a rare case of invasive amoebiasis requiring emergency...
TRANSCRIPT

A rare case of invasive amoebiasis requiring emergency subtotal colectomy in an HIV-positive man DrRobertBall1DrFionaCampbell2,DrStevenWoolley1,3,MrRichardHeath4,DrNickBeeching1,5,DrLanceTurtle1,6,DrTomWingfield1,6,7
TropicalandInfectiousDiseaseUnitRoyalLiverpoolUniversityHospital
1. TropicalandInfectiousDiseaseUnit,RoyalLiverpoolUniversityHospital2. Departmentofcellularpathology,RoyalLiverpoolUniversityHospital3. InstituteofNavalMedicine,Alverstoke,Hampshire4. Departmentofcolorectalsurgery,RoyalLiverpoolUniversityHospital5. LiverpoolSchoolofTropicalMedicine,Liverpool6. InstituteofInfectionandGlobalHealth,UniversityofLiverpool7. DepartmentofPublicHealthSciences,KarolinskaInstitutet,Stockholm

Presentation
• 56yearoldmale,MSM
• 2monthsinIndonesia,VietnamandMalaysia• PresentedonreturntoUK
• 2weekswaterydiarrhoea• >10stools/day,occasionalfreshblood
• HIV+ve,CD4194cells/mm3,viralloadundetectable
• Tenofovir,emtricitabine,nevirapine

Investigations • Observations:
• Heartrate 103bpm• Bloodpressure 155/78mmHg• Temperature 37.0oC• Respiratoryrate 19breaths/min
• Raisedinflammatorymarkers• CRP 282mg/L(<5)• Neutrophils 12.9x109/L(2-10)• Prothrombintime 19.8s (9-13)• AlanineAminotransferase55U/L(<35)
• Consideredlikelybacterialgastroenteritis
• Commencedoralazithromycin

Day 3 of admission
• Morningconsultantwardround• Acuteabdominaldistension,generalisedperitonitis
• CommencedIVceftriaxoneandmetronidazole
• UrgentCTabdomenwithcontrast• Severepancolitis• Perforationsofthecaecumandsigmoidcolon• Twosmallhypoechoiclesionsintheliver

Day 4 of admission
• Emergencylaparotomy• Gangrenousnecroticcaecum• Serosalevidenceofcolitiswithrectalsparing• Faecalcontaminationoftheperitonealcavity
• Subtotalcolectomy• Spoutingendileostomyformation

Day 1 post-op
• RecoveryinIntensiveTherapyUnit(ITU)
• Intra-abdominaldrains• Lactobacillusrhamnosusin,Streptococcusmilleri(anginosus)
• Surgicalwoundswabs• Enterococcusgallinarum,Escherichiacoli
• Continuesceftriaxoneandmetronidazole

Week 1-2 post-op • TransferredtoHighDependencyUnit(HDU)
• IncreasingcholestaticLFTs
• RepeatCTabdomen• Nochangeinthehypoechoiclesions• Likelyhaemangiomas
• MRCP• Normalbiliarytree
• Ceftriaxonechangedtotigecycline
0
500
1000
1500
2000
2500
3000
3500
1 2 3 4 8 9 10 11 12 13 14 15 17
U/L
Dayofadmission
GammaGT(U/L)
Alkalinephosphatase(U/L)
AlanineAminotransferase(U/L)
Laparotomyonday4

0
500
1000
1500
2000
2500
3000
3500
1 2 3 4 8 9 10 11 12 13 14 15 17 18 21 24 27 29 30 35 37 47
U/L
Dayofadmission
GammaGT(U/L)
Alkalinephosphatase(U/L)
AlanineAminotransferase(U/L)
Ceftriaxonechangedtotigecyclineday17
Laparotomyonday4

Day 8 post-op
Discreteulcerswithinthecolon

Flask-shapedulcers
Normalcolon
Normalcolon
1. Imagesfromwww.google.com
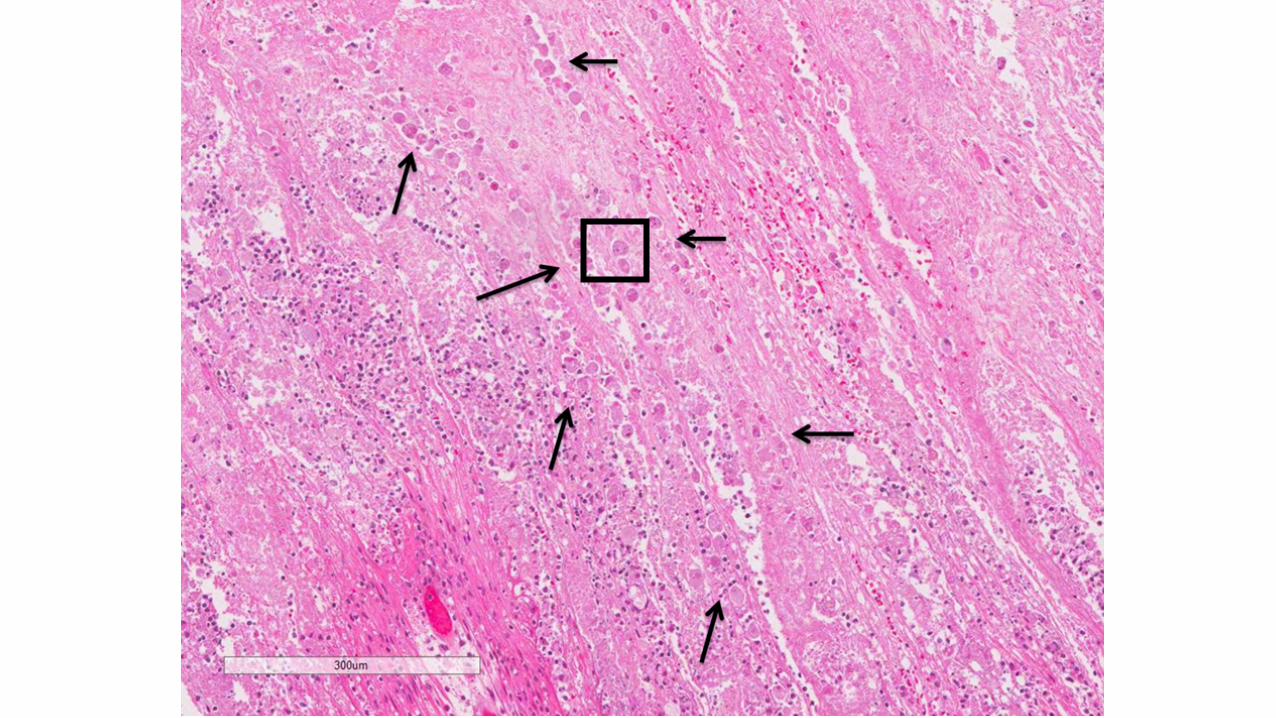

IngestedRBC
“Foamy”cytoplasm
E.histolyticatrophozoite
27dayspost-op
AmoebicIFApositive-1:512Amoebaelatextest-positive
60um

Case - outcome • Turbulentpost-operativerecovery
• IleusrequiringTotalParentalNutrition(TPN)• Abdominalwounddehiscence• Coagulopathy• Weightloss,deconditioningandimmobility
• Recoveredanddischargedhomeonweek5
• Noanti-retroviraltherapymissedduringadmission
• Totalantimicrobialtherapy:• Metronidazole14days• Tigecycline42days(completedasoutpatientIVtherapy)• Oralparomomycin7days

Case – 5 months post-op
• Goodrecovery• Usingstomaindependently• Goodwoundhealing
• Planningileorectalanastomosis• Forfurther7daysoralparomomycin

Fulminant amoebic colitis (FAC)

Fulminant amoebic colitis (FAC)
• Virulenthostresponsetoamoebaecausingfulminatingreaction• Necrotisingcolitis,perforationandperitonitis
• Uncommon(1:200)1
• Male=Female
• Presentsassurgicalemergency
1.Acuna-SotoR,WirthDFetal.AmJGastroenterol2000;95:1277-83

Fulminant amoebic colitis (FAC)
• Mumbai20142• Amoebiasisconsideredpre-operatively5/30• 28requiredemergencysurgery• Mortality17/30(57%)
2.ChaturvediR,JoshiASetal.PostgradMedJ2015;91:200-5


Key questions 1. Couldwehavemadeanearlierdiagnosis?
2. DoesbeingMSMhelpourdiagnosis?
3. DoesbeingHIV+vehelpourdiagnosis?
4. Doesheneedlumicidaltreatmentafterbowelre-anastamosis?
1. Could we have made an earlier diagnosis?
• Investigations• Stoolmicroscopy–3xnegative• Enzyme-linkedimmunosorbentassay(ELISA)• Indirectfluorescentassay(IFA)–took27dayspost-op
• Couldwehavedonebetter?• “Hotstool”formicroscopy?• RequesturgentIFA?• Couldwehavetreatedempirically?

2. Does being MSM help our diagnosis?
• China20103• 602MSM• 42%ofMSMseropositiveonELISAforEntamoebahistolytica• Higherseropositivityin“receptiveanalsex”
• Taiwan20074
• HIVpositivepatients• 70%wereMSM• MSMatsignificantlyhigherriskofamoebiasis
3.ZhouF,GaoCetal.PLoSNTD2013;e223244.HungCC,ColebundersRetal.PLoSNTD2008;e175

3. Does being HIV +ve help our diagnosis? • Mexico20055
• EntamoebahistolyticacystsonmicroscopyandPCR• NoincreaseinHIV+vecomparedto-ve
• Japan20136• 21.3%ofHIV+veonIFAforEntamoebahistolytica• Titresx400predictiveofinvasivedisease
• Linkunproven7• ConfoundedbyMSM
5.MoranP,XiménezCetal.ExpParasitol2005;110:331-46.WatanabeK,GatanagaHetal.JInfectDis2014;209:1801–77.HungCC,JiDDetal.LancetInfectDis2012;12:729-36

4. Does he need lumicidal treatment after bowel re-anastamosis? • Eradicatecoloniccarriageandpreventrecurrence
• Paromomycin25-35mg/kg/dayfor7days• Ordiloxanidefuroate,iodoquinol
• Rectalstumpuntreatedduetoileostomy• Norectalpreparations
• Noevidence/guidelines

Key questions 1. Couldwehavemadeanearlierdiagnosis?
q Possibly
2. DoesbeingMSMhelpourdiagnosis?q Possibly
3. DoesbeingHIV+vehelpourdiagnosis?q Probablynot
4. Doesheneedlumicicaltreatmentafterbowelre-anastamosis?q Probably

Questions?