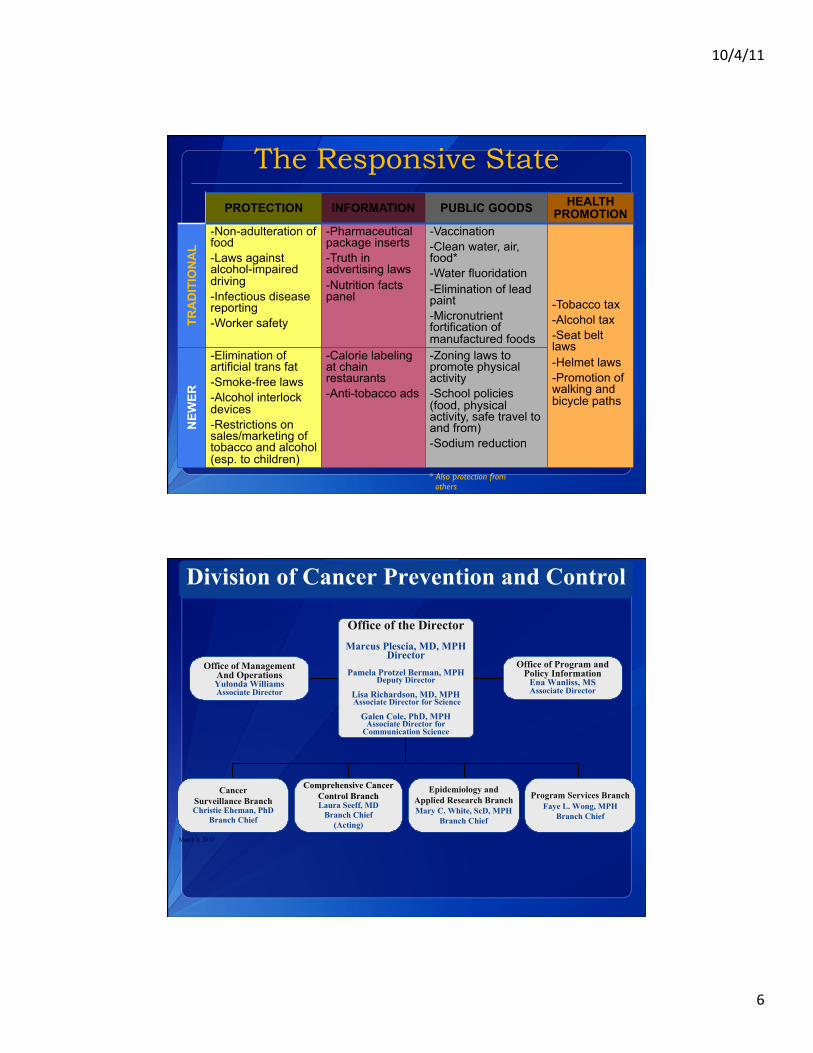
The Responsive State
PROTECTION INFORMATION PUBLIC GOODS HEALTH PROMOTION
TRA
DIT
ION
AL
-Non-adulteration of food -Laws against alcohol-impaired driving -Infectious disease reporting -Worker safety
-Pharmaceutical package inserts -Truth in advertising laws -Nutrition facts panel
-Vaccination -Clean water, air, food* -Water fluoridation -Elimination of lead paint -Micronutrient fortification of manufactured foods
-Tobacco tax -Alcohol tax -Seat belt laws -Helmet laws -Promotion of walking and bicycle paths
NEW
ER
-Elimination of artificial trans fat -Smoke-free laws -Alcohol interlock devices -Restrictions on sales/marketing of tobacco and alcohol (esp. to children)
-Calorie labeling at chain restaurants -Anti-tobacco ads
-Zoning laws to promote physical activity -School policies (food, physical activity, safe travel to and from) -Sodium reduction
* Also protection from others
March 8, 2010
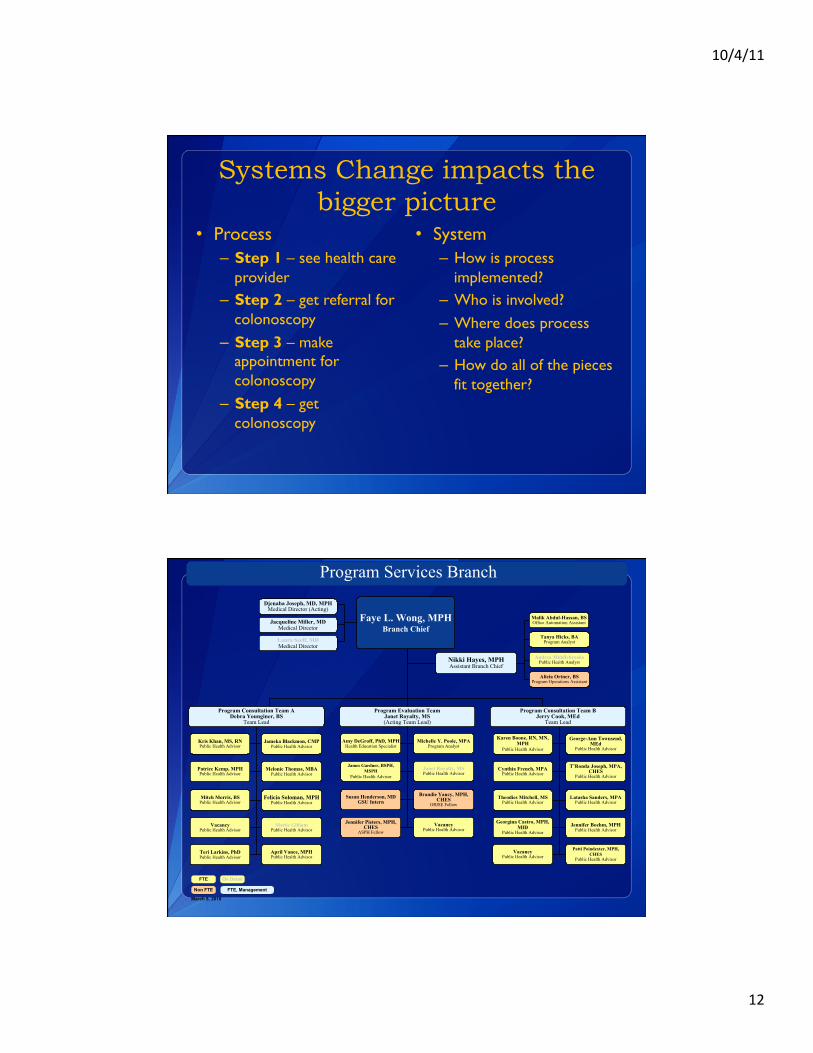
Office of Management And OperationsYulonda WilliamsAssociate Director
Office of Program and Policy Information
Ena Wanliss, MSAssociate Director
Comprehensive Cancer Control BranchLaura Seeff, MD
Branch Chief(Acting)
CancerSurveillance BranchChristie Eheman, PhD
Branch Chief
Epidemiology and Applied Research BranchMary C. White, ScD, MPH
Branch Chief
Program Services Branch Faye L. Wong, MPH
Branch Chief
Division of Cancer Prevention and Control
Office of the DirectorMarcus Plescia, MD, MPH
DirectorPamela Protzel Berman, MPH
Deputy Director
Lisa Richardson, MD, MPH Associate Director for Science
Galen Cole, PhD, MPHAssociate Director for
Communication Science

10/4/11
7
20th Anniversary
VISION: Healthy women living cancer-free
DCPC Cooperative Agreements & Special Projects
• Urban Indian Health Institute (UIHI) • Native American Cancer Research Corporation
(NACR) • “Walking Together: Making a Path Toward Healing” • CCC Tribal BRFSS Project with Tribal Epi Centers

10/4/11
8
Cancer Screening Challenges and Opportunities
Financial barriers • Uninsured, underinsured • Deductibles, Co-pays
• Increase program and clinic efficiencies? • Leverage existing resources to do more? • Affordable Care Act signed into law March 23, 2010 • Deductibles and co-pays waived
• Know screening needed/important? • Know screening available or covered? • Utilize benefits? • Have other barriers?
• Receive quality screening? • Receive complete follow-up? • Receive timely follow-up abnormal tests? • Receive timely referral into treatment? • Assured treatment if have no insurance? • Tracking, follow-up, quality monitoring?
Utilize preventive health screening services B
• Return for screening according to guidelines? • Same questions in “Utilize preventive health screening services A”
Utilize preventive health screening services A
Have access to screening • Eligible for free/low cost screening • Have insurance coverage

10/4/11
9
NCCCP Priorities 2010
• Emphasize Primary Prevention of Cancer • Coordinate Early Detection and Treatment Activities • Address Public Health Needs of Cancer Survivors • Use Policy, Systems, and Environmental Changes to
Guide Sustainable Cancer Control • Promote Health Equity as it Relates to Cancer
Control • Demonstrate Outcomes Through Evaluation
Increase screening from 64% to 80% in funded program states by 2014

10/4/11
10
• Greater emphasis on increasing colorectal cancer screening in all populations 50 and older – Reach insured, under- and uninsured – Invest in interventions ‘that
work’ (Community Guide recommendations)
– Achieve policy and systems changes, and effective health communications
– Leverage existing resources & infrastructures
• Less emphasis on directly providing colorectal cancer screening services to low income, uninsured, and underinsured populations
Systems Change
SYSTEMS CHANGE ????

10/4/11
11
What is Systems Change?*
A shift in the way a community makes decisions about policies, programs, and the allocation of its resources — and, ultimately, in the way it delivers services to its citizens
http://www.ccitoolsforfeds.org/systems_change.asp 2/2011*
*Adapted from Foster-Fishman et al, Using a Systems Change Approach to Evaluate
Comprehensive Community Change Initiatives
Why Systems Change?
When funds are spent just to deliver services, their impact is limited to the
people who receive those services. But when funds are devoted also to systems change, their impact can extend beyond a single program — to multiple programs, agencies, and service recipients, or to the entire community — and far into the future.
http://www.ccitoolsforfeds.org/systems_change.asp 2/2011
10/4/11
12
Systems Change impacts the bigger picture
• Process – Step 1 – see health care
provider – Step 2 – get referral for
colonoscopy – Step 3 – make
appointment for colonoscopy
– Step 4 – get colonoscopy
• System – How is process
implemented? – Who is involved? – Where does process
take place? – How do all of the pieces
fit together?
Nikki Hayes, MPHAssistant Branch Chief
March 8, 2010
FTE
Non FTE FTE, Management
Program Services Branch
On Detail
Program Consultation Team BJerry Cook, MEd
Team Lead
Program Evaluation TeamJanet Royalty, MS(Acting Team Lead)
Program Consultation Team ADebra Younginer, BS
Team Lead
Patrice Kemp, MPHPublic Health Advisor
Mitch Morris, BSPublic Health Advisor
Kris Khan, MS, RNPublic Health Advisor
VacancyPublic Health Advisor
Teri Larkins, PhDPublic Health Advisor
Jameka Blackmon, CMPPublic Health Advisor
Melonie Thomas, MBAPublic Health Advisor
Felicia Soloman, MPHPublic Health Advisor
Mattie GilliamPublic Health Advisor
April Vance, MPHPublic Health Advisor
Karen Boone, RN, MN, MPH
Public Health Advisor
Cynthia French, MPAPublic Health Advisor
Theodies Mitchell, MSPublic Health Advisor
Georgina Castro, MPH, MID
Public Health Advisor
James Gardner, BSPH, MSPH
Public Health Advisor
Susan Henderson, MDGSU Intern
Jennifer Pieters, MPH, CHES
ASPH Fellow
Amy DeGroff, PhD, MPHHealth Education Specialist
Janet Royalty, MSPublic Health Advisor
Brandie Yancy, MPH, CHES
ORISE Fellow
Michelle Y. Poole, MPAProgram Analyst
George-Ann Townsend, MEd
Public Health Advisor
Latasha Sanders, MPAPublic Health Advisor
T’Ronda Joseph, MPA, CHES
Public Health Advisor
Jennifer Boehm, MPHPublic Health Advisor
Patti Poindexter, MPH, CHES
Public Health Advisor
Tanya Hicks, BAProgram Analyst
Andrea MiddlebrooksPublic Health Analyst
Alicia Ortner, BSProgram Operations Assistant
VacancyPublic Health Advisor
VacancyPublic Health Advisor
Djenaba Joseph, MD, MPHMedical Director (Acting)
Laura Seeff, MDMedical Director
Jacqueline Miller, MDMedical Director
Faye L. Wong, MPHBranch Chief
Malik Abdul-Hassan, BSOffice Automation Assistant

10/4/11
13
Disclaimer
Information about CDC’s Cancer Prevention & Control Programs
www.cdc.gov/cancer
The findings and conclusions in this presentation are those of the presenter, and do not necessarily represent official
position of the Centers for Disease Control and Prevention.
THEMES

10/4/11
14
Successful Chronic Disease Programs
q Encourage incremental goal setting
q Encourage collaboration
q Share resources and tools
q Encourage evaluation efforts
q to improve systems
Embrace Changes You Can’t Control
yet address them all with incremental goals
q Epidemic of Chronic Disease
q Fiscal Environment
q Health Reform
q Globalism
q New Technologies
q Health Inequity
q ISMs- Racism, Sexism, that affect the quality of healthcare treatment for patients
10/4/11
15
Collaborating Partners
Emerging Needs for • Data • Communication • Partners
Collaborating Strategically
• Use Interventions and Messages that work
• Vigorous Evaluation (get added to Community Guide)
• Promote your Program & Support Providers
• Prepare to Assist in Health Reform -guides for newly insured
• Change terminology
• Improving health benefits/access through Medicaid/care, Insurance companies to set quality standards like the DQIGs)
• Learn about Health Equity and its impact in target populations
• Use Policy & Systems to advance public health prevention

10/4/11
16
Provider Support and Tools
Professional Development • Performance (as a
contractor for you) • New Technologies • New Guidelines –
impacts/implications for your program
• Impacts of health equity for the population served in your program
• Get to know EHRs selected by providers – who is tracking health disparities or the impact made on the winnable battles
• Get to know big insurance- improve employer benefits
• Untraditional Partners- housing, transportation, labor and justice system and gyms
Congressional Appropriation NBCCEDP FY 2009 – FY 2011
Program
FY 2009
FY 2010
FY2011
Net Difference FY10-FY11
NBCCEDP $186,325 $194,063 $190,148 <$3915>
* >80 percent extramural required. NBCCEDP extramural awards usually 82-84 percent and is 82.5 percent in FY 2011
Sharing Resources and Tools Shifts Focus to Priorities

10/4/11
17
*12.5% NBCCEDP eligible women aged 40-64 years
screened for breast cancer
*8.5% NBCCEDP eligible women aged 18-64 years
screened for cervical cancer
Some things keep changing
Approximation based on most current Census available to CDC matched to NBCCEDP MDE data for same years – 2008-2009 for breast cancer and 2007-2009 for cervical cancer. Includes low income, uninsured women.
While others remain the same…
About Providing Food:
Federal dollars may not be used
for food or beverages!
Find local
sponsors of food for educational
events!

10/4/11
18
Questions?
Thank you