a setting including psychotherapy and psychopharmacological treatment in a case of anorexia nervosa...
TRANSCRIPT
CASE REPORT A setting including psychotherapy andpsychopharmacological treatment in acase of anorexia nervosa withobsessive compulsive disordercomorbidity
A. Ramacciotti*, S. Pallanti* and A. Pazzagli***Istituto di Neuroscienze, and **Department of Neurology and Psychiatry, Florence University, Florence
ABSTRACT. In this case report we describe the therapy followed with a patient affected byatypical anorexia purging, in a setting that includes both psychotherapy and psychopharmacological treatment. The aim of this presentation is to show how the patient’s ambivalencetowards the treatment was faced, and how this work both rendered effective the pharmacological therapy and enabled the progression of the psychotherapy. There is a discussion othe interaction between psychotherapy and pharmacological therapy and their possible beneficial action on the symptomatology. (Eating Weight Disord. 2, 222-228, 1997). ©1997, Editrice Kurtis
CASE REPORT
Motivation to undergo any form of therapyis one of the individual patient variables ofnegative outcome in cases of anorexia ner-vosa (1). Negation of the illness, not feelinginvolved as a subject, and the inability torecognize inner experience all characterizedmost of the early clinical descriptions ofcases of anorexia (2, 3).
Studies of insight [defined by Greenfeld (4)as the ability to acknowledge having an ill-ness or symptoms, as well as an awareness ofthe need for treatment and the risk of recur-rence] conducted on anorexic patients in hos-pital treatment, have considered insight as animportant clinical variable, which can, tosome extent, predict outcome. In particular,the capacity to acknowledge illness has beenassociated with better outcome measures (5).
Fear of possible psychological or physicalchanges, gain for illness, family conflicts,and incomprehensible self-destructive ten-dencies, in variable proportions, generatean ambivalent attitude towards therapy,causing refractoriness, drop out, or theunfruitful flitting from one therapy toanother with negligible results.
Treasure et al. (6) have applied a trans-theoretical model of change and proposed
the use of a motivational interview in orderto indicate how therapy can be targeted tomaximize the level of motivation and to promote change itself.
In psychotherapeutic work with anorexicsBruch (7) advised the strict avoidance of theory-based interpretation of unconsciouswishes in the drive-defense configurationand focused instead on the goal of thepatient recognizing what she really thinksand feels, that is to say, on “clarifyng”. Buresistance can be used not only to indicatetreatment resistance (8), it can also be considered part of the therapeutic process andFreud (9) first discovered transference asresistance, as the main obstacle. The creationof a therapeutic setting is a condition sinequa non of adequate attention to resistanceand transference phenomena. In additionthe establishment of a setting (10) as a safesecure place, free from threat, facilitates theestablishment of the therapeutic relationship. Such positive therapeutic alliances canalso be used to predict outcome (11, 12).
The psychodynamic therapeutic instruments of the treatment process include provision of the setting, recognition, clarification, interpretation, construction, reconstruction and working through, and theseconstitute well-established steps. It’s impor
Key words:Resistance, anorexia,citalopram, psychotherapy,obsessive compulsivesymptoms.Correspondence:Dr. Adriana Ramacciotti,Viale Ugo Bassi 1,50137 Firenze, ItalyReceived: November 6, 1997Accepted: February 11, 1998
222

A. Ramacciotti, S. Pallanti and A. Pazzagli
individual patient and the phase of the ill-ness. Recently, there has been increasinginterest in a systematic integration of dif-ferent approaches (16). Stepped care, deci-sion-tree and integration models which relyon set rules for the delivery of varioustreatment options have a shared value sys-tem of non-allegiance to a single theoreticalorientation, which permits different pointsof emphasis according to given cases (16).
There are, however, many reasons whypharmacological treatment should rarelybe the primary method of treatment foranorexia nervosa. They include the highdrop out rates reported in most medicationtrials, the risk of drug-related side effectsand data suggesting high relapse rates fol-lowing the discontinuation of drugs.
Although it is common practice to simulta-neously implement different therapies in thetreatment of anorexia nervosa, there hasbeen no development of hypotheses regard-ing possible reciprocal interactions (17).Only one controlled study has addressed thequestion of the efficacy of combining psy-chological therapy and pharmacotherapy(18), yet in this study the only parameter thatis evaluated is weight increase, and althoughthe authors conclude that there are noadvantages to be gained by combining ther-apy, there is no consideration of possibleforms of interaction or of the effects of psy-chological factors.
Klerman (19) reviewed the ideologicalconflicts in combined treatment and sug-gested a number of hypotheses about pos-sible interactions (both positive and nega-tive) between psychotherapy and pharma-cotherapy (Table 1) (17 ).
In this case report we describe the therapyfollowed with a patient affected by anorexiapurging, in a setting that includes both psy-choanalytically-orientated psychotherapyand psychopharmacological treatment. Theaim of this presentation is to show how thepatient’s ambivalence towards the treatmentwas faced and how this work has enabledboth the effects of the pharmacological ther-apy and the progression of the psychothera-py, with consequent symptomatic improve-ment.
CASE HISTORY
G.M. is a 33-year-old social worker,unmarried, and with no family history of
223
tant to stress the need for empathy andflexibility in the management of theseinstruments, assessing the clinical utility ofthe interpretation case by case (13).
What must be underlined is the impor-tance of the skillful management of the ten-dency of the patient to act, because there isthe risk of causing boredom, irritation andhostility which could put both patient andtherapist on the defensive. In such condi-tions the therapist may be led to act inways that are incompatible with his or herstance as an empathic listener and clarifier.
These tendencies are precisely themanoeuvers that get the patient into troublein his or her interactions with significantothers and, what is more, they are also oneof the main expressions of ambivalence (14).
No one form of treatment has yet beenfound to be clearly better and experiencedtreatment teams consequently utilize acombination of medication management,nutritional rehabilitation, family education-al therapy, psychoanalytical therapy, andpharmacotherapy as a basis for multidi-mensional approaches (15). These differentcomponents of treatment require varyingdegrees of emphasis, depending on the
TABLE 1
Possible negative effects of drug therapy on psychotherapy
1. Drug-induced reduction of symptoms as motives for discontinuing psy-chotherapy.
2. Pharmacotherapy undercuts defences.
3. Possible deleterious effects of pharmacotherapy on psychotherapy expec-tations.
4. If the psychotherapist is also the person who administers the medication, dele-terious effects could be generated in the psychotherapeutic relationship (anauthoritarian attitude on the part of the psychiatrist, dependency, placinggreater reliance on magical thinking, passivity on the part of the patient).
Possible positive effects of drug therapy on psychotherapy
1. Drugs facilitate accessibility to psychotherapy.
2. Drugs influence the ego psychological functions required for participationin psychotherapy.
3. Drugs promote abreaction.
4. Positive effects of drug therapy on expectations, and a reduction of stigma.
Possible negative effects of psychotherapy on drug therapy
1. Psychotherapy may be symptomatically disruptive.
Possible positive effects of psychotherapy on drug therapy
1. Psychotherapy facilitates drug compliance and adherence.
2. Psychotherapy could be seen as rehabilitation rather than treatment.

Combined treatment in anorexia
psychiatric disorder. When she came forconsultation, she was deeply depressed,anxious and in considerable distress, had aneating disorder and displayed obsessivesymptomatology . These symptoms took upabout 60% of her day and consequently shewas no longer able to work; she walked inthe sun, reading a book, for no less thanthree hours a day, she was continually tidy-ing her house so as to keep everything inprecise order, and she maintained a linkbetween her house and that of her parentsby means of food which she took from herparents’ after having carefully checked thecontents of her mother’s fridge and foodcupboards. In this way she had managed toaccumulate so much food that her kitchenwas crammed with cans, jars and mouldyfood that she nevertheless consumedbecause she was unable to throw anythingaway.
In the month prior to her arrival, she hadreduced her daily food intake, used laxa-tives, and induced vomiting twice a week.Her body weight had diminished by 5 kilosin less than a month (BMI 17,5) and dis-played amenorhoea.
The patient told us she was 16 when heranorexia began, and that it involved a sig-nificant weight loss. She had lost approxi-mately 10 kilos in three months as a resultof self-imposed restrictions on her foodintake which lasted for about 2 years. Thiswas followed in the following 2 years by asignificant weight increase (about 20 kilos)which in turn gave way to another phase offood restriction and the onset of the obses-sive symptomatology (repeated checking,walks and compulsive exposure to the sun).
Ten years ago, when she was 23, with astable body weight (BMI 22 ), she started ajob as a social worker, which she still has,and a relationship with L., which lasted for5 years. It was ended, by her, shortly beforethey were due to marry (the invitations hadalready been sent out). From then on, untillast year, she had a number of brief rela-tionships, intense but doomed to failure,which when they predictably ended, pro-voked deep depressive crises and a wors-ening of the obsessive symptomatology,which led her to try several different kindsof pharmacological treatment (clorim-ipramina 75 mg/d, fluoxetine 60 mg/d).However, she was discontinuous in takingthem and did not adhere to the prescribeddosages. She underwent cognitive behav-
ioral therapy that lasted for one year,which she considered to have been of verylittle value, because the obsessive symp-toms did not alter and the eating symptomsworsened. Not withstanding the fact thatshe accepted programs and regularly kepta record of what she ate, she was unable tofollow them and decreased her food intakeor increased her physical activity. In addi-tion, she had been doing family therapy fortwo years, which involved the whole family.Both the patient and the family were verydisappointed and discouraged by the manyyears of illness and treatment and did nothave much faith in the possibility of a suc-cessful outcome to the treatment. Sheclaimed that the various therapies had beena complete failure, no one was able tounderstand how to cure her and that drugs,even if they were taken regularly, wouldprobably not have any positive effects.
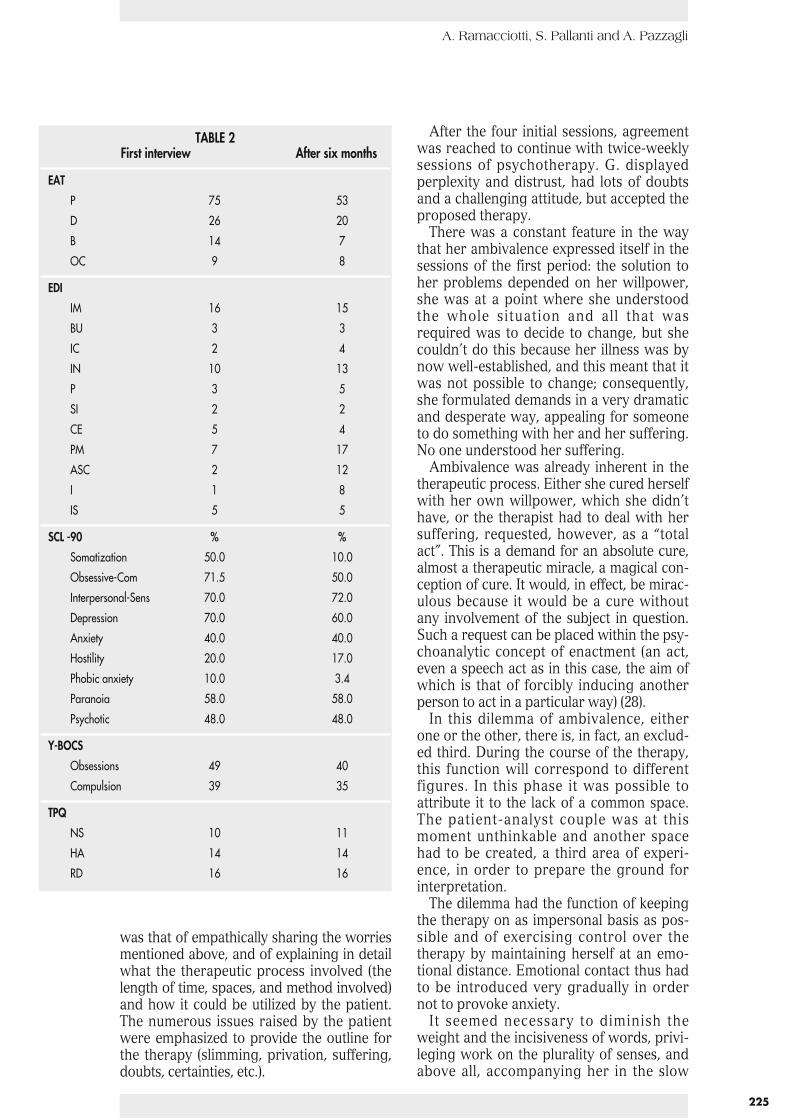
The diagnostic assessment was per-formed with the following instruments:EAT 40 (20, 21); EDI (22); SCL-90(23); TPQ(24); Y-BOCS (25); this took place in the ini-tial sessions and subsequently, six monthslater (Table 2).
We proposed to the patient a therapeuticsetting that included pharmacologicaltreatment and initial interview sessions, inorder to start a psychoanalytically-orientat-ed therapy with a therapist who had notbeen involved in the patient assessment orin the pharmacological treatment.
The pharmacological therapy consistedof 40 mg of citalopram and the therapeuticsetting, which observed the general guide-lines of the Clinical Management fluoxetinecondition (26), aimed to diminish the purg-ing, and the obsessive and depressivesymptomatology. The dosage used was thesame as that adopted in the therapy forobsessive disorders and anorexic restrict-ing type (27) because there is no referencein current literature about the use of citalo-pram in this subtype of anorexic patient.
The initial interviews were marked byintense ambivalence, which affected thedevelopment of the therapy. Feelings ofdesperation about the symptoms and thefear of a possible physical breakdown alter-nated with joy at her great loss of weight,and a feeling of vindication about herchoice of life style, seen as being entirelypersonal and unchallengeable.
In this difficult situation, marked by a senseof impotence, the position of the therapist
224
A. Ramacciotti, S. Pallanti and A. Pazzagli
225
was that of empathically sharing the worriesmentioned above, and of explaining in detailwhat the therapeutic process involved (thelength of time, spaces, and method involved)and how it could be utilized by the patient.The numerous issues raised by the patientwere emphasized to provide the outline forthe therapy (slimming, privation, suffering,doubts, certainties, etc.).
After the four initial sessions, agreementwas reached to continue with twice-weeklysessions of psychotherapy. G. displayedperplexity and distrust, had lots of doubtsand a challenging attitude, but accepted theproposed therapy.
There was a constant feature in the waythat her ambivalence expressed itself in thesessions of the first period: the solution toher problems depended on her willpower,she was at a point where she understoodthe whole situation and all that wasrequired was to decide to change, but shecouldn’t do this because her illness was bynow well-established, and this meant that itwas not possible to change; consequently,she formulated demands in a very dramaticand desperate way, appealing for someoneto do something with her and her suffering.No one understood her suffering.
Ambivalence was already inherent in thetherapeutic process. Either she cured herselfwith her own willpower, which she didn’thave, or the therapist had to deal with hersuffering, requested, however, as a “totalact”. This is a demand for an absolute cure,almost a therapeutic miracle, a magical con-ception of cure. It would, in effect, be mirac-ulous because it would be a cure withoutany involvement of the subject in question.Such a request can be placed within the psy-choanalytic concept of enactment (an act,even a speech act as in this case, the aim ofwhich is that of forcibly inducing anotherperson to act in a particular way) (28).
In this dilemma of ambivalence, eitherone or the other, there is, in fact, an exclud-ed third. During the course of the therapy,this function will correspond to differentfigures. In this phase it was possible toattribute it to the lack of a common space.The patient-analyst couple was at thismoment unthinkable and another spacehad to be created, a third area of experi-ence, in order to prepare the ground forinterpretation.
The dilemma had the function of keepingthe therapy on as impersonal basis as pos-sible and of exercising control over thetherapy by maintaining herself at an emo-tional distance. Emotional contact thus hadto be introduced very gradually in ordernot to provoke anxiety.
It seemed necessary to diminish theweight and the incisiveness of words, privi-leging work on the plurality of senses, andabove all, accompanying her in the slow
TABLE 2First interview After six months
EAT
P 75 53
D 26 20
B 14 7
OC 9 8
EDI
IM 16 15
BU 3 3
IC 2 4
IN 10 13
P 3 5
SI 2 2
CE 5 4
PM 7 17
ASC 2 12
I 1 8
IS 5 5
SCL -90 % %
Somatization 50.0 10.0
Obsessive-Com 71.5 50.0
Interpersonal-Sens 70.0 72.0
Depression 70.0 60.0
Anxiety 40.0 40.0
Hostility 20.0 17.0
Phobic anxiety 10.0 3.4
Paranoia 58.0 58.0
Psychotic 48.0 48.0
Y-BOCS
Obsessions 49 40
Compulsion 39 35
TPQ
NS 10 11
HA 14 14
RD 16 16

Combined treatment in anorexia
process of working through because other-wise words would remain outside of her.
“What’s the point of talking about allthis? Words don’t touch me”.
This enunciation was in reality the affirma-tion of the contrary, words could touch andaffect her, and to a great degree; the ana-lyst’s words too, might be too powerful andcould invade, manipulate or change her.Drugs might also provoke unforseen anduncontrollable changes which frightened hera great deal. Possible unforseen change thatcould affect her physical appearance or herpersonality were sources of anguish. She didnot want to introduce changes into her lifeand her control rituals were absolutely nec-essary for her and even though she recog-nized that this contributed to reinforcing herillness, when she had introduced changesinto her life (which seemed to be of a com-pulsive nature), “things turned out badly”.
In fact the reconstruction of her love liferevealed a kind of split. On the one hand,there was the current boyfriend who repre-sented a monotonous emotional life, lackingin emotion or sex, there not even being timefor them to be together because her ritualstook up so much time. It was however, stableand there was the possibility, even though itwas put off and barely even discussed, ofmarriage. This relationship had begun againthe previous year (a certain degree of contacthad been maintained over the years) and thequestion of marriage was raised once again.It was at this point that she consulted us, dueto the deterioration of her restrictive eatingsymptoms and the increase in her rituals. Onthe other hand, there were relationships thatnever lasted more than a year, that wereintensely involving emotionally, but whichwere relationships with married men, whichdid not allow her to think in terms of a futureas part of a couple. During these relation-ships, the eating and obsessive symptomatol-ogy improved radically but when the rela-tionship predictably ended, she fell into deepcrises of depression, and had feelings ofemptiness, loneliness and abandonment.
Resistance appeared in both the narrationof her life story and the expression of herexpectations of unrealized and unrealisticchange, through continual negations, trans-fers and questions like “What’s the point oftalking about all this?”. Resistance involved aprocess of desubjectivisation when, forexample, in the middle of her own discourse,she would directly introduce the presumed
opinions and desires of other people regard-ing her (“My parents would like to have meadmitted to a clinic specializing in eating dis-orders”, “L. thinks an out-patient clinicwould be better”. “What do you think?”).
The moves adopted by the therapist inthis period were aimed at underlining thatthe continual negations, the attempts atshifting the focus of attention and transfer-ring into the discourse of others, werebeing used to keep away from things thatwere important for her, like, for example,marriage, and being a “flower” (an expres-sion used by the patient to mean being awoman, not being reduced to eating left-overs and hoarding mouldy food.) Theinterpretations of transference and of intra-and extra-transferral acts were used tomake clear a number of different points.
Oedipal problems emerged as a result ofthe long-term relationship, the conse-quences of which were observed funda-mentally in three main areas:
1. in the restriction of pleasure, and adenial of her sexual drives (not eating, nothaving sexual relationships, not wanting tobe caressed or kissed);
2. being intensely wrapped up with herphysical appearance (desiring a thin,strong, shapeless body);
3. self-punishment (not eating things thatshe liked, occupying her time with inex-orable activities and exposure to the sunwhich exhausted her, preventing her fromenjoying pleasurable activities).
However, her ambivalence towards thera-py and her fear of change were not exclusiveto the first phase of the therapy but appearedat different moments, in relation to differentmatters and at different levels of the realityof the therapeutic relationship. For instance,she had to suffer. No one understood how tocure her, her suffering was exhausting, andeven though she openly complained abouthow much she was suffering, she had to suf-fer, as her mother had suffered. G. was thesecond child of a well-off family which wasvery religious, and her parents, who are nowretired, had worked all their lives, the motheras a teacher and the father as a businessman.Both her sister and her brother were mar-ried with two children, and her sister was asuccessful businesswoman. They had, in herview, realized their dreams, while she, thesick and suffering member of the family, hadnot. In this respect the patient was intransi-gent: she reproved her mother for having
226

A. Ramacciotti, S. Pallanti and A. Pazzagli
complained of her suffering and of havingworked. She, however, had to go one stepfurther: “I suffer because you have suffered,but I suffer more than you, because I amdepriving myself of things that you neverdeprived yourself of, and I want you tounderstand that by suffering, and I’ll keepgoing until you do”.
In these six months of therapy, the bodyweight of the patient remained low but sta-ble, she did not vomit or use laxatives, andthe obsessive symptoms modified slightly,above all in their intensity and the timedevoted to them. The most significantchange regarded her personal space: unus-able and out-of-date things were thrownaway, making space for other things andmaterials representing desires that hadnever been realised or expressed withoutbeing punished.
CONCLUSION
Ambivalence and resistance are not spe-cific to anorexia but these dynamics areoften to be found in this disorder and can beespecially intense in the initial phases oftherapy, frequently causing great difficultiesin therapeutic engagement, with the risk oftreatment being discontinuous or aban-doned altogether. We have tried to show apossible way of working with ambivalencein the early phase of therapy with thispatient who is both anorexic and obsessive,through the simultaneous creation of a set-ting in which the problem can be recog-nized, clarified and articulated, and also thecareful observation of the transference phe-nomenon in which resistance is part of thetherapeutic process and appears throughoutthe therapy at different moments, in relationto different questions and at different levelsof the reality of the therapeutic relationship.
We do not use the developmental per-spective of separation-individuationprocess (29, 30) as a key to reading or as atheoretical model. A more in-depth study ofthese aspects is however, essential for thefuture progress of psychotherapy.
It is difficult to specify quantitatively howmuch of an impact the pharmacological ther-apy had on the symptoms and to what extentthe psychotherapy was a factor in the gener-al improvement of the patient. We canhypothesise that the psychotherapeutic workfacilitated continuity in taking pharmacologi-
cal treatment, which had in the past beencompromised. The various forms of pharma-cological treatment with antidepressants andserotoninergics, which have been document-ed as being very effective in the treatment ofdepressive and obsessive symptoms, and ofpurging symptomatology, had been of negli-gible benefit because of the discontinuitywith which they were taken, the nonobser-vance of the doses, and of other treatmentparameters. The work on the ambivalence ofthe patient towards the treatment of her dis-orders (in relation to which she showed verylittle insight) was the most significant aspectof the therapeutic process and made it possi-ble subsequently to enter into the dynamicsof behaviour, feelings and impulses in such away as to give continuity to the narrativethread of the patient’s personal history. Infact, through the interpretation of relationalmodalities that the patient repeated, it waspossible to place a number of emotive-affec-tive moments that not only marked breaks inthe patient’s personal history but which werealso very closely linked to the improvementand deterioration of the symptomatology.
It is a legitimate conjecture that the phar-macological treatment had an effect on themost salient aspects of the symptomatology(the impulsivity, the rituals, the purging con-duct) while the psychotherapy improved theinterpersonal and affective relationships andreduced the self-destructive tendencies,putting the patient into a position where shecould have an attitude that was less punitive,and less characterized by blame and sacri-fice. Moreover, the pharmacological therapyin itself represented a therapeutic act thatoften constituted a material within the psy-chotherapy because of the significance that itassumed - intrusiveness, orality, uncon-trolled effects, protection, etc. - providing anopportunity to analyse its symbolic signifi-cance and the relation with other significantobjects.
REFERENCES
1. Schoemaker C.: Does early interventionimprove the prognosis in anorexia nervosa?A systematic review of the treatment-out-come literature. Int. J. Eating Disord., 21, 1-15, 1997.
2. Lasègue E.C.: De l’anorexie hystérique.Arch. Gen. Med., 21, 385-403, 1873.
3. Bruch H.: Eating disorders: Obesity, anorex-
227
Combined treatment in anorexia
228
ia nervosa, and the person within. NewYork, Basic Books, 1973.
4. Greenfeld D.G., Strauss J., Bowers M.B.,Mandlekern M.: Insight and interpretationof illness in recovery from psychosis.Schizophr. Bull. 15, 245-252, 1989.
5. Greenfeld D.G., Anyan W.R., Hobart M.,Quinlan D.M., Plantes M.: Insight into illnessand outcome in anorexia nervosa. Int. J.Eating Disord., 10, 100-109, 1991.
6. Treasure J., Ward A.: A practical guide tothe use of motivational interviewing inanorexia nervosa. Eur. Eating Dis. Rev. 5,102-114, 1997.
7. Bruch H.: The golden cage. Cambridge, MA,Harvard University Press, 1978.
8. Cuzzolaro M., Ripa di Meana G.: La resisten-za nelle terapie psicoanalitiche: osservazionisull’anoressia nervosa. Psicobiettivo X, 15-28, 1990.
9. Freud S.: L’interpretazione dei sogni. OSF.Boringhieri, 1900.
10. Winnicott D.W.: Maturational processes andthe facilitating environment. New York,International Universities Press, 1965.
11. Luborsky L.: Capire il transfert, Milano,Raffaello Cortina Editore, l992.
12. Horwath A., Greenberg L.: The developmentof the working alliance inventory. In:Greenberg L., Pinsoff W. (Eds.), Psy -chotherapeutic process: A research hand-book. New York, Guildford Press, 1986, pp.529-556.
13. Swift W.: Bruch revisited: The role of inter-pretation of transference and resistance inthe psychotherapy of eating disorders. In:Johnson C. (Ed.), Psychodynamic treatmentof anorexia nervosa and bulimia. New York,Guilford Press, 1991, pp. 51-67.
14. Garner D.M., Garfinkel P.E., Bemis K.M.: Amultidimensional psychotherapy for anorexianervosa. Int. J. Eating Disord., 1, 3-46, 1982.
15. Garner D., Needleman L.: Sequencing andintegration of treatments. In: Garner D.M.,Garfinkel P.E. (Eds.), Handbook of treatmentfor eating disorders. New York, GuilfordPress, 1997, pp. 50-63.
16. Kennedy S.H., Goldbloon D.S.: Psycho -pharma cological treatment. In: Halmi K.A.,Garfinke P.E. (Eds.), Section 10 cap 77:Eating Disorders. In: Gabbard G.O.,Atkinson S.D. (Eds.), Synopsis of treatmentsof psychiatric disorders. Am. PsychiatricPress, 1996, pp. 901-907.
17. Eckert E.D.: Anorexia nervosa. In: Beitman,Klerman (Eds.), Integrating pharmachother-apy and psychotherapy. Am. Psychiatr.Press, 1991, pp 329-351.
18. Goldberg S.C., Halmi K.A., Eckert E.D., etal: Cyproheptadine in anorexia nervosa. Br.J. Psychiatry 134, 67-70, 1979.
19. Klerman G.L.: Ideological conflicts in inte-grating pharmacotherapy and psychothera-py. In: Beitman, Klerman (Eds.), Integratingpharmachotherapy and psychoterapy. Am.Psychiatric Press, 1991, pp. 3-19.
20. Garner D.M., Garfinkel P.E.: The eating atti-tudes test: an index of the sympthoms ofanorexia nervosa. Psychol. Med., 9, 273-279,1979.
21. Cuzzolaro M., Petrilli A.: Validazione dellaversione italiana dell’EAT-40 di GarnerD.M., Garfinkel P.E. Psichiatria dell’Infanziae dell’Adolescenza, 55, 209-217, 1988.
22. Garner D.M., Olmstead M.P., Polivy J.:Development and validation of a multidi-mensional eating disorder inventory foranorexia nervosa and bulimia. Int. J. EatingDisord., 1, 15-34, 1983.
23. Derogatis L.R.: Symptom checklist manual.Baltimore, Johns Hopkins University Press,1977.
24. Cloninger C.R.: A systematic method forclinical description and classification of per-sonality variants. Arch. Gen. Psychiatry, 44573-588, 1987.
25. Goodman W.K., Price L.H., Rasmussen S.A.,Mazure C., Fleischmann R., Hill C.L.,Heninger G.R., Charney D.S.: The YaleBrown obsessive-compulsive scale. I.Development, use, and reliability. Arch.Gen. Psychiatry, 46, 1006-1011, 1989.
26. Goldbloom D.S., Davis R., Olmsted M., ShawB.: Clinical management-fluoxetine adminis-tration manual. Toronto Hospital 1996.
27. Pallanti S., Quercioli L., Ramacciotti A.:Citalopram in anorexia nervosa. EatingWeight Disord., 2, 216-221, 1997. (in press).
28. McLaughlin J.T.: Clinical and theoreticalaspects of enactment on the psychoanalyticsituation. J. Am. Psychoanal. Assoc., 39,595-614, 1991.
29. Mahler M.: On the first three subphases ofthe separation-individuation process. Int. J.Psychoanal., 53, 333-338, 1972.
30. Fischer N.: Anorexia nervosa and unre-solved rapprochement conflicts. A casestudy. Int. J. Psychoanal., 70, 41-54, 1989.