a texting intervention in latino families to reduce ed use
TRANSCRIPT

A Texting Intervention in LatinoFamilies to Reduce ED Use: ARandomized TrialLisa Ross DeCamp, MD, MSPH,a,b Sashini K. Godage, BS,c Doris Valenzuela Araujo, BS,d José Dominguez Cortez,a
Linxuan Wu, MHS,b Kevin J. Psoter, MPA, PhD,b Kassandra Quintanilla, BA,e Tatiahna Rivera Rodri guez, MS,fSarah Polk, MD, ScMa,b
abstractBACKGROUND AND OBJECTIVES: Latino children in immigrant families experience health caredisparities. Text messaging interventions for this population may address disparities. Theobjective of this study was to evaluate the impact of a Spanish-language text messagingintervention on infant emergency department use and well care and vaccine adherence.
METHODS: The Salud al Día intervention, an educational video and interactive text messagesthroughout the child’s first year of life, was evaluated via randomized controlled trialconducted in an urban, academic pediatric primary care practice from February 2016 toDecember 2017. Inclusion criteria were publicly insured singleton infant ,2 months of age;parent age .18, with Spanish as the preferred health care language; and at least 1 householdcellular phone. Primary outcomes were abstracted from the electronic medical record at age15 months. Intention-to-treat analyses were used.
RESULTS: A total of 157 parent-child dyads were randomly assigned to Salud al Día (n = 79) orcontrol groups (n = 78). Among all participants, mean parent age was 29.3 years (SD: 6.2years), mean years in the United States was 7.3 (SD: 5.3 years), and 87% of parents hadlimited or marginal health literacy. The incidence rate ratio for emergency department use forthe control versus intervention group was 1.48 (95% confidence interval: 1.04–2.12). Agreater proportion of intervention infants received 2 flu vaccine doses compared with controls(81% vs 67%; P = .04).
CONCLUSIONS: This Spanish-language text messaging intervention reduced emergencydepartment use and increased flu vaccine receipt among a population at high risk for healthcare disparities. Tailored text message interventions are a promising method for addressingdisparities.
WHAT’S KNOWN ON THIS SUBJECT: Compared with nonimmigrants,immigrant patient populations have benefitted less from advances in healthcare information technology. A comprehensive approach to addressinghealth care disparities may require specific focus on implementation anduse of digital patient engagement tools among at-risk populations.
WHAT THIS STUDY ADDS: A Spanish-language text messaging interventionfor parents with limited health literacy and limited English proficiencydecreased emergency department use and increased flu vaccination. Withthis study, we contribute to emerging literature on the utility of theseinterventions to address health care disparities.
To cite: DeCamp LR, Godage SK, Valenzuela Araujo D, et al.A Texting Intervention in Latino Families to Reduce ED Use:A Randomized Trial. Pediatrics. 2020;145(1):e20191405
aCenter for Salud/Health and Opportunity for Latinos and bDepartment of Pediatrics, School of Medicine, JohnsHopkins University, Baltimore, Maryland; cHarvard Medical School, Harvard University, Boston, Massachusetts;dOregon Health and Science University, Portland, Oregon; eWestern Michigan Homer Stryker M.D. School ofMedicine, Kalamazoo, Michigan; and fStritch School of Medicine, Loyola University Chicago, Maywood, Illinois
Dr DeCamp made a substantial contribution to the conceptualization and design of the study, dataacquisition, and analysis and interpretation of the data and drafted the initial manuscript; MsGodage made a substantial contribution to data acquisition and analysis and interpretation of dataand drafted the initial manuscript; Ms Valenzuela Araujo made a substantial contribution to theconceptualization and design of the study and acquisition of data; Ms Quintanilla and Ms RiveraRodriguez made substantial contributions to the acquisition of data; Mr Dominguez Cortez madea substantial contribution to the analysis and interpretation of data; Ms Wu and Dr Psoter madesubstantial contributions to the analysis and interpretation of data and drafted the initialmanuscript; Dr Polk made a substantial contribution to the conceptualization (Continued)
PEDIATRICS Volume 145, number 1, January 2020:e20191405 ARTICLE by guest on October 11, 2021www.aappublications.org/newsDownloaded from

Latinos are the largest US minorityand comprise the majority of the 25million people in the United Stateswith limited English proficiency(LEP).1,2 Health care disparitiesamong Latino children are partiallyattributable to family-level barriers toeffective health care access and use,particularly among children withimmigrant and/or LEP parents.3–13
Gaps in health care knowledge andskills that contribute to health caredisparities among immigrant Latinopopulations include the following: (1)enrollment in and use of pediatricprimary care and public benefitprograms, (2) management of healthcare interactions and communicatingwith health care providers, and (3)management of routine childhoodillnesses.3,9,14–17 Language barriersand limited parent health literacycomplicate efforts to close these gapsfor Latino immigrant familes.18
Patient engagement interventions areoften focused on addressing healthcare knowledge and skills gaps.19–21
Culturally and linguisticallyappropriate patient engagementinterventions tailored for low healthliteracy populations are needed, butdevelopment of sustainable, scalableinterventions is a challenge.22
The ability to reach largerpopulations at lower cost, with thepotential for increased tailoring andinteractivity, is an underlying premiseof the development of text messaginginterventions (TMIs) to supportpatients in managing their health andhealth care.23,24 TMIs havedemonstrated efficacy in improvingappointment adherence, increasingvaccination, and decreasingemergency department (ED) useamong primary care populations andare increasing in pediatrics.25–31
Immigrant and LEP patientpopulations have benefitted less fromadvances in health care informationtechnology, such as TMIs or patientportals, than nonimmigrants becausethese interventions often targetpatients with high levels of health
literacy and are often not available innon-English languages.32,33
Salud al Día (Health Up-to-Date) ismultimodal intervention including aneducational video and interactive textmessages. The intervention,developed in partnership withimmigrant Latino families, wasdesigned to support health careengagement and navigation byimmigrant Latino parents of infants.We hypothesized that the supportprovided by the intervention wouldpromote family connection with theirchild’s medical home and result indecreased ED use. The purpose of thisstudy was to compare theeffectiveness of Salud al Día withusual care on ED use and well careand vaccination adherence from birthto 15 months.
METHODS
Study Population and Design
This 2-arm randomized controlledtrial (RCT) was conducted at anurban, academic general pediatricsclinic in the United States thataverages ∼13 000 visits annually. Theclinic’s majority patient population ispublicly insured Latino children withLEP immigrant parents. Parents orlegal guardians (referred to asparents) of publicly insured, singletonUS-born infants ,2 months of agewere eligible to participate.Additional inclusion criteria were asfollows: minimum parent age of18 years, self-identification as Latinoor Latina, preferred health carelanguage of Spanish, and 1 householdcellular phone. Potentially eligibleparticipants were identified viareview of the clinic schedule forcompleted initial newborn visits, andfamilies were sent a letter describingthe study. Potential participants werethen recruited either by follow-upphone call or during a subsequentnewborn visit between February andOctober 2016 by a bilingual researchassistant.
Eligible and interested parentsparticipated in an informed consentprocess, in which the Spanish-language form was read aloud andunderstanding was ascertained, andthen the participants completed anenrollment survey. Allocation to theintervention or usual care arm of theRCT was then unmasked toparticipants and research staff.Random assignment was performedby computer random numbergeneration in blocks of 10, with a 1:1allocation ratio. Clinic staff andproviders were not aware of groupassignment unless revealed by theparticipant, excepting a clinic nurseassigned to manage any e-mails to theclinic generated by the text messagesystem. The Institutional ReviewBoard at Johns Hopkins Medicineapproved this study. The study isregistered at ClinicalTrials.gov(identifier: NCT02647814).
Intervention
The Salud al Día intervention,consisting of interactive textmessages throughout the child’s firstyear of life and an educational video,was developed with the Latino FamilyAdvisory Board (LFAB), the patientfamily advisory council for the clinicin which the RCT was conducted.LFAB members assisted with allportions of the intervention design,from grant proposal toimplementation during regularlyscheduled meetings. LFAB meetingswere conducted in Spanish and wereattended by a cohort of 12 to 15members who were immigrantwomen from across Latin America.LFAB members primarily had US-born children insured throughMedicaid and most had less thana high school education;demographics of members reflectedthat of the larger clinic population.The situated Information, Motivation,Behavioral Skills (sIMB) model, whichhas been used previously tounderstand and intervene on patientengagement, was used in thedevelopment of intervention
2 DECAMP et al by guest on October 11, 2021www.aappublications.org/newsDownloaded from

content.34 Application of the modelresulted in intervention componentsto increase parent information,motivation, and behaviors thatpromote health care engagementtailored to the distinct factors amongLEP Latino families across personal,cultural, situational, and structuraldomains. Supplemental Table 4displays application of the sIMBmodel. Bright Futures and theaccompanying Family Voices guidewere used to ensure consistency withanticipatory guidance and educationrecommended by the AmericanAcademy of Pediatrics.35,36
Salud al Día text message interactivesequences included the following:appointment reminders, support forobtaining medicines, support forcompleting referrals, and illness caremonitoring and education. Text
messages used tailored “smart forms”to allow interactivity by deliveringmessages and automated responsesvia preprogrammed algorithms. Someresponse sets generated an e-mail toa clinic nurse to contact theparticipant to offer additionalassistance. The intervention did notinclude an opportunity forparticipants to initiate text sequences.Three different types of pushmessages that did not prompt replieswere also sent during the study: fluvaccine reminders, parent supportprogram reminders, and publicbenefit program reminders. Textmessages were personalized to thename and sex of the child, andmessage delivery was scheduledaccording to birth date and clinicappointment dates. Interventionparticipants began receiving textmessages after random assignment. A
timeline of delivered text messagesare displayed in Figure 1, and sampletext messages are displayed inSupplemental Figs 3 and 4. Messageswere programmed and delivered viaemocha, an open-source, secure,Health Insurance Portability andAccountability Act–compliant, andmodifiable mHealth application.37
Parents viewed the educational videoat the 2-month well-child visit, ratherthan at random assignment, becausepairing viewing with the baselinesurvey and orientation to study textmessages would have negativelyaffected clinic flow. LFAB membersrecommended that all initial studyactivities should be completed inclinic because they believed thiswould increase willingness toparticipate in the study. During the 2-month visit, interention participants
FIGURE 1Timeline of delivered text messages. Sample content from text messages is included as Supplemental Information. APT, appointment reminder textmessage; ICI, illlness care inquiry; ICM, illness care monitoring; MED, prescription medicine support; PUB, public benefit program reminder; REF, specialtycare referral support; WCC, well-child care visit.
PEDIATRICS Volume 145, number 1, January 2020 3 by guest on October 11, 2021www.aappublications.org/newsDownloaded from

were also enrolled in the healthsystem patient portal. Theeducational video, a 9-minuteSpanish-language animated video,was developed in response to LFABconcerns that immigrant parents didnot receive effective orientation topediatric primary care via writtenmaterials or during initial clinic visits.Video content included health carenavigation topics prioritized by boardmembers: clinic hours and supportservices (eg, after-hours telephonetriage, social work), the public healthinsurance enrollment and renewalprocess, selecting a primary careprovider and prioritizing seeing thisprovider at visits, taking an activerole during medical visits, andmanaging infant illness. Video designand production were completed inpartnership with a design fellow fromthe Maryland Institute College of Artand the LFAB.
Data Collection
In addition to the enrollment survey,participants completed a phone-administered midpoint survey (childage: 7–9 months) and an in-personfollow-up survey (child age: 12–15months). All participants received$30 for the enrollment and finalsurveys and $10 for the midpointsurvey. Intervention participants alsoreceived $20 remuneration to providesupport for cellular phone chargesbecause participants’ personalphones were used for text messaging.All surveys were orally administeredby bilingual research assistants.Survey responses were capturedsimultaneously with administrationusing a touchscreen tablet computerand Research Electronic DatabaseCapture software.38,39 Clinical datawere abstracted from the electronicmedical record (EMR) for each childfrom birth to 15 months viastandardized abstraction form.
Measures
Sociodemographic informationobtained during baseline surveysincluded the following: parent age,
educational attainment, country oforigin, length of stay in the UnitedStates, income, birth history, familystructure, and parental employment.English proficiency was assessed byusing the US Census Bureau question,“How well do you speak English?”40
Parent health literacy was measuredby using the Spanish-languageversion of the Newest Vital Sign.41
Parent health care engagement wasevaluated by using the Parent-PatientActivation Measure (P-PAM).42
P-PAM responses generate a scoreranging from 0 to 100; higher scoresrepresent higher parent health careengagement. The Patient HealthQuestionnaire–8 (PHQ-8) was used toassess parent depressivesymptoms.43 Infant health knowledgewas assessed on the basis ofintervention education topics,including (1) fever criteria, (2) publichealth insurance renewal, (3) right tointerpretation during medicalencounters, (4) obtaining an outsidecare report, and (5) availability ofafter-hours clinic resources. Theinfant health knowledge assessmentconsisted of 5 multiple choice or trueor false questions, with 1 pointawarded for each correct response.Parents were also asked about theircellular phone and plan type andchild’s health status. The midpointand follow-up surveys includedquestions assessing usability of andsatisfaction with the interactive textmessages.
Outcomes
ED use, up-to-date (UTD)immunizations, and well visits wereassessed as primary outcomes anddetermined by using individual EMRdata. ED encounters were availablefor any location in the health system,owing to a shared EMR. Childrenwere designated as having UTDimmunizations on the basis of theage-specific schedule used in theclinic that is derived from the Centersfor Disease Control and PreventionRecommended ImmunizationSchedule.44 The American Academy
of Pediatrics Bright Futuresperiodicity guidelines were used todetermine age-specific criteria fornumber of well visits to be consideredas UTD.35
Secondary outcomes were parentexperience of care rating via thefollow-up survey and change in meanparent engagement and infant healthknowledge between baseline andfollow-up surveys. Parents wereasked to report their experience ofcare by using selected questions fromthe Consumer Assessment ofHealthcare Providers and SystemsClinician and Group 12-MonthSurvey.45 Parent satisfaction with theclinic and primary provider wasassessed by using a scale of 0 (“notsatisfied”) to 10 (“extremelysatisfied”). Responses weredichotomized by using a top-boxsystem of “10” versus otherresponses.46
Process outcomes were as follows:receipt of 2 doses of the influenzavaccine, well visit no-shows, well visitcancellations, clinic visit providercontinuity, number of sick care visits,specialty care referral completion,participant-generated telephoneencounters, EMR patient portal(MyChart) status, SupplementalNutrition Assistance Program (SNAP)or food stamp participation, andchange in parent depression. Providercontinuity was measured by using theBice-Boxerman Continuity of CareIndex based on well-child and sickclinic visits in the 15 months sincebirth.47,48
Analysis
The sample size for this study wasestimated by using a nondirectionaltest to achieve 80% power andsignificance of a = .05. A sample sizeof 40 per group was determinedsufficient to detect a difference of oneED visit per group. A priori increasedenrollment was targeted to increasepower to detect differences insecondary outcomes. Demographicand clinical characteristics of parent
4 DECAMP et al by guest on October 11, 2021www.aappublications.org/newsDownloaded from

and child participants randomlyassigned to the Salud al Día and usualcare groups were summarized andcompared by using Student t testswith unequal variances and x2 orFisher exact tests for continuous andcategorical variables, respectively. Inaddition, for the count outcome of EDuse, the total number of ED visits andinfants per group was used tocalculate an incidence rate (numberof ED visits per infant). To comparethe incidence rates between groups,we used an incidence rate ratio andcorresponding 95% confidenceintervals. Lastly, differences in meanparent engagement, infant healthknowledge, and parent depressionfrom baseline to follow-up wereassessed within each group by usinga paired t test. Analyses of primary
outcomes were conducted per theintention-to-treat principle. Analysesof secondary and process outcomesthat were not abstracted from theEMR included only those individualswith corresponding follow-up surveydata. A 2-sided P value ,.05 wasconsidered statistically significant. Allanalyses were conducted using Stata15.1 (StataCorp LP, CollegeStation, TX).
RESULTS
A total of 157 parent-infant dyadsparticipated in the study, with 79randomly assigned to theintervention and 78 randomlyassigned to usual care (Fig 2). Overallmean parent age was 29.3 years (SD:6.2 years), and mean years in the
United States was 7.3 years (SD: 5.3years). Sixty-seven percent ofparents had less than a high schooleducation, and 87% of parents hadlimited or marginal health literacy.Participants were balanced inbaseline characteristics (Table 1).Intervention participants receiveda mean of 45.0 (SD: 8.5) messagesand sent a mean of 15.5 (SD: 6.7)messages. Five percent (n = 4)of intervention participantsdid not send any responses. Ninety-three percent of interventionparticipants rated textmessage sequences as very easyor easy to use, 96% stronglyagreed or agreed that the messagesmade them feel more connectedto the clinic, and 92% strongly agreedor agreed that the text messages
FIGURE 2Study consort diagram. aAll participants allocated to the intervention received the intervention. The number of text messages received by eachparticipant varied by the number of scheduled and completed well visits and participant responses to the interactive message sequences.
PEDIATRICS Volume 145, number 1, January 2020 5 by guest on October 11, 2021www.aappublications.org/newsDownloaded from

made them feel able to do morefor their child’s health. Freetext comments on the programincluded positive comments on
helpfulness in rememberingappointments and in providinginformation about clinic andcommunity services.
Among the primary outcomes for thisstudy, there was a statisticallysignificant difference between groupsin ED use (Table 2). The meannumber of ED visits in theintervention group was 1.23 (SD:1.66), and mean ED visits for thecontrol group was 1.82 (SD: 1.64)(P = .03). The incidence rate ratio forED use for the control versusintervention group was 1.48 (95%confidence interval: 1.04–2.12). Therewere no differences in UTDimmunizations or well visits betweengroups. Among secondary outcomes,both intervention and controlparticipants had a statisticallysignificant increase in parentengagement and infant healthknowledge from baseline to follow-up, but the changes in these scoreswere not significantly differentbetween groups (Table 2).
Among the process outcomes(Table 3), a greater proportion ofinfants in the intervention groupreceived 2 flu vaccine doses versusinfants in the usual care group (81%vs 67%; P = .04). Well visit no-showsapproached significance, with 34% ofintervention group participantshaving 1 or more no-shows comparedwith 49% of usual care (P = .06).Although a minority of interventiongroup participants remained in activestatus for the patient portal, this wassignificantly greater than controlgroup participants. Only 1intervention group participant senta patient portal message to the clinic,and no control participants senta message.
DISCUSSION
In this RCT evaluating the Salud al Díaintervention, we found significantlyreduced infant ED use compared withcontrol group participants. Inaddition, a greater proportion ofinfants in the intervention groupreceived 2 doses of the flu vaccinecompared with the control group. Wedid not, however, find a difference in
TABLE 1 Parent and Child Baseline Characteristics
Characteristic Salud al Día Usual Care
n = 79 n = 78
Mean maternal age, y (SD) 30.1 (6.1) 28.7 (6.3)Maternal education, n (%)Eighth grade or less 27 (34) 37 (47)Some high school 23 (29) 18 (23)High school or greater 29 (37) 23 (29)
Maternal country of origin, n (%)Mexico 18 (23) 16 (21)El Salvador 22 (28) 24 (31)Honduras 22 (28) 25 (32)Other Latin American countries 17 (22) 13 (17)
Mean maternal length of stay in the United States, y (SD) 7.5 (5.1) 7.2 (5.5)Maternal LEP, n (%) 77 (97) 75 (96)Birth history, n (%)Primigravida 19 (24) 25 (32)Multigravida, first US-born child 14 (18) 21 (27)Multigravida, previous US-born child or children 46 (58) 32 (41)
Annual family income, n (%),$20 000 26 (33) 41 (53)$20 000–$30 000 22 (28) 16 (21).$30 000 7 (9) 5 (6)Did not report or unknown 24 (30) 16 (21)
Family structure, n (%)Single 14 (18) 18 (23)Spouse or partner 65 (82) 60 (77)
Maternal plans to work in the next 6 mo,a n (%)Yes 29 (37) 38 (49)No 34 (43) 29 (37)Unsure 16 (20) 11 (14)
Spouse or partner employed,b n (%) 65 (100) 59 (98)Maternal health literacy, newest vital sign, n (%)Limited health literacy, 0–1 36 (46) 40 (51)Marginal health literacy, 2–3 31 (39) 29 (37)Adequate health literacy, 4–6 12 (15) 9 (12)
Mean parent health care engagement score,c P-PAM (SD) 69.22 (17.04) 69.20 (14.01)Mean infant health knowledge scored (SD) 2.95 (0.93) 2.85 (1.01)Maternal depression, PHQ-8, n (%)No significant depressive symptoms, 0–4 49 (63) 57 (73)Mild depressive symptoms, 5–9 22 (28) 17 (22)Moderate or severe depressive symptoms, $10 7 (9) 4 (5)
Parent-reported child health status, n (%)Excellent, very good, or good 77 (97) 78 (100)Fair or poor 2 (3) 0 (0)
Current smartphone user, n (%) 72 (91) 72 (92)Primary user of cell phone, n (%) 75 (95) 77 (99)Cell phone plan, n (%)Contract plan 55 (70) 52 (67)Prepaid 24 (30) 26 (33)
a Current employment measure was not used because of maternal interview timing before 2 mo of age; nearly allmothers remained at home with their infant.b Further specification of hours worked per week or full-time versus part-time was not possible because work as a daylaborer or short-term construction jobs were primary sources of spouse employment.c Parent health care engagement score ranges from 0 to 100; higher scores represent higher parentage of health careengagement.d Infant health knowledge score ranges from 0 to 5. Questions on the assessment were based on educational topicsincluded in the intervention.
6 DECAMP et al by guest on October 11, 2021www.aappublications.org/newsDownloaded from

well care or overall immunizationadherence. Our results demonstratethat delivery of interactive textmessages with preprogrammedalgorithms was feasible and usable byimmigrant Latino parents with loweducational attainment and/or healthliteracy. Employing an establishedhealth behavior theory andinvolvement of immigrant Latinoparents throughout the design andimplementation of the study mayhave contributed to the intervention’susability and feasibility. This studyadds to the growing literature thatTMIs can be used to improve healthcare outcomes among vulnerablepopulations.
Our finding of reduced ED use in theintervention arm is notable given therelatively high ED use among Latinoparents with LEP.10,49 Thisintervention was also designed forparents with limited health literacy,which is common among Latinoimmigrant parents and has beenassociated with increased EDuse.18,50,51 The mechanism by whichthe intervention decreased ED use isunclear, although it is likelymultifactorial. The intervention wasdesigned to provide information and
motivation to increase parent healthcare engagement behaviors. On thebasis of adult studies, wehypothesized that increasedengagement would lead to improvedhealth care outcomes.19,20,52–56 Wefound, however, that parentengagement, as measured by theP-PAM, increased over the studyperiod among parents in both groups,but there was no significantdifference in the magnitude of changeby group. We have demonstratedpreviously that Spanish-dominantimmigrant Latino parents have lowerengagement scores than English-dominant parents, a findingconsistent with adult studies.57,58
Additional studies, however, haveraised concerns about P-PAMmeasurement limitations for parenthealth care engagement.59,60
Intervention participants endorsedhigh levels of feeling connected to theclinic through interventionparticipation, which may indicateparent engagement not captured bythe P-PAM.
Our findings of increased receipt of 2doses of flu vaccine in the Salud al Díagroup is consistent with other TMIsemploying flu vaccine reminders.27,28
In contrast to other studies of textmessage appointment reminders, wedid not find a decreased no-show ratein the intervention group.26 Thesample size may have beeninadequate to detect a differencebecause the study was not poweredfor this outcome, but this measureapproached significance. We alsocannot exclude contamination of thecontrol group because the healthsystem where the study took placeimplemented text messageappointment reminders during thestudy period. Enrollment in the healthsystem reminders was elective andnot advertised in Spanish. We wereunable to link data to determine howmany control group participants mayhave been enrolled, although overallenrollment of patients in the studyclinic was low. Many health caresystems are now employing someform for text message appointmentreminders. In several reviews,authors have found variableeffectiveness of these reminders indecreasing no-shows andconsiderable heterogeneity in textmessaging programs.61–64 Theheterogeneity of TMIs and thecommon practice of focusing on onetheme (eg, appointment or vaccinereminders or singular diseasemanagement) creates a fragmentedmenu of potentially effective TMIs.The current state of narrowly focusedTMIs limits potential effectiveness ofthese interventions to promoteimproved access to or quality ofpediatric primary care.
The impact of the Salud al Díaintervention on some outcomes andthe positive end-user assessmentshighlight the potential of morebroadly focused TMIs to address theemerging digital divide in health care.Salud al Día allowed for families torequest assistance with appointmentrescheduling, medications, andreferrals in a workflow that routedrequests for assistance to clinicnursing staff. This workflow is notunlike a patient portal. Patients
TABLE 2 Intervention Outcomes and Use
Characteristic Salud al Día Usual Care P
n = 79 n = 78
Primary outcomes, intention-to-treat analysisED visits, mean (SD) 1.23 (1.66) 1.82 (1.64) .03a
ED use, n (%)0 visits 33 (42) 17 (22) .03a
1 visit 19 (24) 23 (29) —
$2 visits 27 (34) 38 (49) —
Immunizations UTD, n (%)b 67 (85) 62 (79) .38Well visits UTD, n (%) 60 (76) 53 (68) .26
Secondary outcomes, based on follow-up survey n = 72 n = 63Parent experience of care, top-box rating, n (%)Clinic overall 59 (82) 50 (79) .71Primary provider 58 (81) 46 (73) .30
Parent health care engagement score change, mean (SD) 10.88 (2.14) 8.53 (2.75) .50a
Infant health knowledge score change, mean (SD) 0.67 (0.15) 0.52 (0.15) .52a
—, not applicable.a P value based on x2 or Fisher exact tests for categorical variables; Student t tests were used to compare continuousoutcomes and reflect difference in change in scores from baseline to follow-up between groups.b UTD immunizations through 12 mo well visit vaccines were determined on the basis of available data in the EMR andwere not restricted to those immunizations administered at the clinic. Receipt of rotavirus vaccination was not used inthis determination because of local factors that affected rotavirus vaccine availability during the study period.
PEDIATRICS Volume 145, number 1, January 2020 7 by guest on October 11, 2021www.aappublications.org/newsDownloaded from
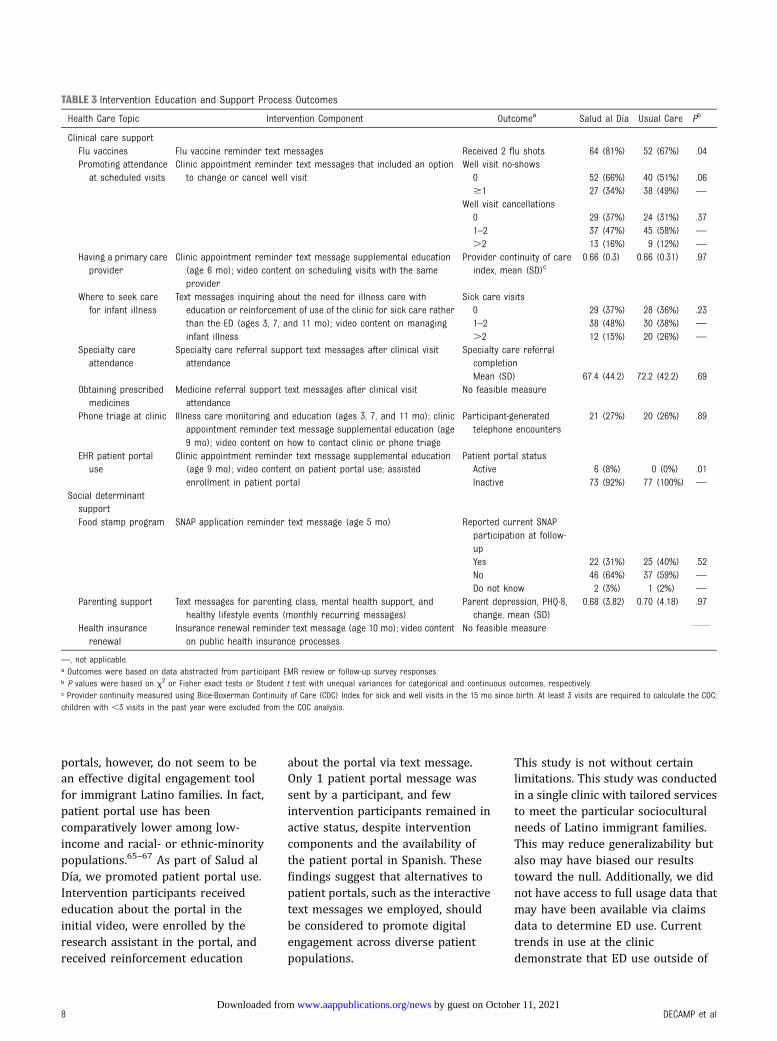
portals, however, do not seem to bean effective digital engagement toolfor immigrant Latino families. In fact,patient portal use has beencomparatively lower among low-income and racial- or ethnic-minoritypopulations.65–67 As part of Salud alDía, we promoted patient portal use.Intervention participants receivededucation about the portal in theinitial video, were enrolled by theresearch assistant in the portal, andreceived reinforcement education
about the portal via text message.Only 1 patient portal message wassent by a participant, and fewintervention participants remained inactive status, despite interventioncomponents and the availability ofthe patient portal in Spanish. Thesefindings suggest that alternatives topatient portals, such as the interactivetext messages we employed, shouldbe considered to promote digitalengagement across diverse patientpopulations.
This study is not without certainlimitations. This study was conductedin a single clinic with tailored servicesto meet the particular socioculturalneeds of Latino immigrant families.This may reduce generalizability butalso may have biased our resultstoward the null. Additionally, we didnot have access to full usage data thatmay have been available via claimsdata to determine ED use. Currenttrends in use at the clinicdemonstrate that ED use outside of
TABLE 3 Intervention Education and Support Process Outcomes
Health Care Topic Intervention Component Outcomea Salud al Día Usual Care Pb
Clinical care supportFlu vaccines Flu vaccine reminder text messages Received 2 flu shots 64 (81%) 52 (67%) .04Promoting attendance
at scheduled visitsClinic appointment reminder text messages that included an option
to change or cancel well visitWell visit no-shows0 52 (66%) 40 (51%) .06$1 27 (34%) 38 (49%) —
Well visit cancellations0 29 (37%) 24 (31%) .371–2 37 (47%) 45 (58%) —
.2 13 (16%) 9 (12%) —
Having a primary careprovider
Clinic appointment reminder text message supplemental education(age 6 mo); video content on scheduling visits with the sameprovider
Provider continuity of careindex, mean (SD)c
0.66 (0.3) 0.66 (0.31) .97
Where to seek carefor infant illness
Text messages inquiring about the need for illness care witheducation or reinforcement of use of the clinic for sick care ratherthan the ED (ages 3, 7, and 11 mo); video content on managinginfant illness
Sick care visits0 29 (37%) 28 (36%) .231–2 38 (48%) 30 (38%) —
.2 12 (15%) 20 (26%) —
Specialty careattendance
Specialty care referral support text messages after clinical visitattendance
Specialty care referralcompletionMean (SD) 67.4 (44.2) 72.2 (42.2) .69
Obtaining prescribedmedicines
Medicine referral support text messages after clinical visitattendance
No feasible measure
Phone triage at clinic Illness care monitoring and education (ages 3, 7, and 11 mo); clinicappointment reminder text message supplemental education (age9 mo); video content on how to contact clinic or phone triage
Participant-generatedtelephone encounters
21 (27%) 20 (26%) .89
EHR patient portaluse
Clinic appointment reminder text message supplemental education(age 9 mo); video content on patient portal use; assistedenrollment in patient portal
Patient portal statusActive 6 (8%) 0 (0%) .01Inactive 73 (92%) 77 (100%) —
Social determinantsupportFood stamp program SNAP application reminder text message (age 5 mo) Reported current SNAP
participation at follow-upYes 22 (31%) 25 (40%) .52No 46 (64%) 37 (59%) —
Do not know 2 (3%) 1 (2%) —
Parenting support Text messages for parenting class, mental health support, andhealthy lifestyle events (monthly recurring messages)
Parent depression, PHQ-8,change, mean (SD)
0.68 (3.82) 0.70 (4.18) .97
Health insurancerenewal
Insurance renewal reminder text message (age 10 mo); video contenton public health insurance processes
No feasible measure
—, not applicable.a Outcomes were based on data abstracted from participant EMR review or follow-up survey responses.b P values were based on x2 or Fisher exact tests or Student t test with unequal variances for categorical and continuous outcomes, respectively.c Provider continuity measured using Bice-Boxerman Continuity of Care (COC) Index for sick and well visits in the 15 mo since birth. At least 3 visits are required to calculate the COC;children with ,3 visits in the past year were excluded from the COC analysis.
8 DECAMP et al by guest on October 11, 2021www.aappublications.org/newsDownloaded from

the health system for which we haddata is low. Urgent care use, however,is common, and we were unable toassess this. Because urgent care use isgenerally less costly than ED use, thefinding of decreased ED use remainsnotable.68 In the future, it will becritical to capture all usage indetermining the impact andcost-effectiveness of TMIs. Next, weare unable to determine theindependent effect of the 2intervention components onoutcomes. We believe that theprimary impact on health careoutcomes stemmed from the textmessages, given the difference inexposure between 1 video andthe text messages over a year, butcannot be certain. Finally, we cannotexclude selection bias in our sampleand in determining outcomesassessed by the follow-up survey. Themajority of approached patients didenroll in the study, but the most at-risk patients may be among thosewho did not. Similarly, our studyretention rates were high, especiallygiven the vulnerability of this sample,but it could be that the most
vulnerable patients were notretained.
CONCLUSIONS
With this study, we contribute tothe emerging literature onthe utility of TMIs to address healthcare disparities. The Salud al Díaintervention was based on existinghealth behavior theory andwas designed in partnership withpatients to ensure that theintervention met user needs andpreferences and wasapplicable across the range ofpediatric primary carepatients. Whether increasinglyavailable TMIs from commercialvendors will be able to meet theneeds of vulnerable populationsremains to be seen. Without a specificfocus on vulnerable populations inthe design and implementation ofnew health care informationtechnology, the gap in digital healthcare engagement may widen,potentially increasing health caredisparities for these populations.
ACKNOWLEDGMENTS
We thank the members of the LFAB,without whom this project wouldnot have been possible. Additionally,this project was partially supportedby the Johns Hopkins Schoolof Medicine Biostatistics,Epidemiology, and DataManagement Core.
ABBREVIATIONS
ED: emergency departmentEMR: electronic medical recordLEP: limited English proficiencyLFAB: Latino Family Advisory
BoardPHQ-8: Patient Health
Questionnaire–8P-PAM: Parent-Patient Activation
MeasureRCT: randomized controlled trialsIMB: situated InformationMotivation: Behavioral SkillsSNAP: Supplemental Nutrition
Assistance ProgramTMI: text messaging interventionUTD: up-to-date
and design of the study and the analysis and interpretation of data; and all authors revised the manuscript critically for important intellectual content, approved
the final manuscript as submitted, and agree to be accountable for all aspects of the work.
This trial has been registered at www.clinicaltrials.gov (identifier NCT02647814).
Data Sharing Statement: Deidentified individual participant data will not be made available.
Dr DeCamp’s current affiliation is the Adult and Child Consortium for Health Outcomes Research and Delivery Science, Department of Pediatrics, School of Medicine,
University of Colorado and Children’s Hospital Colorado, Aurora, CO.
DOI: https://doi.org/10.1542/peds.2019-1405
Accepted for publication Oct 16, 2019
Address correspondence to Lisa Ross DeCamp, MD, MSPH, University of Colorado School of Medicine, Children’s Hospital Colorado ACCORDS (Adult and Child
Consortium for Health Outcomes Research and Delivery Science), 13199 E Montview Blvd, Suite 300, Mail Stop F443, Aurora, CO 80045. E-mail: lisa.decamp@
childrenscolorado.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by the Gordon and Betty Moore Foundation.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
PEDIATRICS Volume 145, number 1, January 2020 9 by guest on October 11, 2021www.aappublications.org/newsDownloaded from

REFERENCES
1. US Census Bureau. 2010 census briefs:the Hispanic population 2010. Availableat: www.census.gov/prod/cen2010/briefs/c2010br-04.pdf. Accessed March31, 2019
2. US Census Bureau. Language spoken athome: 2010 American communitysurvey 1- year estimates. Available at:http://factfinder2.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=ACS_10_1YR_S1601&prodType=table. Accessed March 31, 2019
3. Flores G; Committee On PediatricResearch. Technical report–racial andethnic disparities in the health andhealth care of children. Pediatrics.2010;125(4). Available at: www.pediatrics.org/cgi/content/full/125/4/e979
4. Flores G, Olson L, Tomany-Korman SC.Racial and ethnic disparities in earlychildhood health and health care.Pediatrics. 2005;115(2). Available at:www.pediatrics.org/cgi/content/full/115/2/e183
5. Flores G, Tomany-Korman SC. Racial andethnic disparities in medical and dentalhealth, access to care, and use ofservices in US children [publishedcorrection appears in Pediatrics. 2009;124(3):999–1000]. Pediatrics. 2008;121(2). Available at: www.pediatrics.org/cgi/content/full/121/2/e286
6. Flores G, Abreu M, Tomany-Korman SC.Why are Latinos the most uninsuredracial/ethnic group of US children? Acommunity-based study of risk factorsfor and consequences of being anuninsured Latino child [publishedcorrection appears in Pediatrics. 2006;118(5):2270]. Pediatrics. 2006;118(3).Available at: www.pediatrics.org/cgi/content/full/118/3/e730
7. Flores G, Tomany-Korman SC. Thelanguage spoken at home anddisparities in medical and dentalhealth, access to care, and use ofservices in US children [publishedcorrection appears in Pediatrics. 2009;124(4):1265]. Pediatrics. 2008;121(6).Available at: www.pediatrics.org/cgi/content/full/121/6/e1703
8. DeCamp LR, Choi H, Davis MM. Medicalhome disparities for Latino children byparental language of interview. J Health
Care Poor Underserved. 2011;22(4):1151–1166
9. Brousseau DC, Hoffmann RG, Yauck J,Nattinger AB, Flores G. Disparities forLatino children in the timely receipt ofmedical care. Ambul Pediatr. 2005;5(6):319–325
10. Kubicek K, Liu D, Beaudin C, et al. Aprofile of nonurgent emergencydepartment use in an urban pediatrichospital. Pediatr Emerg Care. 2012;28(10):977–984
11. Inkelas M, Schuster MA, Olson LM, ParkCH, Halfon N. Continuity of primary careclinician in early childhood. Pediatrics.2004;113(suppl 6):1917–1925
12. Weech-Maldonado R, Morales LS,Spritzer K, Elliott M, Hays RD. Racial andethnic differences in parents’assessments of pediatric care inMedicaid managed care. Health ServRes. 2001;36(3):575–594
13. Halfon N, Inkelas M, Mistry R, Olson LM.Satisfaction with health care for youngchildren. Pediatrics. 2004;113(suppl 6):1965–1972
14. DeCamp LR, Bundy DG. Generationalstatus, health insurance, and publicbenefit participation among low-incomeLatino children. Matern Child Health J.2012;16(3):735–743
15. Ngui EM, Flores G. Satisfaction withcare and ease of using health careservices among parents of childrenwith special health care needs: theroles of race/ethnicity, insurance,language, and adequacy of family-centered care. Pediatrics. 2006;117(4):1184–1196
16. Flores G, Abreu M, Brown V, Tomany-Korman SC. How Medicaid and the StateChildren’s Health Insurance Programcan do a better job of insuringuninsured children: the perspectives ofparents of uninsured Latino children.Ambul Pediatr. 2005;5(6):332–340
17. DeCamp LR, Kieffer E, Zickafoose JS,et al. The voices of limited Englishproficiency Latina mothers on pediatricprimary care: lessons for the medicalhome. Matern Child Health J. 2013;17(1):95–109
18. Yin HS, Sanders LM, Rothman RL, et al.Assessment of health literacy and
numeracy among Spanish-Speakingparents of young children: validation ofthe Spanish Parental Health LiteracyActivities Test (PHLAT Spanish). AcadPediatr. 2012;12(1):68–74
19. Hibbard JH, Greene J. What theevidence shows about patientactivation: better health outcomes andcare experiences; fewer data on costs.Health Aff (Millwood). 2013;32(2):207–214
20. Deen D, Lu WH, Rothstein D, Santana L,Gold MR. Asking questions: the effect ofa brief intervention in communityhealth centers on patient activation.Patient Educ Couns. 2011;84(2):257–260
21. Thomas KC, Stein GL, Williams CS, et al.Fostering activation among Latinoparents of children with mental healthneeds: an RCT. Psychiatr Serv. 2017;68(10):1068–1075
22. López L, Tan-McGrory A, Horner G,Betancourt JR. Eliminating disparitiesamong Latinos with type 2 diabetes:effective eHealth strategies. J DiabetesComplications. 2016;30(3):554–560
23. Text4baby. Data and evaluation.Available at: https://www.text4baby.org/about/data-and-evaluation. AccessedMarch 31, 2019
24. Anderson-Lewis C, Darville G, MercadoRE, Howell S, Di Maggio S. mHealthtechnology use and implications inhistorically underserved and minoritypopulations in the United States:systematic literature review. JMIRMhealth Uhealth. 2018;6(6):e128
25. Poorman E, Gazmararian J, Parker RM,Yang B, Elon L. Use of text messagingfor maternal and infant health:a systematic review of the literature.Matern Child Health J. 2015;19(5):969–989
26. Lin CL, Mistry N, Boneh J, Li H, LazebnikR. Text message reminders increaseappointment adherence in a pediatricclinic: a randomized controlled trial. IntJ Pediatr. 2016;2016:8487378
27. Stockwell MS, Kharbanda EO, MartinezRA, Vargas CY, Vawdrey DK, Camargo S.Effect of a text messaging interventionon influenza vaccination in an urban,low-income pediatric and adolescentpopulation: a randomized controlledtrial. JAMA. 2012;307(16):1702–1708
10 DECAMP et al by guest on October 11, 2021www.aappublications.org/newsDownloaded from

28. O’Leary ST, Lee M, Lockhart S, et al.Effectiveness and cost of bidirectionaltext messaging for adolescent vaccinesand well care. Pediatrics. 2015;136(5).Available at: www.pediatrics.org/cgi/content/full/136/5/e1220
29. Ladley A, Hieger AW, Arthur J, Broom M.Educational text messages decreasedEmergency Department utilizationamong infant caregivers: a randomizedtrial. Acad Pediatr. 2018;18(6):636–641
30. Kharbanda EO, Stockwell MS, Fox HW,Andres R, Lara M, Rickert VI. Textmessage reminders to promote humanpapillomavirus vaccination. Vaccine.2011;29(14):2537–2541
31. Fedele DA, Cushing CC, Fritz A, AmaroCM, Ortega A. Mobile healthinterventions for improving healthoutcomes in youth: a meta-analysis.JAMA Pediatr. 2017;171(5):461–469
32. NORC at the University of Chicago.Briefing Paper: Understanding theImpact of Health IT in UnderservedCommunities and Those With HealthDisparities. Chicago, IL: University ofChicago; 2010
33. López L, Green AR, Tan-McGrory A, KingR, Betancourt JR. Bridging the digitaldivide in health care: the role of healthinformation technology in addressingracial and ethnic disparities. Jt CommJ Qual Patient Saf. 2011;37(10):437–445
34. Rivet Amico K. A situated-InformationMotivation Behavioral Skills Model ofCare Initiation and Maintenance (sIMB-CIM): an IMB model based approach tounderstanding and intervening inengagement in care for chronicmedical conditions. J Health Psychol.2011;16(7):1071–1081
35. Bright Futures/American Academy ofPediatrics. Recommendations forpreventive pediatric health care.Available at: https://www.aap.org/en-us/Documents/periodicity_schedule.pdf. Accessed March 31, 2019
36. Vickers M, Anderson B, Dworetzky B,Popper B. Traducción Al Español deMonica Bernot. Bright Futures – GuíaPara Las Familias – Criando Bebés,Niños Y Adolescentes Saludables.Albuquerque, NM: Family Voices; 2014
37. Emocha. Emocha. Available at: www.emocha.com. Accessed March 31, 2019
38. REDCap. REDCap. Available at: http://project-redcap.org. Accessed March 31,2019
39. Harris PA, Taylor R, Thielke R, Payne J,Gonzalez N, Conde JG. Research electronicdata capture (REDCap)–a metadata-driven methodology and workflowprocess for providing translationalresearch informatics support. J BiomedInform. 2009;42(2):377–381
40. US Census Bureau. Why we ask:language spoken at home. Available at:https://www2.census.gov/programs-surveys/acs/about/qbyqfact/Language.pdf. Accessed October 31, 2019
41. US Census Bureau. Language use.Available at: https://www.census.gov/topics/population/language-use/about.html. Accessed November 4, 2019
42. Health I. Parent-Patient ActivationMeasure. 2011. Available at: www.insigniahealth.com. Accessed March 31,2019
43. Kroenke K, Strine TW, Spitzer RL,Williams JB, Berry JT, Mokdad AH. ThePHQ-8 as a measure of currentdepression in the general population.J Affect Disord. 2009;114(1–3):163–173
44. Centers for Disease Control andPrevention. Recommendedimmunization schedule for children andadolescents aged 18 years or younger,United States, 2019. Available at:https://www.cdc.gov/vaccines/schedules/hcp/child-adolescent.html.Accessed March 31, 2019
45. Agency for Healthcare Research andQuality. Consumer Assessment ofHealthcare Providers and Systems.Available at: https://cahps.ahrq.gov/#.Accessed March 31, 2019
46. American Institutes for Research. Howto report results of the CAHPS clinicianand group survey. Available at: https://www.ahrq.gov/sites/default/files/wysiwyg/cahps/surveys-guidance/cg/cgkit/HowtoReportResultsofCGCAHPS080610FINAL.pdf. AccessedMarch 31, 2019
47. Bice TW, Boxerman SB. A quantitativemeasure of continuity of care. MedCare. 1977;15(4):347–349
48. Jee SH, Cabana MD. Indices forcontinuity of care: a systematic reviewof the literature. Med Care Res Rev.2006;63(2):158–188
49. Ngai KM, Grudzen CR, Lee R, Tong VY,Richardson LD, Fernandez A. Theassociation between limited Englishproficiency and unplanned emergencydepartment revisit within 72 hours. AnnEmerg Med. 2016;68(2):213–221
50. Morrison AK, Schapira MM, GorelickMH, Hoffmann RG, Brousseau DC. Lowcaregiver health literacy is associatedwith higher pediatric emergencydepartment use and nonurgent visits.Acad Pediatr. 2014;14(3):309–314
51. Morrison AK, Myrvik MP, Brousseau DC,Hoffmann RG, Stanley RM. Therelationship between parent healthliteracy and pediatric emergencydepartment utilization: a systematicreview. Acad Pediatr. 2013;13(5):421–429
52. Hibbard JH, Stockard J, Mahoney ER,Tusler M. Development of the PatientActivation Measure (PAM):conceptualizing and measuring activationin patients and consumers. Health ServRes. 2004;39(4 pt 1):1005–1026
53. Greene J, Hibbard JH. Why does patientactivation matter? An examination ofthe relationships between patientactivation and health-related outcomes.J Gen Intern Med. 2012;27(5):520–526
54. Mosen DM, Schmittdiel J, Hibbard J,Sobel D, Remmers C, Bellows J. Ispatient activation associated withoutcomes of care for adults withchronic conditions? J Ambul CareManage. 2007;30(1):21–29
55. Greene J, Hibbard JH, Sacks R, OvertonV, Parrotta CD. When patient activationlevels change, health outcomes andcosts change, too. Health Aff (Millwood).2015;34(3):431–437
56. Maranda MJ, Deen D, Elshafey S,Herrera M, Gold MR. Response toa patient activation intervention amongSpanish-speaking patients ata community health center in New YorkCity. J Health Care Poor Underserved.2014;25(2):591–604
57. Cunningham PJ, Hibbard J, Gibbons CB.Raising low ‘patient activation’ ratesamong Hispanic immigrants may equalexpanded coverage in reducing accessdisparities. Health Aff (Millwood). 2011;30(10):1888–1894
58. DeCamp LR, Leifheit K, Shah H, et al.Cross-cultural validation of the parent-
PEDIATRICS Volume 145, number 1, January 2020 11 by guest on October 11, 2021www.aappublications.org/newsDownloaded from

patient activation measure in lowincome Spanish- and English-speakingparents. Patient Educ Couns. 2016;99(12):2055–2062
59. Liberman DB, Pham PK. Parentactivation in the pediatric emergencydepartment: theory vs. reality. PatientEduc Couns. 2018;101(6):1116–1122
60. DeCamp LR, Showell N, Godage SK, et al.Parent activation and pediatric primarycare outcomes for vulnerable children:a mixed methods study [publishedonline ahead of print July 2, 2019].Patient Educ Couns. doi:10.1016/j.pec.2019.07.004
61. Gurol-Urganci I, de Jongh T, Vodopivec-Jamsek V, Atun R, Car J. Mobile phonemessaging reminders for attendance at
healthcare appointments. CochraneDatabase Syst Rev. 2013;(12):CD007458
62. Kannisto KA, Koivunen MH, Välimäki MA.Use of mobile phone text messagereminders in health care services:a narrative literature review. J MedInternet Res. 2014;16(10):e222
63. Schwebel FJ, Larimer ME. Using textmessage reminders in health careservices: a narrative literature review.Internet Interv. 2018;13:82–104
64. Head KJ, Noar SM, Iannarino NT, GrantHarrington N. Efficacy of textmessaging-based interventions forhealth promotion: a meta-analysis. SocSci Med. 2013;97:41–48
65. Irizarry T, DeVito Dabbs A, Curran CR.Patient portals and patient
engagement: a state of the sciencereview. J Med Internet Res. 2015;17(6):e148
66. Ketterer T, West DW, Sanders VP,Hossain J, Kondo MC, Sharif I.Correlates of patient portal enrollmentand activation in primary carepediatrics. Acad Pediatr. 2013;13(3):264–271
67. Goel MS, Brown TL, Williams A, Hasnain-Wynia R, Thompson JA, Baker DW.Disparities in enrollment and use of anelectronic patient portal. J Gen InternMed. 2011;26(10):1112–1116
68. Montalbano A, Rodean J, Kangas J, LeeB, Hall M. Urgent care and emergencydepartment visits in the pediatricmedicaid population. Pediatrics. 2016;137(4):e20153100
12 DECAMP et al by guest on October 11, 2021www.aappublications.org/newsDownloaded from

originally published online December 26, 2019; Pediatrics Rodríguez and Sarah Polk
Cortez, Linxuan Wu, Kevin J. Psoter, Kassandra Quintanilla, Tatiahna Rivera Lisa Ross DeCamp, Sashini K. Godage, Doris Valenzuela Araujo, José Dominguez
TrialA Texting Intervention in Latino Families to Reduce ED Use: A Randomized
ServicesUpdated Information &
019-1405http://pediatrics.aappublications.org/content/early/2019/12/20/peds.2including high resolution figures, can be found at:
References
019-1405#BIBLhttp://pediatrics.aappublications.org/content/early/2019/12/20/peds.2This article cites 47 articles, 7 of which you can access for free at:
Subspecialty Collections
chnology_subhttp://www.aappublications.org/cgi/collection/health_information_teHealth Information Technology_subhttp://www.aappublications.org/cgi/collection/community_pediatricsCommunity Pediatricsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on October 11, 2021www.aappublications.org/newsDownloaded from

originally published online December 26, 2019; Pediatrics Rodríguez and Sarah Polk
Cortez, Linxuan Wu, Kevin J. Psoter, Kassandra Quintanilla, Tatiahna Rivera Lisa Ross DeCamp, Sashini K. Godage, Doris Valenzuela Araujo, José Dominguez
TrialA Texting Intervention in Latino Families to Reduce ED Use: A Randomized
http://pediatrics.aappublications.org/content/early/2019/12/20/peds.2019-1405located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2019/12/19/peds.2019-1405.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2019has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on October 11, 2021www.aappublications.org/newsDownloaded from